")
Back to Journals » Breast Cancer: Targets and Therapy » Volume 11
Knowledge and practices on breast cancer detection and associated challenges among women aged 35 years and above in Tanzania: a case in Morogoro Rural District
Authors Ng’ida FD, Kotoroi GL, Mwangi R, Mabelele MM , Kitau J , Mahande MJ
Received 29 December 2018
Accepted for publication 11 March 2019
Published 28 May 2019 Volume 2019:11 Pages 191—197
DOI https://doi.org/10.2147/BCTT.S199889
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Pranela Rameshwar
Faraja D Ng’ida,1 Gladness L Kotoroi,2 Rose Mwangi,3 Mabula M Mabelele,1 Jovin Kitau,4 Michael J Mahande5,6
1Department of Epidemiology and Biostatistics, Institute of Public Health, Kilimanjaro Christian Medical University College, Moshi, Tanzania; 2Department of Reader Service, Mzumbe University, Morogoro, Tanzania; 3Department of Epidemiology and Biostatistics, Institute of Public Health, Kilimanjaro Christian Medical University, Moshi, Tanzania; 4Department of Parasitology, Kilimanjaro Christian Medical University College, Moshi, Tanzania; 5Department of Epidemiology & Biostatistics, Institute of Public Health, Kilimanjaro Christian Medical University College, Moshi, Tanzania; 6Department of Community Health, Institute of Public Health, Kilimanjaro Christian Medical Centre, Moshi, Tanzania
Background: Breast cancer is the leading cause of cancer-related deaths among women globally including Tanzania. However, timely access to diagnosis remains a challenge due to lack of specialized facilities. Most patients presents with advanced stages of the disease making management impossible. This leads to an increase in breast cancer-related mortality. Little is known about knowledge and practices on breast cancer screening in Tanzania. This study described knowledge and practices on breast-cancer detection and associated challenges among women aged 35 years and above in Morogoro rural District in Tanzania.
Methods: This descriptive cross-sectional study was conducted in Lubungo, Newland and Fulwe villages at Mikese ward in Morogoro rural District from June and July 2017. A standardized questionnaire was used to obtain information from 130 study participants regarding breast cancer knowledge and practices. Data were analyzed using (SPSS) software version 23 and descriptive statistics were summarized in frequencies and percentages.
Results: One hundred and thirty women were studied, all participants have heard of breast cancer; 71.5% knew the effects of breast cancer; 37.7% knew about the signs and symptoms. The most frequently reported cause and risk factor of breast cancer were putting money under brassiere (30.8%) and fat diet (17.7%) respectively. The participants (73.8%) have never heard of breast self-examination (BSE) as an early detection method of breast cancer hence do not practice it. Lack of knowledge on early signs and symptoms of breast cancer was reported as the main challenge for breast cancer screening (73.8%). The frequently reported source of information about this disease was television/radio programs (83.1%).
Conclusion: Most of the women have heard of breast cancer but they lack adequate knowledge on its risk factors, causes, symptoms and effects. The majority of the women do not practice BSE due to lack of knowledge. Efforts to improve women’s knowledge on breast cancer is warranted.
Keywords: breast cancer detection, knowledge, practices, Tanzania
Background
Breast cancer is the most common cancer among women globally.1,2 The incidence of breast cancer has been reported to increase in the developing countries in the recent years due to the increase in life expectancy, urbanization and adoption of western lifestyles.3Breast cancer is diagnosed at a very late stage in developing countries.2 Approximately 50% of breast cancer cases and 58% of deaths have been reported to occur in the developing countries.2 The high mortality rate attributed to breast cancer in sub-Saharan Africa is partly due to lack of knowledge pertaining to risk factors, signs and symptoms such as breast lump, increase in size of the breast and an ulcer on the breast, and early detection methods among women as well as effects such as breast amputation and death are causing these women to seek medical treatment at late stages of the disease when it can no longer be reversed.1,5
In addition, patients, healthcare providers, and system-mediated barriers have also been reported as reasons for late seeking of care among cancer patients.6 For example, there are very few places with specialized capacity for diagnosis of breast cancer as most of these cancer facilities and diagnostic centers are available only in tertiary hospitals making the services less accessible, especially in remote parts of the country. If a woman detects a breast lump in a rural area like Mikese, she has to go to a primary health care center where she has to pay for the services and referall arrangements have to be made. But following screening by different NGOs such as MEWATA (The Medical Women Association of Tanzania), women who are identified with a lump in their breasts are linked to care through referral to the national cancer institute where most of the cost related to treatment is covered by the government.6Consequently, 75–80% of the affected women report very late tohealth centers, often with advanced stages of the disease forwhich no medical intervention can be taken for curative and/or management purposes.4,7
Women looking at and feeling their breasts (which are components of breast self-examination, BSE) is considered to be the best method for early detection of breast cancer and the best option for interval screening among women of all ages.5,8 Other breast cancer detection methods include clinical breast examination (CBE) and mammography.9,12 BSE is an option for women from 20 years of age and above in areas where access to CBE and mammography is rare as in many sub-Saharan African countries including Tanzania.9
To prevent and control breast cancer, several measures have been taken by the WHO, government health ministries, and nongovernmentmental organizations (NGOs). In Tanzania, the Ministry of Heath, Community Development, Gender and Elderly and Children is working to achieve goals in its action and strategic plan to control and prevent cancer for 2016–2020. The goals include a 50% increase in proportion of patients detected with early stage breast cancer, beginning by organizing breast cancer screening and outreach services in 13 regions of the country 4 Early detection of breast cancer leads to better prognosis.1,5,10 A lot has been done by various institutions such as television stations including ITV (Independent Television) and NGOs like MEWATA to sensitize, educate and test for these conditions in many parts of the country.13
However, little has been done in rural communities like the Mikese community of Morogoro region to determine changes in women’s perception following educational and sensitization initiatives with regard to breast cancer.13 There is a need therefore to investigate how much this has changed/improved their understanding and practices regarding breast cancer.
