")
Back to Journals » Patient Preference and Adherence » Volume 12
“I don’t know exactly what you’re referring to”: the challenge of values elicitation in decision making for implantable cardioverter-defibrillators
Authors Carroll SL , Embuldeniya G, Pannag J , Lewis KB, Healey JS, McGillion M, Thabane L, Stacey D
Received 10 May 2018
Accepted for publication 26 June 2018
Published 28 September 2018 Volume 2018:12 Pages 1947—1954
DOI https://doi.org/10.2147/PPA.S173705
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Johnny Chen
Sandra L Carroll,1–3 Gayathri Embuldeniya,3 Jasprit Pannag,1 Krystina B Lewis,4 Jeff S Healey,2,3,5 Michael McGillion,1,2 Lehana Thabane,2,6,7 Dawn Stacey4,8
1School of Nursing, McMaster University, Hamilton, ON, Canada; 2Population Health Research Institute, Hamilton Health Sciences, Hamilton, ON, Canada; 3Hamilton Health Sciences, Hamilton, ON, Canada; 4School of Nursing, University of Ottawa, Ottawa, ON, Canada; 5Department of Medicine, McMaster University, Hamilton, ON, Canada; 6Department of Health Research Methods, Evidence and Impact, McMaster University, Hamilton, ON, Canada; 7Biostatistics Unit, St. Joseph’s Healthcare, Hamilton, ON, Canada; 8Ottawa Hospital Research Institute, Ottawa, ON, Canada
Purpose: Patients’ values are a key component of patient-centered care and shared decision making in health care organizations. There is limited understanding on how patients’ values guide their health related decision making or how patients understand the concept of values during these processes. This study investigated patients’ understanding of their values in the context of considering the risks/benefits of receiving an implantable cardioverter-defibrillator (ICD).
Patients and methods: A qualitative substudy was conducted within a feasibility trial with first-time ICD candidates randomized to receive a patient decision aid or usual care prior to specialist consultation. Semi-structured interviews were conducted with participants post-implantation or post-specialist consultation.
Results: Sixteen patients (ten male) aged 47–87 years participated. Of these, ten (62.5%) received the patient decision aid prior to specialist consultation. Findings revealed patients were confused by the word “values” and had difficulty expressing values related to risks/benefits during ICD decision making. When probed, values were conceptualized broadly capturing other factors such as desire to live, good quality of life, family’s views, ICD information, control over decision, and medical authority.
Conclusion: This study revealed the difficulty patients considering an ICD had with articulating their values in the context of an ICD health decision and highlighted the challenge to effectively elicit patients’ values within health decisions overall. It is suggested that there should be a shift away from the use of the word “values” when speaking directly to patients toward language such as “what matters to you the most” or “what is most important to you”.
Keywords: values, patient preferences, patient engagement, qualitative, health decision
Introduction
Engaging patients is the cornerstone of shared decision making (SDM).1 Patients’ values are commonly referenced in health care as a key component of patient-centered care, evidence-informed decision making, and SDM. In this context, values are most often defined as the relative desirability of specific attributes of a health-related option.2 However, there is limited evidence and understanding on how patients’ values guide health decision making or how patients understand the concept of values. The Ottawa Decision Support Framework defines “values” as a person’s informed attitudes about the relative desirability/undesirability of a health care option’s unique characteristics, rather than the “overarching ethical, religious, political or social principles that guide how an individual lives”.3–5 However, for some people, values overlap with precisely these factors, where decision support interventions intend to “remind patients of an array of simple social and moral values that are important”.5
Patient decision aids (PDAs) are decision support tools used during SDM where there may be no single best course of action, with the “best option” being dependent on attributes of the options mattering most to the patient.1,6 PDAs can be used to facilitate patients’ value clarification and better prepare patients to make informed health decisions that are consistent with what is personally most desirable or valued to them.7 This is achieved through value clarification methods (VCMs) that make clear patients’ personal values, preferences, and treatment goals. PDAs are shown to improve knowledge, reduce decisional conflict, and help patients actively participate in decision making with their health practitioner.8,9 Individuals who use PDAs are more likely to choose options matching their values.6,9
