")
Back to Journals » Infection and Drug Resistance » Volume 13
Knowledge, Attitudes, and Practices Towards COVID-19 Pandemic Among Quarantined Adults in Tigrai Region, Ethiopia
Authors Haftom M , Petrucka P, Gemechu K, Mamo H , Tsegay T , Amare E , Kahsay H , Gebremariam A
Received 6 August 2020
Accepted for publication 7 October 2020
Published 20 October 2020 Volume 2020:13 Pages 3727—3737
DOI https://doi.org/10.2147/IDR.S275744
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Suresh Antony
Mekonnen Haftom,1 Pammla Petrucka,2 Kbrom Gemechu,1,3 Haftamu Mamo,3,4 Tesfay Tsegay,1,5 Embay Amare,4 Hayelom Kahsay,5 Alem Gebremariam4
1Department of Nursing, College of Medicine and Health Sciences, Adigrat University, Adigrat, Ethiopia; 2College of Nursing, University of Saskatchewan, Saskatchewan, Canada; 3Department of Psychiatric Nursing, College of Medicine and Health Sciences, Adigrat University, Adigrat, Ethiopia; 4School of Public Health, College of Medicine and Health Sciences, Adigrat University, Adigrat, Ethiopia; 5School of Medicine, College of Medicine and Health Sciences, Adigrat University, Adigrat, Ethiopia
Correspondence: Mekonnen Haftom Email [email protected]
Background: With the onset of any novel condition, it is the “first” case identified that brings attention and sets into motion the machinery to respond – so it began with a first novel pneumonia case of unknown origin in Wuhan, China. Currently, the World Health Organization has declared SARS-CoV-2 (more commonly known as COVID-19) a public health emergency of international concern. It is projected that the path of COVID-19 could kill 50– 80 million people and impacts the world’s economy in its devastating global sweep. The surge is increasing on global and national levels, causing rapid loss of life, joblessness, deterioration of the healthcare systems, and both national and global economies. In Ethiopia, the first COVID-19 case was reported in March. Since then, the government has been taking different measures to prevent its spread. Locking down all schools, declared social distancing and hand hygiene, and restricting large gatherings were some of the Ethiopian government’s actions.
Objective: To determine knowledge, attitudes, and practices towards COVID-19 pandemic among quarantined adults in Tigrai region, Ethiopia.
Methods: A total of 331 participants selected using a systematic random sampling method were included in the study. We used an interviewer-administered questionnaire. After describing the variables using frequencies, means, and standard deviations, multivariable logistic regression determined factors associated with knowledge and chi-squared tests for attitudes and practices towards COVID-19.
Results: The study participants were primarily males (70%) and mean age 30.5 (SD=11) years. The mean knowledge score was 8.73 (SD=2.64), with less than half 42.9% (95% CI: 37.5– 48%) of the study participants were knowledgeable. Regarding the attitude questions, three-fourths of the participants believed that Ethiopia will control and win the battle against the COVID-19 pandemic. Nearly one-third of the participants replied that the Ethiopian government is handling this pandemic health crisis well. About half of the study participants reported that they had gone to crowded places in recent days, did not wear face mask when leaving home, and practiced preventive measures given by local health authorities. Knowledge score was statistically significantly associated with gender, age, and educational status of the study participants, whereas attitude and practices were significantly associated with educational status and knowledge of participants.
Keywords: knowledge, attitude, practice, quarantine, COVID-19, Ethiopia
Background
Coronavirus disease (COVID-19) has been declared a public health emergency of international concern in January 2020.1–3 As of July 3, 2020, the disease has caused 10,710,005 cases and 517,877 deaths worldwide. In Africa, we have reported 329,796 cases and 6486 deaths.4 This disease affects all ages, but its severity is higher among the aged and those with underlying chronic diseases.5 For instance, the death rate among older people is 48% compared to these younger people.6 The pandemic is causing rapid loss of life, joblessness, deterioration of the healthcare delivery systems, and national and global economies.7 In September 2019, it was projected that there would be a catastrophic respiratory disease that is rapidly moving and could result in the deaths of between 50 and 80 million people while impacting the world economy by 5%.8
In Ethiopia, the first case of COVID-19 was confirmed on March 13, 2020, in Addis Ababa. The infection has been spreading to all parts of the country. On July 26/2020, the Federal Ministry of Health (FMOH) reported 13,968 confirmed cases and 223 deaths with a death rate of 1.6%.9 Since then, the government has been taking different measures to prevent its spread. Locking down all schools, declared social distancing and hand hygiene, restricting large gatherings, limiting travel, preparation of health facilities for treatment and quarantining individuals who had known contact and travel history for five days were some of the actions the Ethiopian government took.10 Community transmission has started in some developing countries, and the pandemic caused psychological and economic insecurities.11,12 Weak health care delivery system, limited resources, the living standards, the cultural norms of the residents, low socio-economic, and environmental factors are some of the risk factors expected to exacerbate the transmission of COVID-19 in developing countries (like Ethiopia).13
Coronavirus spreads primarily through respiratory droplets of saliva or discharge from the nose when an infected person coughs or sneezes.14,15 Control of the virus’s spread could be achieved by limiting human-to-human transmission, identifying, isolating, and caring for victims, and avoiding contact with animals. Infected individuals can be asymptomatic or may present with mild or severe manifestation. The risk of transmission from asymptomatic individuals is high, making the disease difficult to control.16–18
If the disease’s pandemic spread continues in developing countries, its impact will be more severe than that seen in the developed countries due to weak or unresponsive health systems.19 Lack of information, unfavorable attitude, going into crowded places, and inappropriate mask utilization could lead to exacerbated transmission of the pandemic.20–23
Hence, primary prevention through improving the community’s knowledge, attitude, and practice towards COVID-19 prevention methods, and active case detection are demanded.21,24,25 Investigating the knowledge, attitudes, and practices and seeking current evidence on COVID-19 prevention is needed to control the transmission of the disease. Thus, the study aimed to determine knowledge, attitudes, and practices towards the COVID-19 pandemic among quarantined adults in Tigrai region, Northern Ethiopia.
Materials and Methods
Study Design, Setting, and Population
An institutional-based cross-sectional study design was conducted among adults quarantined in Tigrai Region, Northern Ethiopia. A total of 343 randomly selected participants aged 18 to 69 were interviewed from May 15th to 27th, 2020. Using a single population proportion to calculate sample size assuming a 95% confidence level, 5% margin of error, and 50% of the population know about COVID-19 (p=0.5) yielded a calculated sample size of 384. Since the total source population was less than 10,000 (N=2102), the estimated sample size (n=384) was corrected using correction formula. Then, the final sample size after correction (nf=326) and adding a 5% non-response rate becomes 343.
