")
Back to Journals » Patient Preference and Adherence » Volume 15
Knowledge, Attitude and Practice Towards COVID-19 in Ethiopia: A Systematic Review; 2020
Authors Yazew BG , Abate HK , Mekonnen CK
Received 31 October 2020
Accepted for publication 26 January 2021
Published 15 February 2021 Volume 2021:15 Pages 337—348
DOI https://doi.org/10.2147/PPA.S288186
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Johnny Chen
Birhaneselassie Gebeyehu Yazew, Hailemichael Kindie Abate, Chilot Kassa Mekonnen
Department of Medical Nursing, School of Nursing, College of Medicine and Health Science, University of Gondar, Gondar, Ethiopia
Correspondence: Birhaneselassie Gebeyehu Yazew Email [email protected]
Background: Novel coronavirus disease is a very fast spreading respiratory disease. This disease is becoming a public health emergency across the world. Despite many efforts by countries, organizations, and institutions to prevent and control, the pandemic remains a world health danger. Ethiopia is one of the countries which is severely affected by the pandemic. However, a systematic review of the knowledge, attitude, and practice about coronavirus disease in Ethiopia has not previously done. Thus, the main aim of this systematic review is to investigate the status of people’s knowledge, attitude, and practice about coronavirus disease preventive measures in Ethiopia in 2020.
Methods: Data were extracted based on the Preferred Reporting Items for Systematic Reviews and Meta-Analyses guidelines. Studies were accessed through electronic web-based search from PubMed, Cochrane Library, Google, Google Scholar, and Embase. All statistical analyses were done using Stata version 11 software with a random-effects model.
Results: A total of 11 studies with 3818 participants were included in this systematic review and the overall estimated status of the knowledge, attitude, and practice about coronavirus in Ethiopia are 61.78%, 72.39%, and 52.83%, respectively. According to region subgroup analysis, the highest estimated statuses of the knowledge, attitude, and practice are 74% in Tigray, 86.13% in Southern nations, nationalities, and Peoples’ of the region, and 72% in Tigray region, respectively. Subgroup analysis was done based on the focused group and way of questionnaire administration.
Conclusion: This systematic review revealed people’s knowledge, attitude, and practice about coronavirus disease preventive measures were generally more than 50%. However, government and every individual should address those behaviors stipulated by the World Health Organization and Center for Communicable Disease and Control guidelines to prevent coronavirus disease.
Keywords: knowledge, attitude, practice, coronavirus disease, Ethiopia
Background
Novel coronavirus disease 2019 (COVID-19) is a worldwide spreading respiratory disease caused by a positive sense of Ribonucleic Acid (RNA) virus, severe acute respiratory syndrome coronavirus (SARS 2-COV-2) virus.1 This disease was first classified as a zoonotic disease which is transmitted from animal to human, and from human to human through direct contact and airway droplets.2 Those patients who are confirmed with COVID-19 have a clinical symptom of fever, cough, shortness of breath, and sore throat within 14 days of the incubation period.3,4
According to a World Health Organization (WHO) report, COVID-19 has been a public health problem of international concern since January 30, 2020.5 Globally, there is an estimated number of nearly 46 million confirmed cases and 1.2 million deaths according to the WHO report on November 1, 2020.6 In Ethiopia, COVID-19 was announced on March 15, 2020, after an introduced case was reported. As the WHO report of African countries on November 1, 2020 indicated, there were 96,160 cases notified and over 1,469 deaths in Ethiopia.7
Following the pandemic nature of the disease, countries take different preventive measures such as: people's movement restriction, confinement at home, work at home, self-monitoring, public awareness, closure of schools, and different social services.8–11 Therefore, according to the WHO declaration, Ethiopia is also implementing those preventive measures to halt the pandemic nature of this disease.10,11 However, cases continue to exist.
Evidence shows that COVID-19 has no effective treatment but, early recognition of the symptoms of the disease like high-risk conditions, risky practices, prognosis, and timely looking for supportive care will suppress the virus propagation.12,13
Appropriate knowledge, attitude, and practice about COVID-19 preventive measures play an essential role to determine the public readiness to assent to behavioral change measures from health experts and have been recommended to control the spread of this disease.14
Even though there is a strong recognition of public health importance about COVID-19 by the Ethiopian government, there is still a need to emphasize community awareness creation and practice to stop the nationwide spread of the virus. So far, in Ethiopia, different studies have been done on the level of knowledge, attitude, and practice about COVID-19 preventive measures among the public. These levels of knowledge, attitude, and practice of the population ranged from 20% to 90.3%.10,11,15–23 Therefore, the findings of these different studies show that there is a high variability in the prevalence of the knowledge, attitude, and practice across the regions of the country.
Hence, the aim of this systematic review was to indicate the status of the knowledge, attitude, and practice about COVID-19 prevention measures among the different regions of the country.
Measurements of the Results
Research Question
- What is the estimated prevalence status of the knowledge, attitude, and practice towards COVID-19 preventive measures?
The primary aim of this systematic review is to determine the status of knowledge, attitude, and practice towards COVID-19 preventive measures presented as a percentage of the overall participants in Ethiopia.
The study was conducted using tools that were taken from WHO resources and other similar papers.24,25
Knowledge was measured by items containing prevention, transmission, sign and symptoms, severity, and treatment of the COVID-19. Below the mean was considered as poor knowledge whereas greater than or equal to the mean was considered as good knowledge about COVID-19.
Similarly, attitude was measured by three questions about self-efficacy, collective efficacy, and stigma. So, below the mean was considered as unfavorable attitude whereas greater than or equal to the mean was considered as a favorable attitude about COVID-19.
In the same way, the practice instruments had issues on how often the respondent washes his/her hands with soap, avoid non-essential travel, keep 2-meter social distancing, avoid social gatherings, and avoid touching eyes, nose, and mouth with unwashed (unsanitized) hands. Below the mean was considered as poor practice level whereas greater than or equal to the mean was considered as good practice level about COVID-19.
