")
Back to Journals » Risk Management and Healthcare Policy » Volume 12
Knowledge, attitude and practice towards dengue fever prevention and associated factors among public health sector health-care professionals: in Dire Dawa, eastern Ethiopia
Authors Mohammed Yusuf A , Abdurashid Ibrahim N
Received 28 November 2018
Accepted for publication 27 March 2019
Published 7 June 2019 Volume 2019:12 Pages 91—104
DOI https://doi.org/10.2147/RMHP.S195214
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Kent Rondeau
Amir Mohammed Yusuf,1 Neil Abdurashid Ibrahim2
1Department of Public Health, Harar Health Science College, Harar, Ethiopia; 2Department of Midwifery, College of Medicine and Health Science, Dire Dawa University, Dire Dawa, Ethiopia
Background: The Ethiopian national strategy for the prevention, control and elimination of malaria is one of the Health Development Programs (HDP IV). Dengue fever is one of the vector borne diseases that causes Acute Febrile Illness and death in tropical and sub-tropical countries. Knowledge, attitude and practice of health-care professionals towards dengue fever prevention and associated factors among health professionals is not yet well known across the country and concern is varied in context and place. Therefore, the aim of this research was to assess knowledge, attitude and practice towards dengue fever prevention and associated factors among public health sector health-care professionals in Dire Dawa administrative city, eastern Ethiopia.
Materials and methods: An Institution-based cross sectional study was conducted from September 9 to October 13, 2017. The study was conducted among a sample of 348 health-care professionals which were from the randomly selected nine clusters of public health facilities located in urban and rural areas of Dire Dawa. Data were collected by self-administered structured questionnaire. Bivariate and multinomial logistic regression analyses were made to check the associations among predictor variables and to control for confounding factors. A P-value <0.05 was used to declare statistical significance.
Results: Of the 348 sampled health-care professionals, 300 were included in the analysis giving a response rate of 86.2%. Nearly half (148/49.3%) of the participants demonstrated a moderate level of knowledge, 140 (46.7%) a neutral level of attitude and 156 (52%) a low level of practice towards dengue fever prevention. Multinomial logistic regression revealed that type of health profession, type of health facility and dengue fever prevention training status were significantly associated with the knowledge, attitude and practice of health-care professionals. The odds of physicians and public-health officers having a high level of knowledge or a low knowledge level were (AOR [95% CI] =38.793 [7.279, 206.734]) and (AOR[95% CI] =6.15[1.643, 23.026]) times higher than the odds for nurse professionals. The odds for professionals who worked in health centers and had a high knowledge level towards dengue fever prevention were (AOR [95% CI] =0.252 [0.086, 0.737]) times higher than those working in referral hospitals. The odds of health-care professionals who were public-health officers and those who worked in primary hospitals having a favorable attitude towards dengue fever prevention were (AOR [95% CI] =7.011 [1.867, 26.321]) and (AOR [95% CI] =3.683 [1.284, 10.563]) times higher than the odds for nurse professionals and those who worked in a referral hospital setting respectively. The odds of health-care professionals who took dengue fever prevention training were 10.23 times (AOR [95% CI] =10.23 [1.052, 99.478]) higher than the odds for health-care professionals who had not received the training.
Conclusion: Knowledge attitude and practice of health-care professionals were not satisfactory towards dengue fever. Additional training is required to plug this gap. Thus, the regional health bureau and stakeholders should follow up and provide support including provision of the World Health Organization’s standardized guidelines of dengue fever prevention. We recommend similar studies to be done specifically in Ethiopia and elsewhere to better understand the gaps.
Keywords: dengue fever, knowledge, attitude, practice, health care professionals
Introduction
Dengue virus is a single-stranded RNA virus with four serotypes (DENV 1–4) which belong to the genus Flavivirus of the Flaviviridae family.1–3 The arbovirus commonly called break bone fever4 is transmitted to humans by the Aedes aegyptimosquito and Aedes albopictus5 Dengue fever is characterized by fever, which lasts from 5 to 7 days with two or more symptoms: headache, retro-orbital pain, myalgia, arthralgia, rash, hemorrhagic manifestations, or leucopenia.6 Infection with additional dengue serotypes increases the risk of hemorrhagic disease, resulting in severe mucosal and gastrointestinal bleeding, hypovolemia and potentially death.1 Population growth, increased movement of individuals, rapid urbanization, limited financial and human resources, environmental changes and neglected (rural and slums) areas are attributed to vector breeding and the rise in dengue outbreaks.7–9
Dengue virus infection is found in tropical and sub-tropical regions around the world, is increasingly recognized as one of the world’s emerging infectious diseases10 and has become a major international public health concern.11 The World Health Organization estimated that about 2.5 billion people are at risk for dengue fever and, in recent decades, its incidence rate around the world has increased and become an important public health issue.12 The actual numbers of dengue cases have been underreported and misclassified. One recent estimate indicates that there are 390 million dengue infections per year, of which 96 million manifest clinically with any severity of World Health Organization disease classification (Dengue Fever, Dengue Hemorrhagic Fever and Dengue Shock Syndrome).3,13 In the absence of changes in other determinants, studies suggest that climate change could expose an additional 2 billion people worldwide to dengue transmission by the 2080s.14 An estimated 500,000 people with severe dengue (DHF/DSS) require hospitalization each year and about 2.5% of those affected will die.15 In addition, severe dengue (DHF/DSS) remains a leading cause of hospitalization and death of children in at least eight Southeast Asian countries.16 In Africa, dengue fever outbreak has been reported and confirmed in Mauritania, Senegal, and Ethiopia. Dengue is likely under-recognized and under-reported in Africa due to low awareness of health-care providers, other prevalent febrile illnesses, lack of diagnostic testing, and systematic surveillance.17
Most researchers conducted previously were mainly in Asia and focused on how community members view dengue infections; however, there have been few attempts to date to better understand the perspectives of clinicians.18–23 A study conducted in Taiwan among health professionals towards their knowledge on mosquito-transmitted diseases (Malaria, yellow fever and dengue fever) showed significant knowledge deficits.22 Similarly, in a study in Karachi, physicians had basic knowledge but were lacking in clinical diagnosis and management and needed training.18 Whereas a study conducted in Pakistan showed that practitioners had a stronger understanding of dengue patho-physiology than clinical diagnosis and treatment.24 Among primary health-care professionals in Makkah (Saudi Arabia), more than half of them had an excellent knowledge regarding clinical presentation of dengue fever (DF) but insufficient knowledge towards DF diagnosis.25 A study conducted in Abidjan (Cote d’Ivore) among health professionals working in public hospitals showed that one fifth of health professionals had a good knowledge and good diagnostic practice of DF and three-quarters of them knew dengue is a series illness.26 Treatment and management of dengue with co-morbidities is a major health problem, because it causes deaths.27,28 In major cities of Pakistan, half of the physicians surveyed were not aware of the management of dengue patients with liver disease and taking medicines like metformin.29 A recent report showed that 60% of dengue cases had co-morbidities. Hepatitis B and C were major risks to developing dengue shock syndrome.30
One of the HSDP-IV national strategy of Ethiopian is prevention, control and elimination of malaria.31 The prevention and control of dengue outbreak mainly depends on the epidemiological surveillance of cases and mosquito vectors.32,33 Dengue fever emerged for the first time in the eastern part of the country14 and the outbreak continued in this area with more than 12,000 cases reported to the World Health Organization since 2013.34 Also a total of 6,192 new dengue fever cases were reported from Gode of Somalia region, Hadar of Afar region and Dire Dawa city administration in May 2014.35 And it becomes an ongoing outbreak in Dire Dawa city administration and so far about 106 cases were reported by the date of study onset in 2017.36
Since there is no previous study done regarding the knowledge, attitude and practice (KAP) of health-care professionals (HCPs) towards dengue fever prevention and associated factors in Ethiopia including the study area, this study expected to provide evidence-based information in order to bridge the gaps and be used as a milestone for policy makers to improve the prevention of and control the outbreak of the disease.
