")
Back to Journals » Clinical Ophthalmology » Volume 12
Lack of relationship between cigarette smoking and alcohol use with dysplasia grade in ocular surface squamous neoplasia
Authors Early AD, Adelson S, Miller CJ, Mauger TF
Received 20 February 2018
Accepted for publication 9 May 2018
Published 1 October 2018 Volume 2018:12 Pages 1901—1904
DOI https://doi.org/10.2147/OPTH.S165968
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Alison D Early, Sarah Adelson, Craig J Miller, Thomas F Mauger
Department of Ophthalmology, The Ohio State University Havener Eye Institute, Columbus, OH, USA
Objective: To evaluate smoking and alcohol use as risk factors for higher-grade dysplasia in a population of patients with histopathologically proven ocular surface squamous neoplasia.
Materials and methods: This is a retrospective chart review of data extracted from a database comprising demographic information and medical diagnosis information based on International Classification of Disease codes. Outcome measures were analyzed using the Wilcoxon two-sided test, a non-parametric t-test.
Results: Database review yielded 35 patients with ocular surface squamous neoplasia lesions proven by histopathologic analysis. The mean age was 64.51 years with SD 17.54 years. Patients were 28.57% female and 71.43% male. Nearly all patients were White (88.57%), and 5.71% were African American, 2.86% Hispanic, and 2.86% Other. There was no significant difference in dysplasia grade between smokers and non-smokers (P=0.7044), those who used alcohol vs did not use alcohol (P=0.2470), those who used tobacco and alcohol vs those who did not (P=0.5117), and those who used either tobacco or alcohol vs those who did not (P=0.8259).
Conclusion: No statistically significant relationship was found between high-grade dysplasia and cigarette smoking, alcohol use, or both cigarette smoking and alcohol use.
Keywords: ocular surface squamous neoplasia, corneal dysplasia, conjunctival dysplasia, carcinoma in situ, squamous cell carcinoma, ocular surface tumors
Introduction
Ocular surface squamous neoplasia (OSSN) is a spectrum of disease ranging from squamous dysplasia to invasive squamous cell carcinoma (SCC). Dysplasia is graded according to the degree of involvement of the involved epithelium, with mild dysplasia confined to the lower third of the conjunctival epithelial thickness, moderate dysplasia extending into the middle third, and severe dysplasia involving the upper third. Full-thickness involvement is considered carcinoma in situ (CIS) and infiltration through the basement membrane is invasive OSSN or SCC.1 Previous literature has investigated the risk factors associated with the development of OSSN and the data support cigarette smoking as one of these risk factors.2 To date, no studies have examined whether current or prior history of cigarette smoking is associated with higher-grade dysplasia on histopathologic analysis. The purpose of this study was to examine whether a history of cigarette smoking is associated with higher-grade dysplasia in patients with OSSN.
Materials and methods
This is a retrospective case series examining data collected between January 2009 and August 2014. Data were extracted by searching by International Classification of Disease 9 (ICD-9) codes commonly used to code conjunctival and corneal lesions (Table 1). Each chart matching one of these codes was reviewed and data were recorded including the subjects’ smoking history and the histopathologic grading following excision of the conjunctival lesion. Only patients of anterior segment surgeons from The Ohio State Havener Eye Institute were included in the review. The dysplasia grading schematic used for statistical analysis included mild, moderate, and severe dysplasia, and CIS or SCC. Several pathology reports were indeterminate, with diagnoses such as “mild–moderate dysplasia”. In these cases, the lesion was classified in the higher-grade category of dysplasia (eg, a lesion graded as “mild–moderate dysplasia” would be considered moderate dysplasia for the purposes of this study), as these specimens contained some features of higher-grade dysplasia on histopathologic sections. This variability in grading can be attributed to different schematics used by different pathologists.
