")
Back to Journals » Adolescent Health, Medicine and Therapeutics » Volume 14
Knowledge of Sexual and Reproductive Health Rights Among University Students: A Cross-Sectional Study in Southeast Ethiopia
Authors Kene C, Geta G , Ejigu N, Desta F
Received 4 November 2022
Accepted for publication 21 December 2022
Published 5 January 2023 Volume 2023:14 Pages 1—12
DOI https://doi.org/10.2147/AHMT.S394883
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Alastair Sutcliffe
Chala Kene,1 Girma Geta,1 Neway Ejigu,1 Fikreab Desta2
1Madda Walabu University, School of Health Science, Department of Midwifery, Bale Goba, Ethiopia; 2Madda Walabu University, School of Health Science, Department of Public Health, Bale Goba, Ethiopia
Correspondence: Chala Kene, Email [email protected]
Background: In many situations, it can still be challenging to talk about sexual and reproductive health rights, and the little scientific research available indicates that university students have a poor understanding of these issues. Therefore, the aim of this study was to assess the knowledge of sexual and reproductive health rights among university students in southeast Ethiopia.
Methodology: From February to March 2022, 483 study participants took part in an institutionally based cross-sectional study. The study participants were chosen using a SRS method. EpiData version 4.6.2.0 was used to enter data, and SPSS version 26.0 was used to analyze it. A bivariate and multivariable binary logistic regression model was used to identify factors associated with SRHR knowledge. The odds ratio and a 95% confidence interval were used to calculate the significance level.
Results: The optimal level of knowledge on SRHR was discovered to be 52.1% [95% CI (47.32– 55.08)] among university students in southeast Ethiopia. The multivariate binary logistic analysis indicated that being urban in the origin of residency [AOR=1.52, 95% CI (1.02– 1.14)], being a health student [AOR= 12.21, 95% CI (7.27– 14.88)], attending secondary school in private [AOR=6.12, 95% CI (1.02– 1.14)], accessibility of a RH club on campus [AOR=6.12, 95% CI (1.02– 1.14)] and participating in RH club [AOR=3.95, 95% CI (3.47– 5.90)] to be variables that are strongly related to the optimal level of knowledge.
Conclusion and Recommendation: Four out of ten students had poor knowledge of SRHR. The variables associated with a high level of knowledge about SRHR were urban residency, health students, attending a private secondary school, the availability of a RH club on campus, and participation in a RH club. Including sexual education in the non-health department’s course, establishing RH clubs on campus, and encouraging participation of students in these clubs are recommended.
Keywords: university students, knowledge, sexual and reproductive health privileges
Background
It is said that everyone has the freedom to make decisions about their own sexuality and reproduction, regardless of their age, gender, or other traits, as long as they also respect the rights of others.1 Since the International Conference on Population and Development (ICPD) held in Cairo in 1994, human rights legal standards have significantly advanced, and those involved in sexual and reproductive health (SRH) programming have largely become important rights to be realized.2 These rights are based on the recognition of all individuals’ basic human rights, which include the right to access information and services to support these choices and promote sexual and reproductive health rights (SRHR).1,3
Due to the fact that the majority of university students are young adults, they require extensive sex education in order to learn about SRHR and how to preserve their rights all throughout their life.4 Their characteristic early sexual initiation, high-risk sexual behaviors, and insufficient levels of awareness about how to safeguard their sexual health demonstrate the need for sex education.5 Formal education on sexuality and reproductive health (RH) is restricted to biology and science syllabi and does not address all topics related to sexual and reproductive health rights in general.6 Because of hurdles including shame, guilt, embarrassment, not wanting friends and family to know, confidentiality, and fear of not being believed, as well as a lack of understanding, individuals are still unable to cope with reproductive-related violations7 and partially due to their lack of knowledge and experience regarding sexuality-related issues, especially the legal tools that would give them the chance to assert and defend their sexuality-related rights.6
Due to the enormous taboo that surrounds it and is derived from culture, religion, tradition, and the very personal nature of its several subtopics, sexual and reproductive health rights continue to be a topic that is challenging to discuss in many circumstances.8 Despite the fact that it is crucial for everyone at all stages of life, sexual and reproductive health. However, far too many individuals particularly young people, males, and poor women in developing nations like Ethiopia are denied the right to sexual and reproductive health.9 Many sexually active young women believe they are unable to discuss or regulate certain aspects of their sexual conduct as a result.10 Evidence suggests that most young people are not even aware of the extent to which their sexual rights are being violated; worse yet, they continue to be unaware of where they can turn for legal or social advice;5 and the poor quality of rights-based interventions for sexual and reproductive health rights reported in low and middle-income countries like Ethiopia.11
As a result, the issue continues to be a major concern for university students, with limited studies indicating that their knowledge of sexual and reproductive health rights is grossly inadequate. In Nepal, for example, the mean level of knowledge about reproductive and sexual health rights was barely more than fifty percent (51.12%).12 It was around 60.3% in Ikeja and 62.1%% in Ikorodu, Nigeria,13 and Ethiopian university students’ average level of sexual and reproductive health rights knowledge ranged from a very low 16.4% to 57.7%.14–19
According to studies, different backgrounds and other related variables influence students’ knowledge of sexual and reproductive health rights. For instance, according to studies conducted among university students, urban resident,15,19 information and education faculty,19 availability of reproductive health service in the campus clinic,19 attending high school in private schools,15 being student of faculty of health sciences,14–16 participation in reproductive health clubs,15,24 utilization of reproductive health services15 and discussing sexual issues with someone else14,15,24 were all significantly related to knowledge on sexual and reproductive health rights.
