")
Back to Journals » Infection and Drug Resistance » Volume 13
Knowledge, Attitude, and Practice of High-Risk Age Groups to Coronavirus Disease-19 Prevention and Control in Korem District, Tigray, Ethiopia: Cross-Sectional Study
Received 2 August 2020
Accepted for publication 8 October 2020
Published 23 October 2020 Volume 2020:13 Pages 3801—3809
DOI https://doi.org/10.2147/IDR.S275168
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Suresh Antony
Girmay Adhena,1 Hagos Degefa Hidru2
1Department of Reproductive Health, Tigray Regional Health Bureau, Tigray, Ethiopia; 2Department of Public Health, College of Medical and Health Science, Adigrat University, Adigrat, Ethiopia
Correspondence: Girmay Adhena; Hagos Degefa Hidru Email [email protected]; [email protected]
Background: The emerging of the novel coronavirus in Wuhan, China, since the time declared as a public health emergency of international concern, its impact on the lives of people is negatively substantial. Despite the vulnerability of all ages from the pandemic, evidence showed that elder people are at high-risk for adverse outcomes from coronavirus disease-19. Therefore, this study aimed to assess the knowledge, attitude, and practice of high-risk age groups to coronavirus disease-19 prevention and control in Korem district, Tigray, Ethiopia.
Methods: A community-based cross-sectional study was conducted among high-risk age groups from April 2 to May 9/2020 in Korem district, Tigray, Ethiopia. A total of 422 study participants were selected using a simple random sampling technique. The collected data were entered into Epi-data version 3.1 and exported to SPSS version 22.0 for analysis. Multivariable analysis was done using linear regression after checking collinearity, and a p-value of less than 0.05 was considered significant.
Results: A total of 419 study participants were included in the study with a response rate of 99.3%. Overall, about 37.7%, 43.4%, and 52.5% of participants had poor knowledge, negative attitude, and poor practice towards coronavirus disease-19 prevention and control, respectively. Being elder (≥ 80) years, with no formal education, and having low-income status were among the significantly associated factors. About 76.1% of the respondents did not use hand-rub-based alcohol or sanitizer, and 88.8% did not use any mask in crowding area.
Conclusion: Generally, the knowledge about coronavirus disease-19 in elders was roughly appropriate but the preventive practices and attitude towards coronavirus disease-19 were found less and inappropriate. Since no proven medicine is invented yet, so maximizing knowledge, increasing behavioral change, and strengthening preventive practices towards coronavirus disease-19 prevention and control is the appropriate solution.
Keywords: knowledge, attitude, practice, risky group, elders, COVID-19, Korem, Ethiopia
Introduction
Coronavirus disease-19 (COVID-19) is a new strain that has not been identified among humans.1 An initial cluster of cases of pneumonia of unknown origin was reported on December 31, 2019, in people associated with the Huanan Seafood Wholesale market in Wuhan, China.2 Since then, Chinese health authorities have confirmed the association of these clusters with a novel Coronavirus-19.3 Following this, the world health organization (WHO) named this novel virus as Coronavirus disease-19 (COVID-19) and on Jan 30, 2020, it was declared as a Public Health Emergency of International Concern.4 On March 11, 2020, WHO declared Coronavirus Disease-2019 (COVID-19) a pandemic and Africa confirmed its first case in Egypt on Feb 14, 2020.5
The novel COVID-19 has emerged as a global crisis where the world remains at a pivotal juncture in the fight against this pandemic.6 As of December 31, 2019, in Wuhan city, Hubei province, China reported a cluster of 27 pneumonia cases of unknown etiology, including 7 severe cases.7 Following the declaration of COVID-19 as a global public health emergency on 11 March, 2020 by WHO, 118, 319 confirmed cases (4292 deaths), and 80, 955 confirmed cases (3162 deaths) in China and 37,364 confirmed cases (1130 deaths) in about 113 countries other than in China were reported.8 As of 3rd May 2020, the virus spread to more than 210 countries and it affected greater than 3.3 million confirmed cases (234,112 deaths) globally, 1,492,024 confirmed cases (140,586 deaths) in European regions, 60,490 confirmed cases (2256 deaths) in Southeast Asian region, 27,973 confirmed cases (1013 deaths) in the African region and 135 confirmed cases (3 deaths) in Ethiopia.9
Everyone is susceptible to exposed and infected by coronavirus disease-19 (COVID-19), but evidence to date suggests that older people (people over 60 years old) and those with underlying medical conditions such as cardiovascular disease, diabetes, chronic respiratory disease, and cancer are the two groups of at a higher risk of getting severe COVID-19 disease.10 Although the majority of reported COVID-19 cases in China were mild (81%), approximately 80% of deaths occurred were among adults aged ≥60 years old.11 The overall case-fatality rate (CFR) of COVID-19 is around 3.4% and greater than 10.0% for those aged greater than 60 years old. The overall evidence is indicating that significant adverse outcomes have escalated among 60 years and above the aged group.12,13
