")
Back to Journals » International Journal of Chronic Obstructive Pulmonary Disease » Volume 12
“What are my chances of developing COPD if one of my parents has the disease?” A systematic review and meta-analysis of prevalence of co-occurrence of COPD diagnosis in parents and offspring
Authors Li LSK , Paquet C, Johnston K , Williams MT
Received 5 October 2016
Accepted for publication 12 December 2016
Published 24 January 2017 Volume 2017:12 Pages 403—415
DOI https://doi.org/10.2147/COPD.S123933
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Richard Russell
Lok Sze Katrina Li,1 Catherine Paquet,2 Kylie Johnston,1 Marie T Williams3
1School of Health Sciences, Sansom Institute for Health Research, University of South Australia, Adelaide, South Australia, 2Center for Population Health Research, Sansom Institute for Health Research, University of South Australia, Adelaide, South Australia, 3Alliance for Research in Exercise, Nutrition and Activity (ARENA), Sansom Institute for Health Research, University of South Australia, Adelaide, South Australia, Australia
Introduction: Intergenerational associations in chronic obstructive pulmonary disease (COPD) have been well recognized and may result from genetic, gene environment, or exposure to life course factors. Consequently, adult offspring of parents with COPD may be at a greater risk of developing COPD. The aim of this study was to review the prevalence of co-occurrence of COPD in adult offspring with one or both parents having COPD independent of specific genetic variations.
Methods: In total, five databases were searched for original studies in which prevalence of COPD was reported in both offspring (children) and one or both parents. Studies were excluded if COPD was not clearly defined, COPD was linked to specific genetic variations, COPD was combined with other chronic respiratory conditions, or estimates included other first-degree relatives. Data extraction (ie, sample characteristics, prevalence of COPD, and odds ratio [OR] if reported) was completed by two independent reviewers. A meta-analysis of prevalence and OR was conducted, where possible.
Results: Of the 3,382 citations, 129 full texts were reviewed to include eight studies (six case–control, one cross-sectional, and one cohort) reflecting either prevalence of COPD in offspring of parents with COPD (descendent approach, n=3), which ranged from 0% to 17.3%, or prevalence of people with COPD reporting positive parental history of COPD (antecedent approach, n=5), for which the pooled prevalence was 28.6%. Offspring of people with COPD had 1.57 times greater odds (95% confidence interval =1.29–1.93; P<0.001) of having COPD compared with people not having a parental history of COPD.
Conclusion: The prevalence of COPD in adult offspring of people with COPD is greater than population-based estimates, and the ORs indicate a higher risk in this group. This offers clinicians a potential strategy for opportunistic screening, early identification, and intervention in this at-risk group.
Keywords: COPD, intergenerational, prevalence, systematic review
Introduction
Chronic obstructive pulmonary disease (COPD) is a common condition and is estimated to become the third leading cause of death by 2030.1,2 Globally, the prevalence of COPD has been estimated to be between 9% and 10%.3 Although COPD is a progressive disease, early intervention strategies such as optimizing medication, exercise, and pulmonary rehabilitation have been shown to reduce the rate of disease progression and improve symptom control in people diagnosed with COPD.4–8 The high prevalence of undiagnosed COPD has been reported internationally.9,10 Underdiagnosis of COPD is problematic as symptoms of COPD may hinder an individual’s daily activities.11,12 Generalized population level screening for COPD is controversial and, currently, is not recommended for asymptomatic individuals as it is unclear whether early detection improves clinical outcomes.13 Individuals may, however, present asymptomatic because of modification in activities that trigger symptoms.14 Targeted case findings in the community and in primary care commonly focus on people with recognized COPD risk factors or exposures such as smokers and consider them as an at-risk population.15,16
Although cigarette smoking is a key risk factor for COPD development, not all COPD cases can be explained by smoking.17 Lifetime exposure to smoke or pollution has been shown to increase a person’s risk of developing COPD.18,19 In addition, early life factors such as low birth weight, prematurity, nutrition, childhood respiratory illness, and exposure to passive smoking are associated with reduced lung function in later life.20–24
Familial or intergenerational associations for chronic respiratory disease have been observed with an increased risk of chronic bronchitis in people with family members having bronchitis.25,26 Strong familial associations have been reported for increased respiratory symptoms or conditions including wheezing, asthma, and lung cancer among twins and individuals living in the same household.23,27–29 Currently, although alpha-1-antitrypsin deficiency is the only robustly defined inherited form of COPD that can explain familial aggregation of COPD,30 <3% of people with COPD have this deficiency.31 Intergenerational associations overlap with the risk factors associated with the development of COPD, including smoking behavior of parents and offspring, educational achievement, lung function, and conditions or diseases such as asthma and lung cancer.29,32–35 Concepts, knowledge, and behaviors about health can be transmitted from one generation to the next.36 Thus, offspring of people with COPD are considered as an at-risk group for the development of COPD, as they may be exposed to a greater number of these intergenerational factors that could trigger or have a cumulative effect that shapes the trajectory of lung health.37
Apart from studies that focus on associations between genetic forms of COPD, specific genes, and lung function in families,38,39 there seem to be little direct data concerning the likelihood or specific risk of COPD in offspring of parents with COPD. The odds of having COPD have been shown to be 1.7–2.7 times higher in people with family history of COPD (all first-degree relatives included) than in those without family history.40,41 Adult offspring of people with COPD might present with a different risk profile as they are more likely to cohabitate during formative early life periods. It is hypothesized that offspring of people with COPD through exposure to intergenerational and life course factors will have higher rates or an increased risk of COPD compared with people without a parental history of COPD. The overall aim of this systematic review was to collate the reported evidence for co-occurrence and risk of COPD, especially in adult offspring with one or both parents having COPD independent of specific genetic variations.
The following were the two objectives of this review:
- To report the prevalence of COPD in offspring of people with COPD and/or prevalence of a positive parental history of COPD in people with COPD.
- To report the strength of the association between parental and offspring COPD status.
Methods
This review was designed and reported according to the recommendations in the Preferred Reporting Items for Systematic Reviews and Meta-analysis guidelines, and the protocol was registered (PROSPERO no: CRD42015025228).42
Study selection
Electronic databases (ie, Medline, CINAHL, EMBASE, SCOPUS, and Cochrane Library) were systematically searched from inception to mid-September 2015. Search terms (Table 1) were adapted from previous systematic reviews on COPD and the effects of family history.5,8,23,29 Two researchers independently performed the systematic search following a prospectively planned search protocol that was developed with the aid of an academic librarian.
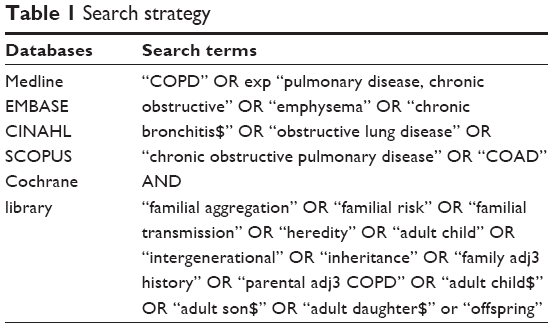 | Table 1 Search strategy |
Inclusion and exclusion criteria
Studies were included if data were reported or could be inferred for the prevalence of COPD, chronic bronchitis, and/or emphysema (through self-report, physician-diagnosed, spirometry-diagnosed, or symptom profile) in parents and adult offspring of people with COPD. No year or language limits were set for inclusion of studies in this review.