Materials and methods
Study design and setting
An institution-based cross-sectional study was conducted from September to October 2017, in Dire Dawa administrative city, which is located 515 km from the capital city of Ethiopia. According to the 2009 census of the Dire Dawa regional health bureau (DRHB), the total population of the city was 466,000. The city has one referral hospital, one primary hospital, 15 health centers (seven in rural and eight in urban areas), 32 health posts, three private hospitals, two higher clinics and 32 mid-level clinics. The source populations were all health-care professionals working in Dire Dawa public health facilities. The study population wwas the total number of HCPs (physicians (GPs), nurses and public-health officers) working in selected Dire Dawa public health facilities and who were working and available at the time of data collection.
Sampling size determination and sampling technique
The sample size was calculated using a single population proportion formula (n= Zα/22p (1−p)/d2) by considering the following assumption; prevalence of knowledge about dengue fever prevention was taken as 0.5 (as there was no previous data available in Ethiopia and elsewhere with a similar setting), 95% level of confidence (Zα/2=1.96), 5% margin of error (d=0.05), making the sample size of 384. However, the total numbers of HCPs working in the selected public health facilities were 348, all of them were included in the study so there was no need for sampling. From the total of 17 public health facilities located in both urban and rural areas of the city administration, nine (seven health centers and two hospitals) were selected using SRS technique and included in the study. In total, 107 HCPs were found in urban and rural health centers. Three health centers from rural areas with a total of 29 HCPs (Wahil health center: eleven HCPs, Jelobelina health center: nine HCPs and Kalicha: 9 HCPs) and the four health centers from urban residency were: Dire-Dawa, Adiss-ketema, Legehare and Gende-gerada with distribution of HCPs 17, 19, 25 and 18 respectively. The two hospitals included were Dilchora referral hospital and Sabiyan primary hospital with 240 HCPs together (175 and 65 HCPs respectively). Our study subjects were primary physicians (G.Ps), public-health officers and nurses because in our set up or context they are the first-line health-care providers to diagnose, notify and manage dengue fever cases. The health professional to population ratio in the city administration were 1:1,324 for nurses, 1:18,957 for public-health officers and 1:6,796 for physicians in 2009.31 Data collection and analysis
Data were collected using a structured self-administered questionnaire which was initially prepared in English then translated into the local language (Amharic) by an individual who had a good knowledge of the language. It was then translated back to English to check for any inconsistencies. The 31-item questionnaires were adapted from the literature25 and composed of four parts: The first part asked about the socio-demographic characteristics of the HCPs. The second part consisted of knowledge assessment questions towards dengue fever prevention and the third part assessed the attitude of HCPs towards dengue fever prevention using a fivepoint Likert scale, where 1 indicated “strongly disagree” and 5 “strongly agree.” And the final part assessed the practice of HCPstowards dengue fever prevention. Pre-testing was done on 18 (5%) of total sample size in another health facility outside the study setting and before the actual data collection and then necessary modifications and corrections were made accordingly before using it for the actual study. Validity and reliability analysis was done. The tool was found to be reliable with Cronbach’s alpha (r) of 0.72, 0.73 and 0.79 for knowledge, attitude and practice respectively. Before Data were collected verbal consent was obtained from the HCPs. The collected data were cleared and entered into EPIDATA 3.0 then exported to SPSS Version 23 (IBM Corporation, Armonk, NY, USA) for analysis. Univariate analysis was done to describe the socio-demographic section of the data and for categorical variables frequency tables and percentages were calculated. Based on bloom’s cut off points we have classified knowledge and practice into three levels. Knowledge- and practice-based questions were analyzed by calculating the cumulative knowledge and practice score percent as an aggregate of all questions and a score from zero to one point was given accordingly for appropriate responses that the participants were familiar with their choice of responses and then calculated participants cumulative score percent. Knowledge (Low <60%), (Moderate 60–80%) and (High 80–100%); Practice (Low level <60%), (Moderate level 60–80%) and (High level 80–100%). Attitude questions were analyzed based on a Likert scale and calculated for cumulative score of participants with maximum possible score of 5 points per question for a total of 10 items and categorized into three scoring categories based on the literature (Favorable attitude: 39–50 score, neutral: 33–38 score and unfavorable <32 score).32 Variables in the bivariate analysis with P-value ≤0.25 were considered for the final multinomial logistic regression model. The strength of statistical association was measured by AOR at 95% CI. Statistical significance was declared at P<0.05.
Ethics statement
Ethical clearance was obtained from the Ethical clearance committee of the College of Public Health and Medical Sciences of Jimma University (Reference number: IHRPGD/849/17). Study participants were oriented and informed about the objective of the study. Then, written/verbal informed consent was secured from each study participant prior to commencement of data collection.