Although 179 nations, including Ethiopia, agreed to take action for universal access to sexual and reproductive health (SRH), the program’s development has been sluggish.20 In order to address the needs of adolescence through a holistic approach, the Ethiopian Ministry of Health designed programs and policies that target vulnerable young people and those at risk of irreversible harm to their reproductive health and rights by recognizing and diversifying services with age, sex, life stage, and vulnerability status,21 yet unsatisfactory implementation of these programs and policies in practice was looked over in public institutions like universities.
In Ethiopia, a vast number of the population were reported as adolescents, in which most of the university students fell into this age group. Despite the fact that the country has over 40 governmental universities, there have been few studies on the level of knowledge on SRHR at the university level. In addition, from the findings that have been observed so far, the issue of reproductive and sexual rights remains unsatisfactory. As a result, the purpose of this study was to determine the level of knowledge on SRHR among regular undergraduate students at Madda Walabu University.
Methodology
Study Duration and Design
From February -March 2022, an institutional-based cross-sectional study was conducted at Madda Walabu University.
Study Area
The research was carried out on undergraduate regular students at Madda Walabu University. Among the universities in the nation, Madda Walabu University was chosen by lottery method. The university was founded in 2006 and is located in Bale Zone, in the town of Robe, about 430 kilometers from Addis Ababa, the capital city. The university currently has 46 undergraduate and 28 postgraduate programs according to data obtained from the registrar’s record office. It currently has 11,000 regular undergraduate students on three campuses: Robe, Goba, and Shashamene.22
Population
The source population consisted of all regular undergraduate students at Madda Walabu University, while the study population consisted of randomly selected students who were present in class at the time of data collection. This study included all regular undergraduate students at Madda Walabu University, but students who were ill or transferred in or out during the data collection period were excluded.
Sample Size Calculation
The sample size was calculated using a single population proportion formula, assuming 52.2% knowledge of sexual and reproductive health rights,16 a 95% confidence interval (CI), and a 5% margin of error. N= (1.96)2 0.522(0.478)/ (0.05)2=383. The final sample size was 483, after accounting for a 5% non-response rate and the design effect of 1.2.
Sampling Procedure
The participants in the study were chosen using a multistage stratified sampling procedure. To properly allocate the sample size, the MWU registrar’s office first verified the campus number and number of students on each campus. As a result, during the study period, the three campuses, namely Goba, Shashamene, and Robe, had approximately 700, 500, and 9800 regular undergraduate students, respectively. After determining the number of students on each campus, samples were assigned to each campus based on the number of undergraduate students enrolled during the study period. Consequently, the campuses in Goba, Shashamene, and Robe each contributed 31, 22, and 430 students, respectively. The students were then split up into colleges, schools, and departments. Students were then further stratified by class year under particular colleges, schools, and departments. Finally, systematic random sampling was performed utilizing a student list obtained from the registrar as a sampling frame per chosen parts every 22 intervals.