The present study is important as it will bring to light the current level of knowledge on breast cancer among rural women in Mikese, Morogoro Rural District, which is representing rural areas in Tanzania. It will also help in promoting early detection and management of breast cancer in the communities by helping both central and local government, and NGOs such as MEWATA in understanding where exactly to allocate resources in matters pertaining to breast cancer awareness and practices among women especially in rural areas.
This study aimed to describe the knowledge and practices on breast cancer and associated challenges among women aged 35 years and above in Mikese, Morogoro Rural District, Morogoro Region.
Methods
Study design and study setting
This was a descriptive cross-sectional study conducted from June to July 2017 in Morogoro Rural District in Mikese Ward. Villages from the ward were selected through simple random sampling by replacement to give each village an equal probability of being selected. Each village was numbered and balloting of the numbers in a basket was done to get the three villages (Fulwe, Lubungo and Newland) out of the five villages in the ward.
Morogoro Rural is one of the six districts of Morogoro region of Tanzania. It is bordered to the north and east by the Pwani Region, to the south by Kilombero District, to the southwest by Kilosa district and to the west by Mvomero and the Morogoro Urban District. According to the Tanzania national population census of 2012, Morogoro Rural was estimated to have a population size of 286,248 people, covering 12,457.44 km2.14 Mikese Ward was estimated to have a population size of 15,569 people, 7,951 males and 7,618 females.14 Mikese Ward is located on the main road from Dar es Salaam to Morogoro. The area is mountaneous in nature, fertile, and small- scale agriculture is the main economic activity. It has a total of four dispensaries, without any health center or hospital, which can be easily accessed by the ward members.14
Study population, sample size, and sampling procedure
The study population comprised of all women aged 35 years and above in the selected villages of Mikese Ward. Women of this age were selected based on the fact that they are at a higher risk of developing breast cancer compared to their younger counterparts. The final sample size was 130 women which was determined using a previous study by Morse et al in Dar es Salaam, Tanzania.6
The method used was multistage sampling, whereas the region was selected then district, division, ward, villages and finally the households where the women live. Participants were reached either at their working places (for those selected households where the women were at work) or home residence. We excluded women with a history of mental illness and women working in health centers.
Data collection methods and tools
A standardized questionnaire which comprised of both closed and open-ended questions was used. The questionnaire was translated into Swahili which was then used by the researcher (principal investigator) to interview the consenting participants and recorded their responses in the questionnaires respectively, as most of the rural women are illiterate and do not understand English. The questionnaire was divided into five sections: (1) sociodemographic characteristics of the participants, (2) knowledge on breast cancer: causes, risk factors, signs, and symptoms, effects and health care seeking behavior,(3) sources of information used by these women to get knowledge on the subject matter, (4) practices on early detection methods for breast cancer, and (5) the challenges these women face in breast cancer detection. The questionnaire used was developed based on questions which were adopted in previous peer-reviewed published studies and those selected based on discretion.2,6–9,12
Ethical consideration
This study was conducted in accordance with the Declaration of Helsinki. Ethical clearance was obtained from Kilimanjaro Christian Medical University College Research and Ethics Committee. Permission to conduct the study was obtained from Morogoro Rural Municipal administrative authority. Verbal consents were sought from individual participants prior to the interview after they had received a full explanation about the objectives and benefits of the study. Verbal consent was preferred to written consent as this study was conducted in a rural area and majority of the population in these settings are illiterate hence written consent would not be possible. This consent form was included in the protocol which was approved by the ethics committee. Participants were also informed that participation in the study was on voluntary basis and the refusal to participate did not have any negative impact on them in terms of accessing their health care services. Both confidentiality and privacy were adhered to where unique patient identification numbers were used instead of names and all interviews were conducted in private.
