")
Back to Journals » Patient Preference and Adherence » Volume 15
Knowledge of Chronic Kidney Disease Among the Population of Saudi Arabia Evaluated Using a Validated Questionnaire: A Cross-Sectional Study
Authors Alobaidi S
Received 12 April 2021
Accepted for publication 2 June 2021
Published 14 June 2021 Volume 2021:15 Pages 1281—1288
DOI https://doi.org/10.2147/PPA.S315369
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Johnny Chen
Sami Alobaidi
Department of Internal Medicine, University of Jeddah, Jeddah, Saudi Arabia
Correspondence: Sami Alobaidi
Department of Internal Medicine, University of Jeddah, Jeddah, Saudi Arabia
Tel +966566482649
Email [email protected]
Introduction: Public knowledge and awareness regarding chronic kidney disease (CKD) is an important factor influencing the successful implementation of CKD prevention and screening programs. To the best of our knowledge, there are no studies conducted among the Saudi population to explore the public knowledge of CKD using a validated questionnaire. Hence, we explored the knowledge of CKD among the population of the Kingdom of Saudi using a validated questionnaire to determine the level of knowledge regarding CKD as well as the predictors of CKD knowledge.
Materials and Methods: This was a cross-sectional online survey study conducted between 12 January 2020 and 11 February 2021. A structured study questionnaire in the GoogleTM platform, with socio-demographic variables and questions assessing CKD knowledge, was used to collect data. A snowball sampling technique was used to recruit participants.
Results: A total of 983 people accessed the survey and 951 provided a complete response. Respondents belonging to the age group 41– 55 years, having masters or PhD level education, having monthly income > 15,000 SR, married, doing > 150 minutes/week physical activity had significantly higher kidney disease knowledge. There were significant differences in the mean kidney disease knowledge total score between participants with and without: a history of kidney disease (5.63, df = 895, p< 0.001), diabetes mellitus (2.34, df = 949, p = 0.019), hypertension (3.25, df = 949, p = 0.001), and family history of kidney failure (4.60, df = 949, p< 0.001).
Conclusion: The study revealed a lack of awareness among the Saudi population regarding knowledge about CKD. However, a significantly higher level of knowledge prevailed among respondents from higher educational and higher economic backgrounds. Those with risk factors for CKD also held a greater knowledge about the disease.
Keywords: knowledge, CKD, Saudi population, validated questionnaire
Introduction
Chronic kidney disease (CKD) is a non-communicable disease characterized by persistent abnormality in the structure or function of kidneys for more than 3 months.1 The prevalence of CKD has been on the rise over the past several decades making it a significant burden on healthcare systems worldwide at present.2 A recent meta-analysis has estimated the worldwide prevalence of CKD at 13.4%.3 The global prevalence of CKD was estimated to be 9.1% in 2017 and 1.2 million deaths were attributed to it.4 Studies reported 17-fold higher mortality among patients with end stage kidney disease (ESKD) compared with age- and gender-matched healthy individuals.5 The number of deaths due to CKD has been projected to be 2–4 million by 2040.4 Apart from the potential to lead to ESKD and premature death, CKD has also been recognized as an independent risk factor for cardiovascular disease; 7% of the total cardiovascular disease burden being attributed to impaired kidney function.5 In the Kingdom of Saudi Arabia, CKD has been recognized as a major health problem in recent decades due to the growing incidence and prevalence of ESKD among the Saudi population.6 The three very important risk factors for CKD – diabetes, hypertension and obesity – are highly prevalent in the Saudi population.5 An epidemiological study conducted in 2010 in the Kingdom of Saudi Arabia found that the overall prevalence of CKD was 5.7%.7 There were around two million cases of CKD and 3818 deaths due to CKD in Saudi Arabia in 2017.4 A recent study also reported the overall prevalence of CKD stages 3 to 5 was 4.4% among the Saudi population.8 However, there is a clear lack of attention from policymakers and researchers regarding this emerging challenge in the Arab world, especially Saudi Arabia, and limited resources are being allocated towards the prevention and management of CKD and its risk factors.5
Considering the significant morbidity and very high rate of mortality among patients with ESKD, efforts are made worldwide in the prevention and early detection of CKD. Prevention, early detection and adequate treatment of major risk factors of CKD such as diabetes, hypertension and obesity together constitute an important public health strategy in this regard and it is critically important in the Arab world where these risk factors are highly prevalent.5 It has been estimated that successful prevention of these risk factors by public health interventions at population level can result in a reduction of up to 40% in the incidence of CKD.9 Screening of individuals with risk factors to detect and treat CKD early is another important strategy adopted by various countries for delaying of CKD disease progression.10 Alsuwaida et al. conducted a pilot community-based screening program to detect CKD in Saudi Arabia and demonstrated that it is feasible and relatively inexpensive.7