It is undeniable that in Africa, particularly in Sub-Saharan Africa (SSA) including Ethiopia will result in a huge challenge to control and respond to the pandemic.14 World Health Organization (WHO) has alarmed all countries to increase their level of knowledge, attitude, and practice to identify, prevent, manage, and care COVID-19 cases.15 Even though the sheltering of individuals at the highest risk of poor outcomes is amongst focus areas identified by WHO, it is a public health and socioeconomic crisis is disproportionately affecting the high-risk age groups.15,16 Despite the various implementations methods to combat the novel COVID-19 pandemic at the national level, high-risk age groups (60 years age and above) constitute a great at risk to adverse outcomes related to the COVID-19 pandemic. Hence, this study aimed to assess the knowledge, attitude, and practice of high-risk age groups towards COVID-19 prevention and control at Korem district, Tigray, Ethiopia.
Materials and Methods
Study Period and Area
The study was conducted in Korem district, Tigray, Ethiopia. It shares bordered on the south by Alamata, on the east by Raya Azebo, on the west by the Amhara region, and the north by Endamehoni. It is located 619 km away from Adis Ababa, the capital city of Ethiopia. The district has a total population of 34,576, out of this number, 17,810 (48.6%) are male and 18,935 (51.4%) are females, of the total population, 3043 (8.8%) are people with an age of 60 years and above.17 The study was conducted from April 2 to May 9/2020 in Korem district, Tigray, Ethiopia.
Study Design and Population
A community-based cross-sectional study was conducted among people age greater than or equal to sixty years. All people with age groups ≥60 years old in Korem district were the source population. All people with age groups ≥60 years at the selected households of Korem district were the study population.
Sample Size Calculations and Sampling Technique
The sample size was determined using a single population proportion formula n = ((Z a/2)2 (p q)/d2) with the assumptions of a confidence level of, 95% =1.96, the margin of error = 0.05, P= 0.5 taken for the prevalence of knowledge, attitude and practice of COVID-19 among the high-risk age groups because there is no previous study conducted in Ethiopia. The calculated sample size was 384. After adding 10% for the non-response rate (384+384*0.1), 422 was the final sample size of the study. A total of 422 study participants were proportionally allocated based on the registration of age categories of the households from each kebeles and the health extension workers then a simple random sampling technique was used to identify study participants.
Data Collection Method
The data were collected through a face-to-face interviewer-administered questionnaire. After extensive revision of the English questionnaire, the final English version was translated into the local language by a language expert person. The principal investigator trained the data collectors and supervisor for three consecutive days on instruction for the method, how to make informed written consent, how to approach participants, ethical procedure, and general information were explained to all participants to keeping at least 2-meter physical distance from interviewees and used personal protective materials (mask, glove, and sanitizer) during the data collection period practically.
Data Quality Control
The questionnaire was pretested on 5% of the study population in the non-selected kebeles to ensure clarity, wordings, logical sequence, and skip patterns of the questions. Appropriate modifications were made after discussing with the supervisor and data collectors before starting the actual data collection process and the filled questionnaire was daily checked.
Data Processing and Analysis
The completed data was entered using Epi-Data statistical software version 3.1 and then exported to SPSS version 22 for final analysis. Frequencies and percentages were used to present categorical data. The uni-variable analysis was done using aIndependent two-Sample t-testand analysis of variance (ANOVA). The correlation between knowledge and practices was evaluated by the Pearson correlation coefficient test. Multivariable analysis was done using linear regression after multi-collinearity was checking using the variance inflation factor and tolerance test. Finally, p < 0.05 was considered a significant level.
Operational Definitions
High-Risk Age
People who are in the age of greater than or equal to sixty (60) years old.
Knowledge
This was measured by nine knowledge questions (items). Those who scored points above or equal to the mean value of the knowledge-related questions on COVID-19 were categorized as good knowledge and those who scored below the mean were considered as they have poor knowledge about COVID-19.
