")
Back to Journals » International Journal of General Medicine » Volume 15
Large-Scale Observational Study on the Current Status and Challenges of General Medicine in Japan: Job Description and Required Skills
Authors Miyagami T , Yamada T, Kanzawa Y, Kosugi S, Nagasaki K, Nagano H, Shimizu T , Fujibayashi K, Deshpande GA, Naito T
Received 30 August 2021
Accepted for publication 16 December 2021
Published 29 January 2022 Volume 2022:15 Pages 975—984
DOI https://doi.org/10.2147/IJGM.S336828
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Taiju Miyagami,1 Toru Yamada,2 Yohei Kanzawa,3 Shunsuke Kosugi,4 Kazuya Nagasaki,5 Hiroyuki Nagano,6 Taro Shimizu,7 Kazutoshi Fujibayashi,1 Gautam A Deshpande,1 Toshio Naito1
1Department of General Medicine, Juntendo University Faculty of Medicine, Tokyo, Japan; 2Department of Family Medicine, Graduate School of Medical and Dental Sciences, Tokyo Medical and Dental University, Tokyo, Japan; 3Department of General Internal Medicine, Akashi Medical Center, Hyogo, Japan; 4Department of General Internal Medicine, Iizuka Hospital, Iizuka, Fukuoka, Japan; 5Department of Internal Medicine, Mito Kyodo General Hospital, Ibaraki, Japan; 6Emergency Medicine and General Internal Medicine, Rakuwakai Marutamachi Hospital, Kyoto, Japan; 7Department of Diagnostic and Generalist Medicine, Dokkyo Medical University Hospital, Tochigi, Japan
Correspondence: Toru Yamada
Department of Family Medicine, Graduate School of Medical and Dental Sciences, Tokyo Medical and Dental University, 1-5-45 Yushima, Bunkyo-ku, Tokyo, 1138519, Japan
, Tel +81 3 5803 5229
, Fax +81 3 5803 0276
, Email [email protected]
Purpose: To identify the current ambiguous status of general medicine (GM) and assess current problems and weaknesses for further development of GM.
Patients and Methods: This study adopted an observational design. GM practitioners were selected from the mailing lists of two primary professional associations for Japanese GM doctors. We included physicians currently working in a GM department, those self-described as GM doctors, and those board-certified in family medicine or general internal medicine. Respondents replied to survey questions about their sociodemographic data, job descriptions, and the requisite skills for practice. GM doctors’ job description and required skills were categorized into “clinical,” “management,” “education,” and “research.” Participants (n = 971) were compared based on job descriptions and important skills in each category by facility type, size, and position.
Results: “Clinical” was indicated as the most important category for both job description and important skills, followed by “management,” “education,” and “research.” For job description details, “follow-up outpatient” (35.6%) ranked first for “clinical,” and “resident education” (57.3%) ranked first for “education.” By facility type and size, job description and important skills decreased for clinical and management categories as facility sizes increased; the opposite was true for “education.” “Research” was generally rated low. By position, no significant difference was found in effort or importance given to research.
Conclusion: This study is the first survey on GM physicians across Japan. The results show that while Japanese GM physicians focus on and place importance on clinical practice, they are less involved in research and do not consider research skills to be important. The challenge for the future development of GM lies in research.
Keywords: general medicine doctors, job description, observational study, research skills
Introduction
In Japan, the first department of general medicine (GM) was established in 1976.1,2 Since then, the department of GM has gradually spread, and as of 2017, 86% of university hospitals have a department of GM.3 However, thus far, GM was not recognized as a specialty, and there were no qualifications for GM specialists. Originally, in Japan, once a physician completed a two-year general rotation after obtaining a medical license, they could work in the specialty of their choice without going through a selection or examination process. This training system has changed significantly since 2018. Under the new medical specialty training system starting in 2018, after two years of general rotation, physicians must choose one of the 18 specialties approved by the Japan Medical Specialists Board (JMSB), including internal medicine, surgery, and pediatrics. GM finally received official recognition from JMSB as the 19th area in this new medical specialty training system, and the training program after general rotation started in 2018.