It goes without saying that public knowledge and awareness regarding CKD is an important factor influencing the successful implementation of CKD prevention and screening programs. Higher rate of early identification of individuals with undetected/early CKD or those at risk of developing CKD might be possible among populations with high levels of knowledge and awareness about CKD.11 Studies conducted in both developed and developing countries have shown that the public understanding of CKD and its risk factors are relatively poor.12 A recent Australian study found limited knowledge among participants regarding the physiological role of the kidneys, and less than half of the participants correctly identified hypertension as a risk factor.12 A study conducted during 2010 among the population of Saudi Arabia showed that less than 7.1% of patients with early CKD reported awareness of their CKD status and there was poor awareness regarding CKD symptoms among the study cohort.7 However, another recent study from Saudi Arabia exploring knowledge and awareness about CKD using a non-validated questionnaire found that more than half of the participants correctly identified HTN and DM as risk factors of CKD, indicating that the knowledge regarding CKD among the Saudi population is relatively increasing.11 To the best of our knowledge, there are no studies conducted among the Saudi population to explore the public knowledge of CKD using a validated questionnaire. Hence, we explored the knowledge of CKD among the population of the Kingdom of Saudi using a validated questionnaire to determine the level of knowledge regarding CKD as well as the predictors of CKD knowledge.
Methodology
This was a cross-sectional online survey study conducted between 12 January 2020 and 11 February 2021. A structured study questionnaire in GoogleTM platform, having socio-demographic variables and the questions assessing CKD knowledge, was used to collect data (Supplementary File 1). Snowball sampling technique was used to recruit participants. We used the CKD knowledge questionnaire developed and validated by Gheewala et al. 2018.12 The CKD knowledge questionnaire consists of 24 questions with the multiple-choice options “True”, “False” and “I don’t know”. Correct responses were given a score of 1 and incorrect responses were given a score of 0. The option “I don’t know” was considered as lack of knowledge and given a score of 0. The questionnaire was developed through a systematic literature review of existing public and related questionnaires. The questionnaire was validated by applying the final version of the questionnaire among 27 students, 28 nephrologists and 121 participants from the public. The analysis showed that the questionnaire had good internal consistency; the Cronbach’s alpha was 0.88 (95% CI: 0.86–0.91).12 The questionnaire was shared with contacts of the researcher through social media across the Kingdom of Saudi Arabia and each recipient was asked to share the link with at least 5 other contacts. The questionnaire started with consent for voluntary participation, from the Saudi population of >15 years, followed by socio-demographic details and the CKD knowledge questions. All participants were informed about the purpose of the study. The study was conducted in accordance with the Declaration of Helsinki.
Statistical Analysis
The collected data were analyzed using Statistical Package for Social Sciences (SPSS Inc., Chicago, IL, version 26.0 for Windows) software. The characteristics of the respondents were described using frequencies, percentages, averages and standard deviations. Univariate analysis using chi-square tests was used to assess relationships between variables. Bivariate analysis was conducted to study the relationship between socio-demographic variables and the CKD knowledge score, using independent t-tests and one-way ANOVA. A two-tailed P value of <0.05 was considered as statistically significant.
Results
A total of 983 people accessed the survey and 951 provided a complete response. The majority of the respondents were aged 26–55 years (71%) and 50.9% were males. 63.1% of the respondents were graduates and 45% were not working currently. 64.5% of the respondents were married, and 25% were earning >15,000 SR per month. 89 (9.4%) respondents reported a history of kidney disease. 13.4% of the participants had DM, 20.7% had HTN, 3.7% had cardiac disorder, 17.9% had osteoarthritis, and 1.2% had stroke. 46.8% of the respondents had a family member working in the healthcare sector, and 21% had a family history of kidney failure. 22.9% of the respondents reported a smoking habit, and only 14.2% reported physical activity >150 minutes/week. 20.7% of the respondents reported usage of pain killers, 24.6% reported usage of herbal medicines. The details are summarized in Table 1.