Recruitment Procedure
Multi-stage sampling was used. We clustered the region into zones (n=7). Three quarantine centers in each zone were randomly selected. The total sample size is proportionally allocated to the number of confined and isolated individuals in the past two weeks. We determined the sampling interval (k) by dividing the number of individuals admitted to the centers in the past two weeks by the sample allocated to that center yielding 7. We used a systematic random sampling technique to choose the study participants. The first participant (between 1 and 7) was selected using a lottery method. Supervisors made the participants’ selection, and data collectors were blinded to avoid selection bias. Therefore, every 7th individual was enrolled in the study until the calculated sample size is achieved.
Study Instrument and Data Collection Procedure
The instrument is adapted from similar studies done in Tanzania and China.26,27 The tool had four sections: socio-demographic profile (sex, age, educational status, and employment status); knowledge about clinical characteristics of COVID-19 (items 1–4); knowledge about modes of transmission of COVID-19 (items 5 to 8); and knowledge about prevention and control of COVID-19 (items 9 to 13). Each item has “true” (coded as 0), “false” (coded 1), and “I don’t know” (coded 2) options. For analysis, it was again re-coded to sum the total scores as 1 for correct answers and 0 for both incorrect and I do not know responses. The possible score ranges from 0–13, a high score indicating good knowledge, with ≥10 being acceptable levels of knowledge.28 The third section was about participants’ attitudes, assessed using three items coded as 1 for “agree,” 0 for “disagree,” and 2 for “I don’t know,” responses respecting the potential that COVID-19 will be controlled. The last section of the questionnaire was about the preventive and control measures taken, assessed using three items coded as 1 if “yes” and 0 if the response is “no.” We collected data using a self-administered questionnaire for the literate participants. If the respondent was illiterate, the data were collected using face-to-face interviews by trained data collectors.
Data Quality Assurance and Control
The questionnaire was prepared in English and back-translated to the local language Tigrigna. Also, the accuracy of the tool was checked by back translating to English by experts who were blind to the original instrument. Before starting the data collection, the pre-test was done on 10% (34 individuals) of the total sample size, and an amendment was made accordingly. Also, data were collected by trained data collectors, and completeness of the filled questionnaires was ensured on a daily basis by data collectors and supervisors.
Data Processing and Analysis
We entered and cleaned data using Epi-data manager™ version 3.1. We used SPSSTM version 26 for analysis. Frequency, means, and standard deviations of socio-demographic characteristics of participants were calculated to identify possible baseline differences and presented using tables and text. We used binary logistic regression to see the magnitude, direction, and strength of association between demographic profiles and knowledge scores. Variables significant at p<0.25 with a knowledge score were selected for multivariable analysis. A chi-squared test was used to determine differences in knowledge, attitudes, and practices towards COVID-19 among different demographic profiles of participants. Odds ratio with 95% confidence level was computed, and p-value <0.05 was considered a significant association.
Ethical Consideration
The study considered the Helsinki Declaration. Tigrai Regional Health Bureau approved the study (TRHB: 1052/1418/20). Support letter submitted to the selected quarantine centers of the region, and letters of permission were secured from the administrative bodies and coordinators of the centers. Participants recruited to the study received a verbal explanation of objectives of the research and provided a written information sheet. All potential participants who agreed to participate provided written consent to continue with the interviews. The confidentiality of information obtained was kept, and respondents’ names were not recorded.
Results
Demographic Characteristics
Of the 343 approached participants, 331 completed the questionnaire, making the response rate 96.5%. Table 1 shows the socio-demographic profiles of the study participants. The mean age of the study participants was 30.5 years (SD = 11). Seventy percent of the participants were males, and more than half of the study participants (59.8%) were in the age range from 18–29. Nearly one third (31.1%) were self-employed and completed secondary school (36%).
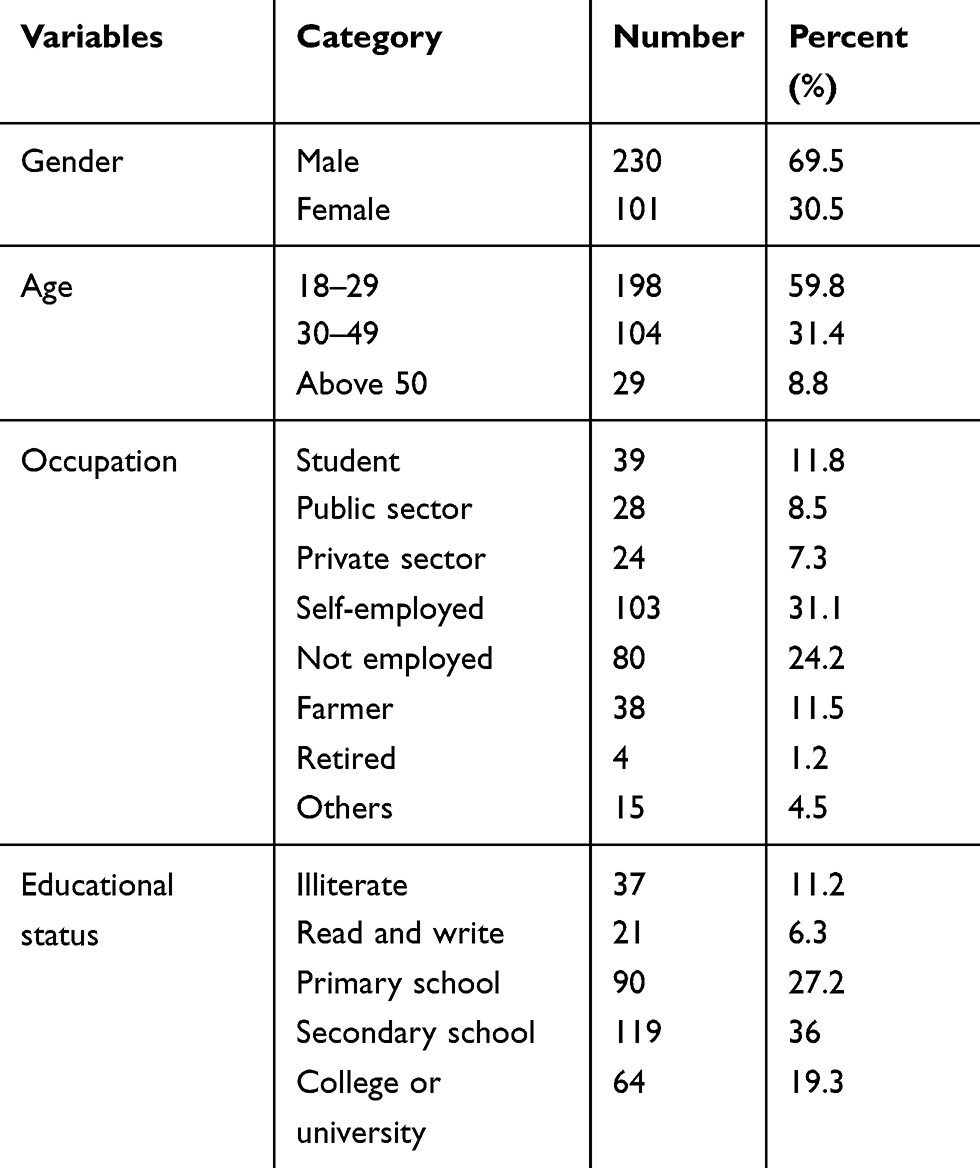 |
Table 1 Demographic Profiles of Study Participants (n=331) |
Participants’ Knowledge Towards COVID-19
The mean (standard deviation) knowledge score was 8.73 (±2.64). The rate of correct answers was 67.2% (8.73/13*100). Less than half (42.9%; 95% CI: 37.5–48%) of the study participants were knowledgeable (score ≥10). The remaining 189 participants (57.1%) (95% CI: 52–62.5%) were not knowledgeable.
