")
Back to Journals » International Journal of Women's Health » Volume 14
Length of Hospital Stay After Cesarean Delivery and Its Determinants Among Women in Eastern Sudan
Authors Hassan B , Mandar O, Alhabardi N, Adam I
Received 2 January 2022
Accepted for publication 24 May 2022
Published 31 May 2022 Volume 2022:14 Pages 731—738
DOI https://doi.org/10.2147/IJWH.S356855
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Elie Al-Chaer
Bahaeldin Hassan,1 Omer Mandar,1,2 Nadiah Alhabardi,3 Ishag Adam3
1Department of Obstetrics and Gynecology, College of Medicine, King Khalid University, Abha, Saudi Arabia; 2Faculty of Medicine, Gadarif University, Gadarif, Sudan; 3Department of Obstetrics and Gynecology, Unaizah College of Medicine and Medical Sciences, Qassim University, Unaizah, Saudi Arabia
Correspondence: Omer Mandar, Faculty of Medicine, Gadarif University, P.O Box 449, Gadarif, 32211, Sudan, Email [email protected]
Background: There is an increasing caesarean delivery (CD) rate globally. Length of hospital stay (LoS) is longer in CD compared with vaginal delivery. There are few published data on LoS following CD in Africa, including Sudan. We aimed to investigate LoS after CD in eastern Sudan and its associated risk factors.
Methods: A cross-sectional study was conducted at Gadarif hospital in eastern Sudan from May to December 2020. Sociodemographic, clinical and obstetrical data were gathered through questionnaires. Poisson regressions were used to model the LoS and provide relative risk (RR) and a 95.0% confidence interval (CI).
Results: We enrolled 544 women with CD. The median (interquartile range, IQR) of their age and parity was 28.0 (24.0 ‒32.0) years and 3(2‒3), respectively. The LoS range was 1.0– 9.0 days (mean = 2.7 days) and its median (IRQ) was 3.0 (2.0‒3.0) days. The median (IQR) of the LoS was significantly higher in women who had emergency CD vs elective CD, [3 (3.0‒3.0) vs 3 (2.0‒3.0) days, P < 0.001] and in women with maternal complications vs women who had no maternal complications [3 (2.0‒3.0) vs 3 (2.0‒3.0) days, P < 0.001]. Poisson regression showed that women with emergency CD stayed for 13.0% longer than women with elective CD (RR=1.13, 95% CI=1.01‒1.29). Women with maternal complications stayed 24.0% longer than women who had no maternal complications (RR=1.24, 95% CI=1.07‒1.43). Women who had neonatal complications stayed for 21.0% longer than women who had no neonatal complications (RR=1.21, 95% CI=1.05‒1.40). Age, parity, residence, education, occupation and postoperative haemoglobin were not associated with LoS.
Conclusion: The mean LoS in this study was 2.7 days, and women with emergency CD and maternal and neonatal complications had longer LoS.
Keywords: caesarean delivery, emergency, elective, hospital stay, Sudan
Introduction
There is an increasing caesarean delivery (CD) rate globally (from 7% in 1990 to 21% in 2021) 1 and in the sub-Saharan region in particular (from 3.2% in 2012 to 5.9% in 2016).2 Compared with vaginal delivery (VD), CD is associated with increased maternal and perinatal morbidity and mortality rates.3 One of these factors is the length of stay (LoS) in the hospital, which is reported to be longer in CD than VD.4,5 Length of hospital stay is becoming an area of interest for researchers worldwide, as it is a readily available health indicator reflecting hospital activity and is an indirect estimator of resource consumption and efficiency.6,7 However, there is much debate on LoS and its duration after CD.
Early hospital discharge has been reported as a widespread practice nowadays, especially in the era of the COVID-19 pandemic.8 After CD, a short hospital stay may reduce the cost, staff and bed capacity.6,9 Moreover, short post-CD LoS is not associated with an increased readmission rate.9 However, the quality of care can be improved with the traditional discharge policy after four days, reducing the need for home care.6 The increasing number of days of stay is associated with an increase in delivery costs, especially in the private sector.5 The concept of a short LoS post-CD of fewer than four days was adopted by the American Academy of Pediatrics and the American College of Obstetricians and Gynecologists.4,10
There are few published data on LoS4,5,9,11,12 in CD and none of these exist in sub-Saharan Africa. Moreover, different criteria were used in these reports, yielding different results. Prolonged LoS was associated with older maternal age, parous, uneducated, low socioeconomic status and rural residents.4,5,12 Obstetric conditions, such as CD history, preeclampsia, preterm labour, low birth weight and multiple pregnancies, were associated with a prolonged LoS.12 Postoperative complications, such as wound infection and endometritis, were associated with prolonged LoS.13
Sudan is one of the low-income countries where the health system is deficient in staff and beds. There has been a dramatic increase in the CD rate in Sudan (43.2% in 2011).14 We aimed to assess LoS after CD in eastern Sudan and the associated factors. With the findings from this study, researchers and policymakers can help establish a protocol for hospital discharge to ensure proper postnatal care.