Studies were excluded: 1) if they did not define family history or specifically report offspring/parents within first-degree relative groups (due to possible inclusions of other family members such as siblings); 2) if they reported specific lung function parameters without a COPD classification definition; 3) if COPD, emphysema, or chronic bronchitis was combined with other respiratory conditions; 4) if data were limited to familial investigation of known genetic variations in COPD (alpha-1-antitrypsin deficiency); and 5) if studies were on participants from specific occupations/living environment (eg, coal miners, coke oven workers, and living close to asbestos factory).
Screening of studies
Two reviewers independently screened the titles and abstracts of citations returned from searches. Full texts of studies were reviewed by two independent reviewers for inclusion or exclusion. Reasons for excluding the studies were recorded, and discrepancies were discussed until consensus was reached. Reference lists of relevant articles were searched, and citation tracking was performed to retrieve any potential additional citations.
Data extraction and appraisal of methodological bias
By using a predetermined template (Table S1), two reviewers independently extracted data from the included studies with disagreements resolved by consensus. A ten-item methodological appraisal checklist for studies reporting prevalence data was used.43 Interpretations specific to the review questions (Table S2) were used by two independent reviewers; when consensus was not reached, then a third reviewer was consulted. No studies were excluded on the basis of the methodological bias.
Data analysis
Study design, participant characteristics, and the method of COPD diagnosis were descriptively reported. Studies were collated and analyzed separately: 1) studies that considered people with confirmed COPD and the prevalence of COPD in their offspring (descendent approach); and 2) studies that considered prevalence of positive parental history of COPD in people with confirmed COPD (antecedent approach). If odds ratios (ORs) were not reported in the study but sufficient data were provided, then the ORs were calculated. The prevalence and ORs were compiled from the reported statistics or calculated when sufficient information was provided, the pooled prevalence and OR were calculated, and forest plots were created by using MedCalc for Windows, Version 15.11.4 (MedCalc Software, Ostend, Belgium). I2 statistics were used to assess the heterogeneity of the studies. The random-effects model was used due to the high level of heterogeneity between the studies.
Results
Search results
One hundred and twenty-nine full-text articles were reviewed (including 18 non-English articles; Figure 1). Studies were excluded for two main reasons: first (51% of the excluded studies), despite reporting data for family history of COPD in people with COPD, studies either did not define family history as a parental history44,45 or reported a pooled analysis of family history that included various combinations of siblings, parents, offspring, and first-degree relatives.46,47 Second (33% of the excluded), studies reported on the prevalence of respiratory problems/symptoms or on measures of lung function in offspring of people with COPD without a reference to a COPD classification.48–50
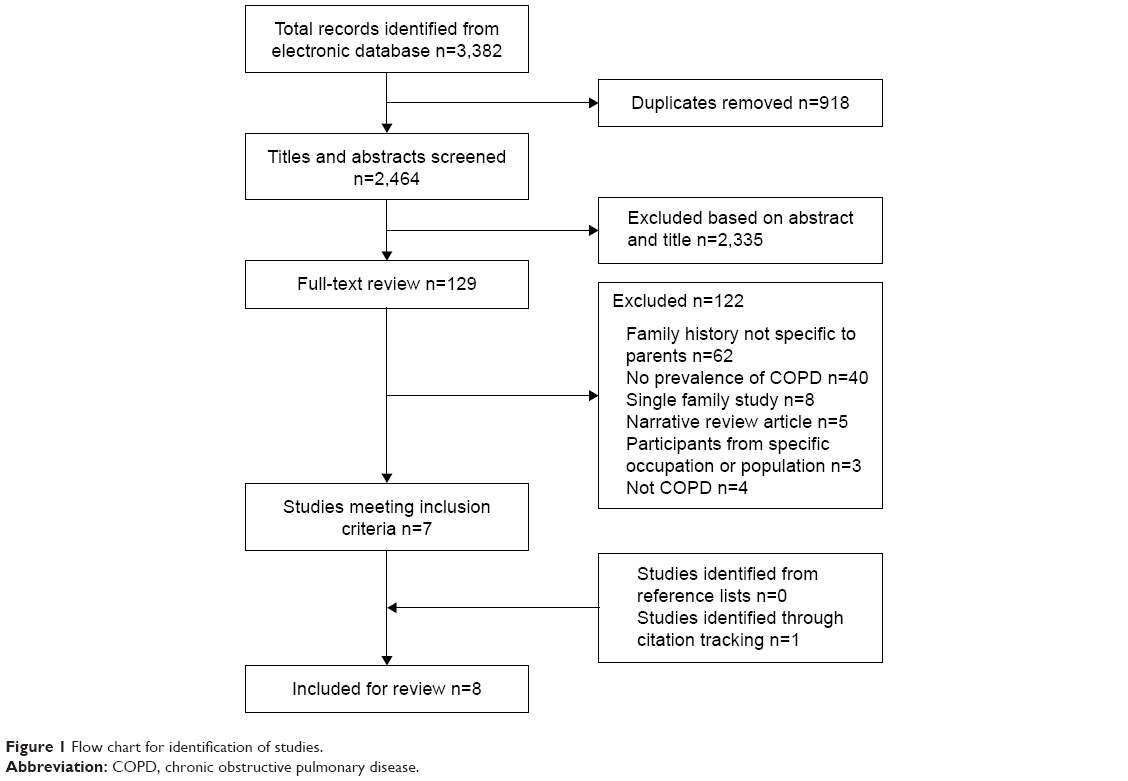 | Figure 1 Flow chart for identification of studies. |
Seven studies were included after full-text review, and one additional study was identified through citation tracking, resulting in a total of eight studies eligible for inclusion in this review.