The majority (87.6%) of the study participants knew that the main clinical symptoms of the novel COVID-19 are fever, fatigue, dry cough, and myalgia. However, about one fifth 20.2% of the participants correctly answered whether eating or contacting wild animals could result in the infection by the COVID-19 virus. The remaining questions regarding knowledge towards COVID-19 and response are detailed in Table 2.
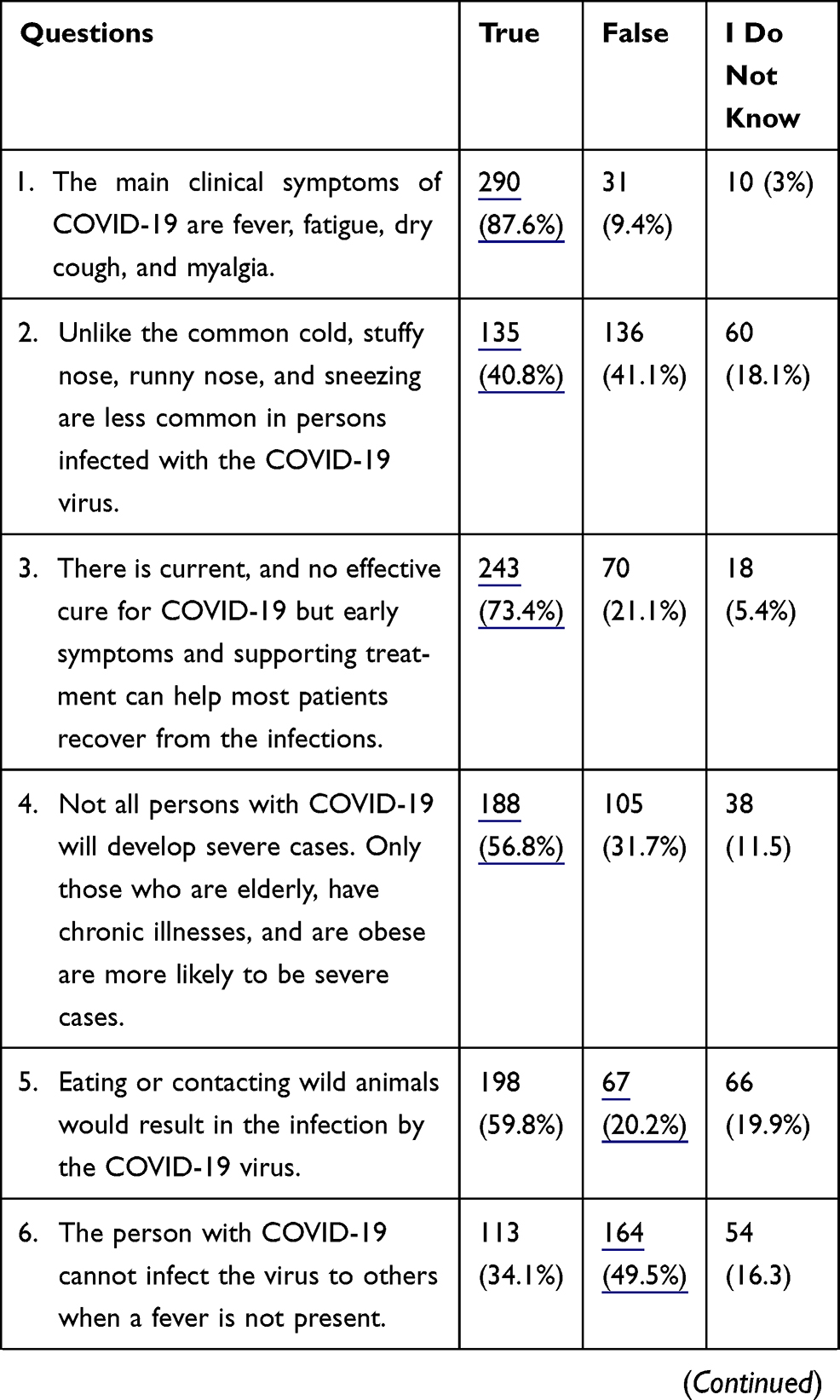 |
Table 2 Participants’ Response to Each Knowledge Questions Towards COVID-19 (n=331) |
In the multivariable logistic regression analysis, gender, age, and educational status were significantly associated with knowledge level. Males were 2.1 (95% CI 1.3–3.5) times more likely to be more knowledgeable than their female counterparts. The odds of being knowledgeable among participants aged 18–29 and 30–49 were 4.7 (95% CI: 1.7–12.8) and 2.9 (95% CI: 1–8.2) times higher than those aged above 50. Those who completed primary school were 4.1 (95% CI: 1.6–10) times more likely to be knowledgeable than those who were illiterate (Table 3).