Materials and Methods
Study Settings
A cross-sectional study was conducted at the Gadarif hospital in eastern Sudan from May to December 2020. Gadarif hospital is a tertiary public hospital. The participants were recruited from the postnatal clinics of the hospital. All women who underwent CD during the study period attended the postnatal clinics, and consented to participate were included.
Data Collection
Sociodemographic, clinical and obstetrical data were gathered through a questionnaire, which was filled by a direct interview. These data included maternal characteristics [eg, age, education, residence, occupation and body mass index (BMI)], neonatal characteristics (eg, gender, birth weight, neonatal intensive care admission and neonatal death) and obstetrics data (eg, parity, gestational age at the time of delivery, CD and anaesthesia types). Other data [eg, haemorrhage, postoperative maternal haemoglobin (second day), postoperative fever, wound infection, endometritis, urinary tract infection and LoS] were also collected from each participant and from the medical records through a questionnaire administered by a trained medical officer.
Outcome Definitions
Low birth weight (LBW) was defined as a birth weight of 2500 grams or less, as per the World Health Organization.15 Wound infection was counted in the presence of seropurulent discharge, redness (or both), induration or swelling of wound site.16 Postoperative fever was defined as a temperature higher than 38°C (100.4°F).17 Post-caesarean endometritis is a clinical diagnosis that includes fever, uterine tenderness and/or purulent lochia requiring antibiotics prescription.17
Maternal complications in this study included preoperative obstetric disorders (eg gestational diabetes, preeclampsia, antepartum haemorrhage and others), anaesthetic complications (eg, infections meningitis, direct needle trauma and vertebral canal hematoma), uterine artery injury, ureteric injury, caesarean hysterectomy, intraoperative haemorrhage, wound infections and postoperative fever. Neonatal complications were LBW deliveries, low APGAR score at one minute, low APGAR score at 5 min, admission to NICU and neonatal death.
Sample Size Calculation
As previously reported,18 the sample size of 544 women was calculated based on the assumption that there was a significant minimum difference in the correlations (r = 0.12) between LoS and the other independent factors, such as age, parity, BMI and haemoglobin. This sample size (544) was necessary to achieve a 95% confidence level with a 5% margin of error and 80% power.
Statistical Analyses
The data were analysed with the Statistical Package for the Social Sciences (SPSS) Statistics for Windows, version 22.0 (IBM, Armonk, NY, USA). Continuous data were checked for normality using the Shapiro–Wilk test. When they were found not to be normally distributed, they were expressed as a median (interquartile range [IQR]), while the categorised data were expressed as a frequency (proportion). Univariate analyses were performed to compare variables with LoS using the Mann–Whitney U–test (non-parametric) or Spearman correlations. The variables in the univariate analysis, with their P < 0.200, were shifted to build Poisson regression to model the LoS and provide relative risk (RR) and 95.0% confidence interval (CI). The LoS was considered the dependent variable, while sociodemographic, obstetric and neonatal factors were the independent variables. A two-sided p-value of less than 0.05 was considered statistically significant.
Results
General Characteristics
We enrolled 544 women with CD. The median (interquartile range, IQR) of their age and parity was 28.0 (24.0 ‒32.0) years and 3(2‒3), respectively. Around one-third (32.4%) of them had ≥ secondary level of education. The majority (91.0%) of these 544 women were housewives. Over half of them (53.1%) resided in rural areas. Almost four out of five (79.6%) had elective CD, and all had spinal anaesthesia. The median (IQR) of the postoperative haemoglobin was 10.3 (9.6 ‒11.2) g/dl, Table 1.