Variables
Socio-demographic factors such as place of residence, monthly stipend from family and relatives, attending secondary school in private schools, being a student’s faculty of health science, and reproductive health-related factors such as participation in reproductive health clubs, utilization of reproductive health services, and discussing sexual issues with someone else were study variables, while level of knowledge on sexual and reproductive health rights was an outcome variable. A total of thirteen questions about sexual and reproductive health rights were asked. For those who answered “yes”, [correct] the value 1 is assigned, and for those who answered “no”, [incorrect] the value 0 is assigned. The questions in the opposite order were recoded. The values were then computed. Participants with at least a mean level of knowledge on sexual and reproductive health rights out of 13 points were classified as having good knowledge, while those with less were classified as having poor knowledge.
Tools and Procedures for Data Collection
Data was collected using a self-administered questionnaire after the classroom was properly set up. A questionnaire was developed from different literature pertinent to the topic of interest.9,15,17–19 An English version tool was used to collect information from the participants, because English is the language of instruction in higher education. The questionnaire was divided into three parts. The first section was used to evaluate the study participants’ socio-demographic characteristics. The second section was used to assess study participants’ use of reproductive health services and sexual experience. The third section assessed participants’ knowledge of sexual and reproductive health rights. The outcome variable was measured using a 13-question survey with yes/no options. For those who answered “yes”, the value 1 is assigned, and for those who answered “no”, the value 0 is assigned. The questions in the opposite order were recoded. The values were then computed, and a score of at least mean or higher was considered to indicate a good level of knowledge about SRHR. To help with data collection, six data collectors and six supervisors were assigned.
Data Quality Control
A pretest was performed on 5% of the sample size to improve the clarity, ease of understanding, and simplicity of the tool messages prior to data collection on sections that were not re-included in the study. After the pretest, ambiguous words were simplified based on recommendations from the participants. Furthermore, the minutes taken for filling out these self –administered questionnaires improved from 5–10 minutes to 10–15 minutes considering the participants who had returned the questionnaire first and last. Prior to data collection, data collectors and supervisors were trained for two days on the objective, method, sampling technique, ethical issues, data collection instrument, and data collection procedure. The study participants were arranged in the classroom so that one participant’s privacy was not compromised by the other participants. Before analysis, all questionnaires were checked for completeness and accuracy both during and after the data collection period. After the data was exported to the fitted model, clearance was granted.
Data Processing and Analysis
The data was coded and entered into EpiData 4.6.2.0. The data was then exported to SPSS version 26.0 and cleaned before being analyzed. The variables’ descriptive statistics were computed. To assess the statistical significance and strength of the association between independent variables and outcome variables, a binary logistic regression model was used. To account for confounding effects, variables with P values less than 0.25 were transferred to a multi-variable binary logistic regression model. The model was run using the enter method. The goodness of fit model of Hosmer and Lemeshow was tested, and the data fit the model well (p=0.91). The crude and adjusted odds ratios, as well as their 95% confidence intervals, were computed. A p value of less than 0.05 was considered significant during the multivariable binary logistic regression model analysis. Finally, based on the data obtained, the study’s findings were presented in the form of tables, graphs, and texts.
Results
The response rate of the study participants was found to be 100% in this study. However, only 434 (89.8%) of the total participants completed the questionnaire correctly, and their data was analyzed, while the remaining 49 (10.2%) participants’ data were excluded from analysis due to the questionnaire’s incompleteness.
Participants’ Socio-Demographic Characteristics in the Study
The participants’ average age was 17.2 years, with a standard deviation of 2.08 years. 314 (72%) of the total participants were male, 310 (71.4%) had been non-health students, and 316 (72.8%) were year II and above students. In terms of ethnicity, 288 (64.5%) of the participants were Oromo, with 118 (27.2%) being Amhara (Table 1).
 |
Table 1 Socio-Demographic Characteristics of Study Participants at Madda Walabu University from February to March 2022 (n=434) |
The Use of Reproductive Health Services and Sexual Experiences of Study Participants
According to the table below, nearly sixty-five percent (64.5%) of study participants had ever heard about sexual and reproductive health rights, with peers serving as the primary source of information for 84 (19.4%). Almost three-quarters (310) of study participants did not discuss their sexual and reproductive health rights with anyone else. In terms of sexual behavior, more than half of the study participants (60%) had sexual intercourse at some point in their lives, with approximately (23.07%) having sexual intercourse before the age of eighteen (Table 2).
 |
Table 2 Reproductive Health Service Utilization and Sexual Experience Among Madda Walabu University Study Participants (n=434) from February to March 2022 |
The Level of Knowledge of SRHR Among Study Participants
To assess the study participants’ knowledge of sexual and reproductive health rights, thirteen yes/no questions were used. Those who answered “yes” received a value of one, while those who answered “no” received a value of zero. The questions with the opposite answers were recoded. The participants’ mean level of knowledge on sexual and reproductive health rights is calculated using a corrected answer. As a result, the sum of questions ranged from 5 to 13, with an 8.25 mean knowledge of sexual and reproductive health rights and a 1.36 standard deviation. Only 120 of the total participants correctly answered all of the questions.