Methods
Data Bases and Searching Strategy
The preferred reporting items for systematic reviews and meta-analysis (PRISMA) guidelines were used to report the result of this systematic review (Table s1). We searched the data through PubMed, Cochrane Library, Google, Google Scholar, and the Embase database for all available studies from June 1 to August 30, 2020, using Medical Subject Headings (MeSH) and free-text terms. The detailed search strategy is presented in Table s2. In this systematic review the searching was developed using “AND” and “OR”. The gray literature was also searched from the Ethiopian university's research repository online library. In addition, a manual search of the reference lists included was performed so as to address all the evidence. We defined the participants, exposure, comparator, outcome(s), and type of study as “PECO (T)”. The PECO (T) statement provides the framework for the identification and selection of studies for inclusion.26 As we were looking for prevalence studies, we only considered participants and the outcomes.
Inclusion and Exclusion Criteria
The studies were included in this systematic review if and only if they met the following criteria: (1) participants who are all adults aged ≥18, (2) studies that clearly reported the proportion of knowledge, attitude, and practice on CVID-19 preventive measures, (3) studies which were conducted in Ethiopia, (4) cross-sectional observational studies, and (5) both published and unpublished including pre-print studies at any time. The field was limited to “title/abstract”, and those studies with no clear report of the outcome, program evaluation studies, studies done outside of Ethiopia, letter to editors, case reports, study protocols, reviews, interventional studies, and citations without full text were excluded from the review. The PRISMA flow chart for the selection of studies is shown in Figure 1, Figure 2, Figure 3, Figure 4.
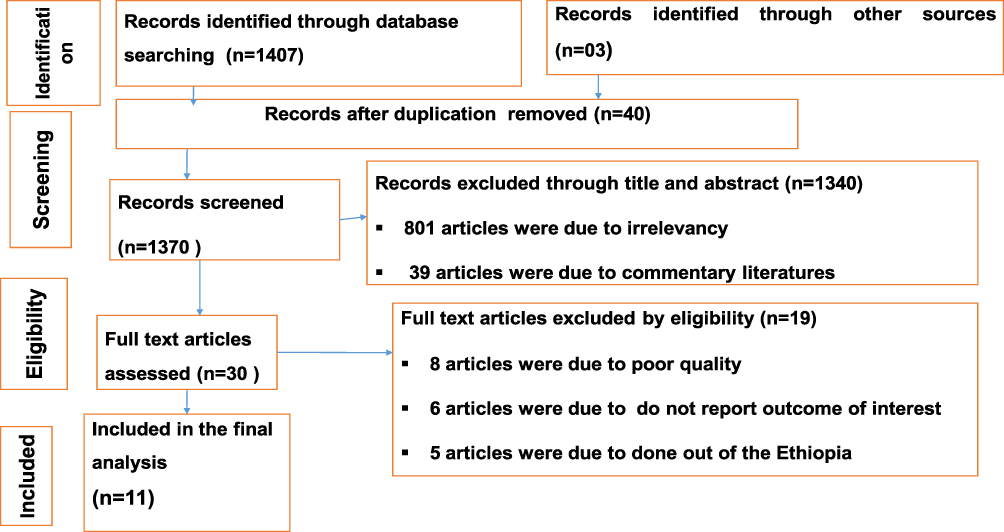 |
Figure 1 Flow chart of study selection for systematic review of the prevalence of KAP towards COVID-19 preventive measures in Ethiopia, 2020. |
Study Selection and Quality Assessment
All the retrieved studies were exported to Endnote version 7 (Thomason Reuters, London). Reference manager and duplicated studies were carefully removed. Two investigators (BGY and HKA) independently screened the titles and abstracts which were followed by a full-text review to determine the eligibility of each study. Any disagreement was solved by consensus with the presence of a third investigator, CKM.
The quality of each study was evaluated by using Joanna Briggs Institute (JBI). Quality appraisal criteria adapted for studies reporting prevalence data and cross-sectional studies.27 Papers with scores of five and above out of a total of nine were involved in the final systematic review.
Data Extraction
Data were independently extracted by two authors (BGY and HKA) using a standardized data extraction format that was developed according to the 2014 Joanna Briggs Institute Reviewers’ Manual.28 The tool includes authors, study year, region, and study design, sample size, and the proportion of knowledge, attitude, and practice about COVID-19 prevention measures in Ethiopia. Articles that fulfilled the predefined criteria were used as a source of data for the final analysis. The two independent reviewers (BGY and HKA) extracted the data by using an Excel spreadsheet, and they cross-checked it to ensure consistency. Any discrepancy was solved through discussion with the presence of a third author (CKM) and the procedure was repeated to overcome the difference which resulted during extracting every single study. The information regarding author, year of publication, study design, sample size, proportion/prevalence of KAP was extracted.
Heterogeneity and Publication Bias
The percentage of total variation across studies due to heterogeneity was assessed by using I2 statistics.29 Therefore, the value of I2, 25%, 50%, and 75% represented low, moderate, and high heterogeneity, respectively. In the same way, a p-value less than 0.05 was used to declare heterogeneity. For the test result which indicates the presence of heterogeneity, a random effect model was used as a method of analysis since it reduces the heterogeneity of studies.30 Funnel plot and Egger’s regression test were done to check whether publication bias exists or not across studies.31 Visual examination of funnel plot asymmetry, Begg-Mazumdar Rank correlation tests, and Egger’s regression tests were also used to check for publication bias.31
Data Analysis
The overall status of knowledge, attitude, and practice was estimated using a random-effect model. Regional subgroup analysis was done to adjust the variation in the estimate status of the KAP towards COVID-19. STATA version 11 (Stata Corp, College Station, TX, USA) statistical software was used for all statistical analysis. In addition, the Begg and Egger’s weighted regression method was used to detect evidence of publication bias. Hence, a p-value of ≤0.05 was considered as indicating the presence of significant publication bias.