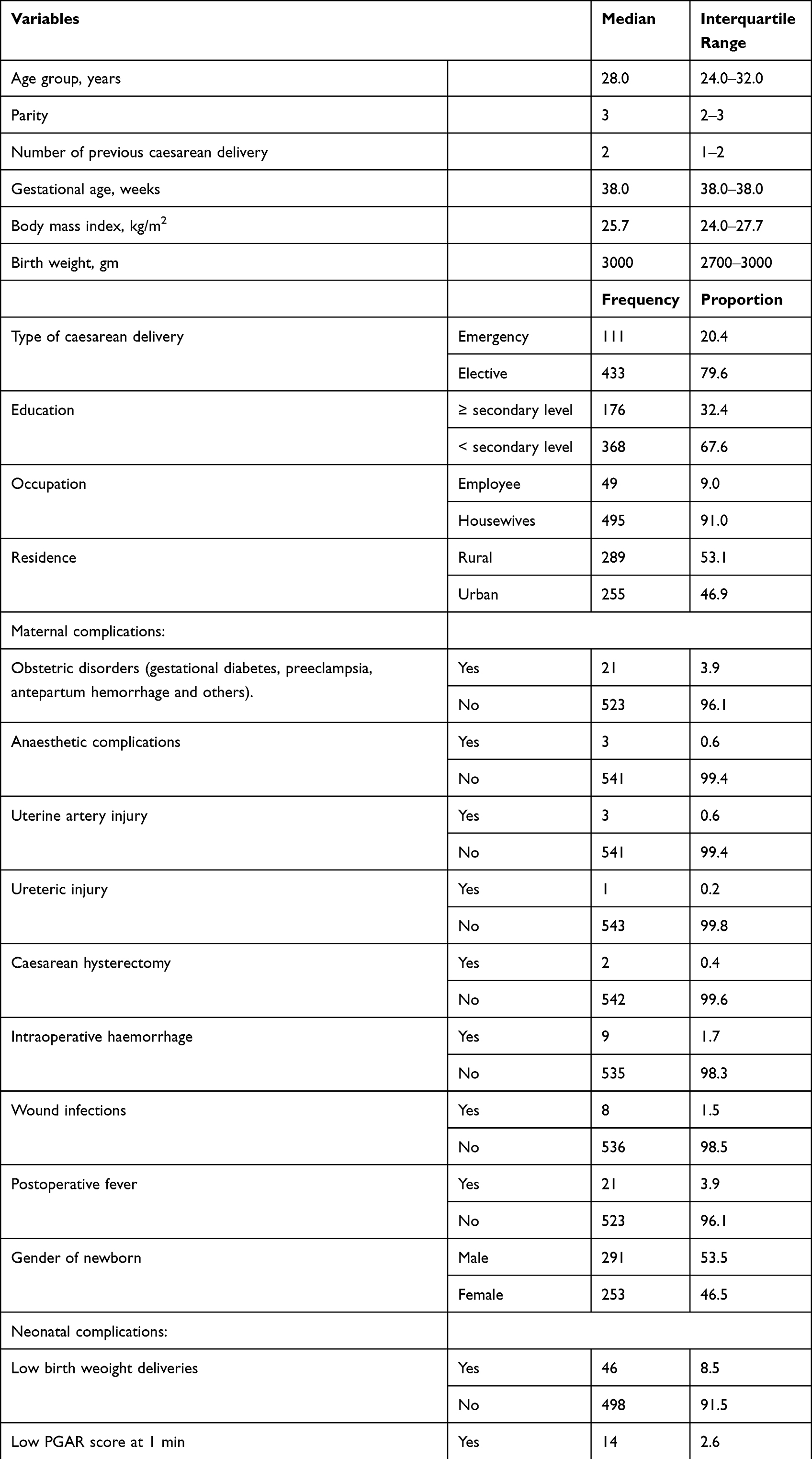 |
Table 1 Maternal and Neonatal Characteristics Women Who Had Caesarean Delivery in Eastern Sudan, 2020 |
Sixty-eight (12.5%) of these women had maternal complications. There were obstetric disorders (21, 3.9%), anaesthetic complications (3, 0.6%), uterine artery injury (3, 0.6%), ureteric injury (1, 0.2%), caesarean hysterectomy (2, 0.4%), intraoperative haemorrhage (9, 1.7%), wound infections (8, 1.5%) and postoperative fever (21, 3.9%). Only 8.8% of these women had two or more complications. There was no case of endometritis. There was no maternal death (Table 1).