Attitude
This was measured by five questions (items). Those who scored points above or equal to the mean of the attitude related questions on COVID-19 have a positive attitude whereas those who scored below the mean value was considered as having a negative attitude.
Practice
This was measured by six practice-related questions (items). High-risk age groups who scored points above or equal to the mean value of the practice-related questions on COVID-19 prevention and control had a good practice and those who scored below the mean value were considered as they have poor preventive practice.
Results
Socio-Demographic Characteristics of Study Participant
A total of 419 participants were included in the study with a response rate of 99.3%. The mean age of participants was 69.5 (±8.8) years. More than half, 256 (61.1%) of the study participants were between the age of 60 to 69 years old and about 213 (51.3%) of the respondents were male. The majority, 402 (95.9%) of the respondents were Orthodox Christian in their religion, and 412 (98.3%) were Tigray in ethnicity. More than half, 236 (56.3%) of the participants had no formal education, and near to one fourth, 103 (24.6%) of the respondents were farmers (Table 1).
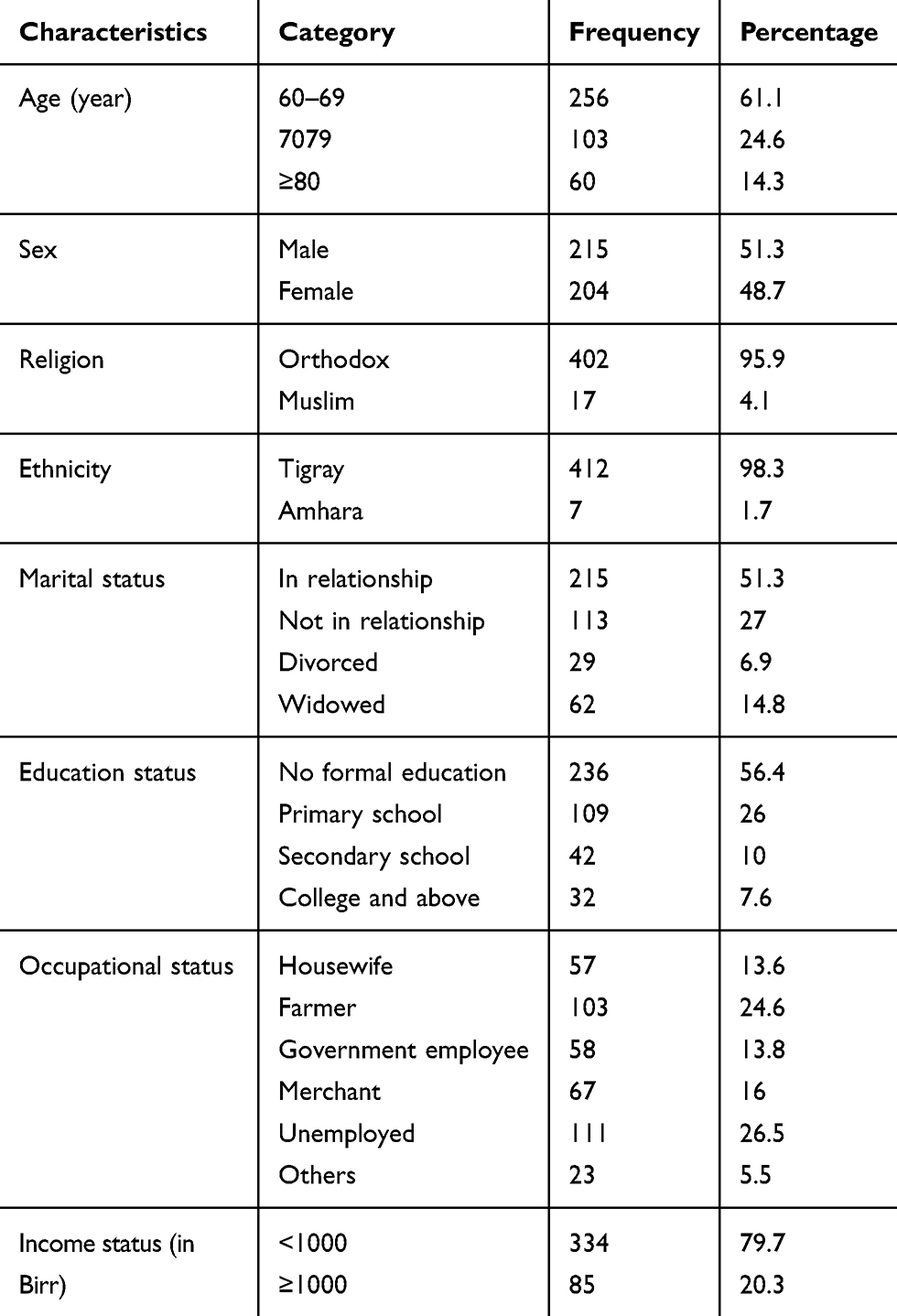 |
Table 1 Socio-Demographic Characteristics of High-Risk Age Groups to COVID-19 Prevention and Control in Korem District, Tigray, Ethiopia (N=419), April 2 to May 9/2020 |
Knowledge, Attitude, and Practice-Related Characteristics
From the total, 158 (37.7%, 95% CI: (33.2, 42.5)) study participants were found with poor knowledge of COVID-19 prevention and control (Figure 1). The majority, 414 (98.8%) of the respondents had heard the information about COVID-19 prevention and control and among these numbers, 150 (35.8%) and 135 (32.2%) had heard from television and health care providers, respectively. One hundred fifty-one (36%) of the respondents did not know the highest risk group to COVID-19. The majority, 395 (94.5%) of the participants had known the sign, symptoms, and preventive methods of COVID-19 (Table 2).