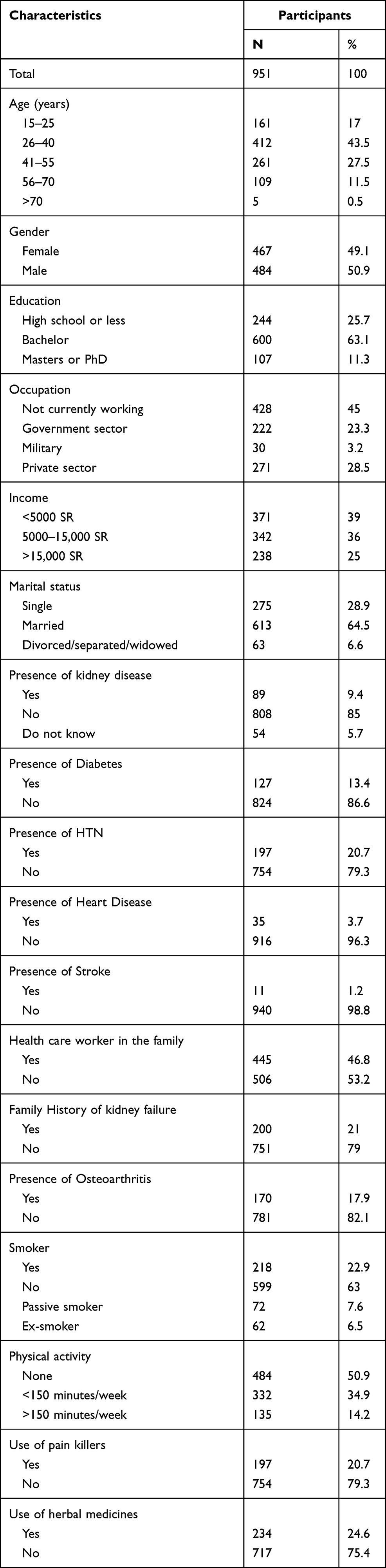 |
Table 1 Participant Characteristics |
The mean (SD) kidney disease knowledge score of the study population was 11.99 (± 4.70), with scores ranging from 0 to 22. 42.9% of the respondents had knowledge scores less than 11. Most of the participants answered the following questions correctly: urine test (87.9%) and blood test (80.4%) are used commonly to determine health of the kidneys, a person can lead a normal life with a single kidney (80.5%), the kidneys clean blood (79.8%), diabetes is a risk factor for kidney disease (69.2%), and water retention (79.8%) and increased fatigue (68.8%) are signs of kidney disease. However, only few respondents reported correct answers for the following questions: nausea/vomiting (44.7%) and loss of appetite (43.7%) are signs of kidney disease, the kidneys help to maintain blood pressure (46.8%) and bone health (28.9%). The majority of the respondents reported wrong answers for the following questions: the kidneys help to keep blood sugar level (74.2%) and breakdown of the proteins (81%), being female (78%), having heart disease (70.9%) and having excess stress (78.4%) are risk factors of kidney disease, and fever is a sign of kidney disease (84.1%). The percentage of correct responses to individual items of the kidney disease knowledge questionnaire are summarized in Table 2.