312 (72.0%) of those polled responded “correctly” to the question of whether a man should have sex whenever he wants, regardless of his wife’s wishes. In addition, 298 (68.7%) of participants responded “correctly” to the question of whether girls have the right to autonomous reproductive choices without the consent of their partners, and 271 (62.4%) responded “correctly” to the question of whether reproductive age groups have the right to the highest attainable standard of health (Table 3).
 |
Table 3 Knowledge of Sexual and Reproductive Health Rights Among Madda Walabu University Study Participants (n=434) from February to March 2022 |
According to the current finding, 52% of the participants (226) had an optimal level of SRHR knowledge, which was at or above the mean of 8.25 with a standard deviation of 1.36 (Figure 1).
 |
Figure 1 Knowledge of sexual and reproductive health rights among Madda Walabu University students in Southeast Ethiopia from February to March 2022 (n=434). |
Factors Related to Sexual and Reproductive Health Right Knowledge
Bivariate binary logistic regression analysis revealed associations between knowledge of sexual and reproductive health rights and place of residence, field of study, year of study, monthly income from family or relatives, secondary school attendance in a private school, talking about reproductive rights with someone else, having heard of them before, the presence of a reproductive health club on campus, and membership in a reproductive health club. These variables were all transferred to the multivariable binary logistic regression model since they all satisfied the predetermined criterion, with a p-value of less than 0.25.
In a multivariate binary logistic regression analysis, the origin of residency, field of study, attending secondary school in a private school, discussing sexual and reproductive health rights with someone else, the availability of a reproductive health club on campus, and participation in a reproductive health club were found to be statistically significant predictors of optimal knowledge on SRHR. According to Table 4, participants from urban areas had nearly twice the odds of knowing about SRHR [AOR=1.52, 95% CI: 1.02 −1.14]. Furthermore, when compared to non-health students, health students were 12 times more likely to have good knowledge of SRHR [AOR= 12.21, 95% CI: 7.27–14.88]. Additionally, students who attended a private secondary school were 6.12 times more likely to have good knowledge of SRHR [AOR=6.12, 95% CI: 7.35–9.26], and students who participated in reproductive health clubs were nearly 4 times more likely to have good knowledge of SRHR [AOR=3.95, 95% CI: 3.47–5.90].
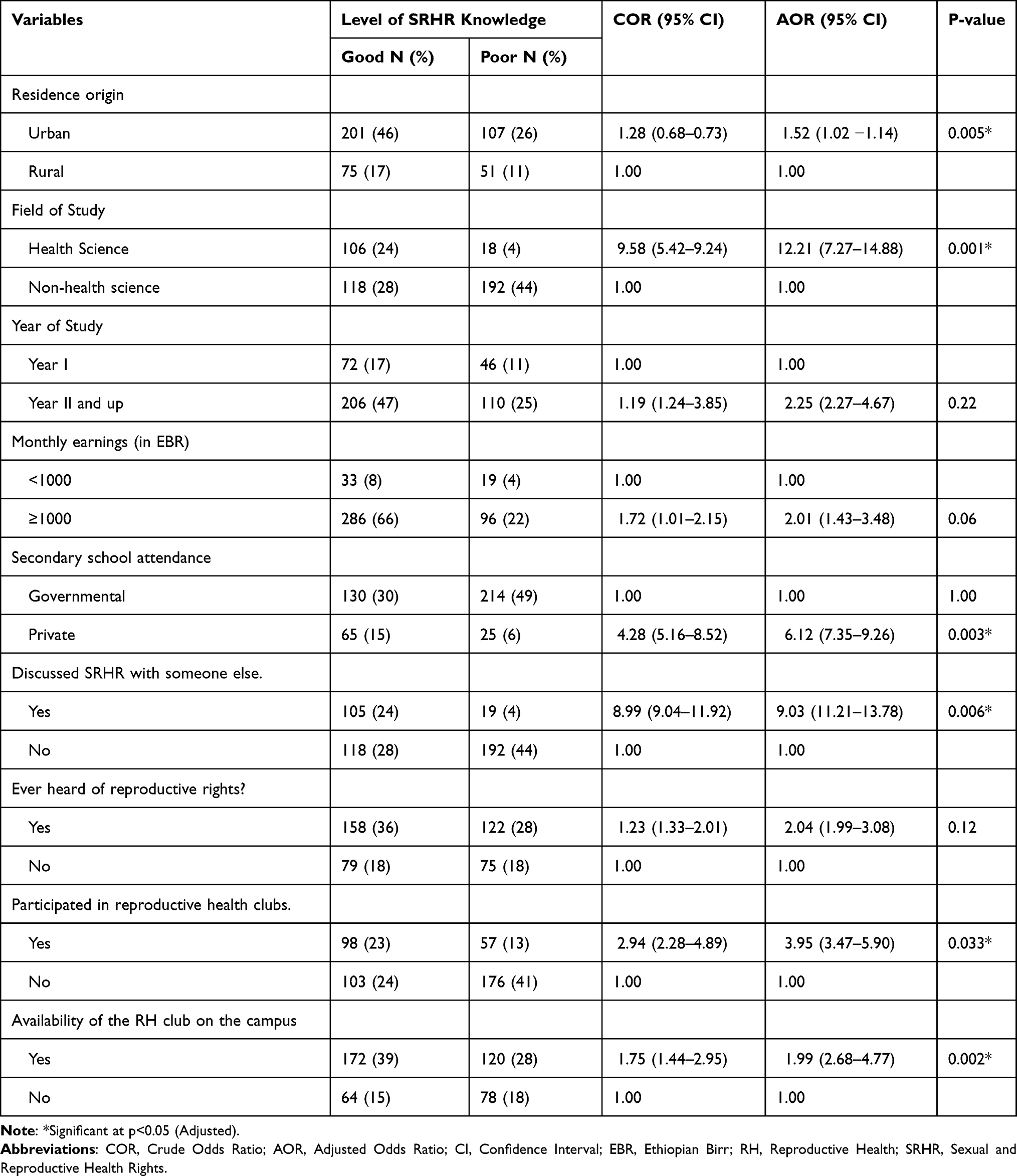 |
Table 4 Bivariate and Multivariate Binary Logistic Regression Analyses of Factors Associated with Knowledge of Sexual and Reproductive Health Rights Among Madda Walabu University Study Participants (n=434) from February to March 2022 |
Discussion