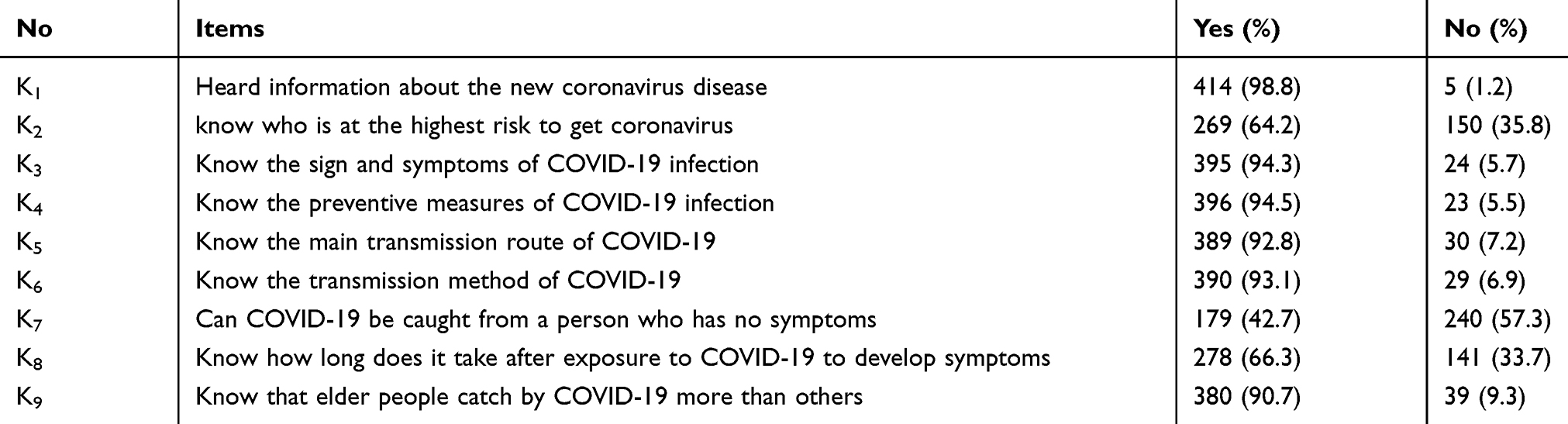 |
Table 2 Knowledge of Participants About COVID-19 Among the Risky Age Group in Korem, Tigray, Ethiopia (N=419), April 2 to May 9/2020 |
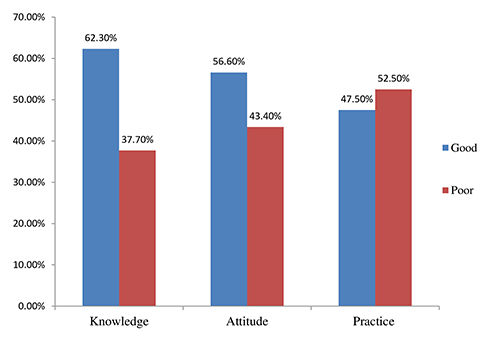 |
Figure 1 Knowledge, attitude, and practice of high-risk age groups to COVID-19 prevention and control in Korem district, Tigray, Ethiopia, April 2 to May 9/2020. |
Concerning attitudes, 182 (43.4%) (95% CI: 38.7, 48.4) of the respondents had a poor attitude to COVID-19 prevention and control (Figure 1). Three hundred thirty-two (79.2%) of the respondents had believed that they are at risk of getting to COVID-19. A total, 342 (81.6%) of the participants were aware of ongoing activities towards the disease. Two hundred thirty-eight (56.8%) and 233 (55.6%) of the respondents globally and in Ethiopia, respectively, had believed that COVID-19 can be controlled successfully. A total, 339 (80.9%) of the respondents had believed that COVID-19 can be transmitted from humans to humans (Table 3).