Of these 544 CD patients, 76 (14.0%) had neonatal complications. These were LBW deliveries (46, 8.5%), low PGAR score at 1 min (14, 2.6%), low PGAR score at 5 min (2, 0.4%), admission to NICU (29, 5.3%) and neonatal death (7, 1.3%). Less than one-third (28.9%) had two or more neonatal complications (Table 1).
The LoS range was 1–9 days (mean = 2.7 days), its median (IRQ) was 3.0 (2‒3) days, and the 90th percentile was three days. Of these 544 women, 227 (41.7%) were discharged in less or equal to two days, 286 (52.6%) were discharged on the third day and 31 (5.7%) were discharged on four or more days. Out of 433 women who underwent elective CD, 204 (47.1%) were discharged in less or equal to two days, 213 (49.2%) were discharged on the third day and 16 (3.7%) were discharged on four or more days. Of 111 mothers who had emergency CD, 22 (19.8%) were discharged in less or equal to two days, 73 (65.8%) were discharged on the third day and 16 (14.4%) were discharged on four or more days (Figure 1).
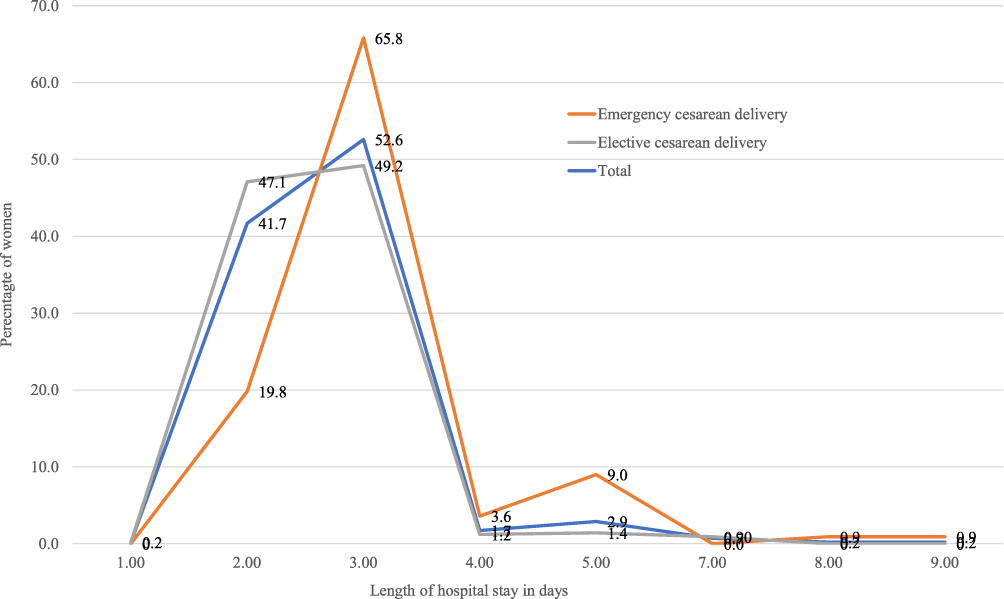 |
Figure 1 Comparing proportion of women between emergency and elective cesarean delivery and length of hospital stay. |
There were significant positive correlations related to age, BMI and LoS. There was a significant negative correlation between postoperative haemoglobin and LoS. There was no significant correlation between parity, gestational age and LoS. The median (IQR) of the LoS was significantly higher in women who had emergency CD (n = 111) vs elective CD (n = 433) [3 (3.0‒3.0) days vs. 3 (2.0‒3.0) days, P < 0.001], women with maternal complications (n = 68) vs women who had no maternal complications (n = 476) [3 (2.0‒3.0) days vs 3 (2.0‒3.0) days, P < 0.001] and in women who had neonatal complications (n = 67) vs women who did not had neonatal complications (n = 67) [3 (30.0 ‒3.75) days vs 3 (2.0‒3.0) days, P < 0.001]. LoS was not significantly different regarding residence, occupation and education (Table 2).