Results
Socio-demographic characteristics
From a total of 348 study subjects, 300 were included in the analysis giving a response rate of (86.2%); among these, 165 (55%) were females and 162 (98.2%) were in the age group between 21 and 40 years old. The mean age of HCPs was 29.89 (SD ±6.21) years and the majority of participants 95 (65%) possessed a BSc degree. More than four-fifths of the participants were nurses 247 (82.3%) and only 10 (3.3%) of the HCPs (3 (1%) nurses, 4 (1.3%) public health officers and 3 (1.3%) physicians) had received training regarding dengue fever prevention. The mean experience of HCPs was 6.73 years and the majority (155/51.7%) of HCPs were from a referral hospital setting (Table 1).
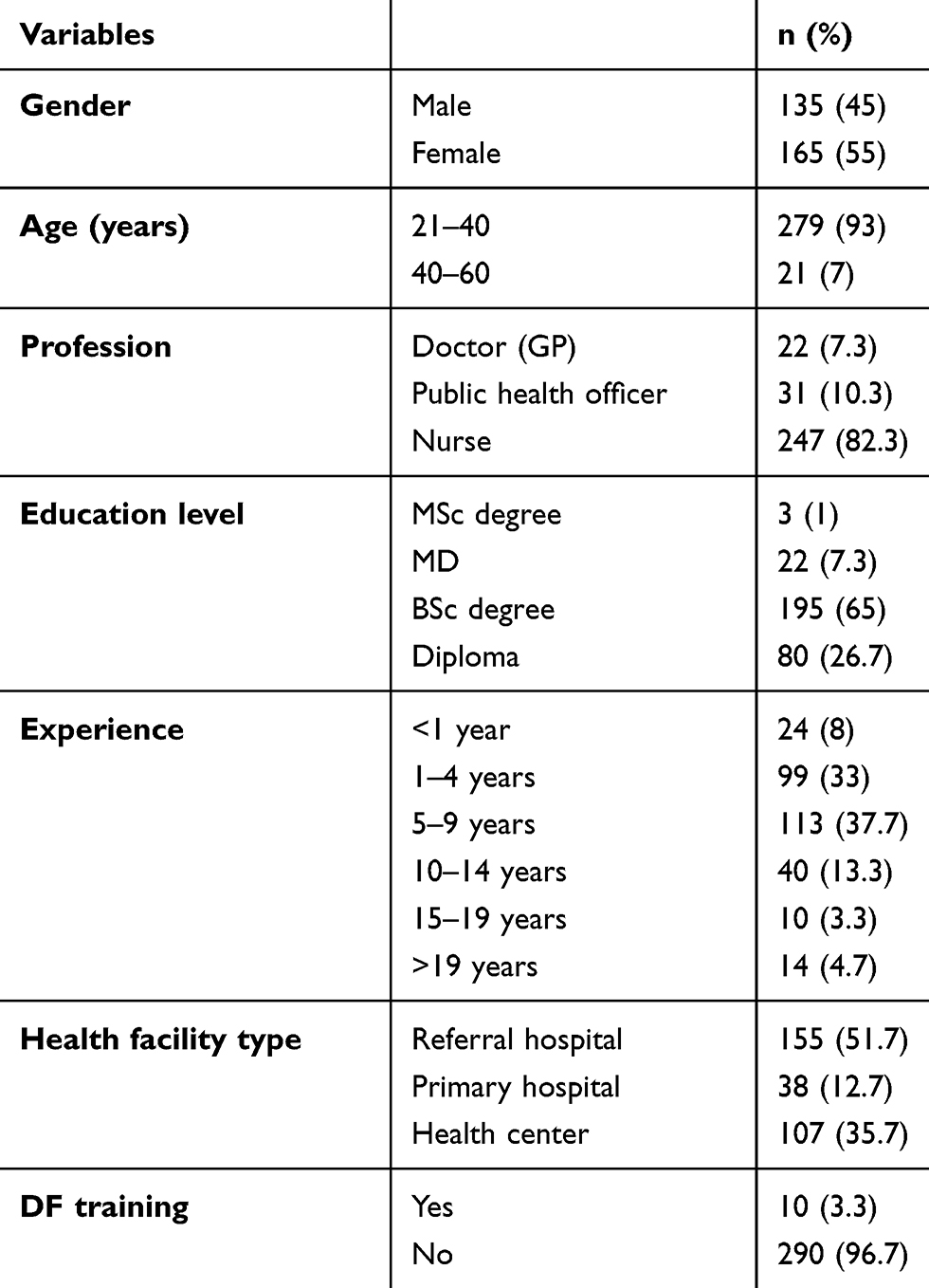 | Table 1 Socio-demographics of HCPs working in public health facilities (N=300) in Dire Dawa, eastern Ethiopia, 2017 |
Knowledge of HCPs towards DF prevention
Knowledge is categorized into high, moderate and low based on Bloom’s cut off. Nearly half of the HCPs 148 (49.3%) demonstrated a moderate level of knowledge and only 31 (10.3%) demonstrated a high level of knowledge while the rest 121 (40.3%) demonstrated a low level of knowledge towards DF prevention. Overall, 270 (90%) HCPs correctly identified treatments that could be used in a patient suspected to have dengue (Table 2).