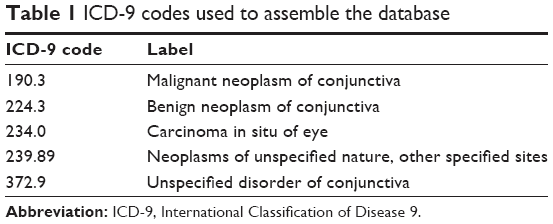 | Table 1 ICD-9 codes used to assemble the database |
Demographic data for each subject, including age, sex, and race, were recorded. Tobacco and alcohol use histories were categorically recorded as either yes, no, or unknown. Analysis of demographic variables was undertaken to determine the average age of subjects, percent of subjects of male and female sex, and percent of subjects identifying their race as White, African American, Asian, or Other. The Wilcoxon two-sample test was used to determine if an association existed between higher-grade dysplasia and cigarette smoking, alcohol use, or both cigarette smoking and alcohol use. This is a retrospective study for which the aim is to examine whether there is an association between cigarette smoking and alcohol use on dysplasia grade in OSSN. All data collected were existing, and the subjects were seen in the Department of Ophthalmology. As such, a waiver of consent process was submitted and approved by The Ohio State University Institutional Review Board. The Ohio State University Wexner Medical Center Institutional Review Board approved the retrospective review of charts for this study, and the methods adhered to the tenets of the Declaration of Helsinki as well as being compliant with the Health Insurance Portability and Accountability Act.
Results
The retrospective chart review based on charts identified using the ICD-9 codes as listed in Table 1 yielded 35 patients with OSSN lesions proven by histopathologic analysis. The mean age was 64.51 years with SD 17.54 years. Females made up 28.57% of the cohort (n=10) and males made up 71.43% (n=25). Nearly all patients were White (88.57%, n=31), with 5.71% African American (n=2), 2.86% Hispanic (n=1), and 2.86% Other (n=1), as shown in Table 2.
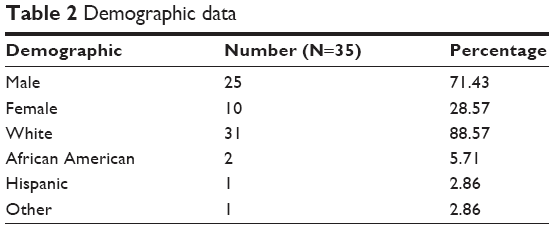 | Table 2 Demographic data |
For the purposes of statistical analysis, each dysplasia grade was assigned a numerical value in order of increasing severity, from zero (no dysplasia) to four (CIS and SCC). CIS and SCC were categorized together due to some ambiguity with several pathology reports reading “SCC in situ”. A Wilcoxon two-sided non-parametric t-test (Table 3) showed no significant difference in dysplasia grade between smokers and non-smokers (P=0.7044). The same test was used to evaluate the difference in dysplasia grade in patients who used alcohol (P=0.2470), who used tobacco and alcohol (P=0.5117), and who used either tobacco or alcohol (P=0.8259). No statistically significant difference in dysplasia grade was found in any of these groups. This test was chosen to assess for difference in population mean ranks between paired samples.
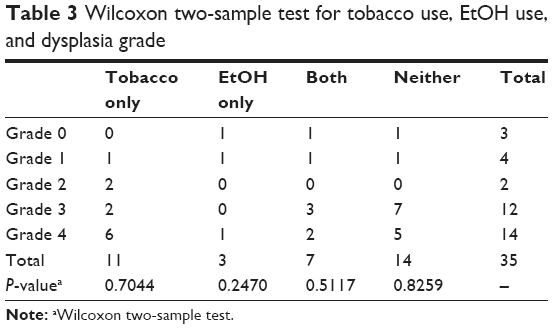 | Table 3 Wilcoxon two-sample test for tobacco use, EtOH use, and dysplasia grade |
Discussion
OSSN is the third most common oculo-orbital tumor behind melanoma and lymphoma1 and the most common ocular surface tumor.3,4 The term OSSN was coined in 1995 by Lee and Hirst,5 and further exploration into the characteristics, risk factors, management strategies, and outcomes has followed. Previous studies have demonstrated cigarette smoking as an accepted risk factor for OSSN. Other known risk factors include advanced age, male sex, ultraviolet light exposure, human immunodeficiency virus, and human papilloma virus.1 A large retrospective analysis of 389 excised OSSN lesions by Galor et al found that higher-grade lesions (CIS and SCC) are at increased risk of recurrence as compared to dysplasia grade lesions.6 Review of the existing literature showed that no studies to date have examined whether a smoking history is associated with development of a higher-grade lesion at the time of excision and histopathologic analysis. Our sample of 35 patients with histopathologically proven OSSN failed to identify a statistically significant relationship between history of smoking and higher-grade OSSN.