 |
Table 3 Attitude of Participants About COVID-19 Among Risky Age Groups in Korem, Tigray, Ethiopia (N=419), April 2 to May 9/2020 |
Regarding the preventive practice, about 220 (52.5%) (95% CI; 47.1, 57.5) of the respondents had a poor practice of COVID-19 prevention and control (Figure 1). The Majority, 401 (95.7%) of the respondents had washed their hands with water and soap. Two hundred ninety-nine (71.4%) of the respondents had gone to the crowded area. About three-fourth, 319 (76.1%) of the respondents were not used any hand-rub-based alcohol or sanitizer, near to half, 198 (47.3%) of the participants were not applied physical distance in every moment, and more than one-third,153 (36.5%) of the respondents did not cover their mouth and nose with a tissue or other material during sneezing and coughing. More than half, 237 (56.6%) of the participants did touch their eyes and noses before they wash their hands by water, soap, or sanitizer daily. A total, 372 (88.8%) of participants had declared that they did not use any type of mask in crowded and during their movement (Table 4).
 |
Table 4 Preventive Practice of Participants About COVID-19 Among the Risky Age Group in Korem, Tigray, Ethiopia (N=419), April 2 to May 9/2020 |
Statistically Significant Factors
The Uni-variable analysis shows that high-risk age groups of ≥80 and with no formal educational status had poor knowledge and practices about different aspects of COVID-19 prevention and control. Those participants who are widowed, divorced, unemployed, and dependent in their family member and with an income of less than one thousand Ethiopian birrs had poor knowledge and practice to COVID-19 prevention and control (Table 5).
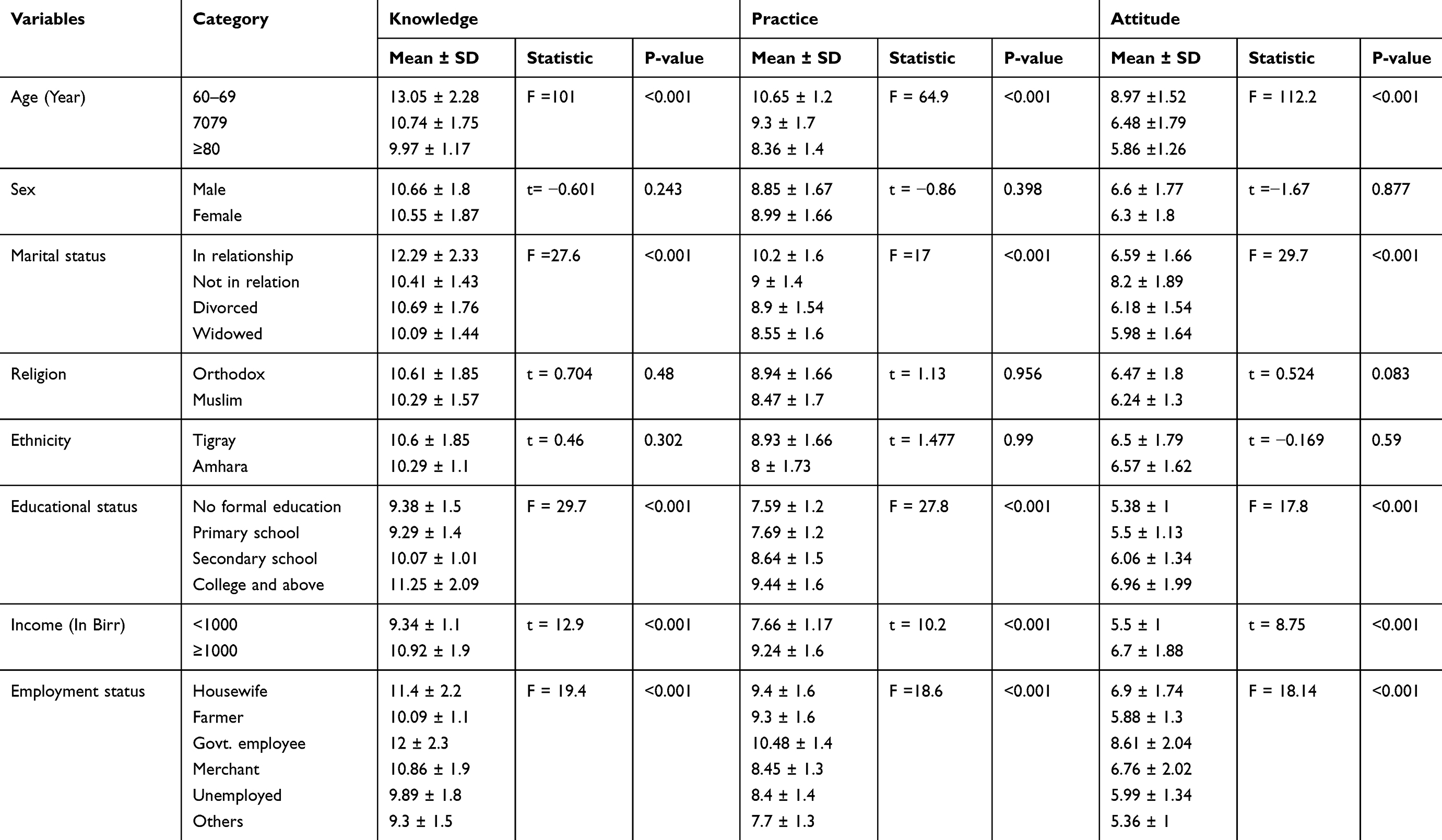 |
Table 5 Univariable Analysis of Demographic Characteristics with Knowledge, Attitude, and Practice Scores of High-Risk Age Groups to COVID-19 Prevention and Control in Korem District, Tigray, Ethiopia, April 2 to May 9/2020 |
On the multivariate analysis, age groups of eighty or above of the respondents had a poor level of knowledge and practices to COVID-19 prevention and control than the age of 60–69 years old. High-risk age groups with no formal educational status had a poor level of knowledge and practice to COVID-19 prevention and control as compared to those colleges and above. Concerning marital status widowed and divorced respondents had poor knowledge and practice to COVID-19 prevention and control than those who are in a relationship. Participants with an income of fewer than one thousand birrs had poor knowledge and practice to COVID-19 prevention and control than those with their income were greater than one thousand and participants who were unemployed and dependent in their family member had poor knowledge and practice towards COVID-19 prevention and control than the employees which were statistically significant (Table 6).