Results
Flow Chart
A total of 1410 studies were included in this literature review (Figure 1). We also added three gray pieces of literature that were not found in the search. Of these studies, 40 articles were duplicated records which were removed. Besides this, we excluded 1340 irrelevant articles when we reviewed the titles and abstracts. Furthermore, we removed 19 articles that do not fulfill the criteria when we assess the full text. Then, a total of 11 unique studies were eligible and enrolled for final review analysis.
Characteristics of Included Studies
A total of 11 studies with 3818 participants were included in this systematic review. Those are summarized in Table 1. The studies were conducted from March 2 to June 20, 2020 in different regions of the country. Of those 11 studies, four of them11,16,17,20 were from multicenters, two studies10,15 were from the Amhara region, three of them19,21,23 were from SNNPR, one study18 was from the Oromia region, and one study22 was from the Tigray region. All the studies enrolled in this systematic review were cross-sectional studies (Table 1).
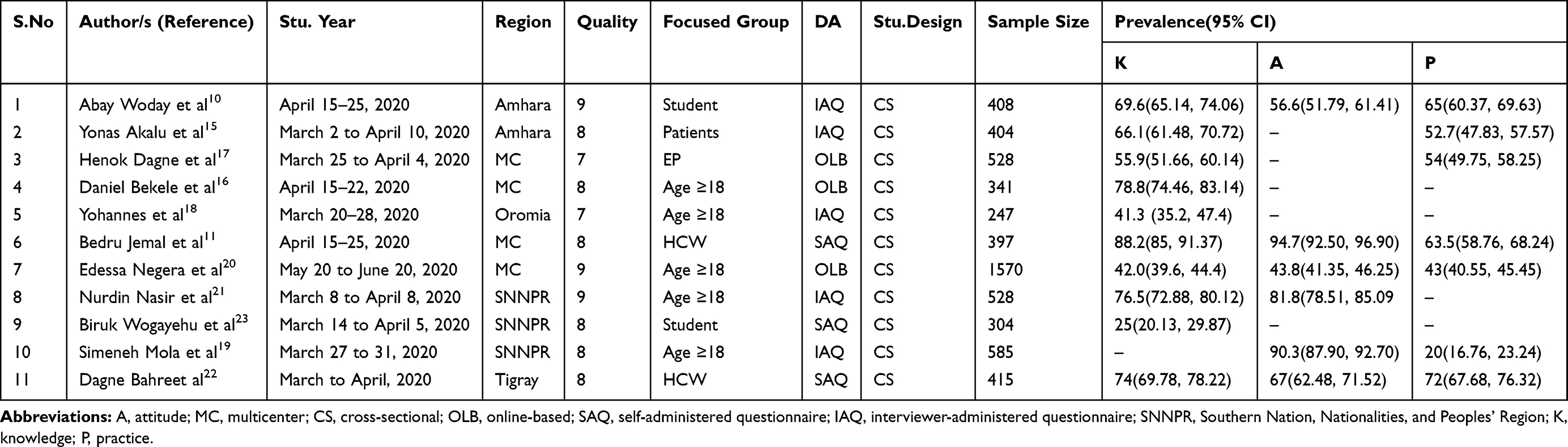 |
Table 1 Characteristics of Studies Included in a Systematic Review of the Prevalence of Knowledge, Attitude, and Practice Towards COVID-19 in Ethiopia, 2020 |
Knowledge, Attitude and Practice Towards COVID-19 (a Systematic Review)
