")
Back to Journals » Clinical Ophthalmology » Volume 14
Lash Impaction in Meibomian Gland Orifice
Authors Mansour AM , El Jawhari KM
Received 10 March 2020
Accepted for publication 26 April 2020
Published 7 May 2020 Volume 2020:14 Pages 1245—1247
DOI https://doi.org/10.2147/OPTH.S253263
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Ahmad M Mansour,1,2 Khalil M El Jawhari3
1Department of Ophthalmology, American University of Beirut, Beirut, Lebanon; 2Department of Ophthalmology, Rafic Hariri University Hospital, Beirut, Lebanon; 3Medical University of Lodz, Lodz, Poland
Correspondence: Ahmad M Mansour
Department of Ophthalmology, American University of Beirut, PO Box 113-6044, Beirut, Lebanon
Tel +9613377633
Email [email protected]
Purpose: To analyze potential risk factors associated with eyelash impaction into meibomian gland orifice.
Methods: Retrospective review of one tertiary clinic over a period of 10 years.
Results: In this study, 18 patients were included, with a mean age of 61.6 years at diagnosis. Ten patients were symptomatic in the form of ocular irritation or foreign body sensation. The location of the impaction included 15 nasal half and 3 temporal half of the lid, 6 upper lid and 12 lower lid, 8 right side and 10 left side. Risk factors included dry eyes (10), allergic conjunctivitis (4), severe rubbing of the eye (6), sleeping on the eye (2), and recent phacoemulsification (1).
Conclusion: Ocular rubbing from either ocular allergy or dryness is associated with impaction of the lash into the orifice of the meibomian gland duct.
Keywords: cilia, eyelash, lash impaction, meibomian gland duct orifice
Introduction
Eyelashes provide a cosmetic role and a protective role (from insects and injury via blink-reflex trigger or mechanical sensor), but also dispense some sunshade and render an air filter action (dust catcher and diversion of airflow away from the surface of the eye). The upper eyelid carries about 150 lashes while the lower eyelid supports around 75 lashes.1–10 Lashes fall after an average of 4 months1 and at least 1–2 lashes are replaced daily.4 While most inferior lashes fall uniformly outside the eye, superior lashes can fall inside the eye; hence, there is a regular supply of loose lashes in the conjunctiva cul-de-sac.7–10 Despite recent advances in lash research, very little has been written about the subject of this report, lash impaction into meibomian gland orifice.1,2
Methods
This is a retrospective review of photographic files archived under the diagnosis of eyelash in the meibomian gland orifice in a single tertiary referral center (AMM) from January 2009 to September 2018. The ocular examination files were retrieved and an excel sheet was filled with the various clinical variables focusing on history of ocular rubbing, dry eyes, and ocular allergies. The study received Institutional Review Board approval (Rafic Hariri University Hospital ID 692018). Written informed consent for the research was obtained from the patients. The study followed the tenets of Helsinki.
Results
The collection data spanned 10 years among a total of about 70,000 patient visits. Mean age of the series was 61.6 years (range: 47–78, standard deviation 12.4) with 18 Caucasians, 9 males, 7 females, 2 unspecified. The location of the impaction included 15 nasal half and 3 temporal half 6 upper lid and 12 lower lid 8 right side and 10 left side. All except one had the bulb inside the duct while one had the bulb end protruding into the eye (Figure 1). Ten patients were symptomatic in the form of ocular irritation or foreign body sensation. Potential risk factors included 10 had dry eyes, 4 had allergic conjunctivitis, 6 admitted severe rubbing of the eye, 2 had the habit of sleeping face down on the eye, and 1 had recent phacoemulsification. One patient each had corneal graft, old herpetic corneal scar, plaque radiotherapy for choroidal melanoma, and proliferative diabetic retinopathy.