Data analysis
After completion of data collection in the field, the questionnaires were carried in a bag, they were numbered sequentially and data was checked for completeness, a double entry of data was done in SPSS to exclude data entry errors and inconsistency. Data was then cleaned and analysed using Statistical Package for Social Science (SPSS) version 23 (IBM Corporation, Armonk, NY, USA). Descriptive statistics were summarized using frequencies and percentages for categorical variables.
Results
Demographic characteristics of the respondents
Of the 135 participants who were approached for this study, 130 (96.3%) agreed to participate.
Demographic characteristics of the study participants are summarized in Table 1. A total of 130 women were studied. The majority (70.8%, N=92) were married, aged above 40years (65.4%, N=85) and over a third (37.7%, N=49) of the women were from Fulwe village. The selection of women in the household was done by proportion to the number of the women in each of the selected villages. The higher the number of the study population, the higher the number of women selected, Fulwe village had slightly higher population compared to other villages, hence more women were selected from this village.
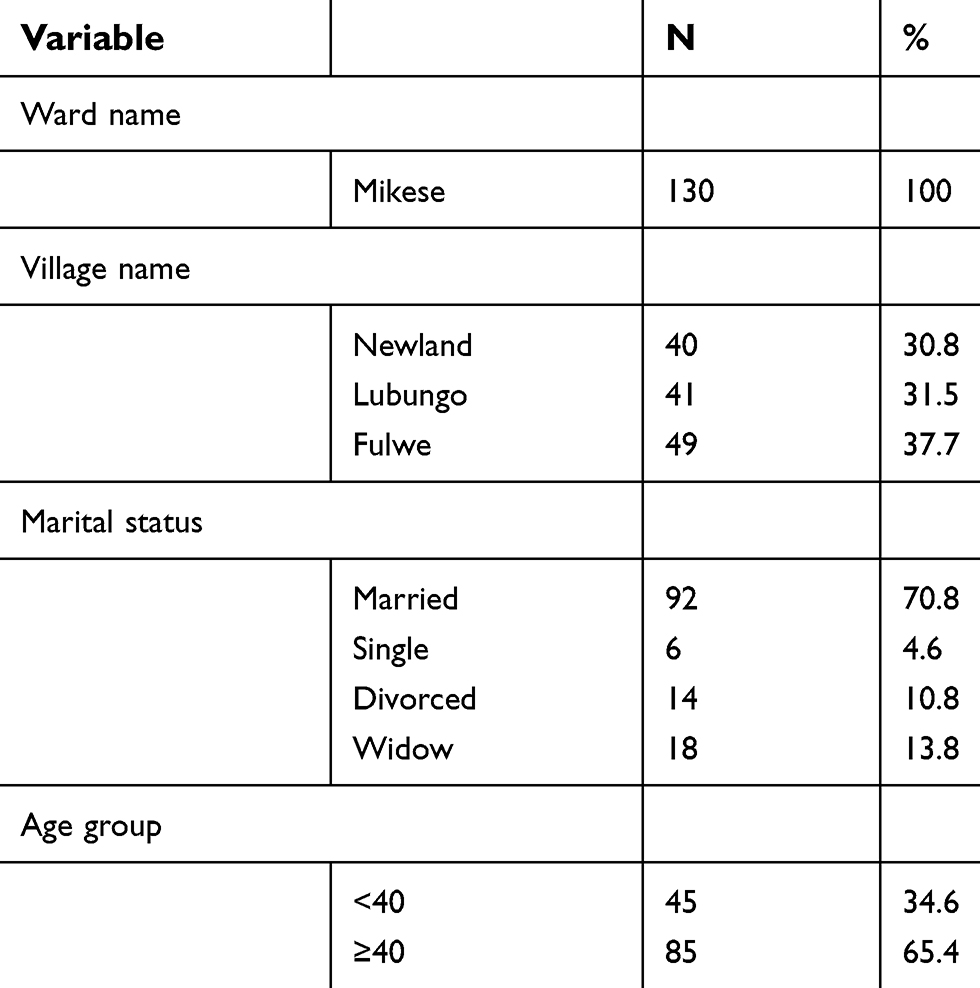 | Table 1 Demographic characteristics of the study participants (N=130) |
Knowledge of the participants on breast cancer
When the respondents were asked if they have ever heard of breast cancer, all the participants reported to have heard of the disease, the commonest (30.8%, N=40) cause of breast cancer reported was putting money under brassiere while scratching of the breasts was infrequently mentioned (6.9%, N=9) (Table 2).