Study characteristics
All the included studies were observational in design. Of the eight studies, three studies reported on the prevalence of COPD in offspring of people with COPD (descendent approach, Table 2), with a total of 204 cases and 161 controls in two case–control studies and 5,054 participants in a cross-sectional study,51–53 and five studies reported on the prevalence of a parental history of COPD in people with COPD (antecedent approach, Table 3), with 1,545 cases and 1,995 controls in four case–control studies and 80,214 participants in a cohort study.54–58 None of the studies included in this review were primarily designed as prevalence studies, and all the studies included had a variable risk of bias when appraised using the prevalence appraisal checklist (Table S2).43
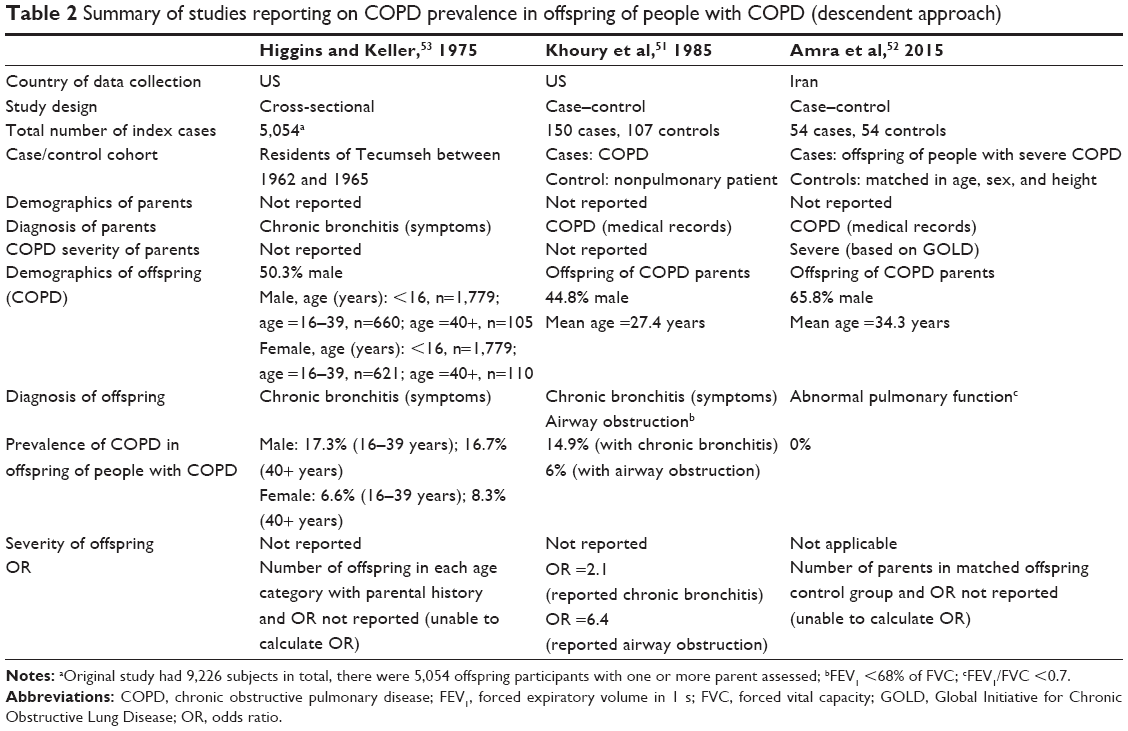 | Table 2 Summary of studies reporting on COPD prevalence in offspring of people with COPD (descendent approach) |
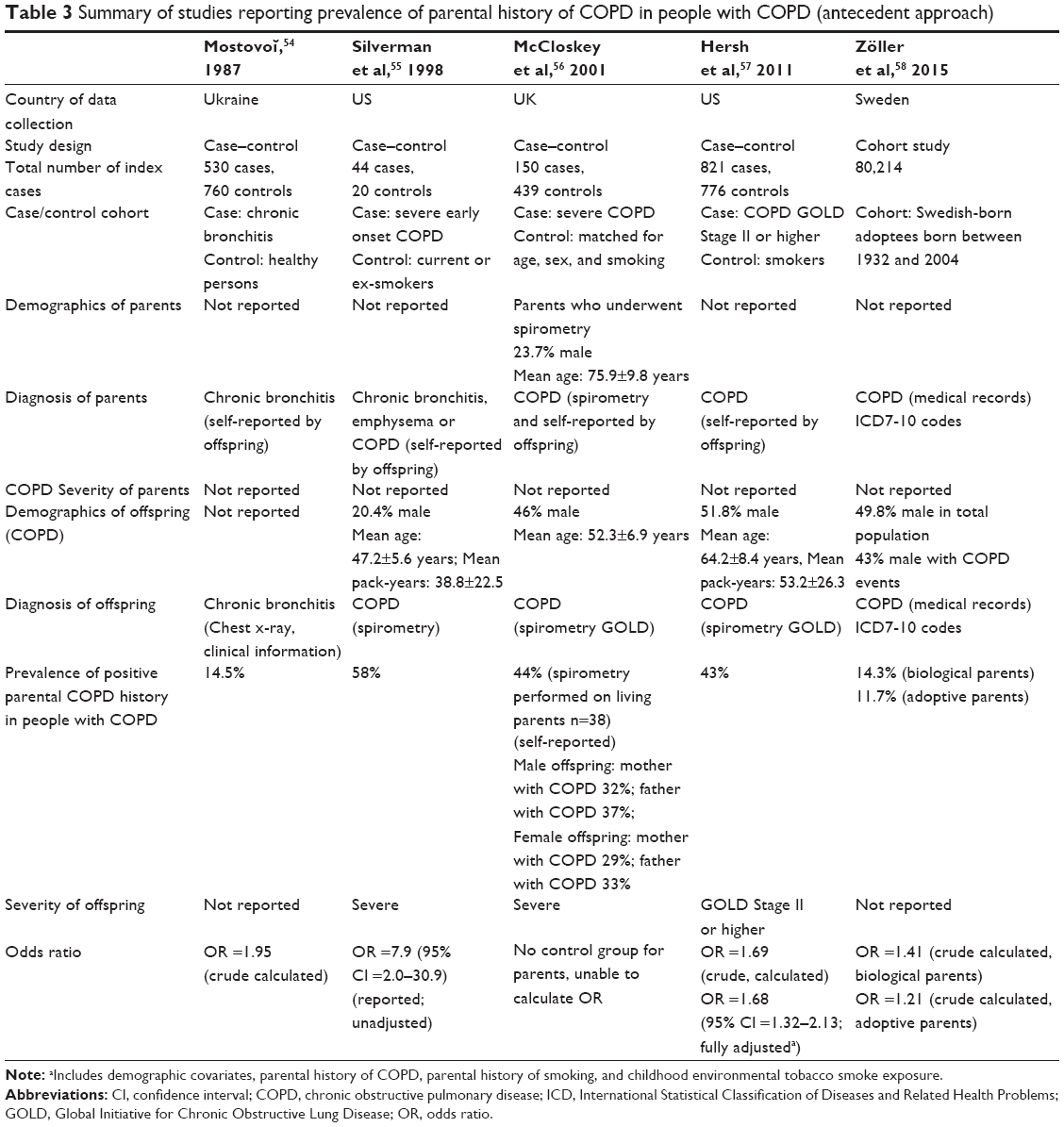 | Table 3 Summary of studies reporting prevalence of parental history of COPD in people with COPD (antecedent approach) |
Prevalence
The prevalence of COPD in offspring of one or more parents with a diagnosis of COPD ranged from 0% to 17.3% in studies that used a descendent approach (Table 2). Studies that used the antecedent approach reported prevalence estimates ranging from 11.7% to 58% in people with COPD with a parental history of COPD (Table 3).