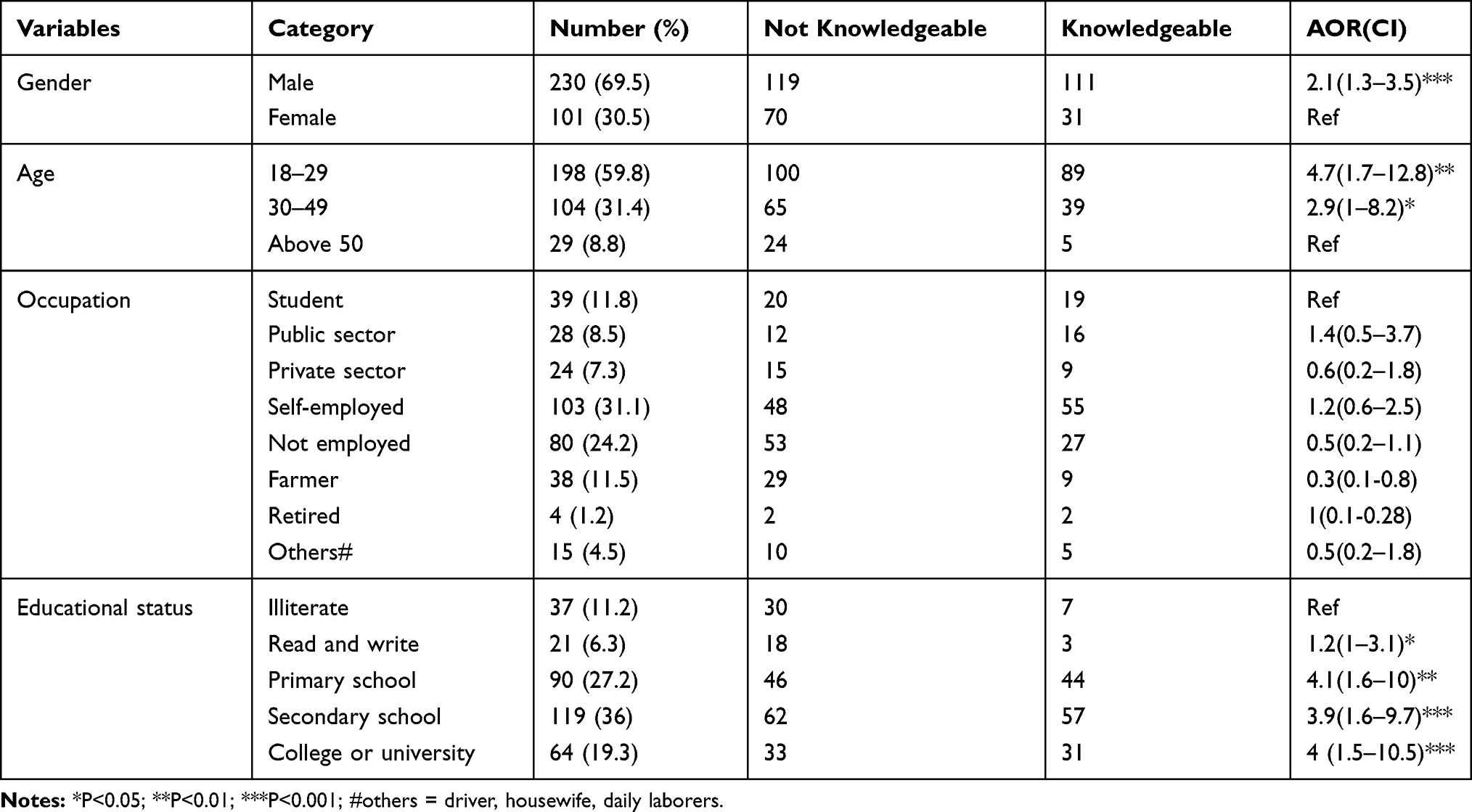 |
Table 3 Multivariable Logistic Regression on Socio-Demographic Characteristics and Knowledge Score of Participants (n=331) |
Participants’ Attitudes Towards COVID-19
We used three questions to assess the participants’ attitudes towards COVID-19. The first question was about their agreement that COVID-19 could be controlled. Two hundred twenty-eight (68.9%, 95% CI: 63.7–73.4%) of the participants agreed that it would be controlled, with 73 disagreeing (22.1%, 95% CI: 17.5–26.3%) and 30 (9.1%, 95% CI: 6.3–12.4) not sure whether the pandemic could be controlled or not. The second question was regarding their confidence that Ethiopia could win the battle against the pandemic. Nearly three fourths [246 (74.3%, 95% CI: 69.2–78.9%)] were confident that Ethiopia would win the fight against COVID-19. The remaining quarter [85 (25.7%, 95% CI: 21.1–30.8%)] of participants were not optimistic that Ethiopia would win the battle against the pandemic. The third question asked whether they agreed or disagreed that the government is handling the health crises well. Nearly half [164 (49.5%, 95% CI: 44.4–55%)] of the study participants responded that the government is not handling the health crises well (Figure 1). In all three questions, educational status and knowledge score showed a positive association. Those who completed college or above were more likely to agree that COVID-19 will eventually be controlled, that Ethiopia will win the battle against COVID-19, and that the government is handling the health crises well. The odds of agreement with the attitude questions amongst those who had an acceptable level of knowledge regarding the pandemic were high compared to their non-agreement counterparts (Table 4).