As the majority of the world’s countries strive for universal health coverage, making every effort to ensure that sexual and reproductive health rights are effectively incorporated becomes increasingly important.2 Due to a lack of knowledge about SRHR, university students are less likely to use existing health services.23 The goal of this study was to assess university students in southeast Ethiopia’s knowledge of sexual and reproductive health rights. In this study, the level of knowledge on sexual and reproductive health rights was found to be 52.1% [95% CI (47.32–55.08)]. This finding is consistent with research from Nepal (51.12%)12,52.2%16, and 54.5%15 in Ethiopia. However, it is higher than studies conducted elsewhere in Ethiopia (16.4%),14 (46.6%),18 (47.1%)17 and lower than studies conducted elsewhere in Ethiopia (57.7%),19 (59.6%)24 and 60.3% in Ikeja and 62.1% in Ikorodu in Nigeria.13 The disparity could be attributed to differences in study settings and methods. For example, the Nigerian study used a mixed study design (both quantitative and qualitative),13 whereas ours is only a quantitative cross-sectional study. Another reason could be that different countries’ implementation of adolescent-based sexual and reproductive health education.
According to the study, participants from urban origins were nearly twice as likely to have good knowledge of sexual and reproductive health rights. The rationale behind this could be that participants from urban areas have more exposure to information and media. Furthermore, participants from urban areas are more likely to come from educated families and to freely discuss the issue with family members and peers than participants from rural areas in a developing country like Ethiopia. A study of regular undergraduate students at Wolaita Sodo and Gonder University backs up the findings.15,19
Participants from the faculty of health sciences were also 12.21 times more likely to be knowledgeable about sexual and reproductive health issues. This could be because health students are taking a course on sexual and reproductive health. It could be explained better because the curriculum of health science programs included information about reproductive health and family planning in particular. A previous study on university students found that being a student in the faculty of health science was more likely to have good knowledge of sexual and reproductive health rights.14–16
Similarly, participants who attended secondary school in private schools were six times more likely to be knowledgeable about SRHR. The most likely reason is that, when compared to governmental schools, the total number of students in private schools was lower, allowing information to reach the majority of students easily through either reproductive health club or mini-media. Also, students from private schools were closer to their teachers, so they could easily inform them about the scenario. Similarly, a study found that students who attended secondary school in private school were twice as likely knowledgeable about sexual and reproductive health right.15
The study discovered that participants who discussed sexual and reproductive health rights with someone else were 9 times more likely to have good knowledge of sexual and reproductive health rights. Similarly, discussing sexual issues with someone else is associated with greater knowledge of sexual and reproductive health rights.14,15,24 Those who discussed the issue with someone else surely got full information about SRHR and may be free of fear of getting reproductive health services and be able to use their rights appropriately.