Pooled prevalence estimate
A pooled prevalence of COPD in offspring of people with COPD could not be calculated across the three studies that employed the descendent approach (Table 2), as one study reported prevalence of COPD in offspring for different age groups and a second study essentially excluded offspring with respiratory conditions.52,53
The calculated pooled prevalence of people with COPD with a positive parental history of COPD (antecedent approach) was 28.6% (random-effects model, 95% confidence interval [CI] =17.4–41.3; Table 3, Figure 2). One study provided prevalence of COPD in both biological and adoptive parents of people with COPD (both included in the pooled prevalence calculation).58 Evidence of heterogeneity between the studies was found (I2=98.8%; P<0.0001). A study by Silverman et al (1998) included a specific group of participants (severe early-onset COPD).55 When excluding Silverman et al (1998), the prevalence of people with COPD with a positive parental history of COPD was 24.0% (random-effects model, 95% CI =13.2–36.8; I2=99.0%; P<0.0001).55
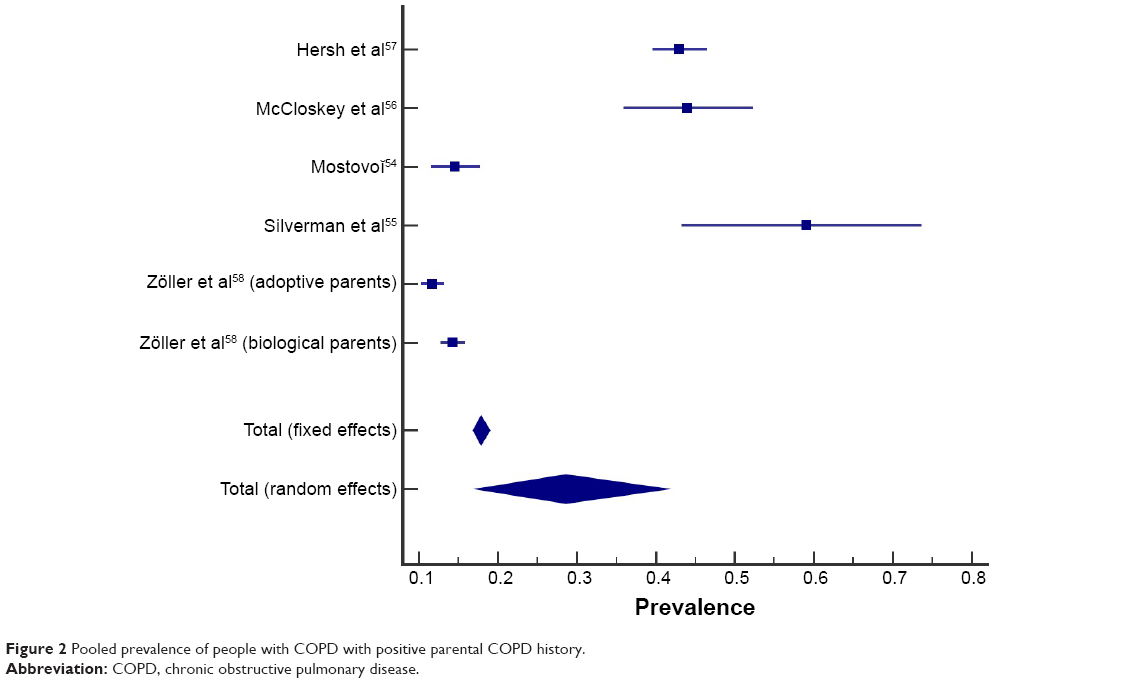 | Figure 2 Pooled prevalence of people with COPD with positive parental COPD history. |
Pooled OR
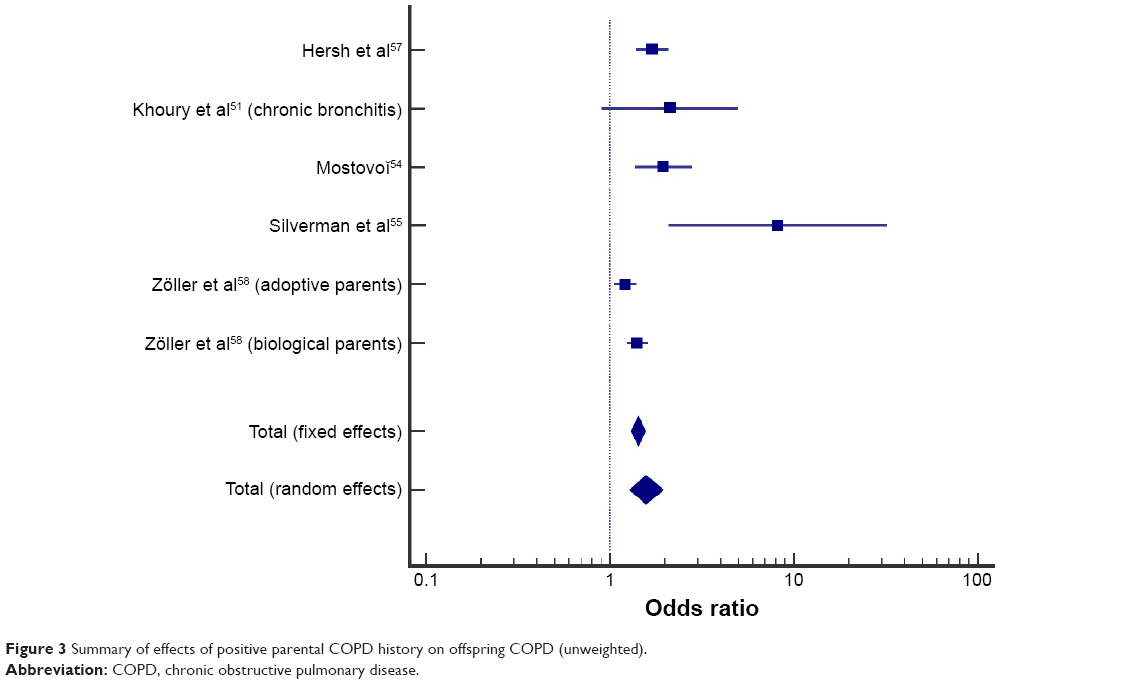
Of the eight included studies, three studies reported an OR (of the increased likelihood of offspring of people with COPD to develop COPD),51,55,57 two studies reported enough information to calculate comparable ORs,54,58 and three studies did not provide sufficient information for OR calculation.52,53,56 A study by Khoury et al reported the prevalence of chronic bronchitis and airway obstruction in the offspring of people with COPD.51 However, this study defined airway obstruction (forced expiratory volume in 1 s [FEV1]/forced vital capacity [FVC] <68%) differently from the conventional ratio used for COPD diagnosis (FEV1/FVC <70%).1 To maintain consistency across diagnosis methods through the studies, only the data on chronic bronchitis from the study by Khoury et al were used in the pooled analysis.51
Meta-analysis of crude OR from five studies indicated that offspring of people with COPD had 57% higher odds of having COPD compared with people without a parental history of COPD (random-effects model, pooled OR =1.57; 95% CI =1.29–1.93; P<0.001; Figure 3). Evidence of heterogeneity between studies was found (I2=72%; P=0.0029). When the study by Silverman et al (in severe early-onset COPD) was excluded from the pooled analysis,55 the heterogeneity decreased (I2=66%; P=0.0198), and offspring of people with COPD had 50% higher odds of having COPD compared with people without a parental history of COPD (random-effects model, pooled OR =1.50; 95% CI =1.26–1.77).
 | Figure 3 Summary of effects of positive parental COPD history on offspring COPD (unweighted). |
Discussion
This review specifically focused on the co-occurrence of COPD in parents and offspring. The pooled prevalence of people with COPD and a positive parental history of COPD was 28.6%, and offspring of people with COPD had 1.57 times greater odds of having COPD compared with people without a parental history of COPD. Although there is evidence to support familial associations in lung function decline in parent and offspring pairs,59 this review identified a paucity of studies (especially recent publications) that provided or enabled an estimate of the prevalence of COPD, especially in offspring of people with COPD, to be obtained.
Due to the inconsistencies in the definition of family history and reporting of outcome measures, only a small number of studies met the inclusion criteria of this review. Lower values for pulmonary function in offspring of COPD probands compared with reference or non-COPD probands have been reported,49,60,61 but in the absence of categorizing offspring with or without COPD or sufficient information to calculate COPD prevalence within offspring, these studies were excluded.