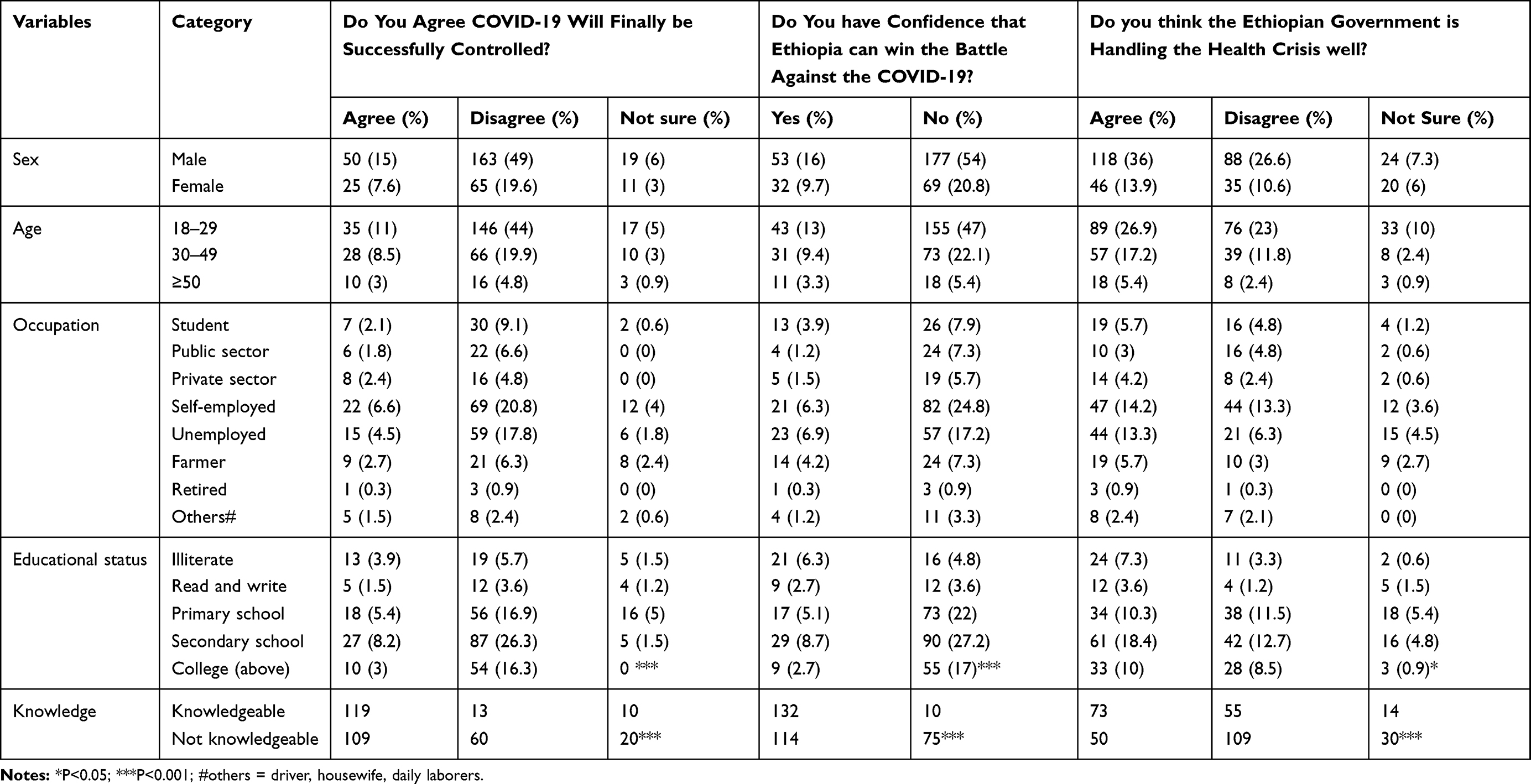 |
Table 4 Socio-Demographic Profile, Knowledge, and Attitude Towards COVID-19, in Tigrai Quarantine Centers, Ethiopia, 2020 (n=331) |
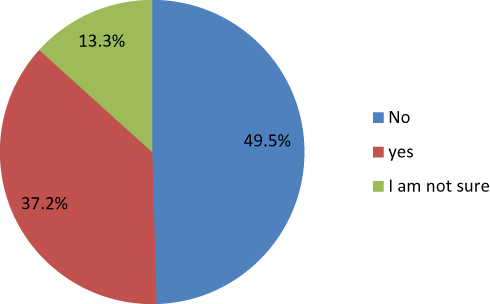 |
Figure 1 Participants believe in government’s handling the health crises. |
Participants Practice Towards COVID-19 Prevention Methods
We used three questions for the assessment of practices to prevent COVID-19. The first question asks if participants have gone to crowded places. Nearly half [165 (49.8%, 95% CI: 44.1–55.3%)] of the participants have gone to crowded places in recent days. Forty-six percent (95% CI: 40.2–51%) of the participants did not use a face mask when leaving home. More than half (54.4%, 95% CI: 48.6–59.8%) of participants did not obey the preventive measures given by local health care authorities.
A chi-squared test showed educational status and knowledge scores were associated with all three questions regarding practices towards COVID-19. As participants got more educated, they tend to practice preventive measures to the pandemic. Those who had an acceptable level of knowledge were more likely to take preventive measures towards COVID-19. No significant difference in going to crowds, wearing a face mask, and taking measures to prevent COVID-19 was seen across gender, age, and occupational groups of study participants (Table 5).
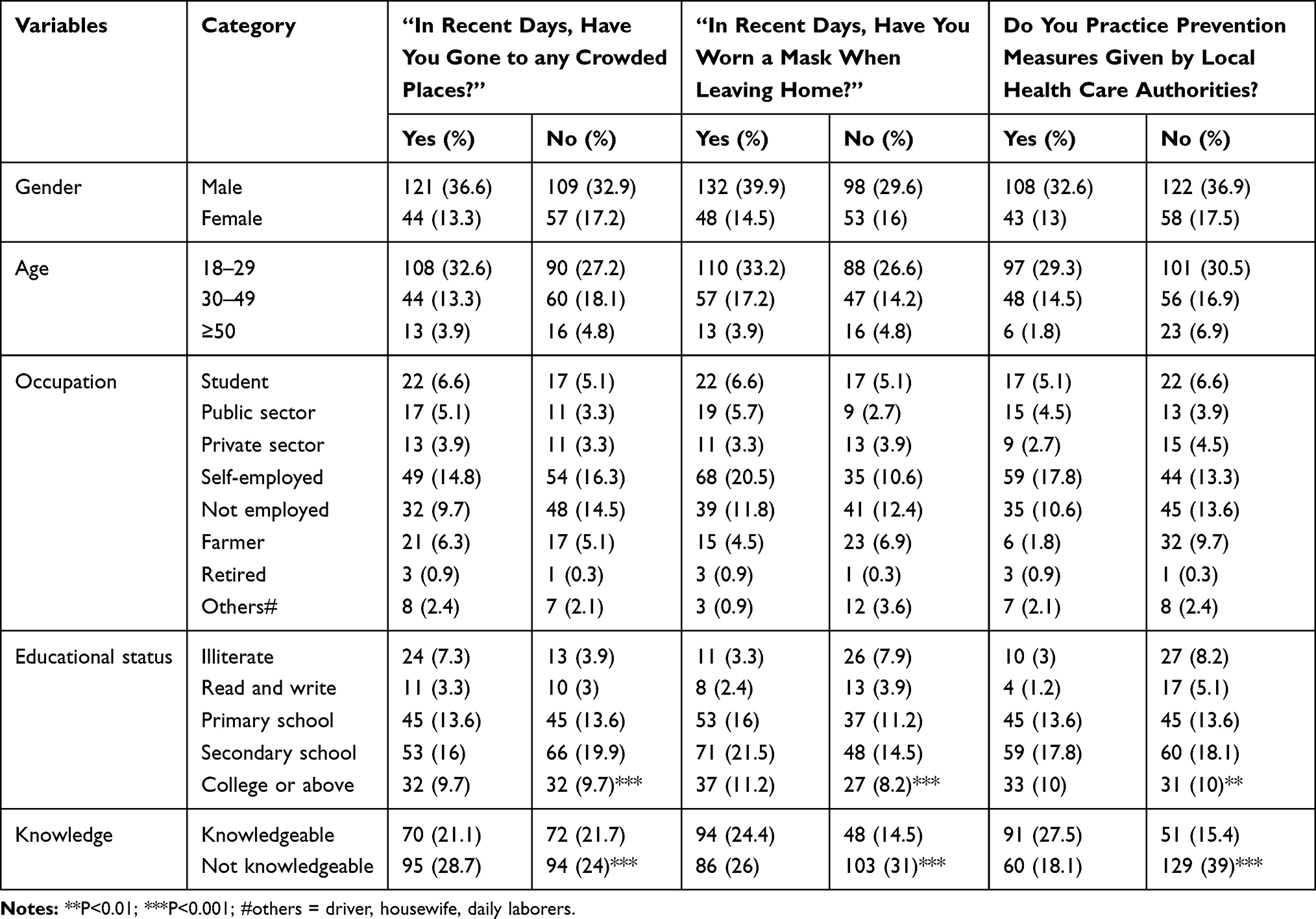 |
Table 5 Demographic Characteristics and Practice to Prevent COVID-19 |
Discussion
After the virus emerged in China, it is argued that information was suppressed, and erroneous. China initially reported that the novel virus showed no evidence of human to human transmission.29,30
To the best of our knowledge, this is the first study done in quarantine centers to assess knowledge, attitudes, and practices (KAP) towards COVID-19 in Ethiopia. Therefore, this study is vital to predicting KAP behaviors towards the pandemic to design appropriate implementation plans. Different studies31–35 have used various methods of measurements for knowledge, attitude, and practice. Despite the reason that more than 3/4th (82.2%) of the total participants have completed primary school or above and it has been more than half a year since the declaration of the pandemic, only 142 [(42.9%) range 0–13 and mean 8.73±2.64] of the participants had an acceptable level of knowledge score regarding COVID-19. This finding is much lower than other studies26–28,32–34,36–41 in different parts of the world. The reason might be due to inadequate access to information. Social media, radio, and television are primary sources of information.26,38,42 However, television channels (Tigrai TV and DW TV), radio (Fana FM radio Mekelle branch), and internet service were blocked in Ethiopia for unknown reasons for a considerable period of time since the onset of COVID-19. Therefore, this lack of access to information sources might have contributed to the low knowledge score level.
Nearly 3/4th of participants correctly answered questions regarding main clinical symptoms of COVID-19 (87.6%), effective cure for COVID-19 and supportive treatment (73.4%), wearing face masks to prevent the pandemic (73.7%), avoiding going to crowded places (81.3%), effectiveness of isolation and treatment of infected individuals (83.1%), immediate isolation of individuals who have contact history (74.6%), and respiratory droplets as vectors to transmit the infection (81.6%). A minimal number of participants [67 (20.2%)] provided the correct answer that eating or contacting wild animals would result in COVID-19. This minimal response could be due to some controversies that wildlife could be the source of the infection.43