The estimated status using the fixed-effect model demonstrated significant heterogeneity among the studies. By random-effects model, the estimated status of knowledge, attitude, and practice about COVID-19 preventive measures reported were 61.78% (95% CI (48.97%, 74.58%)), 72.39% (95% CI (54.02%, 90.77%)), and 52.83% (95% CI (39.26, 66.41%)), respectively. These figures show a significant heterogeneity among studies (I2= 99.1%, p ≤0.001), (I2= 98.6%, p ≤ 0.001), and (I2= 90.9%, p ≤0.001), respectively (Figures 2–4).
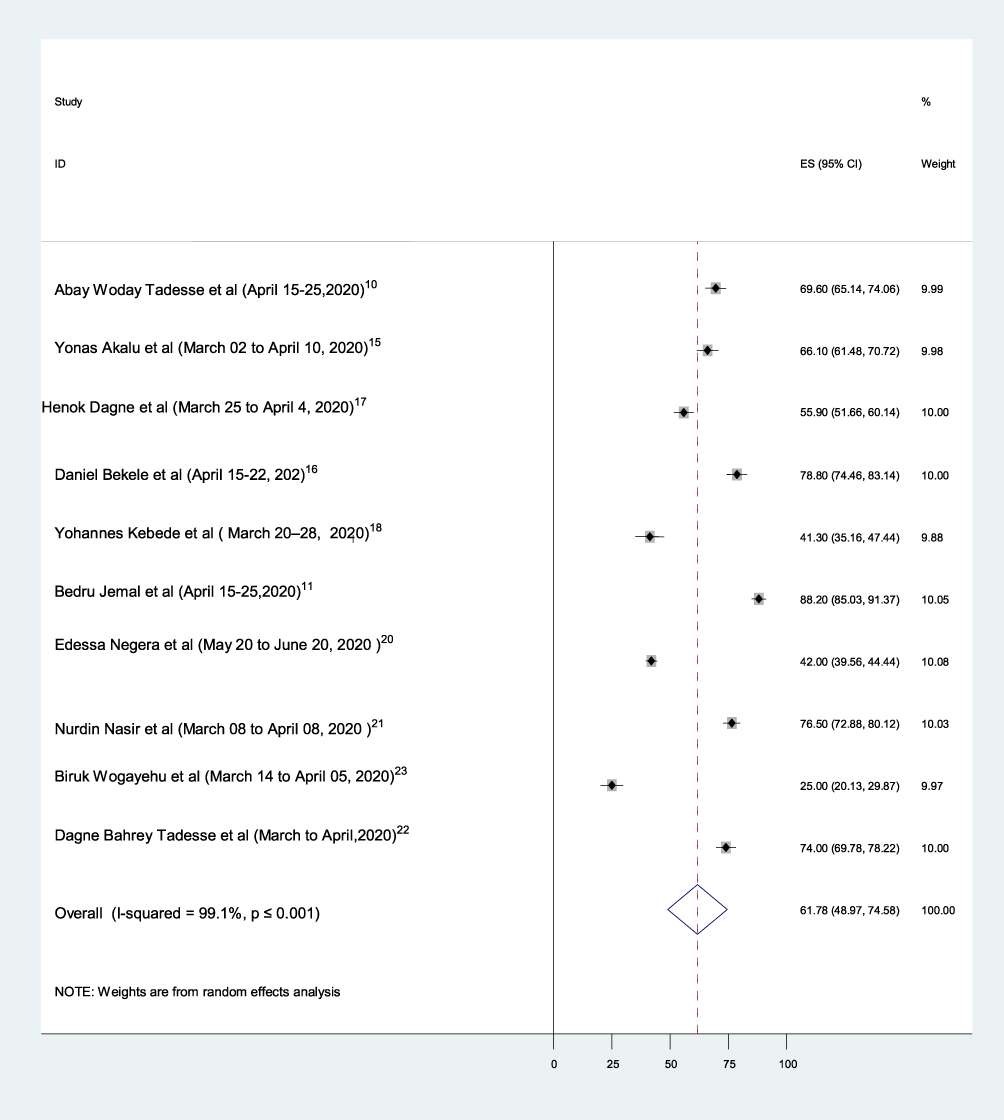 |
Figure 2 Forest plot showing the pooled prevalence of knowledge towards COVID-19 preventive measures in Ethiopia, 2020. |
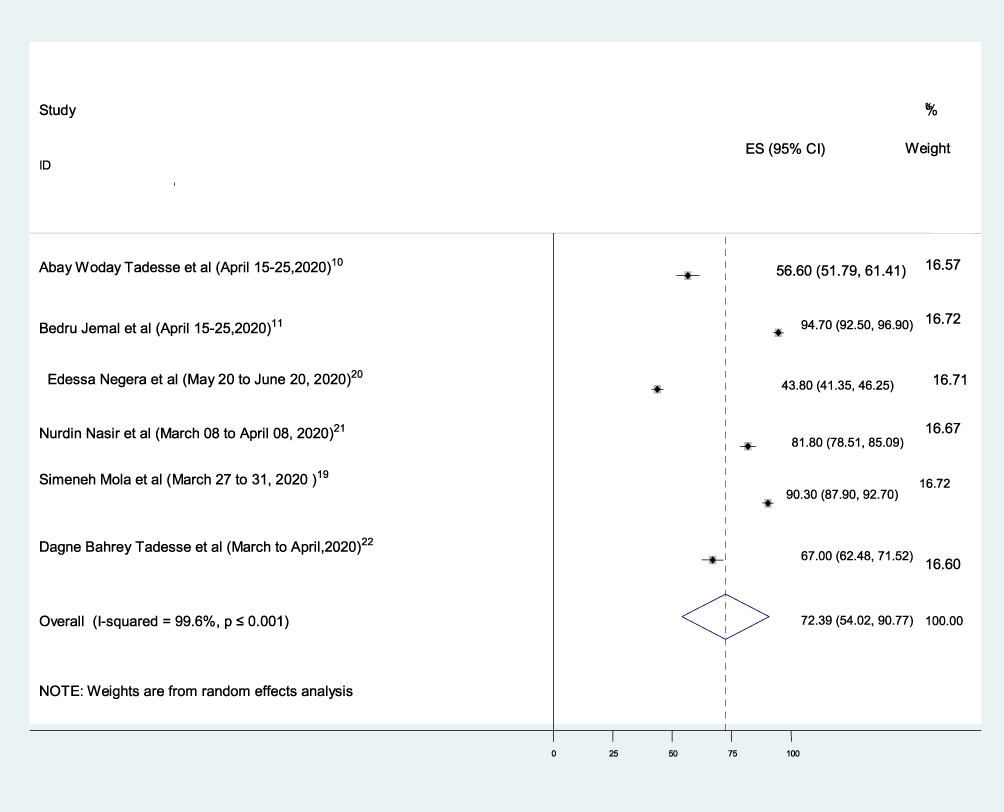 |
Figure 3 Forest plot showing the pooled prevalence of attitude towards COVID-19 preventive measures in Ethiopia, 2020. |
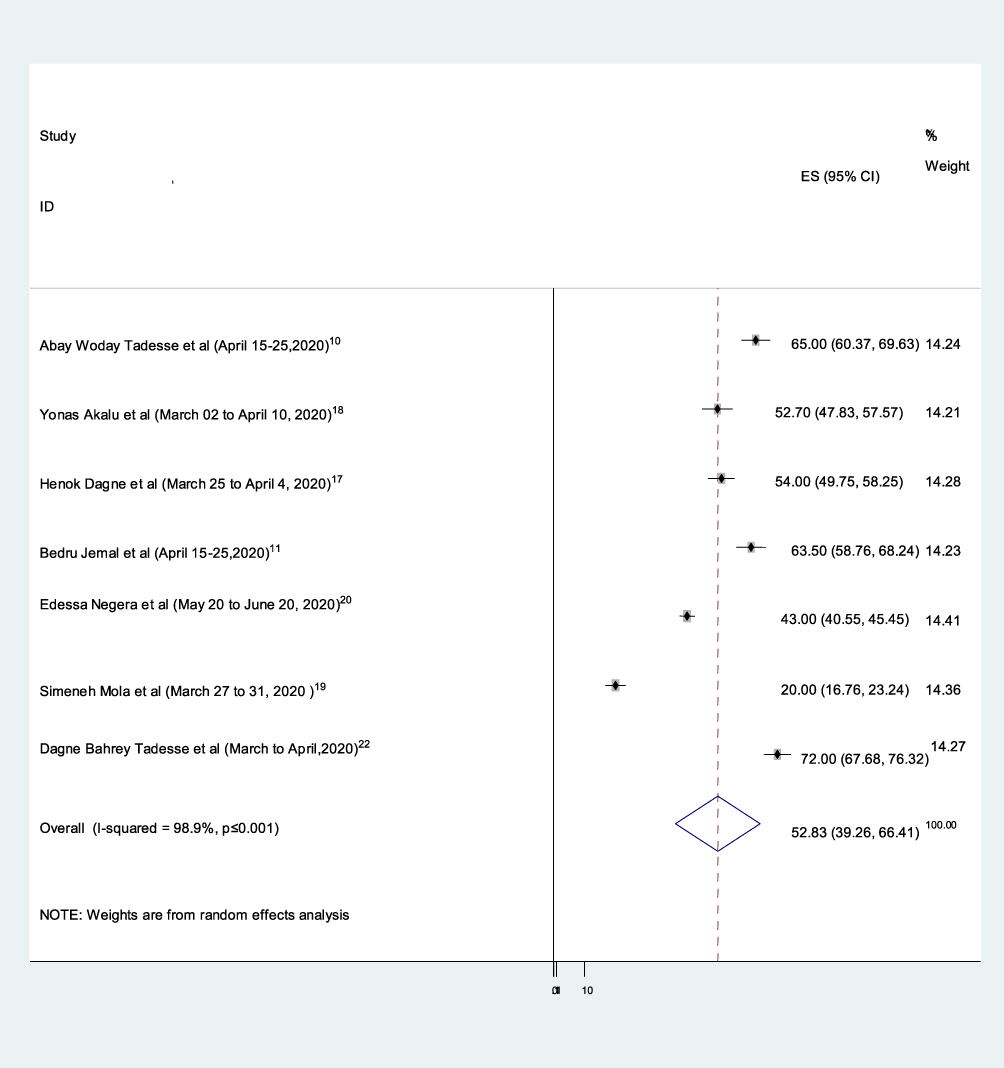 |
Figure 4 Forest plot showing the pooled prevalence of practice towards COVID-19 preventive measures in Ethiopia, 2020. |
Subgroup analysis for knowledge: focused group, methods of questionnaire administered, and study area was used to check the possible heterogeneity among studies. Of the 10 studies, the highest estimated status of knowledge towards COVID-19 was among the age group greater than 18, 81.17% (67.26, 95.09), I2= 94.4%, p ≤ 0.001, whereas the least was among students in college 41.31% (3.60, 91.02), I2=99.4%, p ≤ 0.001 (Figure 5). Furthermore, we have done a subgroup analysis by way of a questionnaire administered, since there is heterogeneity. Hence, the highest estimated status of the knowledge subgroup analysis which was done using interviewer administered questionnaire (IAQ), 63.55% (50.69, 76.42), I2= 96.4%, p ≤ 0.001 while the lowast subgroup