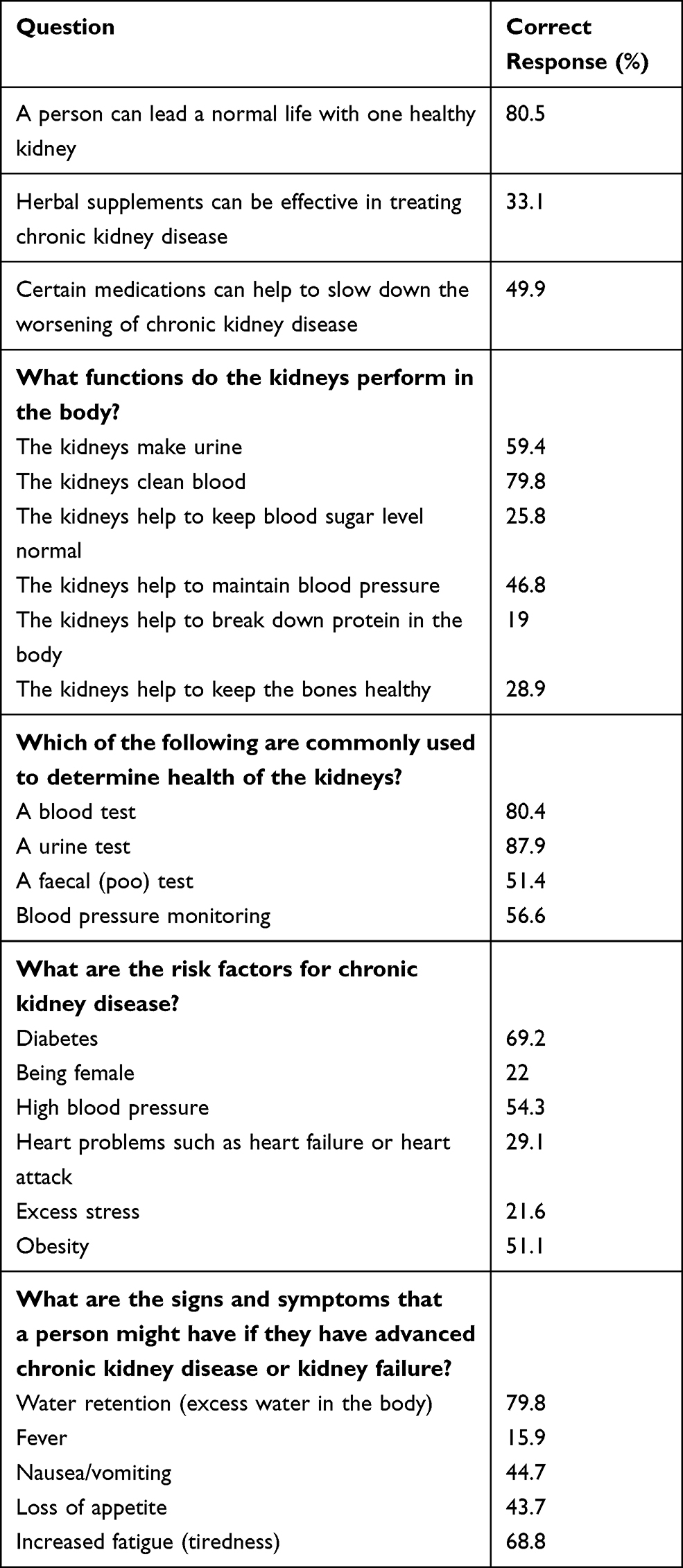 |
Table 2 Percentage of Correct Response to Individual Items on the Questionnaire |
The bivariate analysis performed using one-way ANOVA tests showed that there are significant associations between kidney disease knowledge score and age (3.14, p = 0.014), educational level (4.03, p = 0.018), income (5.87, p = 0.003), marital status (3.78, p = 0.023), and frequency of physical activity (4.49, p = 0.011). Respondents belonging to the age group 41–55 years, having masters or PhD level education, having monthly income >15,000 SR, married, doing >150 minutes/week physical activity had significantly higher kidney disease knowledge. The results of the bivariate analysis performed using one-way ANOVA test between individual participant characteristics and total score are summarized in Table 3. The results of the bivariate analysis performed using independent t-tests between individual respondent characteristics and kidney disease knowledge total score showed that there were significant differences in the mean kidney disease knowledge total score between participants with and without a history of kidney disease (5.63, df = 895, p<0.001), diabetes mellitus (2.34, 949, p = 0.019), hypertension (3.25, df = 949, p = 0.001), and family history of kidney failure (4.60, df = 949, p<0.001). The details of the independent t-tests are summarized in Table 4.