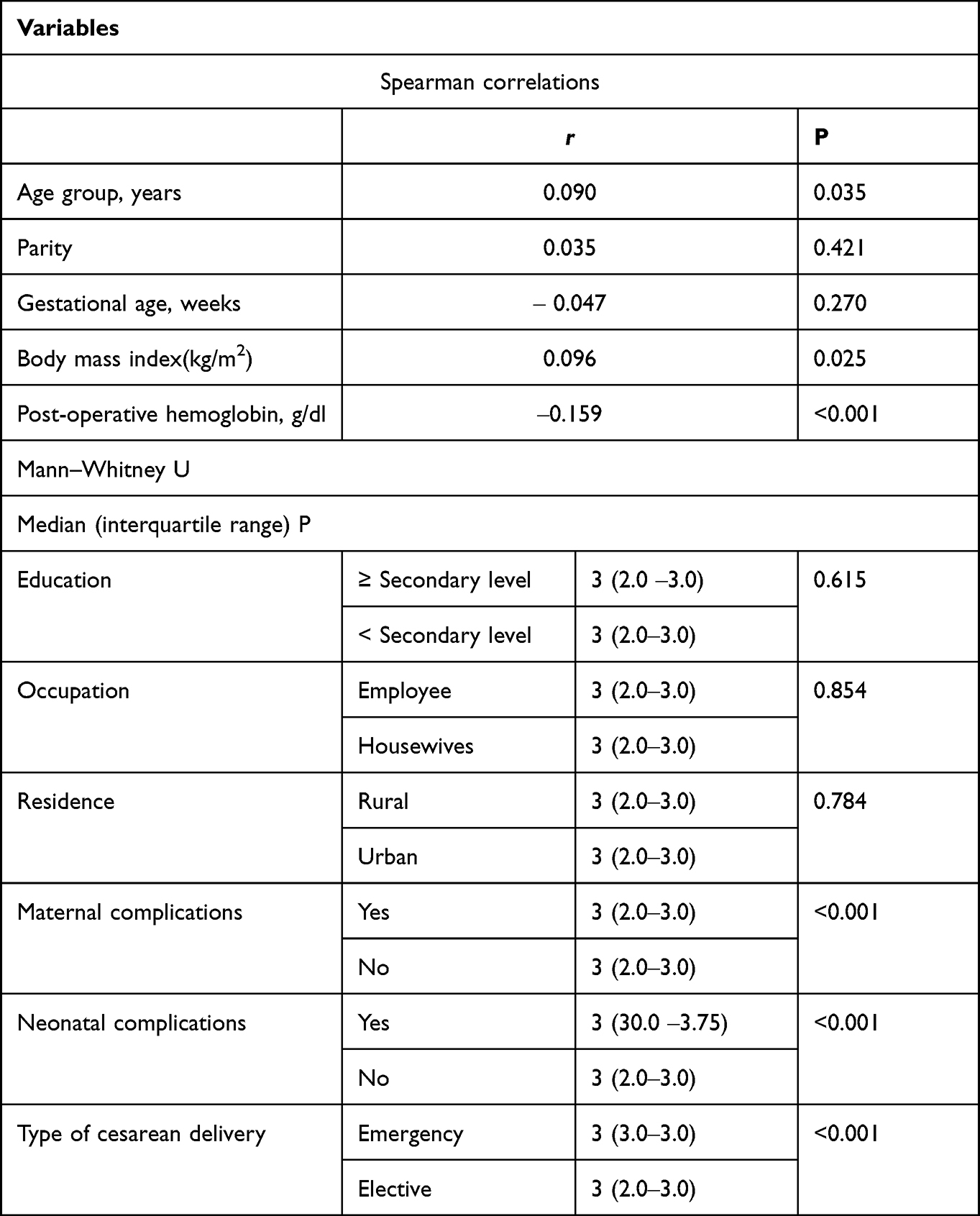 |
Table 2 Univariate Analysis of the Factors Associated with Length of Stay Post-Cesarean Delivery in Eastern Sudan |
Women with emergency CD stayed 13.0% longer than women with elective CD (RR = 1.13, 95% CI = 1.01–1.29) according to Poisson regression. Women with maternal complications stayed 24.0% longer than women with no maternal complications (RR = 1.24, 95% CI = 1.07–1.43). Women with neonatal complications stayed 21.0% longer than women without neonatal complications (RR = 1.21, 95% CI = 1.05–1.40). Age, parity, residence, education, occupation and postoperative haemoglobin were not associated with LoS (Table 3).