With an increasing number of patients having multiple aging-related problems, more GM doctors are needed in Japan.4 However, only approximately 200 doctors (2% of doctors qualified to apply for specialty training) have applied to the GM specialty training program each year.5,6 One of the reasons for this is that the content of work and career path are unclear and not established.7 The GM department had been established for approximately 50 years, but as mentioned above, it was not recognized as a JMSB certified specialty, and there were several leading societies (currently, Japan primary care association [JPCA] and Japanese society of hospital general medicine [JSHGM] are the two major societies) who had their own definition of GM. Each facility’s GM department had its own role. Therefore, the duties of the GM department at each facility varied, and the training content was not standardized. According to a previous study of Japanese GM doctors’ job description in university hospitals, the job varied greatly among universities: 48.1−53.6% of university hospital GM doctors examined only outpatients, 46.4−51.9% examined inpatients, and 15.9% worked in the emergency department.3,8 Another study reported that GM doctors trained in family medicine (FM) typically worked in clinics or provided visiting care; however, 48.3% worked in hospitals.9
However, one of the most significant reasons for the variation in the content of the GM department’s work among facilities was the abstract definition of general practice proposed by the government. The definition of a general practitioner proposed by the Ministry of Health, Labour and Welfare (MHLW) were those practitioners who are able to cover all stages from preventive medicine to acute care, recovery, chronic care, and end-of-life care, have a holistic view of complex problems ranging from single diseases of individual organ systems to psychosocial problems, handle everything from routine medical care to extraordinary disaster medicine to infectious disease pandemics, have a perspective that can accurately respond to the different needs of different regions, and so on.4,10 Although these defined the comprehensiveness of GM doctors, they were not incorporated into specific requirements. Therefore, GM in Japan has come to include both FM, involving clinics, and hospital medicine (HM), which mainly involves hospitals. The JPCA, one of the two major societies in the field of GM, has proposed definitions for both FM and HM.11 In addition, unlike HM in the US, HM in Japan requires skills in ambulatory and emergency care.12 In order to solve these issues and train GM doctors, the JMSB is now taking the lead, and JPCA and JSHGM are cooperating to develop programs for GM doctors based on their basic medical specialties, as well as their subspecialties, HM and FM. Programs for GM doctors officially started in 2018 under the new medical specialist training system certification, but HM and FM specialists have not yet been officially certified by the JMSB.
Although the development of training programs of GM is progressing, there is little published evidence on the current work content of GM in Japan and what GM doctors consider important. The purpose of this study is to clarify the current status of GM in Japan by surveying the members of the two major societies, JPCA and JSHGM, on the content of their work and what they consider important. We conducted this study to provide awareness regarding the current ambiguous status of GM to young doctors in an easy-to-understand manner and to identify current problems and weaknesses in order to further develop GM.
Materials and Methods
Setting and Participants
For this observational study, we emailed a questionnaire to the members of the JPCA and JSHGM mailing lists from January 28 to March 28, 2020. Inclusion criteria were as follows: respondents were physicians who agreed to participate by responding to the email and (1) were currently working in a GM or GIM department, (2) considered themselves GM doctors, and (3) had JPCA board certification as an FM practitioner or JSIM board certification as a GIM practitioner. There are currently no doctors with JMSB board certification working as a GM; therefore, we chose these board certification holders to include family physician-based and hospitalist-based GM doctors. Residents in a two-year general rotation were excluded because they were not affiliated with any department. Participants who submitted incomplete questionnaires were also excluded.13 We used Research Electronic Data Capture (REDCap)14 to store data online.
Survey Instrument
The items measured in the questionnaire were as follows: gender, age, postgraduate medical school years, academic society memberships (JPCA, JSHGM, or both), whether participants considered themselves to be GM doctors, whether they belonged to a GM department, and whether they were certified from one of the boards of FM or GIM. A multiple-choice questionnaire was also used to ask participants about employer facility type (university hospital, city hospital, or clinic), size, and whether they had other specialty qualifications.
The respondents were asked about their job descriptions and requisite skills as GM doctors. Questions were “Choose the jobs, from first to third, that you usually spend most of your time on from the following items” to determine their job description and “Choose the skills, from first to third, that you consider the most important for GM doctors from the following items” to determine the requisite skills. The items were grouped into four categories: clinical, education, research, and management. (Additional Files 1 and 2). Responses were scored by applying 3 points to the first ranked item, 2 points to the second, 1 point to the third, and 0 points for “not applicable.” This scoring method was created based on Borda count.15 We calculated the average points for each of the four categories. Institutions with 19 or fewer beds were referred to as “clinics” and institutions with 20 or more beds were referred to as “hospitals,” according to the standards of the Ministry of Health, Labour and Welfare.16 For convenience, hospitals with 20−199 beds, 200−399 beds, and over 400 beds were categorized as small, medium-sized, and large hospitals, respectively. In Japan, doctor attend a specialty program for three years and are called “Residents;” people working as staff are called “Attendings,” people working as managers are called “Managers,” and people who do not fit into any of these categories are called “Others.”
Participants reported their board certifications for specialties as defined by the JMSB in 2020, including 19 areas such as internal medicine, surgery, and pediatrics.6 Since there is no JMSB board certification for GM, we also asked participants if they held JPCA’s FM board certification and JSIM’s GIM board certification. This questionnaire was originally developed for this study and has not been published previously.