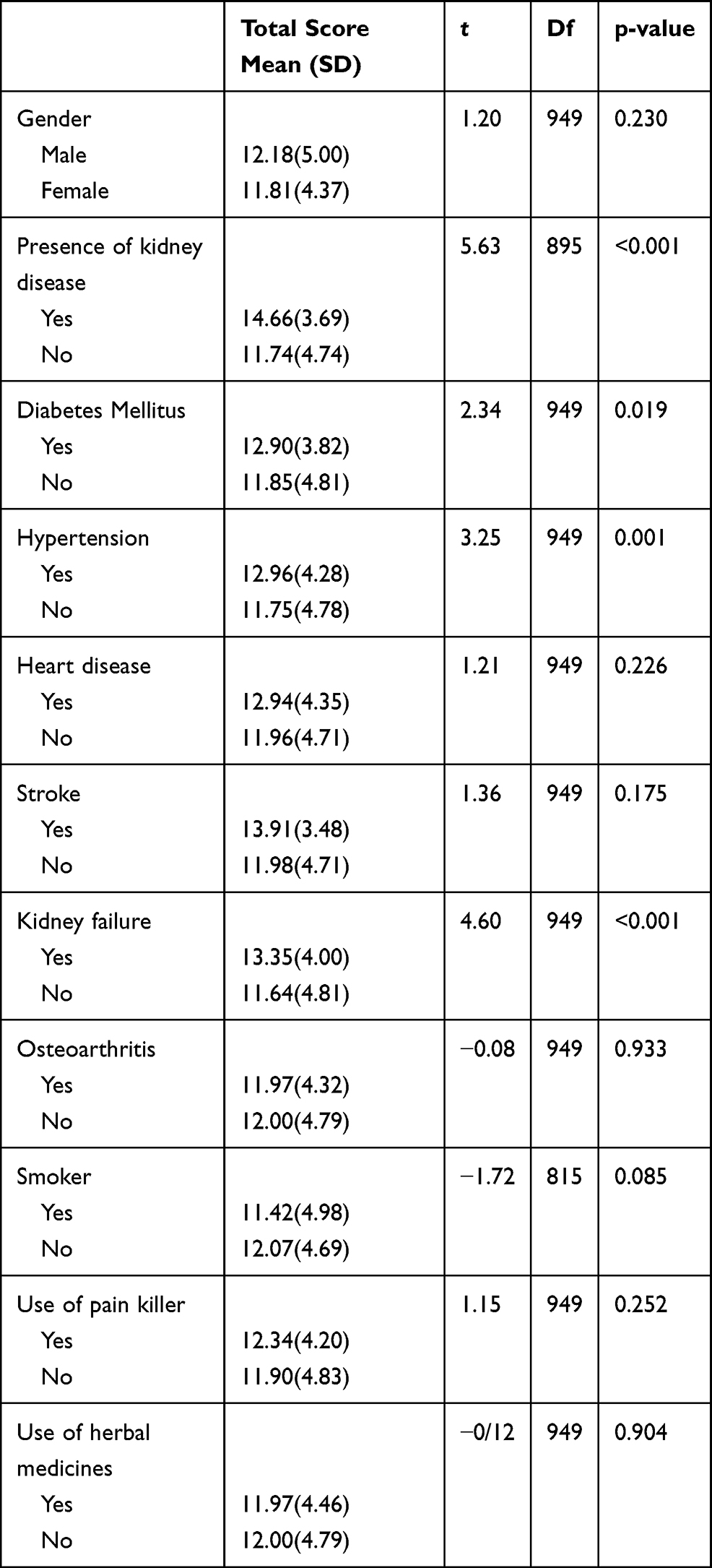 |
Table 3 Results of the Bivariate Analysis Performed Using Independent t-test Between Individual Participant Characteristic and Total Score |
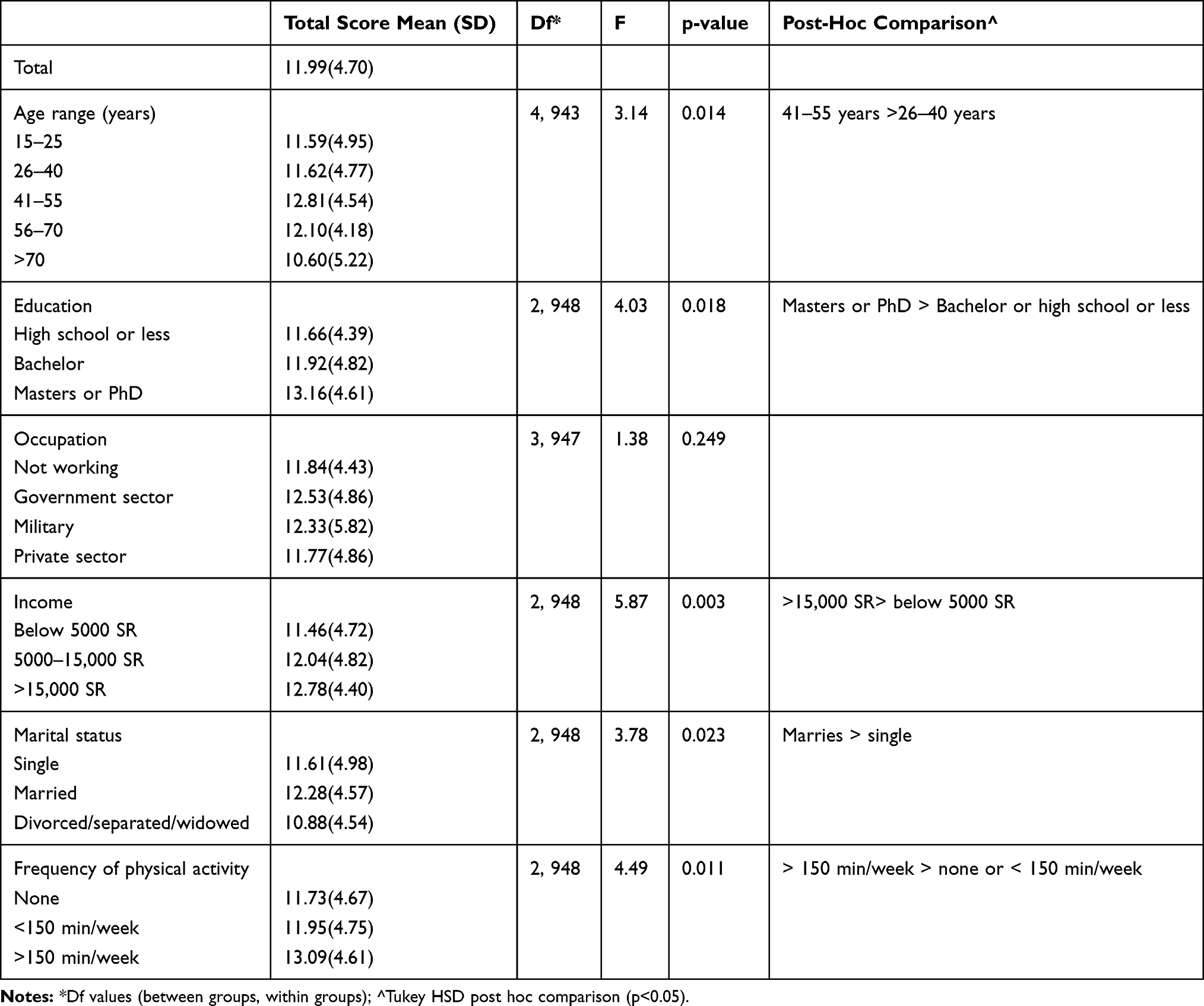 |
Table 4 Results of the Bivariate Analysis Performed Using One-Way ANOVA Test Between Individual Participant Characteristics and Total Score |
Discussion
This study conducted among the Saudi population to explore the public knowledge about CKD revealed that the studied population had an overall poor knowledge in the subject. The respondents held a poor knowledge about the functions of the kidney, especially in blood pressure regulation and maintenance of bone health, similar to a recent study among the Australian public.12 However, the respondents had a relatively good knowledge about the role of blood and urine testing in determining the health of the kidneys. More than half of the respondents correctly identified DM, HTN, and obesity as risk factors of CKD, yet the majority wrongly identified female sex, and stress as risk factors of CKD. Albujays et al. explored CKD knowledge among diabetic patients in Al-Ahsa Governorate, Kingdom of Saudi Arabia, and found that 52.7% of the participants identified DM as a risk factor of CKD, similar to our study.13 Almutary et al. explored CKD knowledge among non‐dialysis CKD patients in the Kingdom of Saudi Arabia, and found significant gaps in their understanding of kidney functioning and clinical presentation of CKD.14 Another study among the Saudi population by Ahmed et al. reported that out of 940 participants, about 60% correctly identified DM and HTN as risk factors of CKD.11 However, a recent study among the Australian public reported that 60.6% of the participants identified DM as a risk factor for CKD, but only 38.3% identified HTN as a risk factor for CKD.12 Similar to our study, lower identification of DM and HTN as risk factors of CKD was also reported from Hong Kong, Nigeria, Singapore and Iran.15–18
In our study, 80.5% of the respondents knew that only one kidney is required to maintain a normal life, which is significantly higher when compared with another study among primary care patients from Singapore which reported that around 50% of the participants knew this.17 However, another study among the Australian public reported that 85.6% of the participants knew that only one kidney is required to maintain a normal life.12