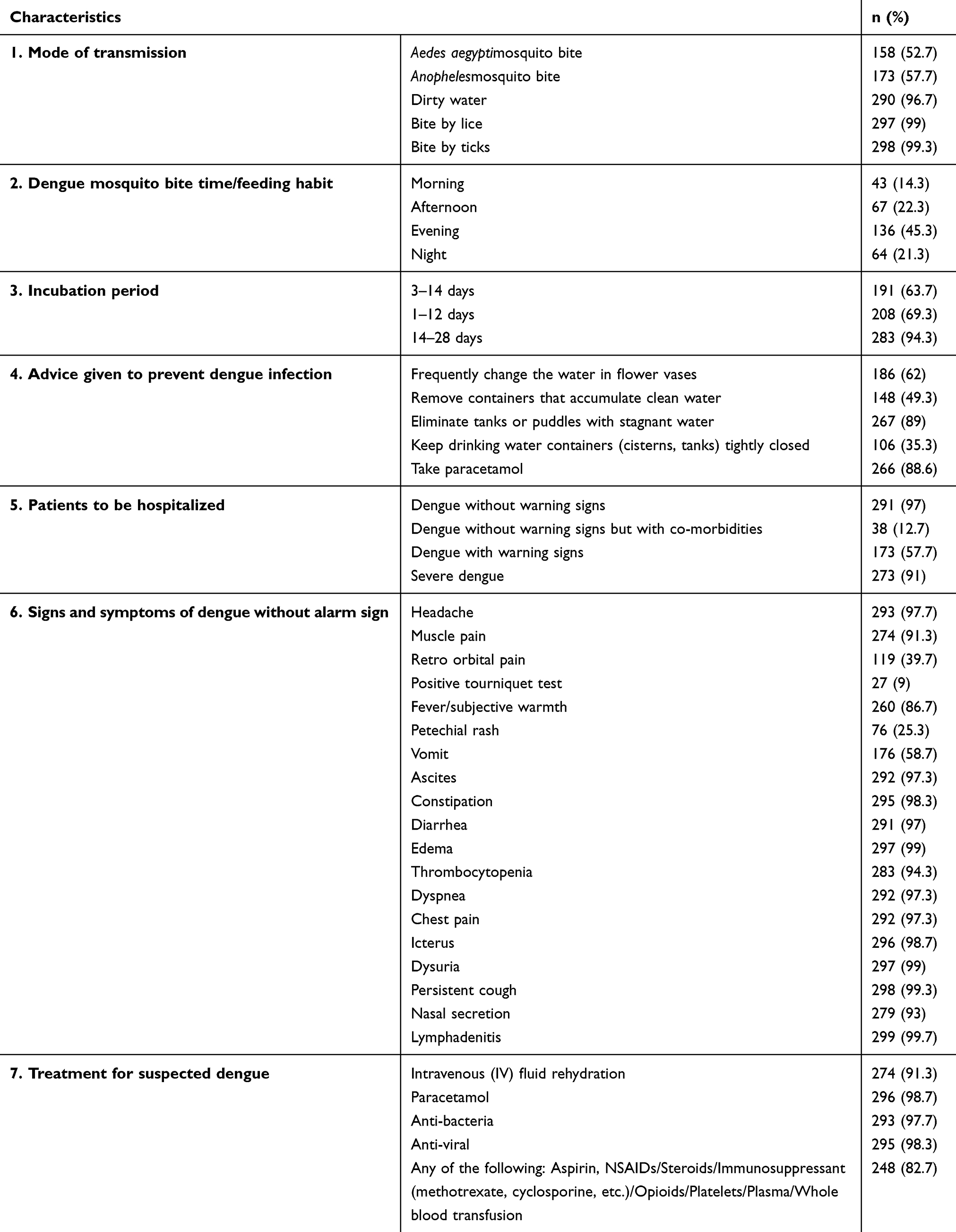 | Table 2 Knowledge assessment of DF prevention among HCPs (N=300) working in public health facilities in Dire Dawa, eastern Ethiopia, 2017 |
Attitude of HCPs towards DF prevention
Less than a quarter 68 (22.7%) of HCPs showed a favorable attitude towards DF prevention but the remaining 140 (46.7%) and 92 (31%) participants showed a neutral and unfavorable attitude towards dengue prevention, respectively. More than half 168 (56%) were not trained to manage patients with an infection of dengue without alarming signs and 133 (44.3%) were agreed that dengue has high morbidity, of which 41 (31%) of them agreed dengue decreases economic productivity (Table 3).
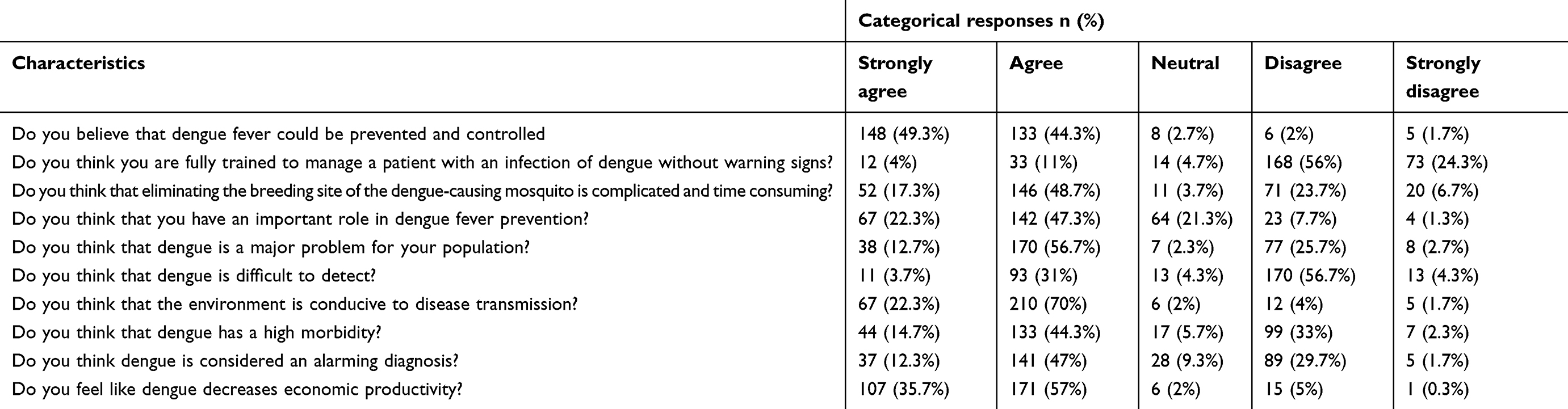 | Table 3 Opinion about DF prevention among HCPs working in public health facilities (N=300), Dire Dawa, eastern Ethiopia, 2017 |
Practice of HCPs towards DF prevention
Only 71 (23.7%) HCPs demonstrated a high level of practice and the remaining 78 (24.3%) and 156 (52%) had moderate and low levels of practice towards DF prevention respectively. The majority (197/66%) of HCPs saw DF cases in the health facility and 255 (85%) of participants reported they were not familiar with the WHO’s 2010 dengue clinical management guideline and 201 (67%) reported that they did not have adequate resources to treat patients with dengue. From the study subjects, 191 63.7%) were lacking training, 12 (4%) were lacking medication needed to treat dengue, 9 (3%) were lacking instruments needed to treat DF. The rest, 74 (24.7%) were lacking access to laboratory tools (Table 4).