analysis was online-based, 58.83% (37.26, 80.43), I2= 99.1%, p ≤ 0.001 (Figure s1). Again, the heterogeneity still existed. So, for the last, we performed subgroup analysis based on the study area but there is no evidence of heterogeneity. The greatest and least prevalences were 74% (95% CI: 69.78, 78.22), I2= 0%, and 41.3% (95% CI: 35.16%, 47.44%), I2= 0% from Tigray and Oromia regions, respectively.
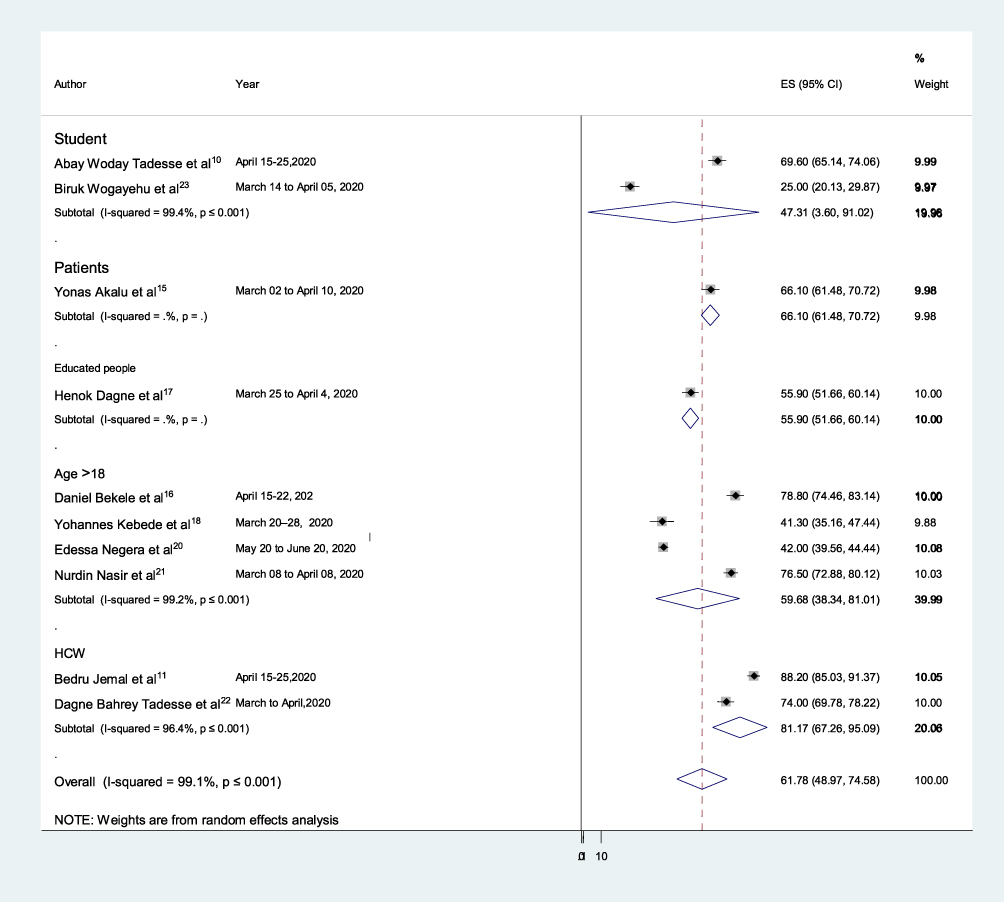 |
Figure 5 Subgroup analysis by focused group on the prevalence of knowledge towards COVID-19 preventive measures in Ethiopia, 2020. |
Subgroup analysis for attitude towards COVID-19 using methods of a questionnaire administered, focused group, and study areas was done. Of the 6 studies, the highest estimated status of attitude towards COVID-19 was with a self-administered questionnaire (SAQ) 80.92% (53.78, 108.07), I2= 99.1%, p ≤ 0.001 whereas, the lowest one was with online-based questionnaire administration 43.80% (41.35, 46.25), I2= 0% (Figure s3). Furthermore, we carried out a subgroup analysis based on a focused group since heterogeneity existed. Hence, the highest estimated status of the attitude was among health care workers (HCW) 80.92% (53.78, 108.07), I2= 99.1%, p ≤ 0.001 but, the lowest one was among students 56.60% (51.78, 61.41) (Figure s4). The final subgroup analysis we carried out was based on the study area. Highest estimate was 86.13% (77.80, 94.09), I2= 94%, p ≤ 0.001 from SNNPR and the lowest was 56.60% (51.79, 61.41) from the Amhara Region, with evidence of heterogeneity (Figure s5).