 |
Table 6 Multivariate Linear Regression of Statistical Association Between Demographic Characteristics with Knowledge, Attitude, and Practice Scores of High-Risk Age Groups to COVID-19 Prevention and Control in Korem District, Tigray, Ethiopia, April 2 to May 9/2020 |
Discussion
Currently, the alarmingly spread of COVID-19 is a major public issue in the world. So far no treatment or vaccine is discovered for it. Therefore, prevention is the best solution. Effective prevention and control of COVID-19 are achieved through increasing the population’s knowledge, attitude, and practice towards COVID-19 prevention and control especially high-risk age groups.
The current study assessed the knowledge, attitudes, and practice of high-risk age groups in Korem district regarding COVID-19 prevention and control. In this study, the overall finding of the study participants was poor knowledge (37.7%, 95% CI: (33.2, 42.5)), negative attitude (43.4%, 95% CI: (38.7, 48.4)), and poor practice (52.5%, 95% CI: (47.1, 57.5)) to COVID-19 prevention and control this finding is almost similar with a study conducted in Addis Zemen hospital northwest Ethiopia.18 This might be due to the similarities in access to information, knowledge, Socio-demographic characters, and awareness of the community. But the poor knowledge, negative attitude and poor practice finding of this study are lower than from the study conducted in Jimma, Ethiopia,19 Iran,2,20 China,21 Jordan,22 and Uganda.23 The reason for this discrepancy might be due to a difference in the socioeconomic status of study participants, variation in time of data collection period, sample size, target populations, study participants, and study area of the study participants, it may also be due to the differences in a tool used for assessment of the knowledge, attitude, and practice. In these studies done in China, Uganda, and Iran, the data were collected during the main phase of the outbreak when most of their populations were exposed to a lot of information about COVID-19. The majority of the Korem district population had no access to electricity and internet17 as a result, they had limited access to COVID-19-related updates and preventive measures posted online by the official government health authorities and different media that are shown to have a positive effect for improving knowledge, behavioral change and to develop a positive attitude.