In our study, 50.1% of the respondents did not know that medications can help to slow down the worsening of CKD, and 66.9% wrongly believed that herbal supplements can be effective in treating CKD, indicating poor understanding of the studied population regarding CKD treatment. Similar results were also observed among the Australian public by Gheewala et al., in which 51.2% of the respondents knew that medications can help to slow down the worsening of CKD, and 76.6% wrongly believed in the effectiveness of herbal supplements in treating CKD.12 There are various safe and cost-effective therapies that can slow down the progression of CKD, and our study highlights the importance of disseminating information related to these effective treatments.19 In the absence of such public and patient outreach activities, there is a real chance that many patients with CKD might end up in taking herbal medications for the treatment of CKD, which might cause more harm to them.20
Screening for CKD among a high-risk population is an effective public health approach to detect and treat CKD early in its course. Public understanding of CKD, especially about the screening methods, can enhance the penetration and effectiveness of such interventions. Our study results are encouraging due to the fact that >80% of the respondents rightly identified blood test and urine test as methods to identify kidney diseases and 56.6% also knew that BP assessment can be used to identify kidney diseases. The rate of correct identification of tests for kidney functioning was significantly higher in our study when compared with studies from other parts of the world, including developed countries. A recent study among the Australian public reported that around 35% of the respondents did not know that blood and urine tests can be used to determine kidney health, and only 20.3% of the respondents knew that BP assessment can be used to determine kidney functioning.12
Our study results also showed significantly higher CKD knowledge score among participants with higher age, higher educational attainments, higher economic status, who were married, and those indulging in physical activities for >150 min/week. Gheewala et al. also found that respondents with higher educational attainment had a significantly higher CKD knowledge score.12 Moreover, they also reported significantly higher CKD