Subgroup analysis for practices towards COVID-19 based on methods of a questionnaire administered focused group, and study areas has been done. Of the 7 studies, the highest estimated status of practice towards COVID-19 with SAQ was 67.81% (59.48, 76.14), I2= 85.2%, p ≤ 0.001. While the lowest was with IAQ 45.86% (16.97, 74.75), I2= 99.3%, p ≤ 0.001 (Figure s6). Furthermore, we performed a subgroup analysis by focused group since heterogeneity existed. Hence, the highest estimated prevalence of the practice was among HCW 72% (67.68, 76.32), I2= 85.2%, p ≤ 0.001, but the lowest was among the age group of those older than 18 31.53% (8.99, 54.07), I2= 99.2%, p ≤ 0.001 (Figure s7). Finally, we have carried out a subgroup analysis based on the study area. The most prevalent was 72% (67.80, 76.32%), I2= 98.9%, p ≤ 0.001 from the Tigray region whereas the lowest was from SNNPR, 20% (16.76, 23.24%), with evidence of heterogeneity (Figure s8).
Publication Bias
The presence of publication bias was assessed using funnel plots and tests. In this systematic review, funnel plots and tests give evidence on publication bias for knowledge, attitude, and practice towards COVI-19 stated as follows. For knowledge, each article's effective size was allocated against the standard error, and visual inspection of the funnel plot suggests asymmetry. Since six studies lay on the right side and four studies on the left side of the line representing the estimated status (Figure s9) and this was corrected by filling (Figure s10). The result of the publication bias by Eggers was not showing significant evidence of bias (p-value = 0.907). On the other hand, for attitude, each article's effective size was not allocated against the standard error, and visual inspection of the funnel plot suggests symmetry, as the two studies lay on the right side, the other two studies lay at the middle, and the final two studies lay on the left side of the line representing the estimated status (Figure s11). The output of the publication bias by Eggers test was not showing significant evidence of bias (p-value = 0.658). Lastly, each article for practice towards COVID-19 effective size was allocated against the standard error and visual inspection of the funnel plot suggests asymmetry as five studies lay on the right side, one study lay at the middle, and one study lay on the left side of the line representing the pooled prevalence (Figure s12) and this was corrected by filling (Figure s13). The finding of the publication bias by Eggers tests was not showing evidence of bias (p-value = 0.234).
Investigation of Heterogeneity
Heterogeneity in a systematic review is inevitable. This heterogeneity is because of the differences in; study quality, method, sample size, and inclusion criteria. In this review, the value of I2 is a definite sign of significant-high heterogeneity. So, we analyzed it using a random-effects model to adjust for the observed variability. Furthermore, the presence of heterogeneity was also assessed by subgroup analysis for knowledge, attitude, and practice. Heterogeneity for knowledge was due to study area differences. Besides this, the level of heterogeneity was high after subgroup analysis for attitude and practice about COVID-19. Thus, we further tried to investigate the sources of the heterogeneity. That was done using a meta-regression model (using sample size as covariates). Meta-regression is a more complex and preferable method than subgroup analysis. So, to check heterogeneity it has some advantages by assessing one or more covariates. The result of this analysis showed that the covariate was not significant. That was for the presence of heterogeneity (Tables 2 and 3).
 |
Table 2 Meta-Regression Analysis of Factors with the Heterogeneity of the Prevalence of Attitude Towards COVID-19 in Ethiopia, 2020 |
 |
Table 3 A Meta-Regression Analysis of Factors with the Heterogeneity of the Prevalence of Practice Towards COVID-19 in Ethiopia, 2020 |
Sensitivity Analysis
The result indicated that no single study unduly influenced the overall estimate of knowledge, attitude, and practice towards COVID-19.
Discussion
Ethiopia is one of the thirteen countries which are considered a top priority by WHO with respect to the need for epidemic response preparedness against COVID-19.32 In Ethiopia, the first COVID-19 cases were announced on March 13, 2020.33 Since then, the number of cases has been raised to over 73,332 currently confirmed cases and over 1170 deaths.34 Thus, this systematic review analysis of knowledge, attitude, and practice study contributes to a better understanding of the current situation, challenges, and solutions for policy decision-makers.
This review stated that the existing finding of the 11 studies described the status of knowledge, attitude, and practice towards COVID-19. Various studies have indicated that, in Ethiopia, the prevalence of knowledge, attitude, and practice about COVID-19 ranged from 20% to 90.3%. This difference in the prevalence of knowledge, attitude, and practice among the different regions of the country can be justified because of the presence of availability of resources, measurement tools, sample size, sampling techniques, sources of information, and designs.