Data Analysis
Results are presented as medians (interquartile range, IQR) for continuous variables, or prevalence (%) for categorical variables. Comparisons between groups were made using the Steel−Dwass test. All calculations were performed using JMP PRO software, version 13.0 (SAS Institute, Cary, NC, USA), and p values < 0.05 were considered statistically significant.
Ethics
The institutional ethics committee of Juntendo University Hospital approved the research (No.19T7009). The survey was web-based, and only those who agreed to participate could respond. There was no patient or public involvement in this study.
Results
The two mailing lists included 7115 members (JPCA: 5329, JSHGM: 1786). Several participants were members of both associations, but only responded to the questionnaire once. A total of 1367 participants (19.2%) responded to the questionnaire, 971 (13.6%) of whom matched the inclusion criteria (Figure 1).
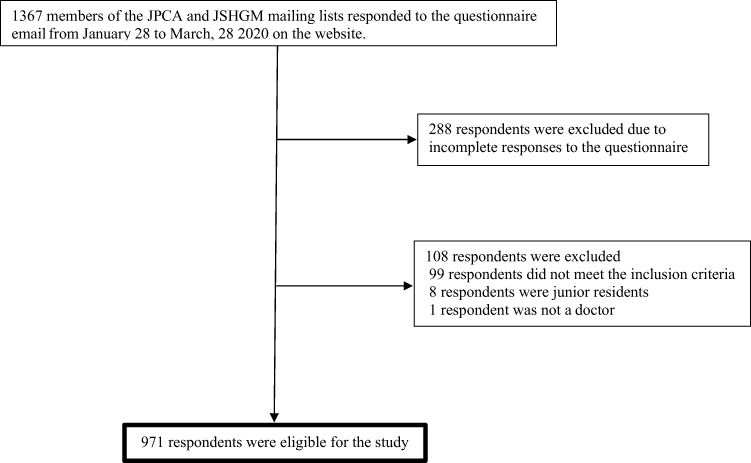 |
Figure 1 Participant Inclusion flow. Abbreviations: JPCA, Japan Primary Care Association; JSHGM, Japanese Society of Hospital General Medicine. |
Interestingly, most participants were male; four-fifths belonged to the JPCA, and of these, 33.0% belonged to both JPCA and JSHGM. Further, most considered themselves GM doctors, and most worked in a GM department. Less than half of the respondents held any medical specialty certification. Approximately half of the participants were employed by city hospitals, and approximately one-third worked in a hospital with more than 400 beds. The participants’ demographics are shown in Table 1.
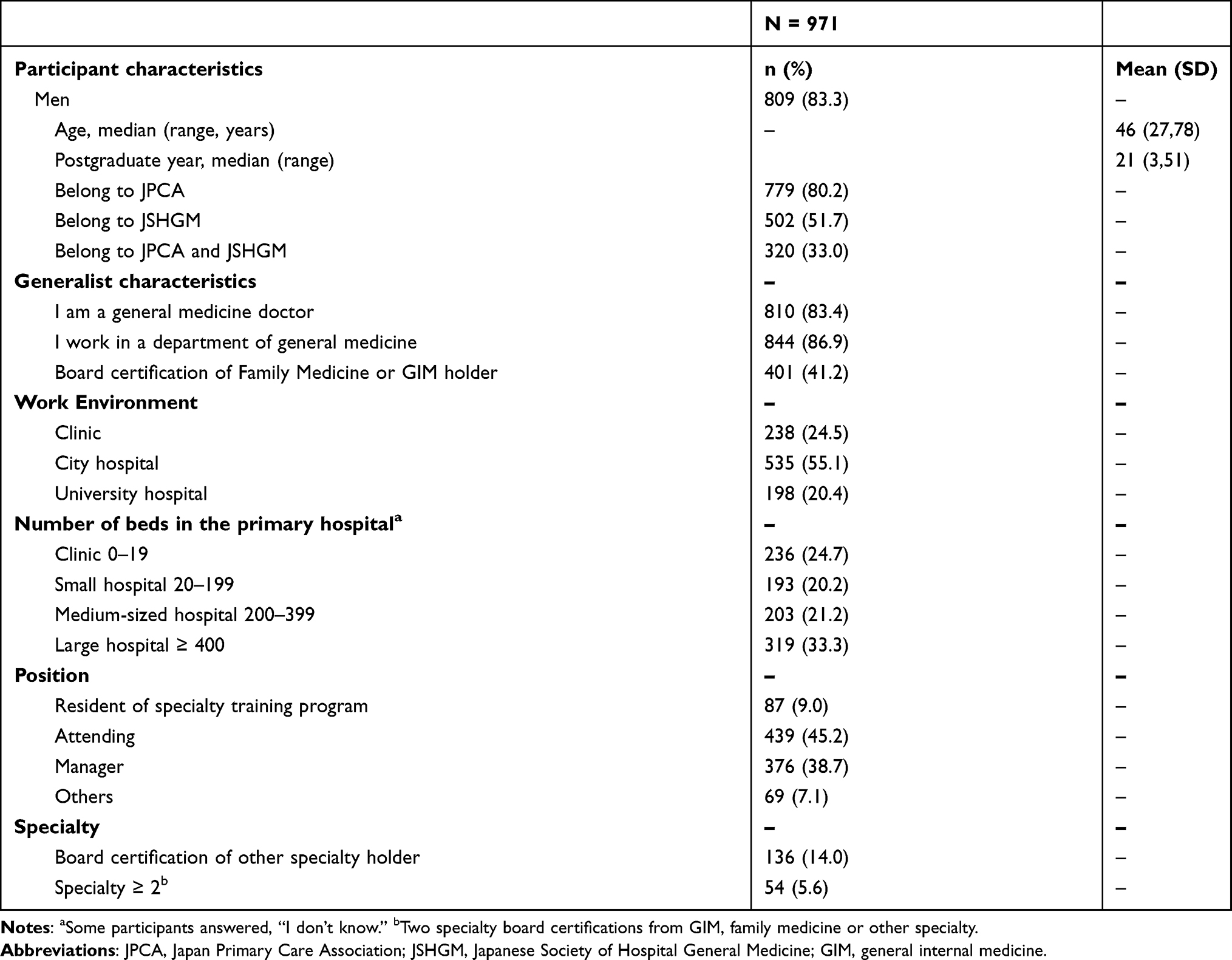 |
Table 1 Participant Characteristics |
Figure 2 shows respondents’ scores for the four categories for job description and requisite skills as GM doctors, including clinical, management, education, and research. Clinical was ranked first, and research was ranked last. There was also a statistically significant difference in the rankings among all groups (p < 0.05; Additional File 3). In the clinical category, the tasks that participants spent the most time on were ward (30.2%), first-visit outpatient (20.7%), follow-up outpatient (35.6%), emergency outpatient (4.9%), and home visit (6.4%; Q14-4 in Additional File 1). As for the educational category, the tasks that participants spent most time on were medical student education (18.8%), resident education (57.3%), and attending doctor education (23.9%; Q14-1~14-3 in Additional File 1).
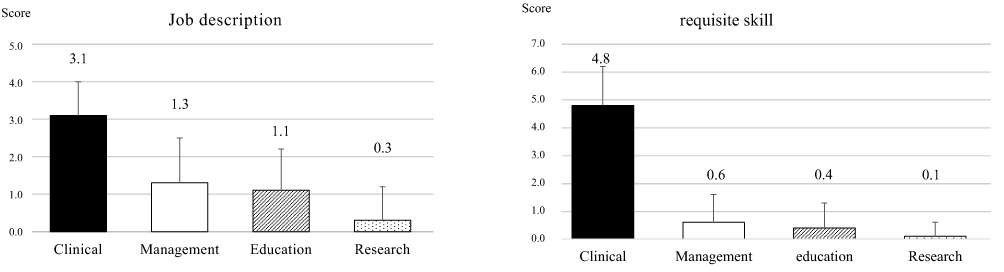 |
Figure 2 General medicine doctors’ job description and requisite skills. Participants’ responses to the items were scored as follows: 3 points to the first ranked item, 2 points to the second, 1 point to the third, and 0 points to “not applicable.” The average score was calculated for each of the four categories and was expressed as mean ± SD. |