The International Patient Decision Aids Standards1 indicates that PDAs should fulfill two key criteria: 1) provision of information about treatment options, benefits, and harms and 2) clarification and expression of values. As well, VCMs should include attributes related to treatment options, the decision context, and options as a whole.2 These are key to informed decision making,10 where clarification of individual values through VCMs encourages patients to weigh their options and improve the match between what is personally most desirable and which treatment option is selected.1 This is referred to as values–choice congruence – a measure of decision quality.11
In addition to the lack of clarity about the meaning of values, there is little consensus in the methods of elicitation.2 Two major forms of VCMs currently exist: implicit approaches (eg, decision boards, attribute tables, narratives) and explicit approaches (eg, rating, ranking, reflecting upon personal importance of the consequences).2 Within these reside a diverse range of VCMs, seen in a review by Witteman et al in 2016 describing 98 specific VCMs.12 Differences in theoretical frameworks, guidelines, representation of trade-offs, whether or not the VCM allowed for individuals’ own concerns, and methods of elicitation were reported. Also, there was variability in methods noted whereby patients answered slightly different questions, such as “What matters to me?”, “What’s best for me?”,10 and “Will I be able to afford to make this change?”.13
Given the variety in VCMs, philosophies, elicitation methods, and uncertainty about the very meaning of the term “values”, it is not surprising that a lack of agreement about the impact of VCMs on decision making exists. Understanding values congruence would provide a step in the right direction; however, values congruence is challenging to measure due to the heterogeneity of current measurements.9,14 Although values congruence reflects the agreement of an individual’s decision with stated values,12 it does not provide an understanding of why there may or may not be congruence between decisions and values or other influential factors. We proposed to bridge this gap by investigating patients’ understanding of values and its elicitation in the context of implantable cardioverter-defibrillator (ICD) decision making. We report findings from a qualitative substudy embedded in a larger feasibility trial where patients eligible for an ICD were randomized to receive a PDA or usual care15 and were later asked if they considered their values when deciding to receive an ICD.
Patients and methods
A descriptive qualitative study16,17 was conducted within a feasibility randomized controlled trial related to the use of a PDA for patients considering prophylactic ICD. This work was grounded within the integrative SDM model, a conceptual model based on a systematic review of definitions of SDM.18 The full study protocol15 and feasibility trial results are published.19 This trial had 41 patients who received the PDA and 41 patients who did not. Equal numbers of patients in each group (24/41; 58.6%) had an ICD implanted at 3 months. Eleven (26.8%) in the usual care group and 14 (34.2%) in the PDA group deferred the ICD, with 5 (12.2%) and 2 (4.9%) declining the ICD. Ethics approval was obtained from the Hamilton Integrated Research Ethics Board (#12-244).
The PDA development was guided by the International Patient Decision Aids Standards20,21 and the Ottawa Decision Support Framework.22 The PDA included a values clarification exercise with six questions (Table 1) developed by a panel of health practitioners, patient representatives, and decision scientists using a modified Delphi process.23 The six questions were identified as features of options that the panel and patients described as important to avoid or value when choosing to receive an ICD and ICD therapy. A two-stage Delphi process was used to determine and reach consensus for these questions.19 This involved a 27-member panel of 13 health professionals and 14 patients providing comments to each element of the decision aid. In the second stage, comments were formed in questions which were ranked for agreement. Results from this stage formed the decision aid. In the feasibility trial, participants were asked to rate the importance of each question on a 5-point scale, from “not important” to “very important”. Only those randomized to receive the PDA completed the values clarification exercise.