High-risk age groups with no formal educational status were found significantly associated with poor knowledge, negative attitude, and poor practice regarding COVID-19 prevention and control which is consistent with the study conducted in Ethiopia and Iran.2,18 The similarities might be due to the similar educational status of the study populations, and similarities in the information, awareness of the study participants. And when someone gets more educated he/she will have a better understanding of control measures and preventive strategies related to COVID19, and the ability to practice recommendations to protect COVID-19 will increase.
In this study, participants with low-income status were found significantly associated with poor knowledge, negative attitude, and poor practice regarding COVID-19 prevention and control which is similar to the study done in Ethiopia,18 United States,24 and Malaysia.25 These similarities might be because low monthly income leads to a feeling of inability to change one’s behavior or condition, and finally inability of executing recommended protective behaviors of COVID-19.
Elders greater than or equal to 80 years old were found significantly associated with poor knowledge, negative attitude, and poor practice regarding COVID-19 prevention and control which is consistent with the study conducted in Addis Zemen, Ethiopia,18 United State,24 and China.21 These similarities might be due to the reason that as age increases hearing ability and visual performance get decreased due to aging and make it challenging to read or understand medical instructions. Besides, aging-associated loss of cognition might cause similar challenges.
Limitations
Measurement of practice using mean is a limitation given predictive validity of a score greater than the mean is not assured. The age of 60 years as a high-risk group in Ethiopia may not be the same as the age of 60 in other high-income countries.
Conclusion
Generally, the overall prevalence of knowledge, attitude, and practice regarding COVID-19 prevention and control was found poor. Being older age (≥80), illiterate, and having less income were significantly associated factors to KAP among high-risk age groups regarding COVID-19 prevention and control. Further, it is important to share this information and evidence with decision-makers and health care workers to address and strengthen health education, information dissemination on the issues such as knowledge, attitude, and practice of high-risk age groups on a special focus program and strategies. Continuous encouragement of people about the preventive and control measures, especially in lower educated people, elders, and those who have less income and dependent on their families is recommended.
Abbreviations
ANOVA, analysis of variance; COVID-19, coronavirus disease-2019; KAP, knowledge, attitude, and practice; WHO, World Health Organization.
Data Sharing Statement
The datasets used and/or analyzed during the current study are available from the principal author upon reasonable request.
Ethical Consideration
The study was conducted following the declaration of Helsinki on human subjects. After the purpose, benefit and risk was briefed, informed consent was obtained from the study participants. Ethical clearance was secured by Adigrat University Institutional Health Research Ethics Review Committee (IHRERC) and official permission was obtained from Korem district health office and municipal.
Acknowledgments
We thank all the study participants for their voluntary participation and for providing essential information. We would also extend our heartfelt thanks to the data collectors and supervisors for their responsible data collection and support.
Author Contributions
Both authors made a significant contribution to the work reported during:
The conception, study design, execution, acquisition of data, analysis and interpretation, drafted or written, or substantially revised or critically reviewed the article.
Agreed on the journal to which the article will be submitted.
Reviewed and agreed on all versions of the article before submission, during revision, the final version accepted for publication, and any significant changes introduced at the proofing stage.
Agree to take responsibility and be accountable for the contents of the article.
Funding
There is no funding to report..
Disclosure
The authors declare that there is no conflict of interest.
References
1. Adhikari SP, Meng S, Wu Y-J, et al. Epidemiology, causes, clinical manifestation and diagnosis, prevention and control of coronavirus disease (COVID-19) during the early outbreak period: a scoping review. Infect Dis Poverty. 2020;9(1):29. doi:10.1186/s40249-020-00646-x
2. Erfani A, Shahriarirad R, Ranjbar K. Knowledge, attitude and practice toward the novel coronavirus (COVID-19) outbreak: a population-based survey in Iran. Bull World Heal Organ. 2020;3.
3. Lana RM, Coelho FC, Gomes MF da C, et al. The novel coronavirus (SARS-CoV-2) emergency and the role of timely and effective national health surveillance. Cad Saúde Pública. 2020;13(36):e00019620. doi:10.1590/0102-311x00019620
4. World Health Organization. Novel Coronavirus (2019-nCoV) Situational report - 2; 2020.
5. World Health Organization. WHO Director-General’s opening remarks at the media briefing on COVID-19. Geneva, Switzerland: world Health Organization; —11 March 2020. Lancet Respir Med. 2020.