Job description was divided into clinical, management, education, and research categories based on facility type, size, and position (Figure 3). Participants who worked in clinics devoted the highest percentage of effort in clinical work, based on facility type and size (3.4 ± 0.9); this tended to decrease as facility size or medical institution level increased. In the clinical category, facility type showed a statistically significant difference among all groups, and facility size showed a statistically significant difference except for small and medium-sized hospitals. In terms of position, residents devoted the highest percentage of effort in clinical work and tended to decrease efforts as their position increased. It showed a statistically significant margin except for attending and managerial roles. Management followed the same trend. In management, facility type showed a statistically significant difference across all groups. In facility size, no statistically significant difference was found between clinics and small hospitals or between medium-sized and big hospitals, but there was a statistically significant difference among all other groups. In position, managers devoted the highest percentage of effort in management work, and this tended to decrease as their position decreased. It showed a statistically significant margin except for resident and attending roles. However, participants from university hospitals and large hospitals devoted the highest proportion of effort to education and research (facility type: education: 1.7 ± 1.2, research: 0.7 ± 1.0; facility size: education: 1.7 ± 1.1, research: 0.5 ± 0.9), which tended to increase as facility size or medical institution level increased. In education, facility type showed a statistically significant difference across all groups. In terms of facility size, there was a significant difference except for clinics and small hospitals. In terms of position, the highest effort was devoted by residents, followed by managers and staff. There were significant differences in effort among different positions except for resident and managerial roles. Facility type showed no statistically significant differences in effort between clinics and city hospitals, but a statistically significant difference among other facility types was observed. In facility size, no statistically significant margin difference was found between clinics and small hospitals, clinics and medium-sized hospitals, and small and medium-sized hospitals; however, a statistically significant difference was found among other facility types in terms of size. Additionally, none of the positions devoted effort to research; there was only a statistically significant difference between attending and managerial roles. Comparisons between groups are shown in Additional File 4.