Furthermore, having access to reproductive health services on campus and participating in reproductive health clubs were linked to having a good understanding of SRHR. Participants who were aware of the availability of reproductive health services on campus knew nearly twice as much about their sexual and reproductive health rights. The reason for this could be that students who were aware of the existence of reproductive health clubs on campus could join them and easily share information with one another. Similarly, a study of Haramaya and Gondar university students found that the presence of reproductive health clubs on campus was significantly associated with optimal knowledge of sexual and reproductive health rights.16,19
Participants in this study who were members of a reproductive health club were nearly four times more likely to have a good knowledge of sexual and reproductive health rights. Similarly, another study among university students found that students who participated in reproductive health clubs were more likely to have good knowledge about sexual and reproductive health rights.15,16,24 Understanding current students’ knowledge of SRHR, in general, is useful for assessing the accessibility of reproductive health services and the need for intervention-based sexual and reproductive health education on campus. The finding implies that university authorities are expected to check the availability of reproductive health club on the campus, prepare training on the sexual and reproductive health rights for the students, have program invite the non-governmental organization on the area to improve the students’ knowledge since it has great social impact.
Limitations of the Study
Even though it strictly adheres to scientific procedures, the current study has some flaws. For example, because the study was limited to one public university in Ethiopia, it lacked representation from all governmental and private universities in the country. Furthermore, data collection using self-report tools may be biased and incomplete. Finally, due to the cross-sectional nature of the study, we were unable to account for temporal relationships between variables.
Conclusion
Four out of ten students in this study had inadequate knowledge of SRHR. Being a city dweller, a health student, attending a private secondary school, having a reproductive health club on campus, and play a part in RH clubs were all independently associated with a high level of SRHR knowledge. SRH education should be included in non-health department courses, SRH training should be prepared on campus, reproductive health clubs should be established, and students should be encouraged to participate in these clubs. In addition, practice and intervention-based studies are recommended for assessing university students’ knowledge of SRHR.
Abbreviations
MWU, Madda Walabu University; SRH, Sexual and Reproductive Health; RH, Reproductive Health; SRHR, Sexual and Reproductive Health Rights; SPSS, Statistical Package for Social Sciences; SRS, Systematic Random Sampling; AOR, Adjusted Odds Ratio; CI, Confidence Interval; EBR, Ethiopian Birr.
Data Sharing Statement
The data set used in the current study is available upon reasonable request from the corresponding author.
Informed Consent
Madda Walabu University’s research and ethical committee granted ethical clearance with a letter of reference number RDD/0048/14. Permission was obtained from the appropriate colleges, schools, and departments. Additionally, the study followed the Declaration of Helsinki’s principles for conducting human subject’s research. After thoroughly explaining the study’s objectives, each study participant provided written informed consent. The study participant was given the option to refuse, discontinue, or withdraw from participation at the time of data collection. Throughout the study, the privacy and confidentiality of information and responses were guaranteed.
Acknowledgments
The authors would like to thank all of the study participants, data collectors, and supervisors for their assistance.
Author Contributions
All authors made a significant contribution to the work reported whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising, or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted, and agree to be accountable for all aspects of the work.
Funding
No funding was provided for this work.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Griffin S. Literature Review on Sexual and Reproductive Health Rights: Universal Access to Services, Focussing on East and Southern Africa and South Asia. Department for International Development; 2006:1–28.
2. Brown R, Kismödi E, Khosla R, et al. A sexual and reproductive health and rights journey: from Cairo to the present. Sex Reprod Health Matter. 2019;27(1):326–328. doi:10.1080/26410397.2019.1676543
3. UNPF. United nations population fund; 2014.
4. WHO. World Health Organization Recommendations on Adolescent Sexual and Reproductive Health and Rights. Geneva: World Health organization; 2018.