6. Gorbalenya AE, Baker SC, Baric RS, et al. The species severe acute respiratory syndrome-related coronavirus: classifying 2019-nCoV and naming it SARS-CoV-2. Nat Microbiol. 2020;2:1–9.
7. European Centre for Disease Prevention and Control. Novel coronavirus disease, Stockholm. Novel coronavirus disease 2019 (COVID-19) pandemic: increased transmission in the EU/ EEA and the UK – sixth update. 2020:28.
8. Kamel Boulos MN, Geraghty EM. Geographical tracking and mapping of coronavirus disease COVID-19/severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) epidemic and associated events around the world: how 21st century GIS technologies are supporting the global fight against outbreaks and epidemics. Int J Health Geogr. 2020;19.
9. Wordometer COVID19 coronavirus Update. 2020;382(10):970–971.
10. World Health Organization MERS situation update. Coronavirus disease 2019 (COVID19) situation report-51. N Engl J Med. 2020;382(10):970–971.
11. Huang C, Wang Y, Li X, et al. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Lancet. 2020;395(10223):497–506. doi:10.1016/S0140-6736(20)30183-5
12. Yang X, Yu Y, Xu J, et al. Clinical course and outcomes of critically ill patients with SARS-CoV-2 pneumonia in Wuhan, China: a single-centered, retrospective, observational study. Lancet Respir Med. 2020;24:31.
13. Guo T, Fan Y, Chen M, et al. Cardiovascular implications of fatal outcomes of patients with Coronavirus Disease 2019 (COVID-19). JAMA Cardiol. 2020;27.
14. Hopman J, Allegranzi B, Mehtar S. Managing COVID-19 in low-and middle-income countries. JAMA Lancet Respir Med. 2020;11.
15. World Health Organization. Critical preparedness, readiness and response actions for COVID-19: interim guidance. Br J Nurs. 2020;29(3):166–167.
16. Cowling BJ, Leung GM. Epidemiological research priorities for public health control of the ongoing global novel coronavirus (2019-nCoV) outbreak. Eurosurveillanc. 2020;25:6. doi:10.2807/1560-7917.ES.2020.25.6.2000110
17. Centeral Statistical Agency (CSA). Korem district Health office report, CSA. Nat Med. 2018;10(4):368–373.
18. Akalu Y, Ayelign B, Molla MD. Knowledge, attitude and practice towards COVID-19 among chronic disease patients at Addis Zemen Hospital, Northwest Ethiopia. Infect Drug Resist. 2020;Volume 13:1949–1960. doi:10.2147/IDR.S258736
19. Kebede Y, Yitayih Y, Birhanu Z, Mekonen S, Ambelu A. Knowledge, perceptions and preventive practices towards COVID-19 early in the outbreak among Jimma university medical center visitors, Southwest Ethiopia. PLoS One. 2020;15(5):e0233744. doi:10.1371/journal.pone.0233744
20. Shahbaznejad L, Navaifar MR, Arabi M, et al. Knowledge, attitude and practice of Sari Birth Cohort members during early weeks of COVID-19 outbreak in Iran.BMC Public Health 2020.
21. Zhong B-L, Luo W, Li H-M, et al. Knowledge, attitudes, and practices towards COVID-19 among Chinese residents during the rapid rise period of the COVID-19 outbreak: a quick online cross-sectional survey. Int J Biol Sci. 2020;16(10):1745–1752. doi:10.7150/ijbs.45221
22. Khasawneh AI, Humeidan AA, Alsulaiman JW, et al. Medical students and COVID-19: knowledge, attitudes, and precautionary measures. A descriptive study From Jordan. Front Public Health. 2020;8.
23. Olum R, Chekwech G, Wekha G, Nassozi DR. Frontiers Coronavirus Disease-2019: Knowledge, Attitude, and Practices of Health Care Workers at Makerere University Teaching Hospitals. Uganda: Public Health; 2020.
24. Wolf SM, Serper M, Opsasnick L, Conor RMO, Curtis LM. Awareness, attitudes, and actions related to COVID-19 among adults with chronic conditions at the onset of the U. S. Outbreak Ann Intern Med. 2020;9:1–10. doi:doi:10.7326/M20-1239.
25. Azlan AA, Hamzah MR, Sern TJ, Ayub SH, Mohamad E. Public knowledge, attitudes and practices towards COVID-19: A cross-sectional study in Malaysia. PLoS One. 2020;15(5):e0233668. doi:10.1371/journal.pone.0233668
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.