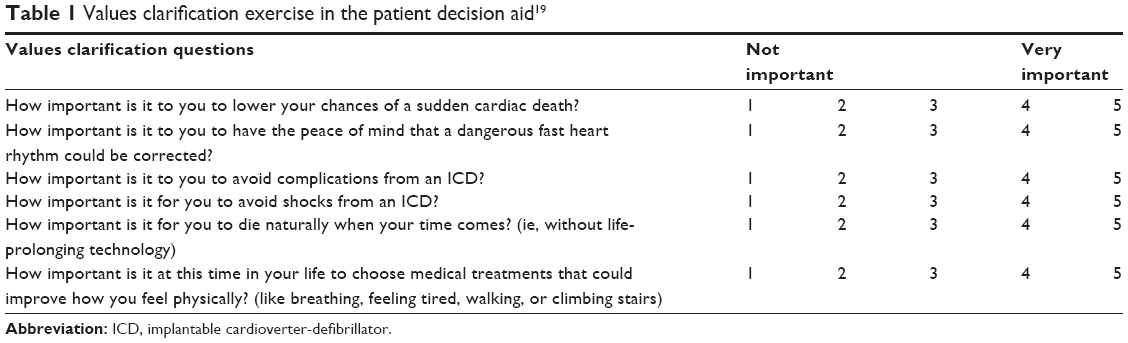 | Table 1 Values clarification exercise in the patient decision aid19 |
Participants
Patients who had been referred for a specialist consultation (with an electrophysiologist) to discuss the option of receiving a prophylactic ICD were invited to participate in the feasibility trial and a semi-structured interview. We used purposeful sampling (ie, maximum variation) to include participants who were: 1) randomized and 2) had gone on to receive an ICD, declined the ICD, or deferred their ICD decision making. Attempts were also made to ensure a balance between male and female participants. Excluded were patients: 1) unable to understand the English-language PDA and 2) referred for cardiovascular resynchronization devices.
Study procedures
Eligible participants were contacted by telephone in the order of trial enrollment by the research assistant (RA). All participants had already signed written informed consent prior to trial enrollment. The RA, who was not involved with direct care, confirmed interest in taking part in the interview. Telephone interviews were conducted by SC and a trained RA 3–6 months after ICD consultation and ICD decision making. The interview duration ranged from 15 to 40 minutes. If the patient desired, their spouse/family member was present, though they were not formally part of the interview or signed consent. The interview guide was revised once to improve readability of questions and add probes. The questions included: “When you hear the word values, what does that mean to you?”, “What is the most important influence when you are making health-related decisions?”, “Were you clear about which benefits and risks mattered most to you?”, and “Was it a shared decision between you and your doctor?”. Data collection continued until saturation for key themes was reached. Interviews were digitally recorded and transcribed verbatim by a transcriptionist. All patient identifying information was removed from transcripts, and participants were given a unique identification number.
Analysis
Transcripts were analyzed using content analysis,24 with key themes iteratively identified and organized using NVivo 10. Three research team members (JP, GE, and SC) read the transcripts numerous times to develop open codes and liaised to review and compare data interpretations. Codes were grouped into categories that were continuously amended during the coding process as their latent or underlying meanings were further explored25 and new concepts emerged.
Results
Of the 16 participants who gave consent, 10 were randomized to receive the PDA and 6 to usual care. Participant age ranged from 47 to 87 years, with ten males and six females (Table 2). Ten participants chose to undergo ICD implantation (seven PDA and three usual care), three declined the ICD (two PDA and one usual care), and three deferred their decision (one PDA and two usual care). Although these proportions differ from the larger feasibility trial, overall, the categories derived from the interviews were similar between all groups of participants (ie, those who did and did not receive the PDA, and those who did or did not elect to get an ICD). The findings are presented together.
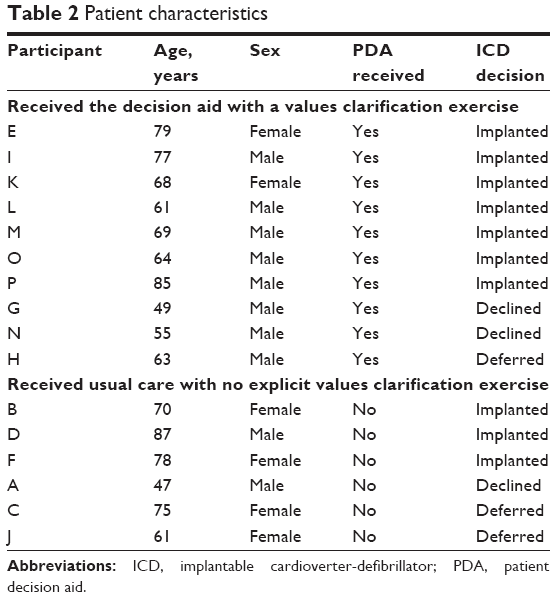 | Table 2 Patient characteristics |
Values – “I don’t know exactly what you’re referring to”
More often than not, participants were unsure of what they were being asked: “It’s a hard question,” said one (Participant-A; declined). “I do not know exactly what you’re referring to,” said another (Participant-D, no PDA; implanted). “I do not know how to answer that one,” said yet another (Participant-F, no PDA; implanted). As a means of providing a tentative explanation where participants could expand within the context of their ICD decision, the interviewer open-endedly described values as “what matters to you most”. Yet, participants still struggled to understand what was being asked of them. Many had trouble with the term values; others were confused by the use of the term as a noun “values” or as a verb “value”:
Value usually equals family for me and what your family thinks of you and vice versa, and your morals and values are kind of the same feeling. [Participant-A, no PDA; declined]
It means I’m doing something that’s going to be worthwhile, getting something that’s … worth my time or my money … [Participant-O, PDA; implanted]
A few adopted a largely instrumentalist approach to the question, focusing on answering what was most important to them when prompted by the interviewer. When participants did this, their responses changed from hesitant and uncertain to confident and pragmatic:
Interviewer: When you hear that word “values”, what does that mean to you?