The results of 10 articles with 5122 participants showed that the estimated knowledge towards COVID-19 was 61.78% (95% CI (48.97, 74.58)). This finding is similar to the studies conducted in bi-national African countries 61.6%.35 However, this result is lower than studies done in China and Iran 90%.25,36 This may be because the developing countries use social media less than developed countries and minimize disruption caused by the coronavirus.
The findings of 6 articles with 3903 participants showed that the estimated attitude towards COVID-19 was 72.39% (95% CI (54.02, 90.77)). This finding is nearly the same as the studies conducted in China 73.8%.37 However, it is lower than study reports from India (97.3%).38 The discrepancy may be subjected to variation in the cut-values to measure the favorable and unfavorable attitude levels. Besides, the discrepancies may be due to differences in sample size, study design, population, and study settings.
The output of 7 articles with 4307 participants showed that the estimated preventive practice towards COVID-19 was 52.83% (95% CI (39.26, 66.41)). This finding was very different from a systematic review and meta-analysis result of 73%.39 The possible justifications might be study area and sample size (27,617) differences.
People’s knowledge, attitude, and practice towards COVID-19 are significant determinants of whether they are involved in pandemic-specific preventive behaviors. Scholars stated that elevated KAP towards COVID-19 preventive measures is definitely related to higher commitment in appropriate defensive behavior during the pandemic.40
Limitations
First, the bias may be there because the search was only in the English language. Secondly, the scarcity of data in some regions of Ethiopia may make it a problem to generalize the findings. Finally, used tools for measuring knowledge, attitude, and practice are quantitative. So, to focus on behavior change, qualitative work is necessary.
Conclusions
This systematic review revealed that the knowledge, attitude, and practice towards COVID-19 preventive measures were around 50% and not sufficient enough to combat this rapidly spreading virus. Health promotions through public education about COVID-19 preventive measures are highly recommended by the government in collaboration with healthcare organizations. Besides the government healthcare organizations, every individual should address those behaviors stipulated by the WHO and CDC guidelines to prevent COVID-19. Furthermore, nationwide studies are needed to understand the determinant factors for the knowledge, attitude, and practice towards COVID-19 preventive measures using meta-analysis.
Abbreviations
COVID-19, coronavirus disease 2019; CDC, Centers for Disease Control and Prevention; WHO, World Health Organization; SNNPR, Southern Nation, Nationalities and Peoples’ of Region; KAP, knowledge, attitude, and practice; USA, United States of America.
Data Sharing Statement
Data will be available by request to the corresponding author.
Authors’ Information
BGY, HKA, and CKM are lecturers and practitioner nurses at the Department of Medical Nursing, School of Nursing, College of Medicine and Health Science, University of Gondar, Gondar, Ethiopia.
Author Contributions
BGY, HKA, and CKM, are involved in the design, selection of articles, data extraction, statistical analysis, manuscript editing, and writing, have agreed on the journal to which the article will be submitted and to take responsibility and be accountable for the contents of the article. All the authors read and approved the final draft of the manuscript.
Funding
There is no funding to report.
Disclosure
The authors declare that they have no conflicts of interest for this work.
References
1. Masters PS. Coronavirus genomic RNA packaging. Virology. 2019;537:198–207. doi:10.1016/j.virol.2019.08.031
2. Guan W-J, Ni Z-Y, Hu Y, et al. Clinical characteristics of coronavirus disease 2019 in China. N Engl J Med. 2020;382(18):1708–1720. doi:10.1056/NEJMoa2002032
3. Saitz R, Palfai TP, Cheng DM, et al. Screening and brief intervention for drug use in primary care: the ASPIRE randomized clinical trial. JAMA. 2014;312(5):502–513. doi:10.1001/jama.2014.7862
4. Organization WH. Modes of Transmission of Virus Causing COVID-19: Implications for IPC Precaution Recommendations: Scientific Brief, 27 March 2020. World Health Organization; 2020.
5. Team EE. Note from the editors: World Health Organization declares novel coronavirus (2019-nCoV) sixth public health emergency of international concern. Eurosurveillance. 2020;25(5):200131e.
6. Organization WH. Coronavirus disease (COVID-2019) situation reports. 2020.
7. Organization WH. Coronavirus disease ( COVID-19): weekly epidemiological update. 2020.
8. Burke RM. Active monitoring of persons exposed to patients with confirmed COVID-19—United States, January–February 2020. MMWR Morb Mortal Wkly Rep. 2020;69.
9. Zettler I, Schild C, Lilleholt L, Böhm R Individual differences in accepting personal restrictions to fight the COVID-19 pandemic: results from a Danish adult sample. 2020.
10. Tadesse AWM, Eshetie N, Chane S, Mulugeta Ali A Knowledge, attitude, and practice and associated factors towards COVID-19 among college students in Amhara Region, Ethiopia; a cross-sectional study; 2020. Available from: https://www.researchsquare.com/article/rs-38099/v1.
11. Jemal B, Ferede ZA, Mola S, et al. Knowledge, attitude and practice of healthcare workers towards COVID-19 and its prevention in Ethiopia: a multicenter study; 2020. Available from: https://assets.researchsquare.com/files/rs-29437/v1/2802c94a-b237-458f-ac48-aee72c4ae793.pdf.
12. Chen N, Zhou M, Dong X, et al. Epidemiological and clinical characteristics of 99 cases of 2019 novel coronavirus pneumonia in Wuhan, China: a descriptive study. Lancet. 2020;395(10223):507–513. doi:10.1016/S0140-6736(20)30211-7
13. Holshue ML, DeBolt C, Lindquist S, et al. First case of 2019 novel coronavirus in the United States. N Engl J Med. 2020;382(10):929–936. doi:10.1056/NEJMoa2001191
14. Cai H, Tu B, Ma J, et al. Psychological impact and coping strategies of frontline medical staff in hunan between january and march 2020 during the outbreak of Coronavirus disease 2019 (COVID-19) in Hubei, China. Med Sci Monit. 2020;26:e924171. doi:10.12659/MSM.924171
15. Akalu Y, Ayelign B, Molla MD. Knowledge, attitude and practice towards COVID-19 among chronic disease patients at Addis Zemen Hospital, Northwest Ethiopia. Infect Drug Resist. 2020;13:1949. doi:10.2147/IDR.S258736
16. Bekele D, Tolossa T, Tsegaye R, Teshome W. The knowledge and practice towards COVID-19 pandemic prevention among residents of Ethiopia. An online cross-sectional study. BioRxiv. 2020.