OSSN lesions are graded by the extent of involvement of the dysplastic epithelium. Mild dysplasia describes less than one-third of the tissue thickness occupied by abnormal cells, moderate dysplasia is up to two thirds involvement, and severe dysplasia is near full-thickness involvement. CIS indicates full-thickness involvement, and SCC or invasive OSSN indicates a breach of the basement membrane and invasion into deeper tissue. Higher pathologic grade has been shown to be a significant predictor of recurrence.6 Recurrence rates of OSSN have been reported at between 15% and 52% of lesions,7 with highest recurrence seen with CIS and SCC. Furthermore, recurrent lesions may have the tendency to be more aggressive and can lead to complications including metastasis and death.4
Continued exploration into the disease entity of OSSN has delved into particular qualities for risk stratification. Cigarette smoking is known to portend increased risk of head and neck cancers, many of which are SCCs of the oral cavity, pharynx, and larynx.8 Previous epidemiological studies show an association with both tobacco and alcohol use and risk of head and neck cancers, and even that alcohol may potentiate the effects of tobacco in regard to risk of these tumors.8 Similarly, smoking has been associated with the risk of OSSN; however, to date, no analyses comparing the history of prior or current cigarette smoking with the grade of dysplasia on histopathologic analysis have been carried out.
Our sample was consistent with previous research showing a higher incidence of OSSN in males than females. Some have suggested that this may be partially explained by differences in rates of cigarette smoking and alcohol consumption between men and women.8
As OSSN is not a commonly encountered diagnosis, many studies including this one are of relatively small sample sizes. Incidence is estimated to be ~20 cases per 1 million people per year.9 This review is limited to data obtained from only patients of the Anterior Segment Division of The Ohio State University Havener Eye Institute, which were further refined to include only those whose pathology reports were available for review. Several patients who carried one of the ICD-9 codes used in data collection were excluded if there was no pathology report available, typically because the excision occurred prior to use of the current electronic medical record or was performed at an outside institution. Cigarette smoking and alcohol use history were self-reported by patients, which could be, therefore, underreported. Additionally, smoking history and alcohol use were both considered binary variables, as data for number of pack-years or quantity or duration of alcohol use were not available for all subjects. Our population of patients may not be representative of the general population, as it was predominantly White males with an average age of 63.51 years. In this sample of 35 patients, 18 had a documented smoking history while 17 denied history of cigarette smoking. According to the current information available from the United States Center for Disease Control, in 2014, ~17 per 100 adults in the US currently identified as cigarette smokers.9 A study with a large population of patients following surgical excision of OSSN lesions with available pathology reports and a more detailed substance use history including the number of pack-years of cigarette smoking, current smoking status, number of weekly alcoholic beverages, and number of years of alcohol use may have stronger statistical power. Smoking and alcohol use have been shown to be risk factors for other head and neck SCCs, so continued investigation into their independent or combined influence on OSSN would further add to the literature.
Disclosure
The authors report no conflicts of interest in this work.
References
Basti S, Macsai MS. Ocular surface squamous neoplasia: a review. Cornea. 2003;22(7):687–704. | ||
Mcclellan AJ, Mcclellan AL, Pezon CF, et al. Epidemiology of ocular surface squamous neoplasia in a veterans affairs population. Cornea. 2013;32(10):1354–1358. | ||
Gichuhi S, Sagoo MS, Weiss HA, Burton MJ. Epidemiology of ocular surface squamous neoplasia in Africa. Trop Med Int Health. 2013;18(12):1424–1443. | ||
Kiire CA, Srinivasan S, Karp CL. Ocular surface squamous neoplasia. Int Ophthalmol Clin. 2010;50(3):35–46. | ||
Lee GA, Hirst LW. Ocular surface squamous neoplasia. Surv Ophthalmol. 1995;39(6):429–450. | ||
Galor A, Karp CL, Oellers P, et al. Predictors of ocular surface squamous neoplasia recurrence after excisional surgery. Ophthalmology. 2012;119(10):1974–1981. | ||
Dandala PP, Malladi P, Kavitha. Ocular Surface Squamous Neoplasia (OSSN): a retrospective study. J Clin Diagn Res. 2015;9(11):NC10–NC13. | ||
Seijas-Tamayo R, Fernández-Mateos J, Adansa Klain JC, et al. Epidemiological characteristics of a Spanish cohort of patients diagnosed with squamous cell carcinoma of head and neck: distribution of risk factors by tumor location. Clin Transl Oncol. 2016;18(11):1114–1122. | ||
Li AS, Shih CY, Rosen L, et al. Recurrence of ocular surface squamous neoplasia treated with excisional biopsy and cryotherapy. Am J Ophthalmol. 2015;160(2):213–219. |
 © 2018 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2018 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.