5. Singh S, Bankole A, Woog V. Evaluating the need for sex education in developing countries: sexual behaviour, knowledge of preventing sexually transmitted infections / HIV and unplanned pregnancy. Sex Educ. 2005;5(4):307–331. doi:10.1080/14681810500278089
6. Muchena J, Awuor L. The center for rights education and awareness (CREAW) multisectoral rapid assessment gender based violence in Kitui country of Kenya; 2019. Available from: https://www.nation.co.ke/news/Controversial-Kamba-tradition/1056-5004020-80bh76z/index.html.
7. Sable MR, Msw D, Danis F, et al. Barriers to reporting sexual assault for women and men: perspectives of college students. J Am Coll Health. 2006;55(3):157–162. doi:10.3200/JACH.55.3.157-162
8. UNESCO. International technical guidance on sexuality education; 2018.
9. DFID. Sexual and reproductive health and rights A position paper; 2004.
10. Rickert VI, Rupal Sanghvi CMW. Is lack of sexual assertiveness among adolescent and young adult women a cause for concern? Perspect Sex Reprod Health. 2002;34(4):178–183. doi:10.2307/3097727
11. Mcgranahan M, Nakyeyune J, Baguma C, et al. Rights based approaches to sexual and reproductive health in low and middle-income countries: a systematic review. PLoS One. 2021;16(4):1–20. doi:10.1371/journal.pone.0250976
12. Muna Bhattarai RD. Knowledge regarding reproductive rights among undergraduate students. Sch J Appl Med Sci. 2015;3(7A):2461–2465.
13. Ogunlayi M. An assessment of the awareness of sexual and reproductive rights among adolescents in South Western Nigeria. Afr J Reprod Health. 2005;9(1):99–112. doi:10.2307/3583164
14. Berhe ET, Ayene M, Gebregyorgis T. Low-level knowledge and associated factor of sexual and reproductive health rights among Aksum University Students, Aksum. Front Public Health. 2022;10:1–8.
15. Adinew YM, Abebaw Gebeyehu Worku ZBM. Knowledge of reproductive and sexual rights among University students in Ethiopia. BMC Int Health Hum Rights. 2015;13(12):1–7.
16. Yuya M, Adem HA, Assefa N, Alemu A. Level and predictors of knowledge of reproductive rights among Haramaya University students, Eastern Ethiopia: a cross-sectional study. Front Reprod Health. 2021;3:1–8.
17. Gebretsadik GG, Weldearegay GG. Knowledge on reproductive and sexual rights and associated factors among youths, Shire town, Tigray, Northern Ethiopia. Int J Res Pharm Sci. 2016;6(2):30–37.
18. Yemaneh Y, Gezahagn R, Yechale M, Assefa M, Abrha K, Alemayehu Abdias FN. Assessment of knowledge, attitude and practice towards reproductive health service among Mizan Tepi University Tepi campus students, Sheka Zone, south nations nationalities and peoples regional State, South West Ethiopia. J Hosp Med Manag. 2017;3:
19. Gebresilassie KY, Boke MM, Melaku Kindie Yenit AGB. Knowledge level and associated factors about sexual and reproductive health rights among University of Gondar students, Gondar Ethiopia. Int J Sex Reprod Health Care. 2019;2(1):016–20. doi:10.17352/ijsrhc.000006
20. UNFPA. UNFPA annual report; 2005.;
21. Youths FA, Town S, Gebretsadik GG, Weldearegay GG. Knowledge on reproductive and sexual rights and associated factors among youths, Shire town, Tigray, Northern Ethiopia. Int J Res Pharm Sci. 2016;20(June):111–120.
22. Madda Walabu University registrar record office report; 2022.
23. Berhane F, Berhane Y, Fantahun M. Adolescents’ health service utilization pattern and preferences: consultation for reproductive health problems and mental stress are less likely. Ethiop J Health Dev. 2005;19(1):29–36.
24. Ayalew M, Nigatu D, Sitotaw G, Debie A. Knowledge and attitude knowledge and attitude towards sexual and reproductive health rights and associated factors among Adet Tana Haik College students, Northwest Ethiopia: a crosssectional study. BMC Res Notes. 2019;12(80):1–7. doi:10.1186/s13104-019-4116-4
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.