Participant: Value – I do not know [laughter]. I have no idea.
Interviewer: So what’s most important to you?
Participant: What’s important for me is to get better. [Participant-K, PDA; implanted]
We found the concept of values was equally uncertain for the group that received the PDA and the group that did not. When asked about what contributed to a specific decision, participants’ responses provided only a partial understanding of what informed their decision making. In the course of the interview, contextual factors of arguably equal importance to the participant became apparent. Below, we present the direct and indirect factors that influenced participants’ ICD decision making.
Factors that mattered directly in ICD decision making
When probed further, participants revealed that they most valued desire to live life, good quality of life (QOL), their family’s views, being informed about the ICD, and ability to exercise control over decision making and medical authority. For a few people, the role of religion and spirituality in their lives impacted their decision making.
Desire to live life
Staying alive was clearly valued by patients, regardless of whether they accepted or declined the ICD and was most frequently cited as important:
There was very little to choose from. I had to take the defibrillator to give me a better chance at life. [Participant-D, no PDA; implanted]
However, the desire to live, although strong across participants, was usually tempered by other considerations, such as a desire to self-manage without medical interventions, coupled with a philosophical attitude toward mortality:
If it had to be done, I’m not going to say no … and then pay the consequences and I die; I still have the chance to extend my life. Definitely not going to pass that up. I just do not feel it’s needed right now. [Participant-G, PDA; declined]
Good QOL
The desire to live was weighed against QOL expectations. A number of participants cited concerns about losing their driver’s license (Participants-H, -L, -M). Another opted to go ahead with ICD implantation despite not being able to play golf, deciding “it’s time to give it up” (Participant-D). Yet another who worked in a factory around heavy machinery (Participant-N) declined the ICD due to concerns about electromagnetic interference with the ICD, which could lead to inappropriate shocks. Others were worried about being a burden: “As well as living, I would like to live without much trouble to or for anybody” (Participant-H). For some, the ICD represented too great an impact on QOL:
Some of the risks, like once the device was put in – well, okay, for so long you cannot lift your arm up you know, or tear the leads out, there’s a possibility it might malfunction, there’s the venturing every 5–7 years or whatever it was to replace the battery; it was a real game changer. And I think if you were going to travel and things like that, it just … opens up a big whole new can of worms. I just didn’t feel I was ready for that. [Participant-G, PDA; declined]
For others, the ICD facilitated greater enjoyment of life and provided them with “back-up” (Participant-M) or peace of mind:
I want to see a couple of the kids get married, and … you just do not really want to go yet. And my mind’s at ease, and it was like a big load was lifted off my shoulders. [Participant-E, PDA; implanted]
Family’s views
For almost all participants, family played a significant role as a consideration in the decision making process (eg, choosing the device to allay family anxieties) or as a key player in the decision making process itself, within a SDM context. Family was an important source of emotional and informational support. The desire to live appeared to be of value to some because it was of value to their families:
The thing that swayed me was my children saying, ‘Dad, we need you.’ [Participant-O, PDA; implanted]
Information about the ICD
A majority of participants valued information about the ICD’s function. Information was acquired through books, videos, Internet, and conversations with doctors and family. For those who received the PDA, its risks, benefits, and background information were important. For some, the work of acquiring knowledge was particularly critical to decide if ICD implantation and its potential risks were worthwhile. Information was sometimes linked to knowledge, power, and control:
You cannot make a decision without good knowledge; then you’re just flipping a coin…. Knowledge is power, so you have control, and it helps with the mental state too. The more information the better. [Participant-A, no PDA; declined]
Control over decision and medical authority
Despite the importance given to informational knowledge, participants were divided on the need to exercise control over the ICD decision. For a small majority, control was of great importance, while others valued the doctor’s expertise above all else, and still others thought of it as a shared decision, made in consultation with their doctor, but taking into account their individual circumstances:
If the doctor was telling me, he was 100%, [that] there’s no ands, ifs, or buts, you should get this done, and they had facts to back it up, then I would make a decision. [Participant-G, PDA; declined]
For others, their doctor’s expertise – and sometimes institutional trust – was valued. In fact, some felt there was no decision to be made once their doctor suggested ICD implantation. Yet, they felt in control of their decision, as relinquishing control of their decision to their doctor was itself seen as an active decision:
I thought … whatever they suggest is good for me, and I’ll go along. That’s what I call values. I valued their opinion. [Participant-D, no PDA; implanted]
Role of religion and spirituality
Although three participants alluded to the influence of religion or spirituality in their decision making, one was quite explicit about the role it played:
The first influence was my church and the fact that I know I’m covered there, and if God didn’t want me to do it, he’d have given me a sign of some sort. [Participant-E, PDA; implanted]
Factors that mattered indirectly in ICD decision making
Another set of factors that impacted participants’ decision making were perhaps of equal significance, though were not part of direct responses to questions eliciting values, but were voiced when explaining the context of their decision making. They revealed that decisions were influenced by age, emotional state, and previous life and health experiences, and as a result, values would change or shift due to these factors.
Changing values
A majority of participants, for instance, claimed that their decision would be different if made 20 years ago or 20 years in the future:
Because I’m on the younger side of the scale, my list of importance would be different than those who are seniors so, yes, in this case, it’s all about keeping alive. It depends what stage of life you’re in. [Participant-A, no PDA; declined]
Twenty years from now, I probably would not care one way or the other. I’m pretty sure I will be ready to go. [Participant-H, PDA; deferred]
A few alluded to their emotional state at the time they were offered the ICD and the impact it had on their decision making:
At that time in January, I had almost chosen not to even bother with the defibrillator if they wanted to give it to me. I was already set to not live any longer. I was ready to die. (Participant-H, PDA; deferred)
Individuals’ health histories also impacted their decision making. One participant with a family history of heart problems was much more amenable to the ICD (Participant-O, PDA; implanted). Another commented on a brother’s success with bypass surgery, whereas his spouse commented on the impact of his family’s history:
[He] lost his younger brother when the brother was 52 years old to a heart attack. So there was a cardiac history … that we were always aware of and [he] was always aware of, which is why he never hesitated. [Participant-P, PDA; implanted]
Although participants directly and indirectly suggested that they took certain factors into consideration when decision making, it is difficult to precisely gauge which were most significant for individuals in terms of value clarification. Participant-N, who received the PDA and declined the ICD, serves as an example. His decision was informed by his dislike of medical interventions and identification with doctors, “I am not anywhere close to doctors and stuff like that; I’m a steelworker,” contrary advice from family and friends, familiarity with his brother’s pacemaker that “screwed up a couple of times …,” his religion, “I’m Catholic …; if the big guy upstairs wants me, he’s going to take me no matter what”. When asked if he could identify the most important influence in his decision making, he replied, “I really cannot answer that because it’s a bunch of maybe little factors you know, both negative and positive.”
Discussion
This study sought to understand how values were perceived by patients in the context of ICD decision making. Overall, participants displayed uncertainty and vagueness about the concept of values. Participants were confused by the meaning of values, and a disconnect lay between associations of “values” with “morals”. Researchers’ framing of values during the interview as “that which matters to you most” or “so what’s most important to you” closely mirrored its definition as “that which is most important to you” featured in the VCM embedded in the PDA. This language is also used in other tools such as the SURE test,26 which includes the question, “Are you clear about which benefits and risks matter most to you?”.26 Despite this, the introduction of the concept of values during the interview process resulted in a layer of complexity that bewildered some and left others unsure of how to respond.