Participants were confused about knowledge questions regarding; 1) COVID-19 could be transmitted via respiratory droplets, 2) “Unlike the common cold, stuffy nose, runny nose, and sneezing are less common” symptoms, and 3) COVID-19 is airborne. The confusion could be due to misinformation COVID-19,39,42,44 or it might be due to the local health extension workers’ limitations on knowledge about the pandemic. Gender (being males were more knowledgeable), age (18–29 and 30–49 groupings were more knowledgeable), and educational status (increasing in education tended to increase the knowledge score) were significant predictors of knowledge score. This finding mirrors studies26,27,32,36,38 conducted in different parts of the world. Nearly 70% of the participants agreed that the pandemic would finally be controlled, 74.3% were confident enough to respond that our country Ethiopia will win the battle against the pandemic. Only one-third of them reported that the government is handling the pandemic well. It was expected that majority of them would be optimists to the attitude questions because it has been a considerable time since the pandemic was declared. However, limited resources (personal protective equipment (PPE)) are available in the market to prevent the pandemic; it could be why the participants have an unfavorable attitude.
Our findings are inconsistent with some studies26–28,36,39,45 in which the majority of the participants agreed COVID-19 would finally be controlled, expressed confidence that their country will win the battle against COVID-19, and their government is doing well to control the pandemic. Our findings showed that high levels of educational and good knowledge scores were significantly associated with a favorable attitude towards the pandemic. It is consistent with the study done in China,26 India,36 and Malaysia.28 Participants’ education and knowledge are crucial to having a favorable attitude and preventing the perpetuation of the pandemic.46,47
On average, half of the study participants did not avoid crowded places, use a face mask when leaving home, or practice preventive measures given by local health authorities. It is consistent with studies done in Bangladesh41 where the practice was not impressive and Malaysia28 where only half (51.2%) of the total participants used face mask when leaving home. It is contrary to studies done in Tanzania27 where 77%, and 80% avoided crowds and wore face masks; in India36 where the majority of participants take preventive measures; in China26 where 96.4% and 98% avoided crowding and used a face mask; in Nepal45 where 94.9%, 88.2%, and 93.7% avoided crowded, appropriately used a face mask, and took preventive measures; and in Malaysia28 where 83.4% and 87.8% avoided crowding and took precautionary measures, respectively.
Low report of practices (among all the three practice questions) to prevent COVID-19 was significantly associated with educational status (ie, illiterate persons showed poor practices) and a low level of participants’ knowledge scores. It is consistent with prior studies26,36 in which a high level of education and knowledge predicted good practices. The differences might be that when participants do not have adequate knowledge and are uneducated, they are unlikely to exhibit good practices. It could be due to differences in the participants’ socio-demographic and living standards, COVID-19 caused a shortage of personal protective equipment48 and lack of water49 to meet hygiene recommendation making it difficult to avoid crowds. Most community-based studies26,28,32,36,38,40,45 used online surveys or phone calls, potentially recruiting participants who can read and write and exposed to such media, which may have impacted higher reports of a high level of knowledge, favorable attitude, and good practice towards COVID-19.