Variation in the original intent of the included studies resulted in differences in study design, source and nature of participants, and classification of COPD. Index cases in the case–control studies varied from people with chronic bronchitis to people with severe early-onset COPD,54,55 whereas index cases in the control groups varied from matched individuals to smokers.52,57 Apart from two older studies (published in 1975 and 1987), all other studies employed spirometry to classify COPD in offspring;53,54 only one study directly assessed both parents and offspring with spirometry.56 Parental COPD history was self-reported by participants in all but one of the antecedent studies,54–57 with the remaining study using medical records to identify COPD in parents and offspring.58 High prevalence of undiagnosed COPD has been reported worldwide;10,62 thus, identifying COPD by self-report or medical record screening may be an underestimation and not reveal the true prevalence of positive parental COPD history.11,59
Three of the eight studies used a descendent approach and reported a wide range of COPD prevalence (0%–17.3%) in offspring of people with COPD.51–53 Amra et al represent an outlier within this group as none of the offspring (n=54) met spirometric criteria for COPD (FEV1/FVC <0.7).52 However, young mean age of offspring (34.3 years) and exclusion criteria applied to offspring cases (smokers, employed in high-risk jobs for the respiratory system, or had a pulmonary disease) biased the case group toward including only those with lower risk profile for COPD. The other two studies reported prevalence ranging between 6% and 17.3% which was higher than contemporaneous published prevalence estimates of COPD in the general population for a comparable age-group (4% in 25–44 years).51,53,63
Across five studies that used the antecedent approach, between 11.7% and 58.0% of people with COPD reported a positive parental history.54–58 No comparable reviews or population-based data were found to compare these estimates of parental history of COPD; however, this prevalence appears high when compared to the estimate of prevalence of COPD in the general population (9%–10%).3 Studies that recruited participants with moderate-to-severe COPD reported a relatively higher positive parental history of COPD (43%–58%) and alluded that the increased risk of COPD in families was likely to be the result of genetic factors.55–57 Although there are ongoing studies on genome-wide association exploring genotypes of COPD, there remain unanswered questions on COPD heritability and susceptibility.64 Another possible explanation for the higher prevalence of positive parental COPD history reported by participants with more severe COPD may be an increased awareness of respiratory problems in their immediate family and greater vigilance or likelihood of reporting.65
The risk of developing COPD in people with a parental history of COPD (OR =1.57) was comparable to those exposed to passive smoking (OR =1.48), maternal smoking (OR =1.7), and childhood pneumonia (OR =1.4) and lower compared with the effects of personal smoking in the development of COPD (OR =6.3).18,66–68 Further epidemiological studies are required to promote understanding of the mechanism of interactions between various risk factors and differentiate shared lifestyle factors from true genetic risk in parents with COPD and their adult offspring.
Early identification of those at a risk of developing COPD is commonly based on modifiable behavior such as smoking or symptom profiles. Smokers are a common target population in COPD case-finding studies as smoking cessation is a well-recognized early intervention that slows the progression of the disease.16,69,70 As universal screening of asymptomatic individuals for COPD is not recommended,13 offspring of people with COPD may be considered as an at-risk group due to their shared genetic and environment factors, which presents an opportunity for case finding. By capitalizing on the increased prevalence and the risk of developing COPD in adult offspring of people with confirmed COPD, health practitioners working with people with COPD could use opportunistic screening of adult offspring to enable early lifestyle intervention strategies such as smoking cessation, physical activity, appropriate pharmacologic support, and pulmonary rehabilitation to reduce the rate of lung function decline, improve symptom control, and improve quality of life.7,71,72
Limitations
This review included studies that were published over a 40-year period (1975–2015). The two oldest studies included in this review reported on the prevalence of COPD in offspring of people with COPD, and unsurprisingly the diagnostic criteria used differed from the current standard.1,51,53 Diagnostic criteria and terminology for COPD have changed over time.73 As no time limit was set for the systematic search strategy, studies were eligible for inclusion in this review if participants were classified as having emphysema, chronic bronchitis, or COPD. The prevalence of co-occurrence of COPD reported in this review may differ from the present day due to changes in the definition of COPD, lifestyle, and increased education and health promotion on the health consequences of smoking.74
A critical appraisal checklist for studies reporting on prevalence data was used even though the included studies were not specifically designed to report prevalence.43 As no studies were excluded from the review, modifications were required to adapt the checklist to determine the representativeness of the study sample and interpretation of the results specific to the review question.
Meta-analysis was performed despite significant heterogeneity among the studies. The pooled prevalence and OR calculated provided a summary of the available evidence but may not be generalizable due to the heterogeneity and limited populations of the included studies.
Conclusion
Although familial associations with COPD have been generally well recognized, the results of this review indicate that there were few studies that specifically reported on the co-occurrence of COPD diagnosis in both parents and offspring. Nevertheless, the findings of this review indicate that offspring of people with COPD are at an increased risk of developing COPD. Targeted screening in this at-risk group (adult offspring of people with COPD) may lead to opportunities to capitalize on familial links and promote early identification and intervention.
Acknowledgment
This systematic review abstract was presented at the Thoracic Society of Australia and New Zealand Annual Scientific Meeting (April 1–5, 2016) in Perth, Australia (poster). This project received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Author contributions
All the authors (LSKL, CP, KJ, and MTW) contributed substantially to the study design, data collection, data analysis and interpretation, and the writing and critical revision of the manuscript.
Disclosure
The authors report no conflicts of interest in this work.