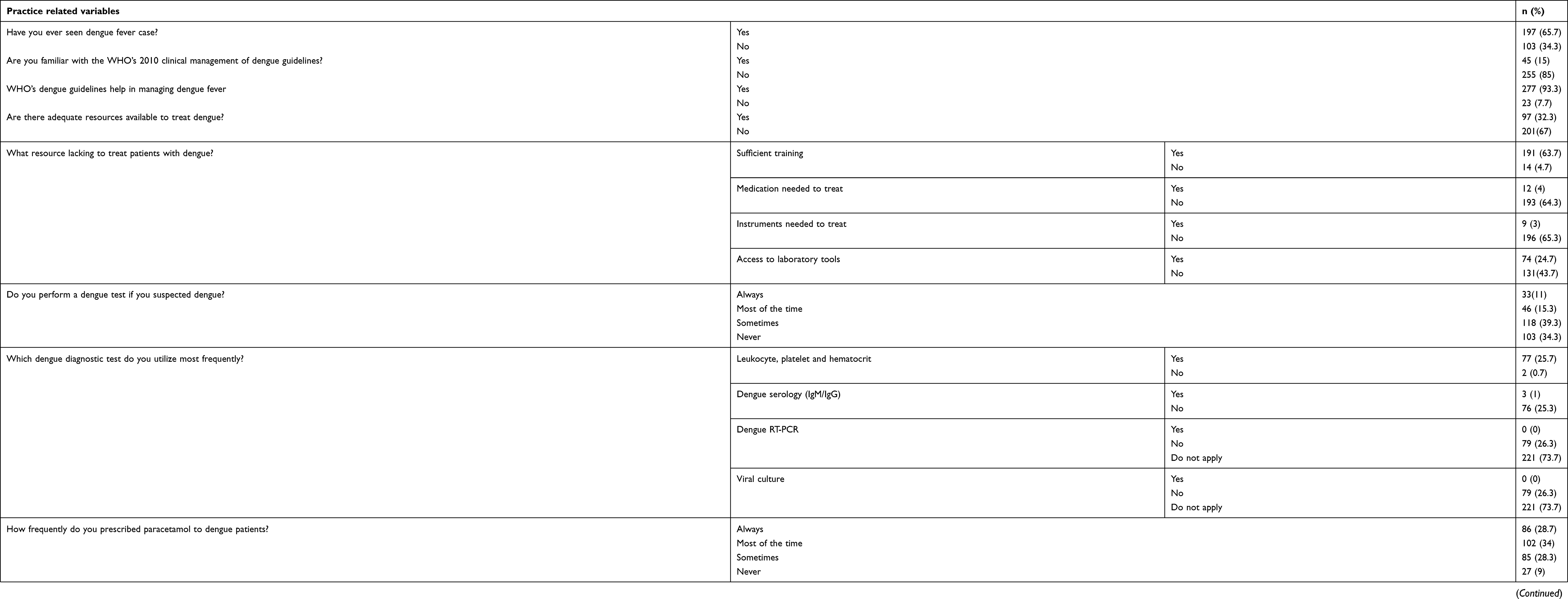 | Table 4 Practice towards DF prevention among HCPs (N=300) working in public health facilities in Dire Dawa, eastern Ethiopia, 2017 |
Factors associated with knowledge level of HCPs towards DF prevention
All predictor variables (sex, age, type of profession, experience, practice setting and dengue training status) were checked individually for the presence of association in bivariate analysis and those variables with P-value less than 0.25 were sex, age, type of profession and practice setting were associated with the knowledge level of HCPs in bivariate analysis. However, in the final model only type of profession and type of health facility (practice setting) were significantly associated (P<0.05) with the knowledge level (High) of HCPs towards DF prevention. So, the odds of HCPs who were physicians and public health officers having a high rather than a low knowledge level were 38.793 times (AOR[95% CI] =38.793 [7.279, 206.734]) and 6.15 times (AOR[95% CI] =6.15 [1.643, 23.026]) higher than the odds for nurses respectively. HCPs who worked in health centers having a high rather than a low knowledge of DF prevention were 74.8% lower than the odds for HCPs who worked at a referral hospital (AOR [95% CI] =0.252 [0.086, 0.737]) (Table 5).
 | Table 5 Bivariate and multinomial logistic regression model showing factors associated with a high level of knowledge of HCPs towards DF prevention in Dire Dawa public health facilities, eastern Ethiopia, 2017 (N=300) |
Factors associated with attitude of HCPs towards DF prevention
In the bivariate analysis, sex, type of profession and practice setting were associated (P<0.25) with the attitude of HCPs towards DF. However, in the multinomial logistic regression only type of profession and type of health facility (practice setting) were significantly associated with the attitude level (favorable and neutral) of HCPs towards DF prevention.
The odds of HCPs who were public health officers and who worked in primary hospitals and had a positive rather than negative attitude were 7.011 times (AOR [95% CI] =7.011 [1.867, 26.321]) and 3.683 times (AOR [95% CI] =3.683 [1.284, 10.563]) higher than the odds for nurses and referral hospital workers towards DF prevention respectively. The odds of HCPs who were public health officers having a neutral rather than negative attitude were 3.452 times (AOR [95% CI] =3.452 [1.126, 15.027]) higher than the odds for nurse professionals towards dengue fever prevention (Tables 6 and 7).
 | Table 6 Bivariate and multinomial logistic regression model showing factors associated with a favorable attitude level of HCPs (N=300) towards DF prevention in Dire Dawa public health facilities, eastern Ethiopia, 2017 |
 | Table 7 Bivariate and multinomial logistic regression model showing factors associated with a neutral attitude level of HCPs towards DF prevention in Dire Dawa public health facilities, eastern Ethiopia, 2017 (N=300) |
Factors associated with practice level of HCPs towards DF prevention
All variables like sex, age, type of profession, practice setting and dengue training status were checked for the presence of association in the bivariate analysis. Hence, age, sex, type of profession, practice setting and DF training status were significantly associated with the practice level of HCPs towards DF prevention. However, in the multinomial logistic regression analysis, type of profession, type of health facility and DF training status were significantly associated with the practice level of HCPs towards DF prevention. The odds of physicians and public health officers having a high rather than a low practice level were 17.618 times (AOR [95% CI] =17.618 ([.072, 149.787]) and 7.65 times (AOR [95%CI] =7.65 [2.523, 23.194]) higher than the odds for nurses towards dengue fever prevention. The odds of HCPs who took DF training were 10.23 times (AOR [95% CI] =10.23 [1.052, 99.478]) higher than the odds for HCPs who had not received DF prevention training. The odds of male HCPs having a moderate rather than a low level of practice was 2.211 times (AOR [95% CI] =2.211 [1.179, 4.146]) higher than the odds for female HCPs. The odds of having a moderate rather than a low level of practice among physicians and public health officers were 28.524 times (AOR [95% C.] =28.524 [3.500, 232.436]) and 4.706 times (AOR [95% CI] =4.706 [1.466, 15.108]) higher than the odds for nurses towards DF prevention respectively (Tables 8 and 9).