Limitations
Social desirability bias was likely, especially regarding attitude and practice questions. The study was conducted among quarantined adults, and the small sample size might not represent the general population. Even though the tool was valid and used in other studies, it would have been better to make it inclusive of all the risk factors related to KAP, and we would have widened questions regarding attitude and practice. However, the limited time we had did not allow us to develop a new tool and go through all reliability and validity testing procedures.
Conclusion
A substantial number of the participants lacked knowledge and poorly adhered to practices related to COVID-19 prevention methods. Approximately 3/4th of the participants agreed that Ethiopia would win the battle against the pandemic, and it will finally be controlled. But only 1/3rd felt that the government is handling the pandemic well. Gender, age, and educational status were significant predictors of knowledge score. Educational status and knowledge scores were significantly associated with attitudes and practices towards COVID-19. The study revealed the presence of sub-optimal knowledge of COVID-19 among guaranteed people underscoring the knowledge gap in the community is worse. Attitude and practice towards COVID-19 were also sub-optimal. Thus, interventions that improve the community’s knowledge, attitude, and practice towards COVID-19 prevention are needed. Researchers around the world might also consider their investment in COVID-19, especially on innovation for new treatments and diagnostics that can be affordable for developing countries. Epidemiological investigations of possible risk factors to COVID-19, and clinical trials for evidence-based practices are also recommended.
Data Sharing Statement
The datasets used and analyzed during for study are available from the corresponding author on reasonable request. Data are available at [email protected].
Ethics Approval and Consent to Participate
Tigrai Regional Health Bureau approved the study (TRHB: 1052/1418/20) and written informed consent was obtained from the study participants.
Acknowledgments
We thank the staff members of all the quarantine centers of the Tigrai region for their cooperation in arranging the eligible study participants. We thank study participants for their genuine responses and participation.
Author Contributions
All authors made a significant contribution to the work reported, in the conception, study design, execution, acquisition of data, analysis, and interpretation, and in all these areas; took part in drafting, revising and critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
The authors declare that they have no financial or non-financial competing interests.
References
1. Cucinotta D, Vanelli M. WHO declares COVID-19 a pandemic. Acta bio-medica: Atenei Parmensis. 2020;91(1):157–160.
2. Gagliano A, Villani PG, Manelli A. et al. COVID-19 epidemic in the middle province of Northern Italy: impact, logistics, and strategy in the first line hospital. Disaster Med Public Health Prep;2020. 1–5. doi:10.1017/dmp.2020.51
3. Huynh TLD. Data for understanding the risk perception of COVID-19 from Vietnamese sample. Data in Brief. 2020;105530.
4. World health organization (WHO). Coronavirus disease ( COVID-19): situation report. 2020.
5. Davies NG, Klepac P, Liu Y, et al. Age-dependent effects in the transmission and control of COVID-19 epidemics. MedRxiv. 2020.
6. Li H, Wang S, Zhong F, et al. Age-dependent risks of incidence and mortality of COVID-19 in Hubei Province and other parts of China. Fron Med. 2020;7:190.
7. Ivailo Lzvorski SM, Moorty L, Gallin A. A policy framework for mitigating the economic impact of COVID-19. 2020; https://www.brookings.edu/blog/future-development/2020/04/20/a-policy-framework-for-mitigating-the-economic-impact-of-COVID-19/.
8. Broberg MA. Critical appraisal of the World Health Organisation’s International Health Regulations (2005) in times of pandemic – it is time for revision. Eur j Risk Regulation. 2020;2:1–9.
9. “COVID-19 pandemic preparedness and response in Ethiopia weekly bulletin”. 2020; https://www.ephi.gov.et/images/novel_coronavirus/EPHI_-PHEOC_COVID-19_Weekly-bulletin_13_English_27_July_2020.pdf.
10. Baye K. COVID-19 prevention measures in Ethiopia: current realities and prospects. Intl Food Policy Res Inst. 2020;141.
11. Shammi M, Bodrud-Doza M, Islam ARMT, Rahman MM. Strategic assessment of COVID-19 pandemic in Bangladesh: comparative lockdown scenario analysis, public perception, and management for sustainability. Environ Dev Sustainability. 2020;1:1–44.
12. Bodrud-Doza M, Shammi M, Bahlman L, Islam ARM, Rahman M. Psychosocial and socio-economic crisis in Bangladesh due to COVID-19 pandemic: a perception-based assessment. Fron Public Health. 2020;8:341. doi:10.3389/fpubh.2020.00341
13. Shammi M, Bodrud-Doza M, Islam ARMT, Rahman M. COVID-19 pandemic, socio-economic crisis, and human stress in resource-limited settings: a case from Bangladesh. Heliyon. 2020;6(5):e04063. doi:10.1016/j.heliyon.2020.e04063
14. Abdi M. Coronavirus disease 2019 (COVID-19) outbreak in Iran; actions and problems. Infect Control Hospital Epidemiology. 2020;1–5.
15. Xu R, Cui B, Duan X, Zhang P, Zhou X, Yuan Q. Saliva: potential diagnostic value and transmission of 2019-nCoV. Int J Oral Sci. 2020;12(1):1–6. doi:10.1038/s41368-020-0080-z
16. Wang L, Shi Y, Xiao T, et al. Chinese expert consensus on the perinatal and neonatal management for the prevention and control of the 2019 novel coronavirus infection. Ann Translational Med. 2020;8:3. doi:10.1186/s12967-019-02180-3
17. Moorthy V, Restrepo AMH, Preziosi M-P SS, Swaminathan S. Data sharing for novel coronavirus (COVID-19). Bull World Health Organ. 2020;98(3):150. doi:10.2471/BLT.20.251561
18. Wei WE, Li Z, Chiew CJ, Yong SE, Toh MP, Lee VJ. Presymptomatic transmission of SARS-CoV-2—Singapore, January 23–March 16, 2020. Morbidity Mortality Weekly Rep. 2020;69(14):411. doi:10.15585/mmwr.mm6914e1
19. Madad S, Moskovitz J, Boyce MR, Cagliuso NV, Katz R. Ready or not, patients will present: improving urban pandemic preparedness. Disaster Med Public Health Prep. 2020;1–4. doi:10.1017/dmp.2020.7
20. Huynh TL. The COVID-19 risk perception: a survey on socioeconomics and media attention. Econ Bull. 2020;40(1):758–764.