References
Global Initiative for Chronic Obstructive Lung Disease. Pocket Guide to COPD Diagnosis, Management and Prevention 2015; 2015. Available from: http://www.goldcopd.org/uploads/users/files/GOLD_Pocket_2015_Feb18.pdf. Accessed March 25, 2015. | ||
World Health Organization. World Health Statistics: 2008; 2008. Available from: http://www.who.int/gho/publications/world_health_statistics/EN_WHS08_Full.pdf. Accessed March 30, 2015. | ||
Halbert R, Natoli J, Gano A, Badamgarav E, Buist A, Mannino DM. Global burden of COPD: systematic review and meta-analysis. Eur Respir J. 2006;28(3):523–532. | ||
Abramson M, Crockett AJ, Dabscheck E, et al. The COPDX Plan: Australian and New Zealand Guidelines for the Management of Chronic Obstructive Pulmonary Disease 2014; 2014. Available from: http://2014-new.copdx.org.au/wp-content/uploads/2011/08/COPDX-V2.39-October-2014_FINAL.pdf. Accessed July 23, 2015. | ||
Ngai SP, Jones AY, Tam W. Tai Chi for chronic obstructive pulmonary disease (COPD). Cochrane Database Syst Rev. 2016;(7):CD009953. | ||
Welte T, Vogelmeier C, Papi A. COPD: early diagnosis and treatment to slow disease progression. Int J Clin Pract. 2015;69(3):336–349. | ||
McCarthy B, Casey D, Devane D, Murphy K, Murphy E, Lacasse Y. Pulmonary rehabilitation for chronic obstructive pulmonary disease. Cochrane Database Syst Rev. 2015;(2):CD003793. | ||
Maltais F, Dennis N, Chan CK. Rationale for earlier treatment in COPD: a systematic review of published literature in mild-to-moderate COPD. COPD. 2013;10(1):79–103. | ||
Toelle BG, Xuan W, Bird TE, et al. Respiratory symptoms and illness in older Australians: the Burden of Obstructive Lung Disease (BOLD) study. Med J Aust. 2013;198(3):144–148. | ||
Moreira GL, Manzano BM, Gazzotti MR, et al. PLATINO, a nine-year follow-up study of COPD in the city of São Paulo, Brazil: the problem of underdiagnosis. J Bras Pneumol. 2014;40(1):30–37. | ||
Seymour J, Spruit M, Hopkinson N, et al. The prevalence of quadriceps weakness in COPD and the relationship with disease severity. Eur Respir J. 2010;36(1):81–88. | ||
Kessler R, Partridge MR, Miravitlles M, et al. Symptom variability in patients with severe COPD: a pan-European cross-sectional study. Eur Respir J. 2011;37(2):264–272. | ||
Guirguis-Blake JM, Senger CA, Webber EM, Mularski RA, Whitlock EP. Screening for chronic obstructive pulmonary disease: evidence report and systematic review for the US Preventive Services Task Force. JAMA. 2016;315(13):1378–1393. | ||
Labaki WW, Martinez CH, Han MK. COPD in 2016: some answers, more questions. Lancet Respir Med. 2016;4(12):941–943. | ||
Sansores RH, Ramírez-Venegas A, Hernández-Zenteno R, et al. Prevalence and diagnosis of chronic obstructive pulmonary disease among smokers at risk. A comparative study of case-finding vs screening strategies. Respir Med. 2013;107(4):580–586. | ||
Stratelis G, Jakobsson P, Molstad S, Zetterstrom O. Early detection of COPD in primary care: screening by invitation of smokers aged 40 to 55 years. Br J Gen Pract. 2004;54(500):201–206. | ||
Eisner MD, Anthonisen N, Coultas D, et al. An official American Thoracic Society public policy statement: novel risk factors and the global burden of chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 2010;182(5):693–718. | ||
Yin P, Jiang C, Cheng K, et al. Passive smoking exposure and risk of COPD among adults in China: the Guangzhou Biobank Cohort Study. Lancet. 2007;370(9589):751–757. | ||
Hu G, Zhou Y, Tian J, et al. Risk of COPD from exposure to biomass smoke: a metaanalysis. Chest. 2010;138(1):20–31. | ||
Svanes C, Omenaas E, Jarvis D, Chinn S, Gulsvik A, Burney P. Parental smoking in childhood and adult obstructive lung disease: results from the European Community Respiratory Health Survey. Thorax. 2004;59(4):295–302. | ||
Kouzouna A, Gilchrist F, Ball V, et al. A systematic review of early life factors which adversely affect subsequent lung function. Paediatr Respir Rev. 2016;20:67–75. | ||
Edwards CA, Osman LM, Godden DJ, Douglas JG. Wheezy bronchitis in childhood: a distinct clinical entity with lifelong significance? Chest. 2003;124(1):18–24. | ||
Burke H, Leonardi-Bee J, Hashim A, et al. Prenatal and passive smoke exposure and incidence of asthma and wheeze: systematic review and meta-analysis. Pediatrics. 2012;129(4):735–744. | ||
Pike K, Pillow JJ, Lucas JS. Long term respiratory consequences of intrauterine growth restriction. Semin Fetal Neonatal Med. 2012;17(2): 92–98. | ||
Oswald N, Harold J, Martin W. Clinical pattern of chronic bronchitis. Lancet. 1953;262(6787):639–643. | ||
Ogilvie AG. Chronic bronchitis in Newcastle upon Tyne. J R Soc Promot Health. 1959;79(1):80–87. | ||
Tarnoki DL, Tarnoki A, Lazar Z, et al. A possible genetic influence in parenchyma and small airway changes in COPD: a pilot study of twins using HRCT. Acta Physiol Hung. 2014;101(2):167–175. | ||
Tager IB, Rosner B, Tishler PV, Speizer FE, Kass EH. Household Aggregation of Pulmonary Function and Chronic Bronchitis. Am Rev Respir Dis. 1976;114(3):485–492. | ||