knowledge score among married participants, similar to our study.12 Chow et al. also reported a higher CKD knowledge score among participants with higher education level.15 Our study results also showed significantly higher CKD knowledge score among participants with kidney disease, DM, HTN, and family history of kidney failure. Previous studies also reported significantly higher CKD knowledge scores among participants with personal history of DM and participants with a family history of kidney failure.12,15,16 However, higher CKD knowledge score among patients with personal history of HTN was not reported in the past. Our study results suggest that individuals with lower educational attainments, lower economic status, unmarried, leading a sedentary lifestyle, having no risk factors such as DM, HTN and having no family history of kidney disease should be specifically targeted for CKD education as they reported significantly poor CKD knowledge score.
There are a few limitations of this study that need to be considered before interpreting the study results. We conducted an online cross-sectional study based on an online questionnaire that was distributed via various social media platforms, which can lead to selection bias. Moreover, our study sample is not representative of the general Saudi public, limiting generalizability of the study findings.
To conclude, this study evaluated the CKD knowledge among the Saudi population using a validated questionnaire. The CKD knowledge of the Saudi population was poor overall. However, significantly higher CKD knowledge was found among respondents with higher educational and economic status. There was significantly higher CKD knowledge among respondents with CKD risk factors. Our study results highlight the need for conducting targeted CKD educational activities among those in the population with lower educational and economic status.
Data Sharing Statement
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Ethics Approval and Consent to Participate
The project was approved by the institutional ethical committee, University of Jeddah. Consent to participate was obtained from all the participants.
Acknowledgment
The author would like to thank Professor Khaled Alswat for reviewing the manuscript and for his valuable comments.
Funding
There is no funding to report.
Disclosure
The author reports no conflicts of interest in this work.