17. Dagne H, Alemu KA, Dagnew B, et al. Prevention practice and associated factors of Coronavirus disease 2019 (COVID-19) outbreak among educated Ethiopians: an online based cross-sectional survey; 2020. Available from: https://www.researchsquare.com/article/rs-34504/v1.
18. Kebede Y, Yitayih Y, Birhanu Z, Mekonen S, Ambelu A. Knowledge, perceptions and preventive practices towards COVID-19 early in the outbreak among Jimma university medical center visitors, Southwest Ethiopia. PLoS One. 2020;15(5):e0233744. doi:10.1371/journal.pone.0233744
19. Mola S, Aweke Z, Jemal B, et al. Magnitude and associated factors for attitude and practice of Southern Ethiopian residents toward COVID-19 and its preventions: a community based cross sectional study; 2020. Available from: https://www.researchsquare.com/article/rs-36120/v1.
20. Negera E, Demissie TM, Tafess K. Inadequate level of knowledge, mixed outlook and poor adherence to COVID-19 prevention guideline among Ethiopians. BioRxiv. 2020.
21. Nigussie TF, Azmach NN. Knowledge, attitude and practice towards Covid-19 among Arba Minch Town, Southern Ethiopia. GSJ. 2020;8(6).
22. Tadesse DB, Gebrewahd GT, Demoz GT Knowledge, attitude, practice and psychological response toward COVID-19 among nurses during the COVID-19 outbreak in Northern Ethiopia; 2020. Available from: https://www.researchsquare.com/article/rs-26236/v1.
23. Wogayehu B, Taye W, Faraja K Knowledge regarding 2019 novel coronavirus (2019-nCoV) infection among final year health science students at Arbaminch College of Health Sciences, Southern Ethiopia: a cross-sectional study; 2020. Available from: https://www.researchsquare.com/article/rs-24777/v1.
24. Organization WH. Risk Communication and Community Engagement (RCCE) Action Plan Guidance: COVID-19 Preparedness & Response. World Health Organisation; 2020.
25. Zhong B-L, Luo W, Li H-M, et al. Knowledge, attitudes, and practices towards COVID-19 among Chinese residents during the rapid rise period of the COVID-19 outbreak: a quick online cross-sectional survey. Int J Biol Sci. 2020;16(10):1745. doi:10.7150/ijbs.45221
26. Woodruff TJ, Sutton P. The Navigation guide systematic review methodology: a rigorous and transparent method for translating environmental health science into better health outcomes. Environ Health Perspect. 2014;122(10):1007–1014. doi:10.1289/ehp.1307175
27. Wells G, Shea B, O’Connell D, Peterson J, Welch V, Losos M. The Newcastle-Ottawa Scale (NOS) for Assessing the Quality of Nonrandomized Studies in Meta-Analysis. Ottawa (ON): Ottawa Hospital Research Institute; 2012.
28. Munn Z, Moola S, Riitano D, Lisy K. The development of a critical appraisal tool for use in systematic reviews addressing questions of prevalence. Int J Health Policy Manag. 2014;3(3):123. doi:10.15171/ijhpm.2014.71
29. Huedo-Medina TB, Sánchez-Meca J, Marín-Martínez F, Botella J. Assessing heterogeneity in meta-analysis: q statistic or I2 index? Psychol Methods. 2006;11(2):193. doi:10.1037/1082-989X.11.2.193
30. Higgins JP, Thompson SG, Deeks JJ, Altman DG. Measuring inconsistency in meta-analyses. BMJ. 2003;327(7414):557–560. doi:10.1136/bmj.327.7414.557
31. Rücker G, Schwarzer G, Carpenter J. Arcsine test for publication bias in meta‐analyses with binary outcomes. Stat Med. 2008;27(5):746–763. doi:10.1002/sim.2971
32. WHO. COVID-19 preparedness bulletin Ethiopia; 2020. Available from: https://extranet.who.int/sph/news/covid-19-preparedness-bulletinethiopia.
33. Africa W. First case of COVID-19 confirmed in Ethiopia. Available from: https://www.afro.who.int/news/first-case-covid-19-confirmed-ethiopia.
34. WHO. COVID-19 in the WHO African Region; 2020; Available from: https://who.maps.arcgis.com/apps/opsdashboard/index.html#/0c9b3a8b68d0437a8cf28581e9c063a9.
35. Hager E, Odetokun IA, Bolarinwa O, Zainab A, Okechukwu O, Al-Mustapha AI. Knowledge, attitude, and perceptions towards the 2019 Coronavirus pandemic: a bi-national survey in Africa. PLoS One. 2020;15(7):e0236918. doi:10.1371/journal.pone.0236918
36. Erfani A, Shahriarirad R, Ranjbar K, Mirahmadizadeh A, Moghadami M. Knowledge, attitude and practice toward the novel coronavirus (COVID-19) outbreak: a population-based survey in Iran. Bull World Health Organ. 2020;30.
37. Peng Y, Pei C, Zheng Y, et al. Knowledge, attitude and practice associated with COVID-19 among university students: a cross-sectional survey in China. 2020.
38. Tomar BS, Singh P, Nathiya D, et al. Indian community’s knowledge, attitude & practice towards COVID-19. medRxiv. 2020.
39. Bhagavathula AS, Aldhaleei WA, Rahmani J, Khubchandani J. Knowledge, attitude, perceptions and practice towards COVID-19: a systematic review and meta-analysis. medRxiv. 2020.
40. Gentili D, Bardin A, Ros E, et al. Impact of communication measures implemented during a school tuberculosis outbreak on risk perception among parents and school staff, Italy, 2019. Int J Environ Res Public Health. 2020;17(3):911. doi:10.3390/ijerph17030911
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.