Matakidou A, Eisen T, Houlston R. Systematic review of the relationship between family history and lung cancer risk. Br J Cancer. 2005;93(7):825–833. | ||
Castaldi PJ, Cho MH, Cohn M, et al. The COPD genetic association compendium: a comprehensive online database of COPD genetic associations. Hum Mol Genet. 2010;19(3):526–534. | ||
Ioachimescu OC, Stoller JK. A review of alpha-1 antitrypsin deficiency. COPD. 2005;2(2):263–275. | ||
Burke W, Fesinmeyer M, Reed K, Hampson L, Carlsten C. Family history as a predictor of asthma risk. Am J Prev Med. 2003;24(2):160–169. | ||
Palmer L, Knuiman M, Divitini M, et al. Familial aggregation and heritability of adult lung function: results from the Busselton Health Study. Eur Respir J. 2001;17(4):696–702. | ||
Dustmann C. Parental background, secondary school track choice, and wages. Oxf Econ Pap. 2004;56(2):209–230. | ||
Bailey SL, Ennett ST, Ringwalt CL. Potential mediators, moderators, or independent effects in the relationship between parents’ former and current cigarette use and their children’s cigarette use. Addic Behav. 1993;18(6):601–621. | ||
Taylor J, Price K, Braunack-Mayer A, Haren MT, Mcdermott R. Intergenerational learning about keeping health: a qualitative regional Australian study. Health Prom Int. 2014;29(2):361–368. | ||
Ben-Shlomo Y, Kuh D. A life course approach to chronic disease epidemiology: conceptual models, empirical challenges and interdisciplinary perspectives. Int J Epidemiol. 2002;31(2):285–293. | ||
Joost O, Wilk JB, Adrienne Cupples L, et al. Genetic loci influencing lung function: a genomewide scan in the Framingham study. Am J Respir Crit Care Med. 2002;165(6):795–799. | ||
Castaldi P, DeMeo D, Kent D, et al. Development of predictive models for airflow obstruction in alpha-1-antitrypsin deficiency. Am J Epidemiol. 2009;170(8):1005–1013. | ||
Nihlén U, Nyberg P, Montnémery P, Löfdahl C-G. Influence of family history and smoking habits on the incidence of self-reported physician’s diagnosis of COPD. Respir Med. 2004;98(3):263–270. | ||
Hooper R, Burney P, Vollmer WM, et al. Risk factors for COPD spirometrically defined from the lower limit of normal in the BOLD project. Eur Respir J. 2012;39(6):1343–1353. | ||
Liberati A, Altman DG, Tetzlaff J, et al. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: explanation and elaboration. Ann Intern Med. 2009;151(4):65–94. | ||
Munn Z, Moola S, Lisy K, Riitano D. The Joanna Briggs Institute Reviewers’ Manual 2014.The Systematic Review of Prevalence and Incidence Data. Adelaide, SA: The Joanna Briggs Institute; 2014. | ||
Pallasaho P, Kainu A, Sovijärvi A, Lindqvist A, Piirilä PL. Combined effect of smoking and occupational exposure to dusts, gases or fumes on the incidence of COPD. COPD. 2014;11(1):88–95. | ||
Özge A, Özge C, Kaleagasi H, Yalin OÖ, Ünal Ö, Özgür ES. Headache in patients with chronic obstructive pulmonary disease: effects of chronic hypoxaemia. J Headache Pain. 2006;7(1):37–43. | ||
Celedon J, Speizer F, Drazen J, et al. Bronchodilator responsiveness and serum total IgE levels in families of probands with severe early-onset COPD. Eur Respir J. 1999;14(5):1009–1014. | ||
Zhou Y, Wang C, Yao W, et al. COPD in Chinese nonsmokers. Eur Respir J. 2009;33(3):509–518. | ||
Lebowitz M, Holberg C, Martinez F. A longitudinal study of risk factors in asthma and chronic bronchitis in childhood. Eur J Epidemiol. 1990;6(4):341–347. | ||
Kawakami Y, Irie T, Kishi F, et al. Familial aggregation of abnormal ventilatory control and pulmonary function in chronic obstructive pulmonary disease. Eur J Respir Dis. 1981;62(1):56–64. | ||
Hansen J, Gao W, Dupuis J, et al. Association of 25-hydroxyvitamin D status and genetic variation in the vitamin D metabolic pathway with FEV1 in the Framingham Heart Study. Respir Res. 2015;16(1):1–8. | ||
Khoury MJ, Beaty TH, Tockman MS, Self SG, Cohen BH. Familial aggregation in chronic obstructive pulmonary disease: use of the loglinear model to analyze intermediate environmental and genetic risk factors. Genet Epidemiol. 1985;2(2):155–166. | ||
Amra B, Borougeni VB, Golshan M, Soltaninejad F. Pulmonary function tests and impulse oscillometry in severe chronic obstructive pulmonary disease patients’ offspring. J Res Med Sci. 2015;20(7):697–700. | ||
Higgins M, Keller J. Familial occurrence of chronic respiratory disease and familial resemblance in ventilatory capacity. J Chron Dis. 1975;28(4):239–251. | ||
Mostovoĭ I. [Clinico-genetic research in chronic bronchitis]. Ter Arkh. 1987;60(3):52–55. Russian. | ||
Silverman EK, Chapman HA, Drazen JM, et al. Genetic epidemiology of severe, early-onset chronic obstructive pulmonary disease: risk to relatives for airflow obstruction and chronic bronchitis. Am J Respir Crit Care Med. 1998;157(6):1770–1778. | ||
McCloskey SC, Patel BD, Hinchliffe SJ, Reid ED, Wareham NJ, Lomas DA. Siblings of patients with severe chronic obstructive pulmonary disease have a significant risk of airflow obstruction. Am J Respir Crit Care Med. 2001;164(8 Pt 1):1419–1424. | ||