The VCM embedded within the PDA focused on ICD-centered risk and benefit considerations such as prolonging life vs dying naturally, QOL, and specific risks of the ICD compared to medical management. Although participants dwelled on these when identifying decision-making considerations of importance, other factors surfaced that did not align with the PDA or weighing of treatment option risks/benefits. Direct considerations included desire to live life, good QOL, family’s views, being well-informed, advice from a trusted doctor, and the ability to exercise control. Indirect considerations included age, life and health experiences, and emotional well-being. Participants’ accounts of their values significantly extended beyond the values represented in the ICD-centered VCM, affirming the importance of discussion alongside decision aids allowing space and opportunity for individuals to express their own concerns.12 Participants’ ultimate decision was the convergence of several valued influences, which resonate with layered “webs of significance”27 that have been described by others.
There have been other studies examining patient experiences related to ICD decision making. In a cross-sectional survey of 295 patients, 28% indicated that they had not been told about the option of not getting an ICD and 37% did not recall being asked if they wanted an ICD.30 Another qualitative study has found that some patients did not feel that they were fully aware of risks until they personally experienced these post-implantation.31 In some cases, this lack of awareness contributed to patients’ eventual decisional regret.30,32 Using behavioral theories to further investigate these omissions, Matlock et al suggested that cognitive biases in favor of the ICD are at play as a result of clinicians’ strong positive framing for ICD therapy when meeting with eligible patients.33 Some would argue that a positive framing is entirely justifiable given the ICD’s Class I recommendation in Clinical Practice Guidelines; yet, it is documented that some patients have declined ICD therapy in accordance with their personal preferences and values.19,33,34 These works reinforce the complexity of decision making for ICD implantation and the need to carefully balance evidence with patients’ values for or against the intervention.
It is also very likely that patients’ values will change from the decision point during the initial ICD implantation period, and as such, patients’ value clarification would require future revisiting. Of significance would be when the decision to replace the ICD approaches. This occurs when the ICD nears the end of its mechanical life (approximately every 5–7 years). Research exploring this line of inquiry suggests that the majority of patients are unaware that replacement is optional, with 27% of patients indicating that not replacing the ICD would have been considered.35 Here, patients may be valuing QOL over quantity of life, which may reflect differing values as patients age.
Other recent research has found that patients perceive values more broadly than the clinical consequences. Lee et al spoke with patients making decisions about insulin use and recommended that values should include patients’ priorities, their life philosophies, and personal background.28 Armstrong and Mullins29 proposed a taxonomy of values to be considered during decision making that included situational, global, external, and decisional values. They suggest that all four areas should be raised by the clinician and used to frame the SDM process.
To improve the trustworthiness of the findings, several strategies were applied. The use of a qualitative approach enabled us to capture personal experiences as told by participants through their own narratives. As well, the background and experience of the investigative team with this subject matter and population offer additional credibility to the interpretation of our findings. Our sample included a range of participants: those exposed to the PDA, usual care, and those who declined, accepted, or deferred the ICD. Moreover, all of our participants received the same ICD referral processes, where they met with a specialist to consider an ICD for primary prevention of sudden cardiac death – an elective procedure in Canada. This offers potential transferability of our findings to other primary prevention ICD candidates using similar processes. However, given that the interviews took place 3–6 months after the specialist consultation, it is possible that some patients were not able to fully recall the discussion that had taken place. Another limitation is the use of a brief interview as a means of uncovering closely held and difficult-to-articulate concepts for patients, whereby a more fulsome discussion may have helped unpack the complexity of values elicitation.
Practice implications
Based on experiences from patients in this substudy, we suggest that decision scientists consider the conceptualization of VCMs and the elicitation of values on both semantic and methodological grounds. This would involve two key suggestions. First, is a shift away from the use of the word “values” when speaking directly to patients toward language such as “what matter to you the most” or “what is most important to you”. Others have suggested a focus on goals and concerns as concepts that relate to decision quality.36 Asking patients what matters to them rather than what their values are could reduce confusion about the term, while allowing patients to identify relevant factors taken into account during the decision making process.