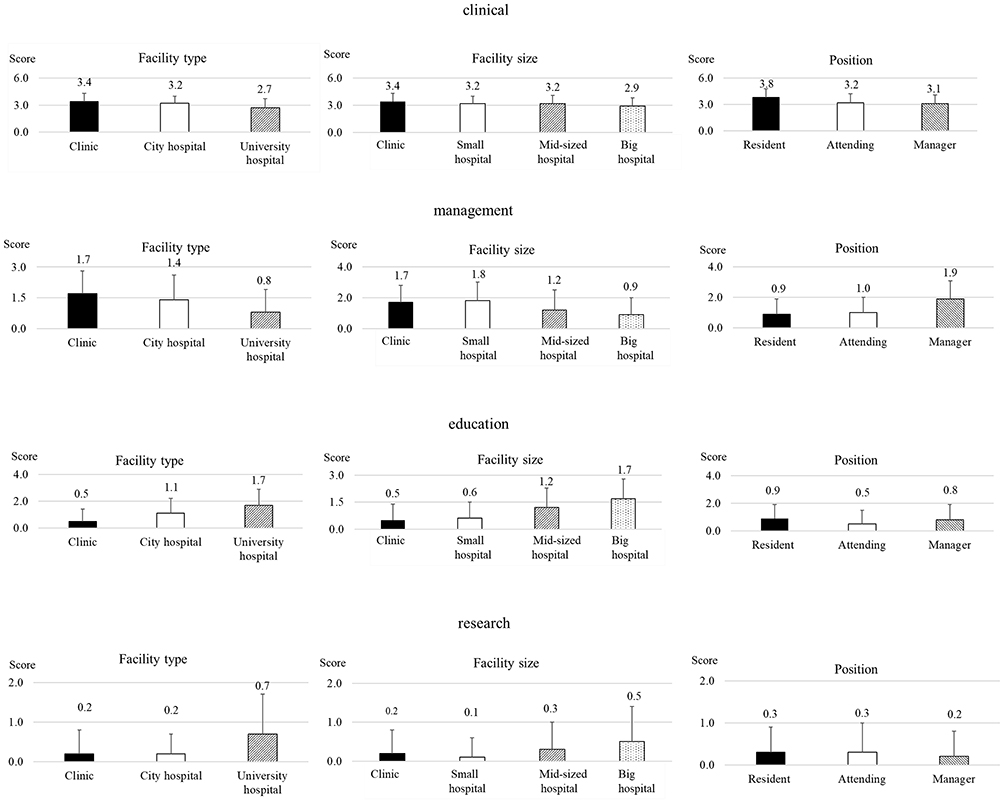 |
Figure 3 Job description by facility type and size. Participants’ responses to the items were scored as follows: 3 points to the first ranked item, 2 points to the second, 1 point to the third, and 0 points to “not applicable.” The average score was calculated for each of the four categories and was expressed as mean ± SD. |
The essential skills necessary for GM doctors were divided into clinical, management, education, and research by facility type and size (Figure 4). Participants working in clinics had the highest level of requisite clinical skills as medical doctors, by facility type and size (5.4 ± 1.0); this tended to decrease as facility size or medical institution level increased, and a statistically significant difference was found among all groups in facility type. In terms of facility size, no statistically significant difference was found between small, medium-sized, and big hospitals, but a statistically significant difference was found among other facilities. In terms of position, resident had the highest level of requisite clinical skills as medical doctors, and no statistically significant difference was found between attending and manager roles; however, a statistically significant difference was found among other roles. Management was clearly more important for city hospitals by facility type, but there was no clear difference by facility size. In terms of position, managerial roles involved the highest level of requisite management skills, and there was a statistically significant difference in terms of position between only clinics and city hospitals. Participants working in university hospitals and large hospitals placed the most value on education (facility type: 0.6 ± 1.1, facility size: 0.7 ± 1.1). In terms of facility type, no statistically significant difference was found between city hospitals and university hospitals, but a statistically significant difference was found between other facilities. In terms of facility size, no statistically significant difference was found between clinics and small hospitals, medium-sized and big hospitals, but a statistically significant difference was found between other facilities. Participants working in university hospitals placed the most importance on research, compared to other groups; however, there were no significant differences by facility type or size among non-university hospitals in terms of value placed in research. In terms of position, no statistically significant difference was found among any of the groups in value placed in research. The comparisons between groups are shown in Additional File 5.