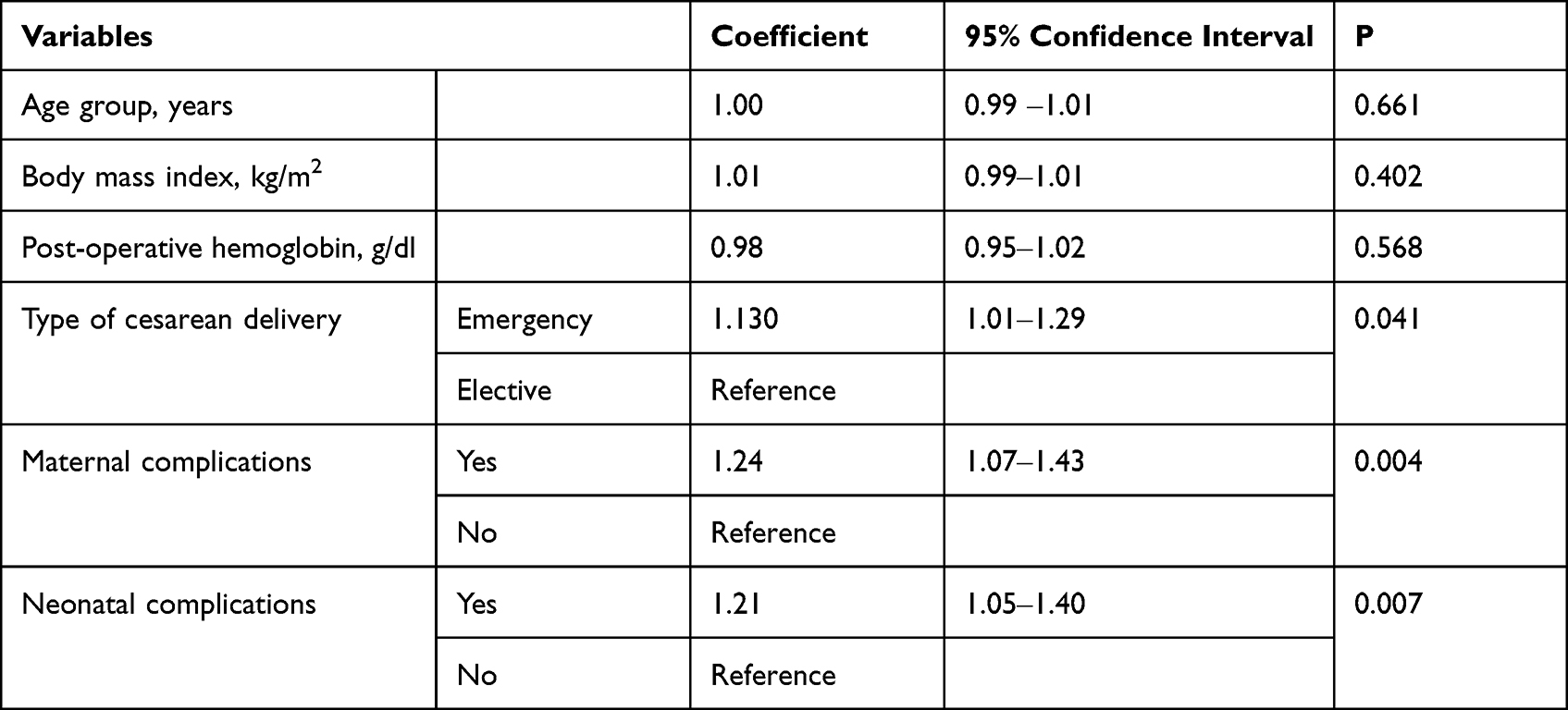 |
Table 3 Poisson Regression Analysis of the Factors Associated with Length of Stay Post-Cesarean Delivery in Eastern Sudan, 2020 |
Discussion
The main findings of the current study were that the mean LoS was 2.7 days and LoS was longer in women with emergency CD and in women with maternal and neonatal complications. In our study, the mean LoS was 2.7 days. Such findings are in agreement with a previous report in which the mean LoS was 2.71 days in California.19 Moreover, it has previously been documented that the LoS following CD has large variability (2.5–9.3 days) in 92 low- to middle-income countries.4 On the other hand, the mean (2.7 days) LoS following CD in our study was shorter than the mean (6.21 days) LoS following CD documented in a population-based cohort of 6632 women who gave birth in Brisbane, Australia.11 Acharya observed that the mean LoS was seven days in Nepal.20 Kumar et al recently reported that women had a mean LoS of 8.6 days following CD in India.5 Recently, Federspiel et al reported that in 456,312 patients with uncomplicated CD from 1535 hospitals, few (1.8%) patients stayed less than two days following CD or more than four days (1.2%). Most patients stayed two days (39.1%), three days (46.4%) or four days (11.5%).9 As mentioned above, this is the first data collection on the LoS in Sub-Saharan Africa. Therefore, our results should be compared with the results of later studies with caution. There are many differences in the settings; for example, some of these data are from public and private hospitals.5 Women admitted to public hospitals stay longer following CD than those admitted to private health facilities.5
Moreover, we investigated the LoS in elective and emergency CD, whereas the LoS in uncomplicated CD was documented in a previous study.9 Several factors, such as cost, insurance status, readmission and hospital distance, must be considered when dealing with LoS. Our findings may be a valuable guide for assessing LoS in VD and several other surgical procedures. It is worth mentioning that Bayoumi et al, in Egypt have reported that maternal hospital readmissions were not different if women were discharged at one day or three days following CD.21
The direct effect of maternal complications on LoS was observed in our results and the results of several prior studies.5,9,11,22 Perinatal complications, such as LBW, were associated with a longer LoS in our study. A similar finding was reported in a previous Italian study.12 The mothers of neonates with complications stayed on additional days to breastfeed their babies, explaining why they had a longer LoS. Women with emergency CD stayed 13.0% longer than women with elective CD in this study, [3 (3.0‒3.0) days vs. 3 (2.0‒3.0) days, P < 0.001], similarly to a previous study.9 The emergency CD is associated with more maternal complications and, hence, longer hospitalisation, as observed from a study published in Sudan.23 Thus, elective CD should be encouraged to shift the practice towards elective operations.