21. Huynh TLD. Does culture matter social distancing under the COVID-19 pandemic? Saf Sci. 2020;130:104872. doi:10.1016/j.ssci.2020.104872
22. Huynh TLD. “If you wear a mask, then you must know how to use it and dispose of it properly!”: a survey study in Vietnam. Rev Behav Economics. 2020;7(2):145–158. doi:10.1561/105.00000121
23. Reuben RC, Danladi MM, Saleh DA, Ejembi PE. Knowledge, attitudes, and practices towards COVID-19: an epidemiological survey in North-Central, Nigeria. J Community Health. 2020;1–14.
24. Olum R, Chekwech G, Wekha G, Nassozi DR, Bongomin F. Coronavirus Disease-2019: knowledge, attitude, and practices of health care workers at Makerere University Teaching Hospitals, Uganda. Fron Public Health. 2020:1(8):181.
25. Alzoubi H, Alnawaiseh N, Al-Mnayyis A, Lubad M, Aqel A, Al-Shagahin H. COVID-19-knowledge, attitude and practice among medical and non-medical university students in Jordan. j Pure Appl Microbiol. 2020;14:17–24.
26. Zhong B-L, Luo W, Li H-M, et al. Knowledge, attitudes, and practices towards COVID-19 among Chinese residents during the rapid rise period of the COVID-19 outbreak: a quick online cross-sectional survey. Int J Biol Sci. 2020;16(10):1745. doi:10.7150/ijbs.45221
27. Byanaku A, Ibrahim M. Knowledge, attitudes, and practices (KAP) towards COVID-19: a quick online cross-sectional survey among Tanzanian residents. MedRxiv. 2020;2;1254.
28. Azlan AA, Hamzah MR, Sern TJ, Ayub SH, Mohamad E. Public knowledge, attitudes, and practices towards COVID-19: a cross-sectional study in Malaysia. PLoS One. 2020;15(5):e0233668. doi:10.1371/journal.pone.0233668
29. Ogden C. The role of competing narratives in China and the West’s response to COVID-19. British j Chin Studies. 2020:2;145.
30. Davidson H. Chinese inquiry exonerates coronavirus whistleblower doctor. Guardian. 2020;20.
31. Haryana D. Comparative study of knowledge, attitude, and practice (KAP) of a global pandemic, COVID-19 in urban population of Rohtak, a suburb near Delhi. Alochana Chakra Journal. 2020.
32. Alahdal H, Basingab F, Alotaibi R. An analytical study on the awareness, attitude, and practice during the COVID-19 pandemic in Riyadh, Saudi Arabia. J Infect Public Health. 2020;13(10):1446–1452. doi:10.1016/j.jiph.2020.06.015
33. Roy D, Tripathy S, Kar SK, Sharma N, Verma SK, Kaushal V. Study of knowledge, attitude, anxiety & perceived mental healthcare need in Indian population during COVID-19 pandemic. Asian J Psychiatr. 2020;51:102083. doi:10.1016/j.ajp.2020.102083
34. Al Ahdab S. Knowledge, attitudes, and practices (KAP) towards pandemic COVID-19 among Syrians. Res Square. 2020.
35. Ferdousa MZ, Islama MS, Sikdera MT, Md AS. Knowledge, attitude, and practice regarding COVID-19 outbreak in Bangladesh: an online-based cross-sectional study. MedRxiv Preprint. 2020.
36. Tomar BS, Singh P, Nathiya D, et al. Indian communitys knowledge, attitude & practice towards COVID-19. MedRxiv. 2020.
37. Karim A, Akter M, Mazid AT, et al. Knowledge and attitude towards COVID-19 in Bangladesh: population-level estimation and a comparison of data obtained by phone and online survey methods. MedRxiv. 2020.
38. Abdelhafiz AS, Mohammed Z, Ibrahim ME, et al. Knowledge, perceptions, and attitude of Egyptians towards the novel coronavirus disease (COVID-19). J Community Health. 2020;1–10.
39. Bhat Bilal A. Awareness, attitude, and practice of rural people in Kashmir towards COVID-19: a sample survey. IJSDR. 2020.
40. Vaidya B, Bhochhibhoya M, Baral R, Nakarmi S. Knowledge, attitude and practice towards COVID-19 among patients with musculoskeletal and rheumatic diseases in Nepal: a web-based cross-sectional study. Res Square. 2020:5:126.
41. Haque T, Hossain KM, Bhuiyan MMR, et al. Knowledge, attitude and practices (KAP) towards COVID-19 and assessment of risks of infection by SARS-CoV-2 among the Bangladeshi population: an online cross-sectional survey. Res Square. 2020:2:458.
42. Saqlain M, Munir MM, Rehman S, et al. Knowledge, attitude, practice, and perceived barriers among healthcare professionals regarding COVID-19: a cross-sectional survey from Pakistan. J Hospital Infect. 2020;105(3):419–423. doi:10.1016/j.jhin.2020.05.007
43. Vox. “How wildlife trade is linked to coronavirus” online video clip youtube, youtube, 2020.
44. Malik S. Knowledge of COVID-19 symptoms and prevention among Pakistani adults: a cross-sectional descriptive study. PsyArxiv Preprint. 2020.
45. Hussain A, Garima T, Singh BM, Ram R, Tripti RP. Knowledge, attitudes, and practices towards COVID-19 among Nepalese residents: a quick online cross-sectional survey. Asian j Med Sci. 2020;11(3):6–11. doi:10.3126/ajms.v11i3.28485
46. McEachan R, Taylor N, Harrison R, Lawton R, Gardner P, Conner M. Meta-analysis of the reasoned action approach (RAA) to understanding health behaviors. Ann Behav Med. 2016;50(4):592–612. doi:10.1007/s12160-016-9798-4
47. Desai AN, Patel P. Stopping the spread of COVID-19. J Am Med Assoc. 2020;323(15):1516. doi:10.1001/jama.2020.4269
48. Kampf G, Scheithauer S, Lemmen S, Saliou P, Suchomel M. COVID-19-associated shortage of alcohol-based hand rubs, face masks, medical gloves, and gowns – proposal for a risk-adapted approach to ensure patient and healthcare worker safety. J Hospital Infect. 2020;105(3):424–427. doi:10.1016/j.jhin.2020.04.041
49. Behailu M, Haile M Water harvesting in northern Ethiopia: environmental, health, and socio-economic impacts. Integrated water and land management research and capacity building priorities for Ethiopia. 2002;185.
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.