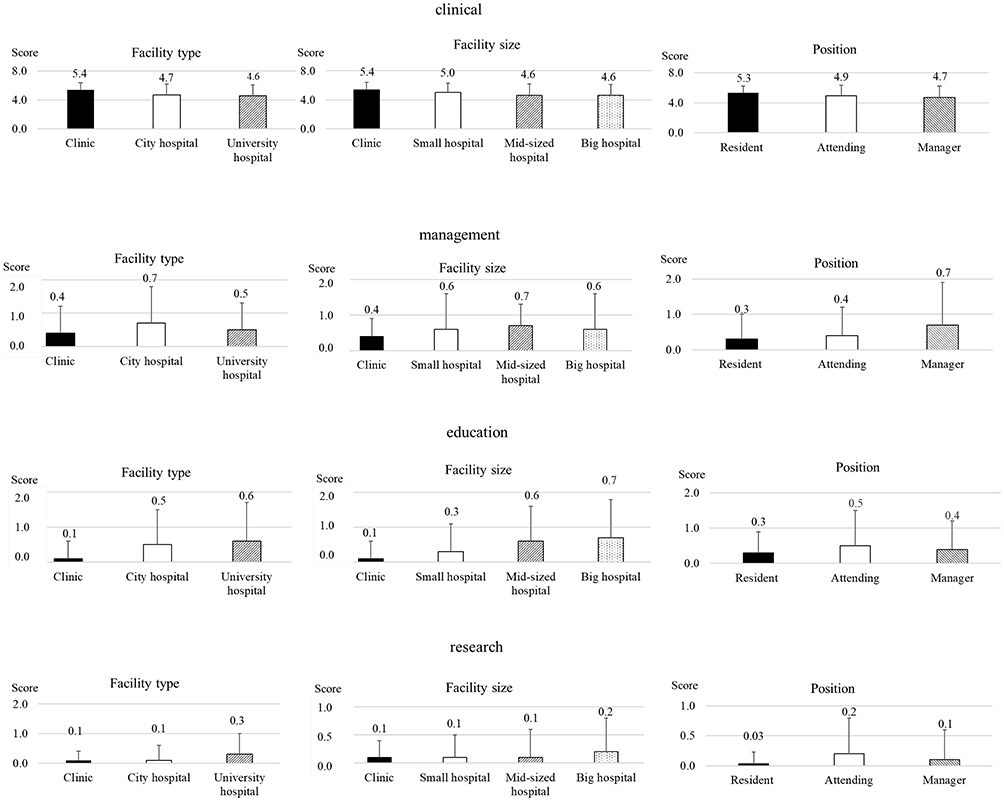 |
Figure 4 Requisite skill by facility type and size. Participants’ responses to the items: 3 points to the 1st ranked item, 2 points to the 2nd, 1 point to the 3rd, and 0 points to “not applicable.” The average was calculated for the points in each of the 4 categories. The score was calculated expressed as mean ± SD. |
Discussion
This study assessed the job description and essential skills for Japanese GM doctors. To the best of our knowledge, this is the largest-ever study of GM doctors in Japan. There were three important findings. First, Japanese GM doctors placed a significantly higher priority on clinical factors related to the job description and requisite skills of a GM doctor than on the other three categories. This trend was not influenced by facility type, size, and position. Second, Japanese GM doctors did not spend much time on research or think research skills are important compared to the other three categories, especially in non-university hospitals. Third, compared by facility type and size, the percentage of clinical and management work tended to decrease as facility size or medical institution level increased. Conversely, the percentage of education and research work tended to increase as facility size or medical institution level increased. Additionally, we found that regardless of the position, they do not perform research work and do not consider it to be important.