Hersh CP, Hokanson JE, Lynch DA, et al. Family history is a risk factor for COPD. Chest. 2011;140(2):343–350. | ||
Zöller B, Li X, Sundquist J, Sundquist K. Familial transmission of chronic obstructive pulmonary disease in adoptees: a Swedish nationwide family study. BMJ open. 2015;5(4):e007310. | ||
Kurzius-Spencer M, Sherrill DL, Holberg CJ, Martinez FD, Lebowitz MD. Familial correlation in the decline of forced expiratory volume in one second. Am J Respir Crit Care Med. 2001;164(7):1261–1265. | ||
Lu B, He Q. Correlation of pulmonary functions of COPD patients to those of their first-degree children. Chin Med J. 2003;116(7):991–995. | ||
Givelber RJ, Couropmitree NN, Gottlieb DJ, et al. Segregation analysis of pulmonary function among families in the Framingham Study. Am J Respir Crit Care Med. 1998;157(5):1445–1451. | ||
Miravitlles M, Soriano JB, Garcia-Rio F, et al. Prevalence of COPD in Spain: impact of undiagnosed COPD on quality of life and daily life activities. Thorax. 2009;64(10):863–873. | ||
Mannino DM, Homa DM, Akinbami LJ, Ford ES, Redd SC. Chronic obstructive pulmonary disease surveillance – United States, 1971–2000. Respir Care. 2002;76(10):1184–1199. | ||
Hardin M, Silverman EK. Chronic obstructive pulmonary disease genetics: a review of the past and a look into the future. J COPD F. 2014;1(1):33–46. | ||
Madison R, Mittman C, Afifi A, Zelman R. Risk factors for obstructive lung disease. Am Rev Respir Dis. 1981;124(2):149–153. | ||
Upton MN, Smith GD, McConnachie A, Hart CL, Watt GC. Maternal and personal cigarette smoking synergize to increase airflow limitation in adults. Am J Respir Crit Care Med. 2004;169(4):479–487. | ||
Hayden LP, Hobbs BD, Cohen RT, et al. Childhood pneumonia increases risk for chronic obstructive pulmonary disease: the COPDGene study. Respir Res. 2015;16(1):115. | ||
Løkke A, Lange P, Scharling H, Fabricius P, Vestbo J. Developing COPD: a 25 year follow up study of the general population. Thorax. 2006;61(11):935–939. | ||
DeJong SR, Veltman RH. The effectiveness of a CNS-led community-based COPD Screening and Intervention Program. Clin Nurse Spec. 2004;18(2):72–79. | ||
Soriano JB, Zielinski J, Price D. Screening for and early detection of chronic obstructive pulmonary disease. Lancet. 2009;374(9691):721–732. | ||
Garcia-Aymerich J, Serra I, Gómez FP, et al. Physical activity and clinical and functional status in COPD. Chest. 2009;136(1):62–70. | ||
Vincken W, Van Noord J, Greefhorst A, et al. Improved health outcomes in patients with COPD during 1 yr’s treatment with tiotropium. Eur Respir J. 2002;19(2):209–216. | ||
Fishman AP. One hundred years of chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 2005;171(9):941–948. | ||
Ng M, Freeman MK, Fleming TD, et al. Smoking prevalence and cigarette consumption in 187 countries, 1980–2012. JAMA. 2014;311(2):183–192. |
Supplementary materials
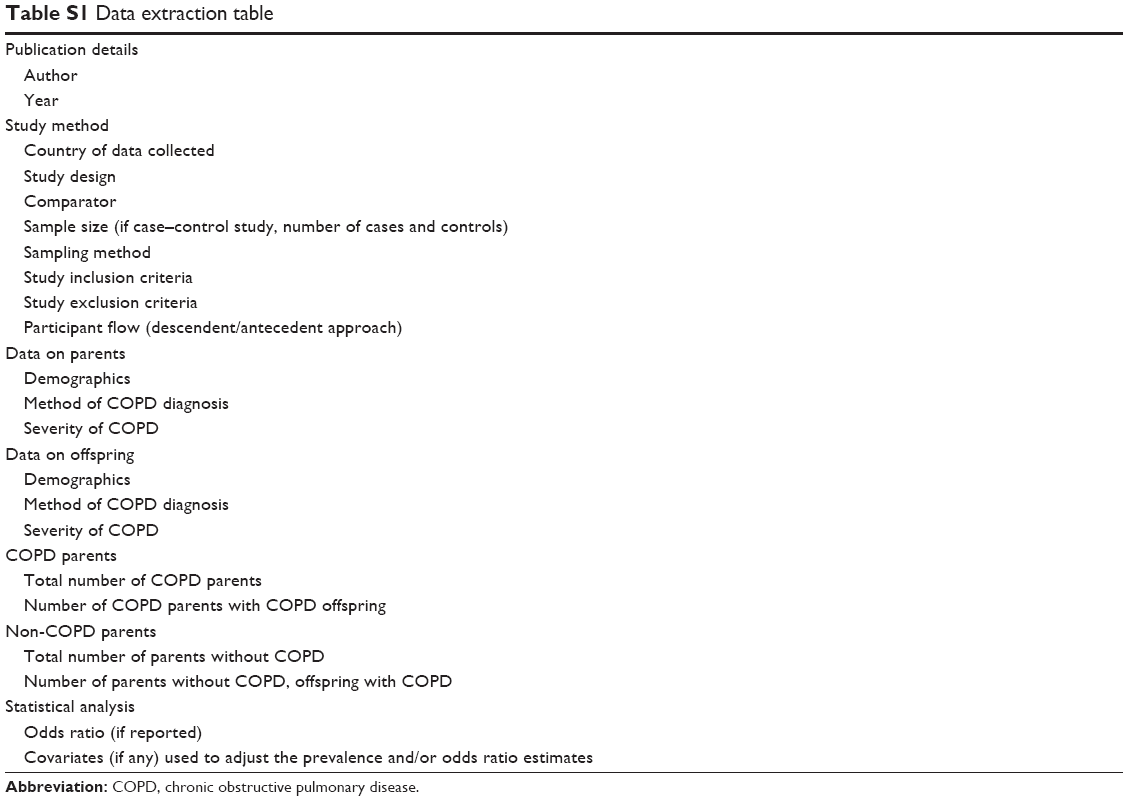 | Table S1 Data extraction table |
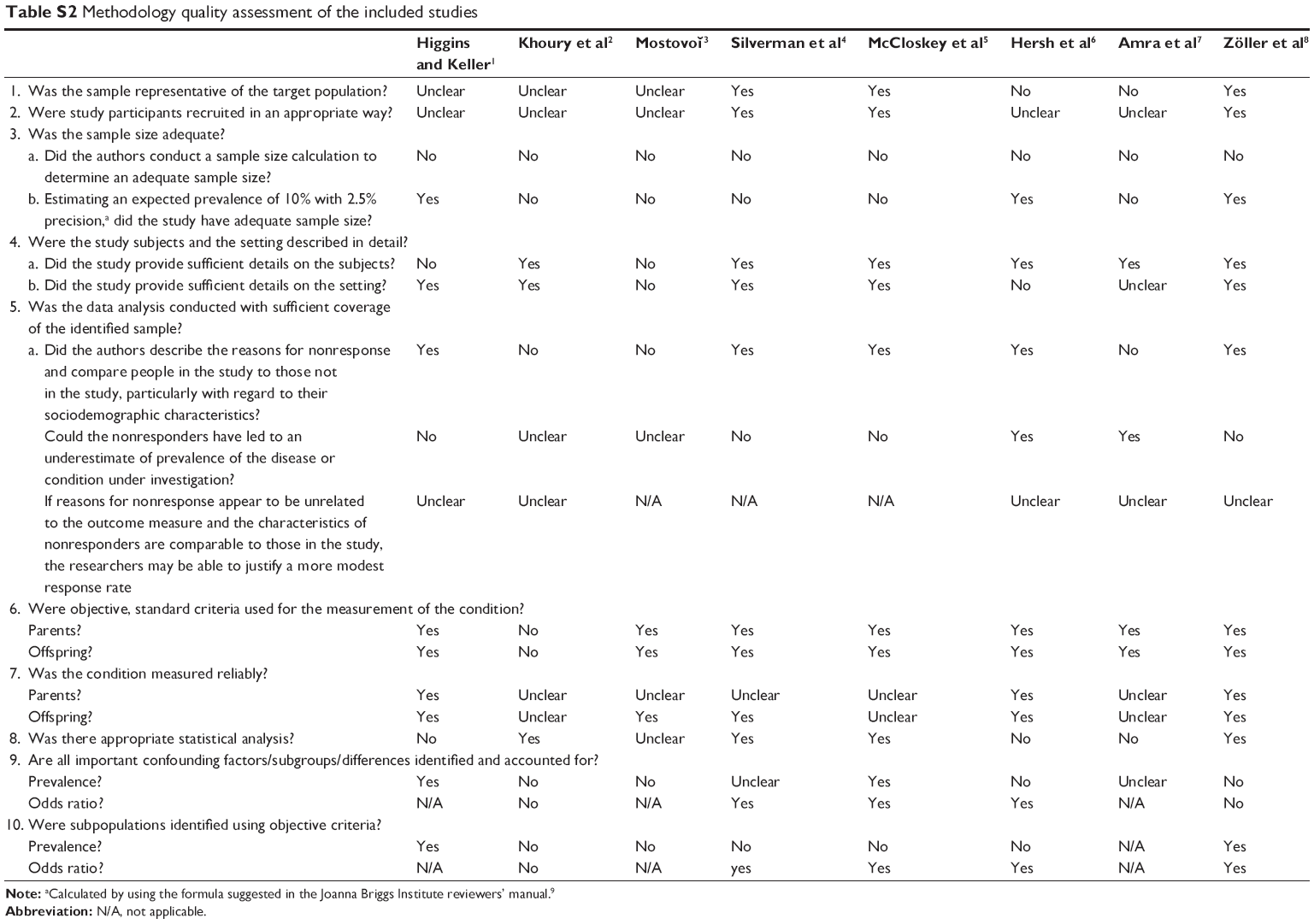 | Table S2 Methodology quality assessment of the included studies |
References
Higgins M, Keller J. Familial occurrence of chronic respiratory disease and familial resemblance in ventilatory capacity. J Chron Dis. 1975;28(4):239–251. | ||
Khoury MJ, Beaty TH, Tockman MS, Self SG, Cohen BH. Familial aggregation in chronic obstructive pulmonary disease: use of the loglinear model to analyze intermediate environmental and genetic risk factors. Genet Epidemiol. 1985;2(2):155–166. | ||
Mostovoĭ I. [Clinico-genetic research in chronic bronchitis]. Ter Arkh. 1987;60(3):52–55. Russian. | ||
Silverman EK, Chapman HA, Drazen JM, et al. Genetic epidemiology of severe, early-onset chronic obstructive pulmonary disease: risk to relatives for airflow obstruction and chronic bronchitis. Am J Respir Crit Care Med. 1998;157(6):1770–1778. | ||
McCloskey SC, Patel BD, Hinchliffe SJ, Reid ED, Wareham NJ, Lomas DA. Siblings of patients with severe chronic obstructive pulmonary disease have a significant risk of airflow obstruction. Am J Respir Crit Care Med. 2001;164(8 Pt 1):1419–1424. | ||
Hersh CP, Hokanson JE, Lynch DA, et al. Family history is a risk factor for COPD. Chest. 2011;140(2):343–350. | ||
Amra B, Borougeni VB, Golshan M, Soltaninejad F. Pulmonary function tests and impulse oscillometry in severe chronic obstructive pulmonary disease patients’ offspring. J Res Med Sci. 2015;20(7):697–700. | ||
Zöller B, Li X, Sundquist J, Sundquist K. Familial transmission of chronic obstructive pulmonary disease in adoptees: a Swedish nationwide family study. BMJ open. 2015;5(4):e007310. | ||
Munn Z, Moola S, Lisy K, Riitano D. The Joanna Briggs Institute Reviewers’ Manual 2014. The Systematic Review of Prevalence and Incidence Data. Adelaide, SA: The Joanna Briggs Institute; 2014. |
 © 2017 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2017 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.