Furthermore, more actions are needed to minimise maternal and perinatal complications and shorten LoS. One of the factors that might shift CD towards elective ones and reduce maternal and perinatal complications is antenatal care. We did not assess antenatal care in this study. However, an inadequate level of antenatal care was observed in eastern Sudan.24 We did not observe a significant association among age, parity, BMI, residence, education and LoS. Age, parity, residence, education and obesity were shown to be associated with LoS in previous studies.5,11
Conclusion
In this study, the mean LoS was 2.7 days and women with emergency CD and maternal and neonatal complications had longer LoS.
Abbreviations
CD, caesarean delivery; VD, vaginal delivery; Los, length of stay; GMH, Gadarif Maternity Hospital; BMI, body mass index; LBW, low birth weight; NICU, neonatal intensive care unit; CI, confidence interval; IQR, interquartile range; AOR, adjusted odds ratios.
Ethics Approval and Informed Consent
Ethics approval was obtained from the Ethics Committee of the Faculty of Medicine of Gadarif University, Sudan (Reference number #2020.05). Written informed consent was collected from each participant. This study complies with Declaration of Helsinki.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Disclosure
All authors declare no conflicts of interest in this work.
References
1. Caesarean section rates continue to rise, amid growing inequalities in access (World Health Organization). Available from: https://www.who.int/news/item/16-06-2021-.
2. Waniala I, Nakiseka S, Nambi W, et al. Prevalence, indications, and community perceptions of caesarean section delivery in Ngora District, Eastern Uganda: mixed method study. Obstet Gynecol Int. 2020;2020:5036260. doi:10.1155/2020/5036260
3. Mascarello KC, Horta BL, Silveira MF. Maternal complications and cesarean section without indication: systematic review and meta-analysis. Rev Saude Publica. 2017;51:105. doi:10.11606/S1518-8787.2017051000389
4. Campbell OMR, Cegolon L, Macleod D, Benova L. Length of stay after childbirth in 92 countries and associated factors in 30 low- and middle-income countries: compilation of reported data and a cross-sectional analysis from nationally representative surveys. PLoS Med. 2016;13:e100197. doi:10.1371/journal.pmed.1001972
5. Kumar P, Dhillon P. Length of stay after childbirth in India: a comparative study of public and private health institutions. BMC Pregnancy Childbirth. 2020;20(1):1–13. doi:10.1186/s12884-020-2839-9
6. Bowers J, Cheyne H, Panda P, Dror D, Bedi A. Reducing the length of postnatal hospital stay: implications for cost and quality of care. BMC Health Serv Res. 2016;16:1–2. doi:10.1186/s12913-015-1214-4
7. Ghaffari P, Vanda R, Aramesh S, Jamali L, Bazarganipour F, Ghatee MA. Hospital discharge on the first compared with the second day after a planned cesarean delivery had equivalent maternal postpartum outcomes: a randomized single-blind controlled clinical trial. BMC Pregnancy Childbirth. 2021;21:1–6. doi:10.1186/s12884-021-03873-8
8. Tesfaye WY, Worku BT. Early postnatal discharge during COVID-19: a cross-sectional study. Women's Heal. 2021;17:17455065211042177. doi:10.1177/17455065211042177
9. Federspiel JJ, Suresh SC, Darwin KC, Szymanski LM. Hospitalization duration following uncomplicated cesarean delivery: predictors, facility variation, and outcomes. AJP Rep. 2020;10(2):E187–E197. doi:10.1055/s-0040-1709681