Compared with the clinical category, the research category was not regarded as essential; GM doctors in Japan did not spend as much time on research as on other categories. Job description and requisite skills regarding research were not significantly different among non-university hospitals, regardless of type, size, and position and were clearly rated lower than the other categories. A previous study revealed that only 38.9% of doctors who have JPCA board certification of FM had written an original article.9 GM doctors may not have much interest in research because of their population background. In a survey of Japanese medical students, those who chose GM tended to have interest in community medicine and not in research.17 In other countries, previous studies reported that students interested in research tended to choose not to work in a GM department,18 while other studies suggest that the small role played by research in this field is a major reason for doctors choosing not to opt for GM.19 In the US, family physicians and hospitalists place a high value on research, but do not typically engage in it.20–22 Although there are some differences in the importance of research between GM doctors in Japan and family physicians and hospitalists in the US and other countries, they tend to do less research. When considering the future development of GM, research work involving the acquisition of funds is said to be indispensable.23 In fact, hospitalists in the US also saw a six-fold increase in the number of papers published between 2006 and 2013.24 Another report from Japan suggests that it is important for GMs in university hospitals to promote research work.25 Therefore, one of the challenges GMs face is the need to develop their research work and allocate time to conduct research. In order to increase research work, it is important to have a mentor and secure time for research (25% of daily work) and to conduct it effectively.24
Contrary to the clinical category, the percentage of educational work performed and its importance tended to increase as facility size or medical institution level increased. Previous studies showed that Japanese teaching hospitals with a GM department scored higher on resident knowledge than those without a GM department, and hospital size and the number of physicians were positively correlated with resident knowledge during a two-year general rotation.26,27 These findings suggest that GM doctors working in hospitals have a high affinity for education.
This study has several limitations. The response rate for this survey was low at 13.6%. As 33.0% of the respondents participated in both conferences, the actual number of participants may also be lower than the total number of 7115 mailing list participants in both conferences. Therefore, the response rate may be a little higher than the actual recorded rate. The results of this survey may be subject to bias caused by participants who did not respond (non-responder bias), and it is difficult to conduct additional surveys to track and follow-up responses because of the anonymity of the study. In order to assess the current status of GM in Japan more accurately, further large-scale surveys based on this study are needed. Another limitation is the low amount of research activity for GM doctors. It was clear that GM doctors in Japan did not spend time on research and were not interested in work related to research; however, it was not clear whether this was lower than that in other specialties. Although a previous study reported that research comprised 15% of the total work performed in emergency departments, we could not find data for other specialties as a whole.28 We did not assess board-certified GM doctors; therefore, further study is needed to assess them in the future.
Conclusions
This study is the first large-scale survey of GM physicians in Japan. The results showed that GM physicians in Japan place importance and focus on clinical practice. On the contrary, we found that they are less involved in research and place less importance on their research skills. The challenge for the future development of GM lies in research, and it is important to conduct more research.
Abbreviations
FM, family medicine; GIM, general internal medicine; GM, general medicine; HM, hospital medicine; JMSB, Japanese Medical Speciality Board; JPCA, Japanese Primary Care Association; JSHGM, Japanese Society of Hospital General Medicine; JSIM, Japanese Society of Internal Medicine.
Data Sharing Statement
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Ethics Approval and Informed Consent
The institutional ethics committee of Juntendo University Hospital approved the research (No.19T7009). The survey was web-based, and only those who agreed to participate could respond. There was no patient or public involvement in this study.
Acknowledgments
We are grateful to Dr. Hiroyuki Terukina of the Department of Human Pathology, Juntendo University Faculty of Medicine for helpful discussions regarding the case. We would like to thank Editage (www.editage.com) for English language editing. The authors work as a general practice in Japan and are deeply involved in both JPCA and JSHGM. Therefore, it would be difficult to conduct a study on a similar scale in Japan.
Funding
This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.
Disclosure
The authors have no relevant financial or non-financial interests to disclose.
References
1. Fujinuma H. Textbook of Generalist Medicine Family Medicine. Ver 3. Tokyo: Kaishorin; 2019.
2. Ishizuka T. Specialists internal medicine and subspecialties. Nihon Naika Gakkai Zasshi. 2008;97(5):1130–1134. doi:10.2169/naika.97.1130
3. Takeoka H, Horibata K, Masui S, Ajisaka K, Nabeshima S. Trends in departments of general medicine in university hospitals in Japan searched from websites. Med Bull Fukuoka Univ. 2017;44:81–86.
4. Ministry of Health, Labour and Welfare. Report of the study group on the way forward for medical specialists; 2013. Available from: https://www.mhlw.go.jp/stf/shingi/2r985200000300ju.html.
5. Ministry of Health, Labour and Welfare. Announcement of successful completion of the 112th national medical examination; 2019. Available from: https://www.mhlw.go.jp/general/sikaku/successlist/2018/siken01/about.html.
6. Ministry of Health, Labour and Welfare. The 5th medical council of the doctor specialized subcommittee training of doctor in the year of Reiwa; 2020. Available from: https://www.mhlw.go.jp/stf/newpage_10761.html.