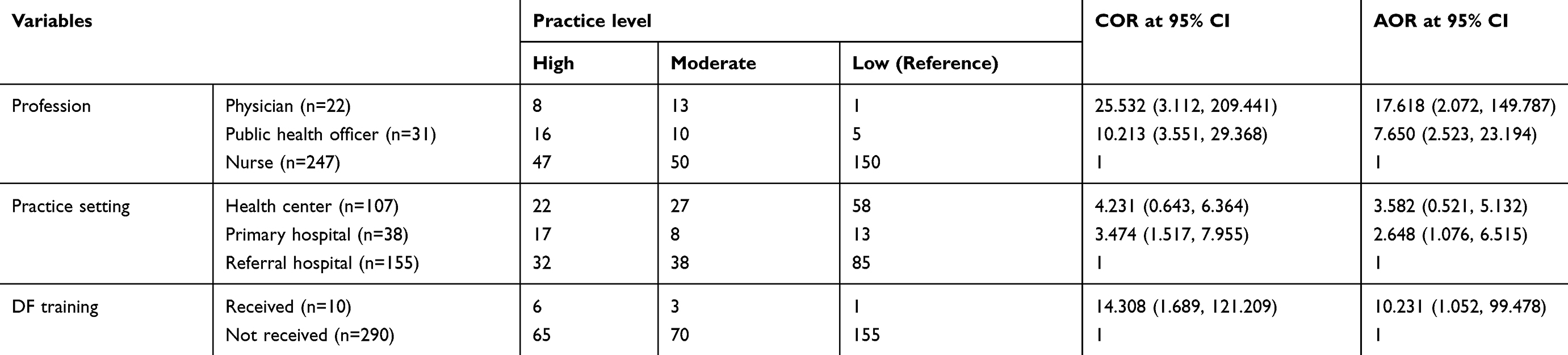 | Table 8 Bivariate and multinomial logistic regression model showing factors associated with a high practice level of HCPs (N=300) towards DF prevention in Dire Dawa public health facilities, eastern Ethiopia, 2017 |
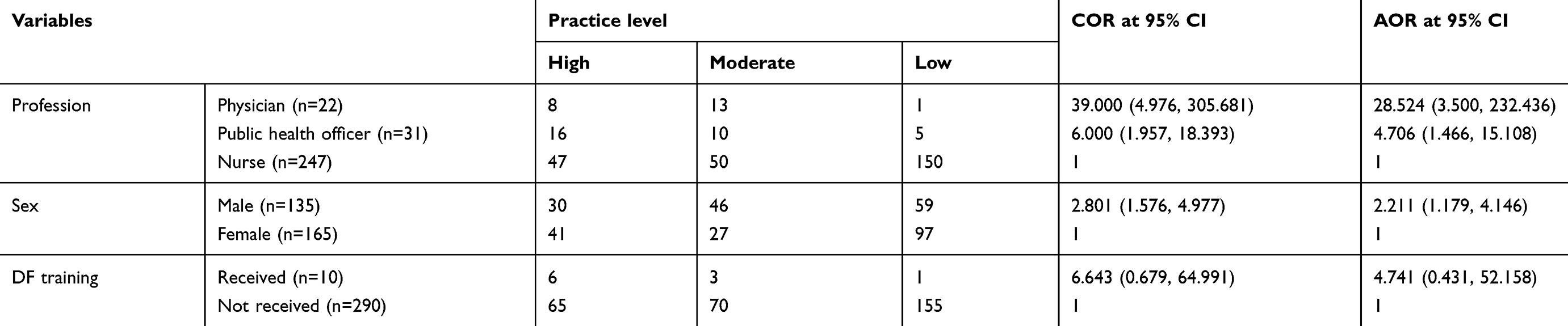 | Table 9 Bivariate and multinomial logistic regression model showing factors associated with a moderate practice level of HCPs (N=300) towards DF prevention in Dire Dawa public health facilities, eastern Ethiopia, 2017 |
Discussion
Primary physicians and nurses serve as the first-line health care providers to diagnose, notify and treat dengue cases. The KAP of HCPs regarding dengue diseases also provide early recognition and improve the outcome of dengue.21,37 According to this study, the larger proportion of HCPs 148 (49.3%) demonstrated a moderate level of knowledge towards dengue fever prevention. One of the possible reasons attributed to this might be the lack of training of the first line HCPs towards the subject matter. It has also identified specific gaps in knowledge of dengue infection, prevention and management. A total of 63 (21%) HCPs did not correctly identify the correct time of feeding habit of the Aedes mosquito. This finding is higher than a study conducted in Taiwan 14.4%.22 However, in both cases the result was low and may reflect a significant knowledge gap of health care providers towards the Aedes mosquito.
The attitude of HCPs towards DF prevention was largely neutral 138 (46%). This is because the study was conducted among different HCPs who provided health services at different health facility sites (urban versus rural), different health service departments, responsibilities and some of the HCPs might not have even seen a dengue case. Of the total, 168 (56%) HCPs reported that they were not fully trained to manage a patient with an infection of dengue without alarming signs. This simply indicates the majority of HCPs general lack of training about DF prevention and hence this shows the need for an avenue to be created to plug this gap in knowledge.
In this study, more than half, 156 (52%) HCPs demonstrated a low level of practice towards DF prevention. This might be due to one-third of our study areas being rural health centers where cases of DF were unusual. Another possible reason could be the lack of diagnostic testing.30 No published study has evaluated specifically the practice level of HCPs towards DF prevention and hence limited our comparison. Only 45 (15%) of the HCPs reported they were familiar with the WHO’s 2010 dengue clinical management guideline. This finding was inconsistent and much lower than a study done on Sri Lankan practitioners 45%.18 The possible explanation could be Kularatne’s study was conducted prior to the current version of the WHO dengue guidelines and might be more cognate to local context. And it was also noted that there was an absence of WHO dengue standard guidelines across most of the study sites.
In our study, 201 (67%) of the HCPs reported the presence of inadequate resources to treat dengue patients. This result is much higher than a study conducted in Machala, Ecuador (31%).17 This difference might be due to differences in the health settings, health system management and economic set up of Ecuador. Overall, only 45 (15%) of our HCPs “most of the time” perform a dengue test when they suspect dengue. This is lower than a study done in Makkah, Saudi Arabia (75%).38 This difference might be due to the fact that the incidence of dengue fever and dengue hemorrhagic fever has increased significantly in Makkah over the last few years38 and endemic occurrence of the disease in the city was recently confirmed which increased the physicians’ suspicion of the diseases.