References
1. Chen TK, Knicely DH, Grams ME. Chronic kidney disease diagnosis and management: a review. JAMA. 2019;322:1294–1304. doi:10.1001/jama.2019.14745
2. Khan UA, Garg AX, Parikh CR, Coca SG. Prevention of chronic kidney disease and subsequent effect on mortality: a systematic review and meta-analysis. PLoS One. 2013;8:e71784. doi:10.1371/journal.pone.0071784
3. Hill NR, Fatoba ST, Oke JL, et al. Global prevalence of chronic kidney disease - a systematic review and meta-analysis. PLoS One. 2016;11:e0158765. doi:10.1371/journal.pone.0158765
4. Collaboration GBDCKD. Global, regional, and national burden of chronic kidney disease, 1990–2017: a systematic analysis for the Global Burden of Disease Study 2017. Lancet. 2020;395:709–733. doi:10.1016/S0140-6736(20)30045-3
5. Farag YM, Kari JA, Singh AK. Chronic kidney disease in the Arab world: a call for action. Nephron Clin Pract. 2012;121:c120–3. doi:10.1159/000345149
6. Almutary HH, Bonner A, Douglas C. Chronic kidney disease in Saudi Arabia: a nursing perspective. Middle East J Nurs. 2013;101:1–9.
7. Alsuwaida AO, Farag YM, Al Sayyari AA, et al. Epidemiology of chronic kidney disease in the Kingdom of Saudi Arabia (SEEK-Saudi investigators) - a pilot study. Saudi J Kidney Dis Transpl. 2010;21:1066–1072.
8. Mousa D, Helal I, Alhejaili F, et al. Sun-137 prevalence of chronic kidney disease markers in Saudi Arabia: population based pilot study. Kid Int Rep. 2020;5:S258.
9. Shaheen FA, Al-Khader AA. Preventive strategies of renal failure in the Arab world. Kidney Int Suppl. 2005;68:S37–40. doi:10.1111/j.1523-1755.2005.09807.x
10. Luyckx VA, Cherney DZI, Bello AK. Preventing CKD in developed countries. Kidney Int Rep. 2020;5:263–277. doi:10.1016/j.ekir.2019.12.003
11. Ahmed IAB, Alharbi SH, Alateeq FA, et al. Knowledge and awareness towards chronic kidney disease risk factors in Saudi Arabia. Int J Clin Med. 2018;9:799–808. doi:10.4236/ijcm.2018.911066
12. Gheewala PA, Peterson GM, Zaidi STR, Jose MD, Castelino RL. Public knowledge of chronic kidney disease evaluated using a validated questionnaire: a cross-sectional study. BMC Public Health. 2018;18:371. doi:10.1186/s12889-018-5301-4
13. Albujays DS, El-barbary HS, Althafar AK, Almulla AH, Hussain MAAS, Ali SI. Study of the level of awareness of chronic kidney diseases among diabetic patients in Al-Ahsa governorate, Kingdom of Saudi Arabia (cross-sectional study). J Sci Stud. 2018;5(12):88–91.
14. Almutary HH. Assessment of kidney disease knowledge among chronic kidney disease patients in the Kingdom of Saudi Arabia. J Ren Care. 2021;47:96–102. doi:10.1111/jorc.12363
15. Chow KM, Szeto CC, Kwan B, Leung CB, Li PK. Public lacks knowledge on chronic kidney disease: telephone survey. Hong Kong Med J. 2014;20:139–144. doi:10.12809/hkmj134134
16. Oluyombo R, Ayodele OE, Akinwusi PO, et al. Awareness, knowledge and perception of chronic kidney disease in a rural community of South-West Nigeria. Niger J Clin Pract. 2016;19:161–169. doi:10.4103/1119-3077.175960
17. Chow WL, Joshi VD, Tin AS, et al. Limited knowledge of chronic kidney disease among primary care patients–a cross-sectional survey. BMC Nephrol. 2012;13:54. doi:10.1186/1471-2369-13-54
18. Roomizadeh P, Taheri D, Abedini A, et al. Limited knowledge of chronic kidney disease and its main risk factors among Iranian community: an appeal for promoting national public health education programs. Int J Health Policy Manag. 2014;2:161–166. doi:10.15171/ijhpm.2014.37
19. Ward F, Holian J, Murray PT. Drug therapies to delay the progression of chronic kidney disease. Clin Med. 2015;15:550–557. doi:10.7861/clinmedicine.15-6-550
20. Jha V. Herbal medicines and chronic kidney disease. Nephrology. 2010;15(Suppl 2):10–17. doi:10.1111/j.1440-1797.2010.01305.x
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.