7. Tsuchida T, Ie K, Nishisako H, Matsuda H. Why did you choose not to be a generalist? A qualitative study about career decision-making among physicians who were interested in general practice but chose to be a specialist. J Gen Fam Med. 2019;42:134–140. doi:10.14442/generalist.42.134
8. Sasaki Y, Yoshihisa U, Takahiro S, et al. The actual condition of medical treatment in university hospital general medical department: what is required for general medical department of university hospital. J Japan Hosp Gen Med Assoc. 2015;9:1–8.
9. Takahiro T, Akiko M, Hiroshi O, Manabu K, Hiroki O, Tesyu K. A survey of the activities of family medicine specialists. J Gen Fam Med. 2016;39:243–249.
10. Japan Medical Specialists Organization. What is a general medicine doctor?; 2021. Available from: https://jmsb.or.jp/sogo/.
11. Kaneko M, Matsushima M. Current trends in Japanese health care: establishing a system for board-certificated GPs. Br J Gen Pract. 2017;67(654):29. doi:10.3399/bjgp17X688669
12. Japan Primary Care Association. Hospital general medicine trial program; 2014. Available from: https://www.primary-care.or.jp/nintei_ge/index.html.
13. Ministry of Health, Labour and Welfare. Changes in junior resident clinical training system; 2018. https://www.mhlw.go.jp/topics/bukyoku/isei/rinsyo/hensen/.
14. Blumenberg C, Barros AJ. Electronic data collection in epidemiological research. The use of REDCap in the Pelotas birth cohorts. Appl Clin Inform. 2016;7(03):672–681. doi:10.3402/meo.v21.29448
15. Black D. Partial justification of the Borda count. Public Choice. 1976;28(1):1–15. doi:10.1007/BF01718454
16. Ministry of Health, Labour and Welfare. Summary of the 2013 medical facilities (Movement) survey and hospital report; 2014. Available from: https://www.mhlw.go.jp/toukei/saikin/hw/iryosd/13/.
17. Kawamoto R, Ninomiya D, Kasai Y, et al. Factors associated with the choice of general medicine as a career among Japanese medical students. Med Educ Online. 2016;21(1):29448. doi:10.3402/meo.v21.29448
18. Tanriover O, Hidiroglu S, Akan H, et al. A qualitative study on factors that influence Turkish medical students’ decisions to become family physicians after the health transformation program. N Am J Med Sci. 2014;6(6):278–283. doi:10.4103/1947-2714.134374
19. Barber S, Brettell R, Perera-Salazar R, Greenhalgh T, Harrington R. UK medical students’ attitudes towards their future careers and general practice: a cross-sectional survey and qualitative analysis of an Oxford cohort. BMC Med Educ. 2018;18(1):160. doi:10.1186/s12909-018-1197-z
20. Harrison R, Hunter AJ, Sharpe B, Auerbach AD. Survey of US academic hospitalist leaders about mentorship and academic activities in hospitalist groups. J Hosp Med. 2011;6(1):5–9. doi:10.1002/jhm.836
21. Nichani S, Crocker J, Fitterman N, Lukela M. Updating the core competencies in hospital medicine—2017 revision: introduction and methodology. J Hosp Med. 2017;12(4):283–287. doi:10.12788/jhm.2715
22. Hinami K, Whelan CT, Miller JA, Wolosin RJ, Wetterneck TB. Job characteristics, satisfaction, and burnout across hospitalist practice models. J Hosp Med. 2012;7(5):402–410. doi:10.1002/jhm.1907
23. Friedman RH, Alpert JJ, Green LA. Strengthening academic generalist departments and divisions. J Gen Intern Med. 1994;9(Suppl S1):S90–98. doi:10.1007/BF02598123
24. Dang Do AN, Munchhof AM, Terry C, Emmett T, Kara A. Research and publication trends in hospital medicine. J Hosp Med. 2014;9(3):148–154. doi:10.1002/jhm.2148
25. Watari T, Tago M, Shikino K, et al. Research trends in general medicine departments of university hospitals in Japan. Int J Gen Med. 2021;14:1227–1230. doi:10.2147/IJGM.S306543
26. Mizuno A, Tsugawa Y, Shimizu T, et al. The impact of the hospital volume on the performance of residents on the general medicine in-training examination: a multicenter study in Japan. Intern Med. 2016;55(12):1553–1558. doi:10.2169/internalmedicine.55.6293
27. Shimizu T, Tsugawa Y, Tanoue Y, et al. The hospital educational environment and performance of residents in the general medicine in-training examination: a multicenter study in Japan. Int J Gen Med. 2013;6:637–640. doi:10.2147/IJGM.S45336
28. Meislin HW, Spaite DW, Valenzuela TD. Meeting the goals of academia: characteristics of emergency medicine faculty academic work styles. Ann Emerg Med. 1992;21(3):298–302. doi:10.1016/S0196-0644(05)80891-1
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.