Second, is the recognition of the limitations of many VCMs as currently designed, which privilege the particularities of the clinical decision being considered as somehow detached from the larger personal and social context of decision making. This would require acknowledging that many key factors patients take into account in decision making may be impossible for researchers to represent in VCMs, given their heterogeneity and sociocultural particularity to individual patients. In addition, certain implicit decision making factors may be difficult for patients to express as they are a part of their worldview itself, but as such will unavoidably be taken into account in decision making contexts. This work brings to light our need to communicate with patients in a way that they understand what we are asking and why.
Conclusion
This study underscores not only the challenges of VCMs as a means of helping patients evaluate the desirability of treatment options they are presented with, but also the challenges of traditionally employed methods of values elicitation, both during and after decision making. Given the emphasis on patient-centered care, evidence informed decision making, SDM, and patient-oriented research across health care and research institutions where consideration of patient “values” is espoused, our work reveals the real challenges to effectively elicit what patients value in the context of health decisions. Our work reinforces the importance of conversation to clarify patient values and understand the breadth of factors that patients take into consideration.
Acknowledgment
This study was funded by the Canadian Institutes of Health Research (CIHR)-operating grant #119449.
Disclosure
The authors report no conflicts of interest in this work.
References
Volk RJ, Llewellyn-Thomas H, Stacey D, Elwyn G. Ten years of the International Patient Decision Aid Standards Collaboration: evolution of the core dimensions for assessing the quality of patient decision aids. BMC Med Inform Decis Mak. 2013;13 (Suppl 2):S1. | ||
Fagerlin A, Pignone M, Abhyankar P, et al. Clarifying values: an updated review. BMC Med Inform Decis Mak. 2013;13 (Suppl 2):S8. | ||
Llewellyn-Thomas HA, Crump RT. Decision support for patients: values clarification and preference elicitation. Med Care Res Rev. 2013;70(1 Suppl):50S–79S. | ||
Feather NT. Values, valences, expectations, and actions. J Soc Issues. 1992;48(2):109–124. | ||
Reyna VF, Nelson WL, Han PK, Pignone MP. Decision making and cancer. Am Psychol. 2015;70(2):105–118. | ||
Munro S, Stacey D, Lewis KB, Bansback N. Choosing treatment and screening options congruent with values: do decision aids help? Sub-analysis of a systematic review. Patient Educ Couns. 2016;99(4):491–500. | ||
Stacey D, Légaré F, Col NF, et al. Decision aids for people facing health treatment or screening decisions. Cochrane Database Syst Rev. 2014;(1):CD001431. | ||
Feldman-Stewart D, Tong C, Siemens R, et al. The impact of explicit values clarification exercises in a patient decision aid emerges after the decision is actually made: evidence from a randomized controlled trial. Med Decis Making. 2012;32(4):616–626. | ||
Stacey D, Bennett CL, Barry MJ, et al. Decision aids for people facing health treatment or screening decisions. Cochrane Database Syst Rev. 2011;(10):CD001431. | ||
Witteman HO, Chipenda Dansokho S, Exe N, Dupuis A, Provencher T, Zikmund-Fisher BJ. Risk communication, values clarification, and vaccination decisions. Risk Anal. 2015;35(10):1801–1819. | ||
Sepucha KR, Borkhoff CM, Lally J, et al. Establishing the effectiveness of patient decision aids: key constructs and measurement instruments. BMC Med Inform Decis Mak. 2013;13(Suppl 2):S12. | ||
Witteman HO, Scherer LD, Gavaruzzi T, et al. Design features of explicit values clarification methods: a systematic review. Med Decis Making. 2016;36(4):453–471. | ||
Sheridan SL, Griffith JM, Behrend L, Gizlice Z, Cai J, Pignone MP. Effect of adding a values clarification exercise to a decision aid on heart disease prevention: a randomized trial. Med Decis Making. 2010;30(4):E28–E39. | ||