10. Cegolon L, Mastrangelo G, Campbell OM, et al. Length of stay following cesarean sections: a population based study in the Friuli Venezia Giulia region (North-Eastern Italy), 2005-2015. PLoS One. 2019;14(2):e0210753. doi:10.1371/journal.pone.0210753
11. Mamun AA, Callaway LK, O’Callaghan MJ, et al. Associations of maternal pre-pregnancy obesity and excess pregnancy weight gains with adverse pregnancy outcomes and length of hospital stay. BMC Pregnancy Childbirth. 2011;11(1):62. doi:10.1186/1471-2393-11-62
12. Rakita A, Nikolić N, Mildner M, et al. Re-epithelialization and immune cell behaviour in an ex vivo human skin model. Sci Rep. 2020;10(1):1–26. doi:10.1038/s41598-019-56847-4
13. Blumenfeld YJ, El-Sayed YY, Lyell DJ, Nelson LM, Butwick AJ. Risk factors for prolonged postpartum length of stay following cesarean delivery. Am J Perinatol. 2015;32(9):825–832. doi:10.1055/s-0034-1543953
14. Abbaker AO, Abdullahi H, Rayis DA, Imam AM, Adam I. An epidemic of cesarean deliveries at Khartoum hospital in Sudan with over two- fifths of neonates delivered through the abdomen. J Women's Health Issues Care. 2013;2:6. doi:10.4172/2325-9795.100012
15. UNICEF. Low birthweight: Country, regional and global estimates - UNICEF DATA. Available from: https://data.unicef.org/resources/low-birthweight-country-regional-and-global-estimates/.
16. Oyeyemi N, Oyeneyin L, Oluwole A, Oyeyemi A, Afolabi B. Post-operative management in uncomplicated caesarean delivery: a randomised trial of short-stay versus traditional protocol at the Lagos University Teaching Hospital, Nigeria. Niger Postgrad Med J. 2019;26(1):31–37. doi:10.4103/npmj.npmj_166_18
17. Kaur TP, Rathore AM, Sahu L. Efficacy of betadine vaginal toileting before caesarean section in postoperative infections. Int J Reprod Contraception Obstet Gynecol. 2020;9(6):2457. doi:10.18203/2320-1770.ijrcog20202329
18. Bujang MABN, Baharum N. Bujang: sample size estimation-correlation. World J Soc Sci Res. 2016;3(1):37–46. doi:10.22158/wjssr.v3n1p37
19. Leung KM, Elashoff RM, Rees KS, Hasan MM, Legorreta AP. Hospital- and patient-related characteristics determining maternity length of stay: a hierarchical linear model approach. Am J Public Health. 1998;88(3):377–381. doi:10.2105/AJPH.88.3.377
20. Acharya J. Are free maternity services completely free of costs? Osong Public Heal Res Perspect. 2016;7(1):26–31. doi:10.1016/J.PHRP.2015.11.002
21. Bayoumi YA, Bassiouny YA, Hassan AA, Gouda HM, Zaki SS, Abdelrazek AA. Is there a difference in the maternal and neonatal outcomes between patients discharged after 24 h versus 72 h following cesarean section? A prospective randomized observational study on 2998 patients. J Matern Fetal Neonatal Med. 2016;29(8):1339–1343. doi:10.3109/14767058.2015.1048678
22. Lee AH, Ng ASK, Yau KKW. Determinants of maternity length of stay: a gamma mixture risk-adjusted model. Health Care Manag Sci. 2001;4(4):249–255. doi:10.1023/A:
23. Fazari AB, Eldeen NS, Mohammed W, Muror M, Gailii E. Re-Laparotomy after caesarean section at Omdurman Maternity Hospital-Khartoum, Sudan. Open J Obstet Gynecol. 2015;05(08):448–454. doi:10.4236/ojog.2015.58065
24. Ali AAA, Osman MM, Abaker AO, Adam I. Use of antenatal care services in Kassala, eastern Sudan. BMC Pregnancy Childbirth. 2010;10. doi:10.1186/1471-2393-10-67
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.