Based on multinomial logistic regression, type of health profession and type of health facility were significantly associated with a high level of knowledge of HCPs towards DF prevention. The physicians and public health officers were 38.793 and 6.15 times more likely to have a highrather than a low level of knowledge towards DF prevention when compared with nurse professionals’ respectively. The possible explanation for this difference might be differences in educational qualifications and responsibilities. No published studies are in line with our current study and hence limited the comparison. HCPs who worked in health centers were 74.8% times less likely to have a high rather than a low level of knowledge towards DF prevention when compared with HCPs who worked in referral hospital settings. Similarly, type of profession and type of health facility were significantly associated with a positive attitude level of HCPs towards DF prevention. Public health officers were 7.011 times more likely to have a positive rather than a negative attitude towards DF prevention when compared to nurse professionals. This is because public health officers are usually involved in patient diagnosis and management in the outpatient department and might have frequent exposure to DF cases.
Similarly, type of profession and DF training status were significantly associated with the high level of practice of HCPs towards DF prevention. Physicians were 17.618 times and public health officers were 7.65 times more likely to have a high rather than a low practice level towards DF prevention when compared with nurse professionals. One of the possible reasons might be the differences in professional education qualifications and responsibilities. The odds of having a moderate rather than a low level of practice towards DF prevention among public health officers were 4.706 times higher than the odds for nurse HCPs. The difference is because physicians and public health officers are usually involved in patient diagnosis and management. The odds of HCPs who took DF prevention training and had a high rather than a low practice level towards DF prevention were 10.23 times higher than the odds for HCPs who did not take the training. The main reason for this difference was the lack of training. So providing effective training tailored to all first line HCPs towards DF prevention could be advantageous and a step forward for updating the knowledge of HCPs towards DF prevention. But good knowledge does not necessarily lead to good practice.39
Overall in our study, there existed inadequacy in the sample especially from physicians and public health officers which were not proportional and the small sample size may limit the precision of certain bivariate relationships between variables. Therefore, comparison across certain factors might not have enough sample or power. However, most low-income courtries suffer from a severe shortage of health professionals and Ethiopia is no exception. Ethiopia has a health workforce of 0.7 per 1,000 population, which is low compared with the WHO recommendation of 2.3 health workers per 1,000 population. Health extension workers and general nurses dominate the available supply of health workers and there are critical shortages of physicians, dentists, midwifes, and anesthesia professionals. The greatest inadequacy is for physicians with a decreasing trend in the past and now only 1:42,706 population which is among the lowest ratio in sub-Saharan Africa. However, the country has achieved the minimum WHO recommendation of 1 nurse per 5,000 population.35
Generally, there is a deficit in published studies evaluating the KAP of primary HCPs and associated factors towards DF prevention. Hence, limiting the comparison of our findings. KAP surveys are of the utmost important in determining effective evidence-based prevention and control strategies through changing poor KAPs. To the best of our knowledge, this is the first study on the KAPs of Ethiopian HCPs in Dire Dawa administrative district towards dengue. It is noteworthy that in spite of such limitations, the present findings unveil the existing gaps in the KAPs of Dire Dawa administrative city HCPs and highlights the need for further large-scale studies that consider the possible limitations for the sake of a better generalization of results.
Limitations
Since the study is a public health facility-based (not including private health facilities), it might not indicate the overall KAP of HCPs towards DF prevention. It is also difficult to establish a temporal relationship as the study design was cross-sectional and the wider confidence interval observed with some variables may also indicate inadequate sample size. The study is also limited by the survey method in collecting data only using the quantitative method. Despite these limitations, the findings of this study are expected to contribute a lot to the understanding of the existing problems associated with DF prevention in the study area.
Conclusion and future recommendations
The results of this study showed that the larger proportion of HCPs demonstrated a moderate level of knowledge, neutral level of attitude and low level of practice towards DF prevention. However, there is a lack of knowledge about dengue infection, diagnosis and management. Further, HCPs showed a lack of knowledge about the Aedes mosquito, important clinical features, management of co-morbid cases and prevention methods of dengue disease. Finally, there is a need for similar studies to be done in Ethiopia and elsewhere in the world to better understand the gaps.
Based on the finding of this study, we recommended that:
The regional health bureau should provide training about dengue fever prevention, transmission, and high-risk patient populations. It is also recommended that workshops regarding dengue fever prevention be prepared for the first line health care providers including guidelines preparation. And should continue to strengthenthe surveillance system including assessment of the need of health facilities with provision of the necessary resources to manage dengue patients.
Abbreviations
DF, dengue fever; DENV, dengue virus; DHF, dengue hemorrhagic fever; DSS, dengue shock syndrome; DRHB, Dire Dawa regional health bureau, HCP, health care professionals; HDP; health development program; KAP, knowledge, attitude and practice; WHO, world health organization.
Data sharing statement
Data will not be shared in order to protect the participants‘ anonymity.
Acknowledgments
We are very grateful to Jimma University, College of Public Health and Medical Sciences, for their technical support and giving clearance to conduct this study. We would like to express our gratitude to Mr Desta and Mr Mamo for their guidance from the beginning to the end of this study.
Author contributions
Both authors contributed toward data analysis, drafting and revising the paper, gave final approval of the version to be published and agree to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Halstead S. Dengue. Lancet. 2007;370(9599):1644–1652. doi:10.1016/S0140-6736(07)61687-0
2. Heinz FX, Collett MS, Purcell RH, et al., editors. Virus Taxonomy: Seventh Report of the International Committee on Taxonomy of Viruses, Part Three Ed. San Diego: Academic Press; 2000:859–878.
3.
4. Awoke A, Kassa L. Vector and Rodent Control. Ethiopia Public Health Training Initiative, The Carter Center, the Ethiopia Ministry of Health, and the Ethiopia Ministry of Education; 2006. Available from:
5. Qadir MI, Abbas K, Tahir M, et al. Dengue fever: natural management. Pak J Pharm Sci. 2015;28(2):647–655.
6. Jamaiah I, Rohela M, Nissapatorn V, et al. Retrospective study of dengue fever (DF) and dengue hemorrhagic fever (DHF) patients at university Malaya Medical Center, Kualalumpur, Malaysia. Southeast Asian J Trop Med Public Health. 2005;38(1):224–230.