Winn K, Ozanne E, Sepucha K. Measuring patient-centered care: an updated systematic review of how studies define and report concordance between patients’ preferences and medical treatments. Patient Educ Couns. 2015;98(7):811–821. | ||
Carroll SL, Mcgillion M, Stacey D, et al. Development and feasibility testing of decision support for patients who are candidates for a prophylactic implantable defibrillator: a study protocol for a pilot randomized controlled trial. Trials. 2013;14:346. | ||
Kim H, Sefcik JS, Bradway C. Characteristics of qualitative descriptive studies: a systematic review. Res Nurs Health. 2017;40(1):23–42. | ||
Colorafi KJ, Evans B. Qualitative descriptive methods in health science research. HERD. 2016;9(4):16–25. | ||
Makoul G, Clayman ML. An integrative model of shared decision making in medical encounters. Patient Educ Couns. 2006;60(3):301–312. | ||
Carroll SL, Stacey D, McGillion M, et al. Evaluating the feasibility of conducting a trial using a patient decision aid in implantable cardioverter defibrillator candidates: a randomized controlled feasibility trial. Pilot Feasibility Stud. 2017;3:49. | ||
Elwyn G, O’Connor AM, Bennett C, et al. Assessing the quality of decision support technologies using the International Patient Decision Aid Standards instrument (IPDASi). PLoS One. 2009;4(3):e4705. | ||
Elwyn G, O’Connor A, Stacey D, et al. Developing a quality criteria framework for patient decision aids: online international Delphi consensus process. BMJ. 2006;333(7565):417. | ||
O’Connor AM, Tugwell P, Wells GA, et al. A decision aid for women considering hormone therapy after menopause: decision support framework and evaluation. Patient Educ Couns. 1998;33(3):267–279. | ||
Carroll SL, McGillion M, McGrath C, et al. Application of a delphi method to develop a patient decision aid for implantable cardioverter defibrillator candidates. Circ Qual Care Outcomes Res. 2013;6:A117. | ||
Elo S, Kyngäs H. The qualitative content analysis process. J Adv Nurs. 2008;62(1):107–115. | ||
Graneheim UH, Lundman B. Qualitative content analysis in nursing research: concepts, procedures and measures to achieve trustworthiness. Nurse Educ Today. 2004;24(2):105–112. | ||
Légaré F, Kearing S, Clay K, et al. Are you SURE?: Assessing patient decisional conflict with a 4-item screening test. Can Fam Physician. 2010;56(8):e308–e314. | ||
Geertz C. The Interpretation of Cultures. USA: Basic Books; 1973. | ||
Lee YK, Low WY, Ng CJ. Exploring patient values in medical decision making: a qualitative study. PLoS One. 2013;8(11):e80051. | ||
Armstrong MJ, Mullins CD. Value assessment at the point of care: incorporating patient values throughout care delivery and a draft taxonomy of patient values. Value Health. 2017;20(2):292–295. | ||
Green AR, Jenkins A, Masoudi FA, et al. Decision-making experiences of patients with implantable cardioverter defibrillators. Pacing Clin Electrophysiol. 2016;39(10):1061–1069. | ||
Matlock DD, Nowels CT, Masoudi FA, et al. Patient and cardiologist perceptions on decision making for implantable cardioverter-defibrillators: a qualitative study. Pacing Clin Electrophysiol. 2011;34(12):1634–1644. | ||
Standing H, Exley C, Flynn D, et al. A qualitative study of decision-making about the implantation of cardioverter defibrillators and deactivation during end-of-life care. Health Services and Delivery Research. 2016;4(32). | ||
Matlock DD, Jones J, Nowels CT, Jenkins A, Allen LA, Kutner JS. Evidence of cognitive bias in decision making around implantable-cardioverter defibrillators: a qualitative framework analysis. J Card Fail. 2017;23(11):794–799. | ||
Carroll SL, Strachan PH, de Laat S, Schwartz L, Arthur HM. Patients’ decision making to accept or decline an implantable cardioverter defibrillator for primary prevention of sudden cardiac death. Health Expect. 2013;16(1):69–79. | ||
Lewis KB, Nery PB, Birnie DH. Decision making at the time of ICD generator change: patients’ perspectives. JAMA Intern Med. 2014;174(9):1508–1511. | ||
Sepucha KR, Belkora JK, Chang Y, et al. Measuring decision quality: psychometric evaluation of a new instrument for breast cancer surgery. BMC Med Inform Decis Mak. 2012;12:51–51. |
 © 2018 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2018 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.