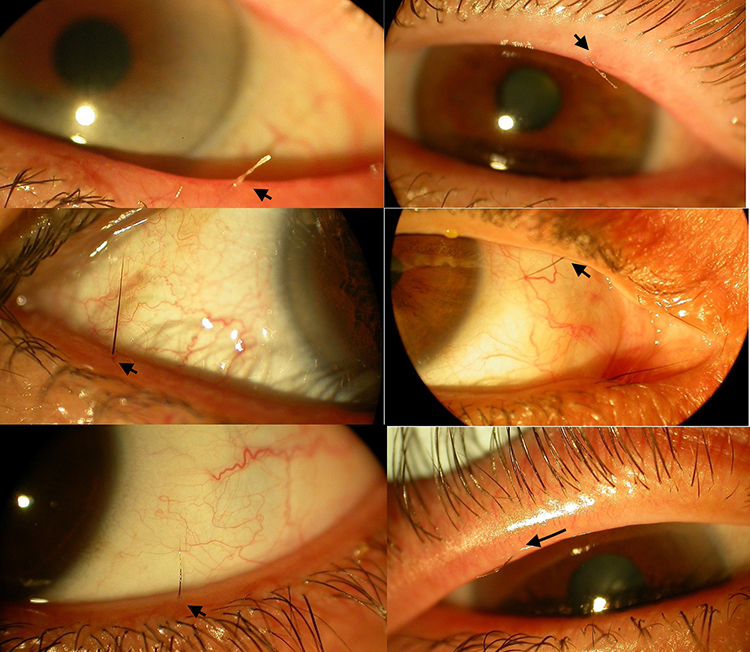 |
Figure 1 Composite showing eyelash protruding from a meibomian gland orifice (arrow) in lower eyelids (left) or upper eyelids (right) in 6 patients. |
Discussion
It appears from the current study that ocular rubbing from either ocular allergy or dryness constitutes a risk factor in the causation of lash impaction. Loose cilia cause mild-to-severe ocular irritation and are often mistaken for allergic conjunctivitis, nodular episcleritis or keratoconjunctivitis sicca.3 Lash can inadvertently enter the subconjunctival space, especially with previous scars and rarely find their way into the vitreous8 without a history of trauma or into the anterior chamber following phacoemulsification.9 Cilia entrapped in the lacrimal ductule may play a role in the formation of lacrimal ductular cysts.7 Cilia constitute a nidus for dacryoliths of the lacrimal excretory and secretory systems.10
Lash impaction into meibomian gland orifice appears to be very often overlooked and also quite rare occurring in 18/70,000 patient visits in the current study. Nagashima et al1 collected 39 cases of lash impaction into the meibomian gland duct out of a total of 30,456 outpatients. Treatment is simple removal of the lash and simultaneous treatment of underlying ocular cause that will help in avoiding eye rubbing. Differential diagnosis includes cilia incarnata interna5 (misdirected in-growing cilia present subconjunctivally), distichiasis6 (growth of cilia from meibomian gland orifice), and cilia impacted in lacrimal punctum.3
In conclusion, the current study suffers from being retrospective and with a small number of patients. Clinicians need to include impacted cilia in meibomian gland orifice in the differential diagnosis of ocular irritation. Impacted cilium is a rare cause of ocular irritation very often overlooked. The risk factor for its occurrence appears to be forceful ocular rubbing that allows cilia to get impacted.
Acknowledgments
This work and preparation of manuscript received no commercial sponsorship and assistance.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Nagashima K, Kido R. Relative roles of upper and lower lacrimal canaliculi in normal tear drainage. Jpn J Ophthalmol. 1984;28(3):259–262.
2. Gutteridge IF. Curious cilia cases. Clin Exp Optom. 2002;85(5):306–308. doi:10.1111/j.1444-0938.2002.tb03087.x
3. Singh S, Narang P, Mittal V. Getting hooked: eyelash in lacrimal punctum. Saudi J Ophthalmol. 2017;31(3):201–202. doi:10.1016/j.sjopt.2017.05.004
4. Khong JJ, Casson RJ, Huilgol SC, Selva D. Madarosis. Surv Ophthalmol. 2006;51(6):550–560. doi:10.1016/j.survophthal.2006.08.004
5. Belfort R, Ostler HB. Cilia incarnata. Br J Ophthalmol. 1976;60(8):594–596. doi:10.1136/bjo.60.8.594
6. Choo PH. Distichiasis, trichiasis, and entropion: advances in management. Int Ophthalmol Clin. 2002;42(2):75–87. doi:10.1097/00004397-200204000-00008
7. Lee JY, Woo KI, Suh YL, Kim YD. The role of entrapped cilia on the formation of lacrimal ductular cysts. Jpn J Ophthalmol. 2015;59(2):81–85. doi:10.1007/s10384-014-0360-2
8. Oh KT, Oh KT, Singerman LJ. An eyelash in the vitreous cavity without apparent etiology. Ophthalmic Surg Lasers. 1996;27(3):243–245.
9. Walker NJ, Hann JV, Talbot AW. Postoperative cilium entrapment by clear corneal incision. J Cataract Refract Surg. 2007;33(4):733–734. doi:10.1016/j.jcrs.2006.12.020
10. Baratz KH, Bartley GB, Campbell RJ, Garrity JA. An eyelash nidus for dacryoliths of the lacrimal excretory and secretory systems. Am J Ophthalmol. 1991;111(5):624–627. doi:10.1016/S0002-9394(14)73709-2
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.