7. Gubler DJ. The changing epidemiology of yellow fever and dengue, 1900 to 2003: full circle? Comp Immunol Microbiol Infect Dis. 2004;27(5):319–330.
8. Gubler DJ. Dengue and dengue hemorrhagic fever. Clin Microbiol Rev. 1998;11(3):480–496.
9. Malhotra G, Yadav A, Dudeja P. Knowledge, awareness and practices regarding dengue among rural and slum communities in north Indian city, India. Int J Med Sci Public Health. 2014;3(3):295–299. doi:10.5455/ijmsph.2013.181220132
10. Mairuhu AT, Wagenaar J, Brandjes DP, van Gorp ECM. Dengue: an arthropod-borne disease of global importance. Eur J Clin Microbiol Infect Dis. 2004;23:425–433. doi:10.1007/s10096-004-1145-1
11. Gibbons RV, Vaughn DW. Dengue: an escalating problem. Br Med J. 2002;324(7353):1563–1566.
12.
13. Bhatt S, Gething PW, Brady OJ, et al. The global distribution and burden of dengue. Nature. 2013;496:504–507. Federal Ministry of Health of Ethiopia National Framework of Climate Resilient Health Sector. December 2014. Addis Ababa, Ethiopia. doi:10.1038/nature12060
14. Protecting health from climate change, WHO. 2008. Available from:
15.
16.
17. Franco L, di Caro A, Carletti F, et al. Recent expansion of dengue virus serotype 3 in West Africa. Euro Surveill. 2010;15(7):2.
18. Thaver AM, Sobani ZA, Qazi F, Khan M, Zafar A, Beg MA. Assessing the need for training: general practitioners’ knowledge, attitude and practice concerning dengue and malaria in Karachi, Pakistan. Int Health. 2011;3:126–130. doi:10.1016/j.inhe.2011.03.001
19. Prasad D, Kumar C, Jain A, Kumar R. Accuracy and applicability of the revised WHO classification (2009) of dengue in children seen at a tertiary healthcare facility in Northern India. Infection. 2013;41(4):775–782. doi:10.1007/s15010-013-0405-3
20. Kularatne SA. Survey on the management of dengue infection in Sri Lanka: opinions of physicians and pediatricians. Southeast Asian J Trop Med Public Health. 2005;36(5):1198–1200.
21. Lee LK, Thein TL, Kurukularatne C, Gan VC, Lye DC, Leo YS. Dengue knowledge, attitudes, and practices among primary care physicians in Singapore. Ann Acad Med Singapore. 2011;40(12):533–538.
22. Huang H-L, Chiu T-Y, Huang K-C, Cheng S-Y, Yao C-A, Lee L-T. Travel-related mosquito-transmitted disease questionnaire survey among health professionals in Taiwan. J Travel Med. 2011;18(1):34–38. doi:10.1111/j.1708-8305.2010.00483.x
23. Ho T-S, Huang M-C, Wang S-M, Hsu H-C, Liu C-C. Knowledge, attitude, and practice of dengue disease among healthcare professionals in southern Taiwan. J Formos Med Assoc. 2013;112(1):18–23. doi:10.1016/j.jfma.2012.11.004
24. Handel S, Ayala B, Borbor-Cordova J, et al. Knowledge, attitude and practice regarding dengue infection among public sector healthcare providers in Machala, Ecuador. Trop Dis Travel Med Vaccines. 2016;2(8):2–8. doi:10.1186/s40794-016-0024-y
25. Alzahrani A. Knowledge and practice of primary health-care physicians regarding the dengue fever in Makkah Al-Mokarramah city, 2013. Int J Med Sci Public Health. 2015;4:266–274. doi:10.5455/ijmsph.
26. Ekra KD, Cherif D, Kouassi DP, et al. Determinants of practices for dengue diagnosis among healthcare professionals working in public hospitals of Abidjan, Cote d'Ivoire. J Public Health Epidemiol. 2017;9(8):212–218. doi:10.5897/JPHE2017.0933
27. Leo YS, Thein TL, Fisher DA, et al. Confirmed adult dengue deaths in Singapore: 5-year multi-center retrospective study. BMC Infect Dis. 2011;11:123. doi:10.1186/1471-2334-11-208
28. Trung DT, le Thao TT, Hien TT, et al. Liver involvement associated with dengue infection in adults in Vietnam. Am J Trop Med Hyg. 2010;83:774–780. doi:10.4269/ajtmh.2010.10-0090
29. Rafique I, Saqib ANF, Munir MA, et al. Dengue knowledge and its management practices among physicians of major cities of Pakistan. JPMA. 2015;65:392.
30. Saqib MA, Rafique I, Bashir S, Salam AA. A retrospective analysis of dengue fever case management and frequency of co-morbidities associated with deaths. BMC Res Notes. 2014;7:205. doi:10.1186/1756-0500-7-205
31. Federal Democratic Republic of Ethiopia Ministry of Health Health Sector Development Programme IV2010/11 – 2014/15. Draft Version. January 16, 2011.
32. Amarasinghe A, Kuritsky JN, Letson GW, Margolis HS. Dengue virus infection in Africa. Emerg Infect Dis. 2011;17(8):1349–1354. doi:10.3201/eid1701.100876
33. Chow VTK, Chan YC, Yong R, et al. Monitoring of dengue viruses in field-caught Aedes aegypti and Aedesalbopictus mosquitoes by a type-specific polymerase chain reaction and cycle sequencing. Am J Trop Med Hyg. 1998;58(5):578–586. doi:10.4269/ajtmh.1998.58.578
34. Shuaib F, Todd D, Campbell-Stennett D, Ehiri J, Jolly PE. Knowledge, attitudes and practices regarding dengue infection in Westmoreland, Jamaica. West Indian Med J. 2010;59:139–146.
35.
36.
37. Nguyen NM, Whitehorn JS, Luong Thi Hue T, et al. Physicians, primary caregivers and topical repellent: all under-utilised resources in stopping dengue virus transmission in affected households. PLoS Negl Trop Dis. 2016;10(5):e0004667. doi:10.1371/journal.pntd.0004667
38. Shahina W, Nassara A, Kalkattawia M, Bokharia H. Dengue fever in a tertiary hospital in Makkah, Saudi Arabia. Dengue Bull. 2009;33:34–44.
39. Hairi F, Ong CH, Suhaimi A, et al. Knowledge, attitude and practices (KAP) study on dengue among selected rural communities in the Kuala Kangsar district. Asia Pac J Public Health. 2003;15:37–43. doi:10.1177/101053950301500107
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.