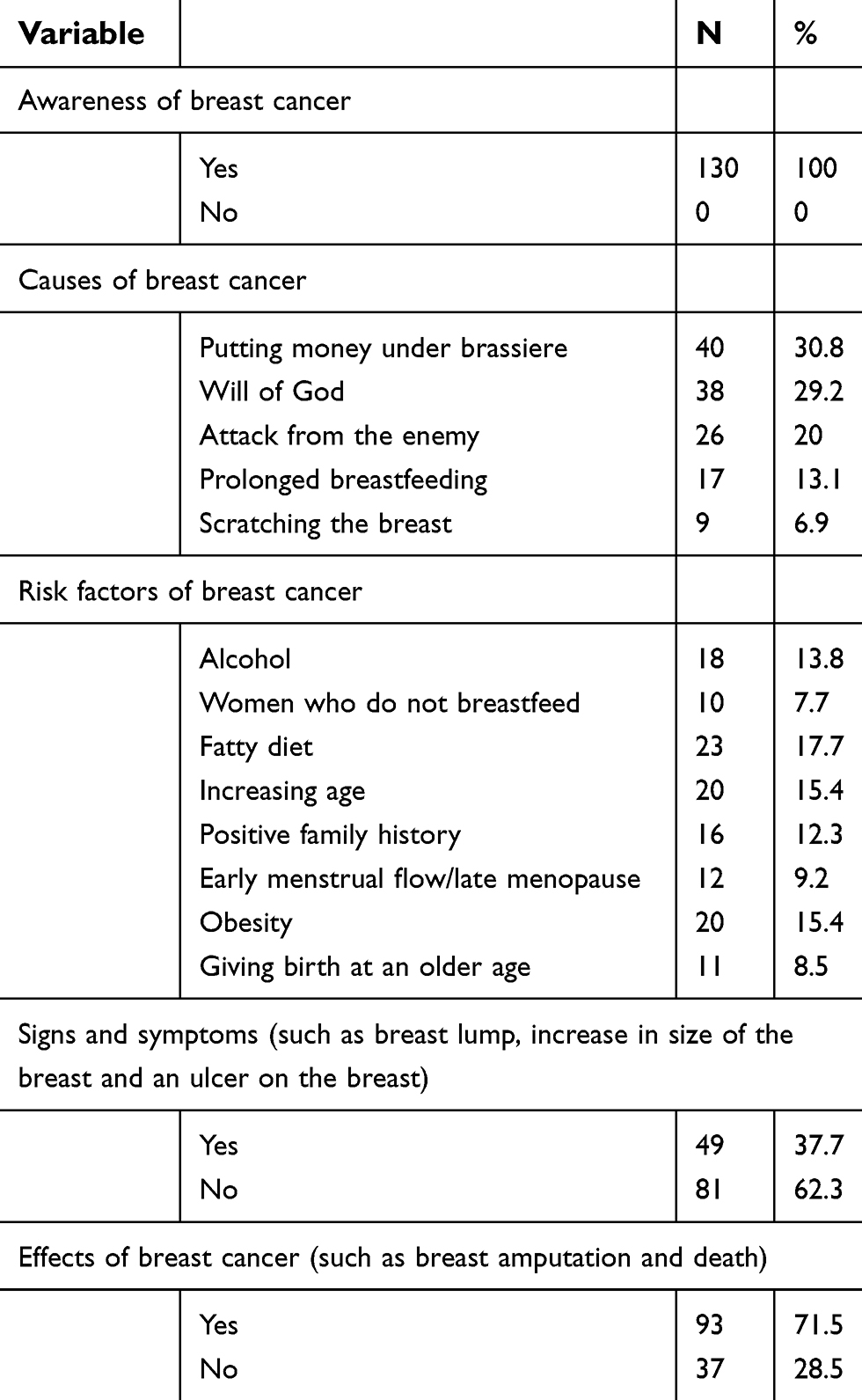 | Table 2 Knowledge of the participants on breast cancer (N=130) |
Participants were also asked about their knowledge on the risk factors of breast cancer. Fat diet was pointed out by 17.7% (N=23) as the highest risk factor, 37.7%, (N=49) of the participants knew about the signs and symptoms such as breast lump, increase in size of the breast and an ulcer on the breast, and 71.5% (N=93) knew about the effects of this disease such as breast amputation and death (Table 2).
Sources of information on breast cancer
Participants were requested to point out the sources of information from which they obtained knowledge on breast cancer. The most frequent source reported was television/radio (83.1%, N=108); colleagues (56.9%, N=74); health workers (45.4%, N=59); clinic (44.6%, N=58) and newspapers (31.5%, N=41), while posters (13.8%, N=18) was infrequently reported (Table 3).
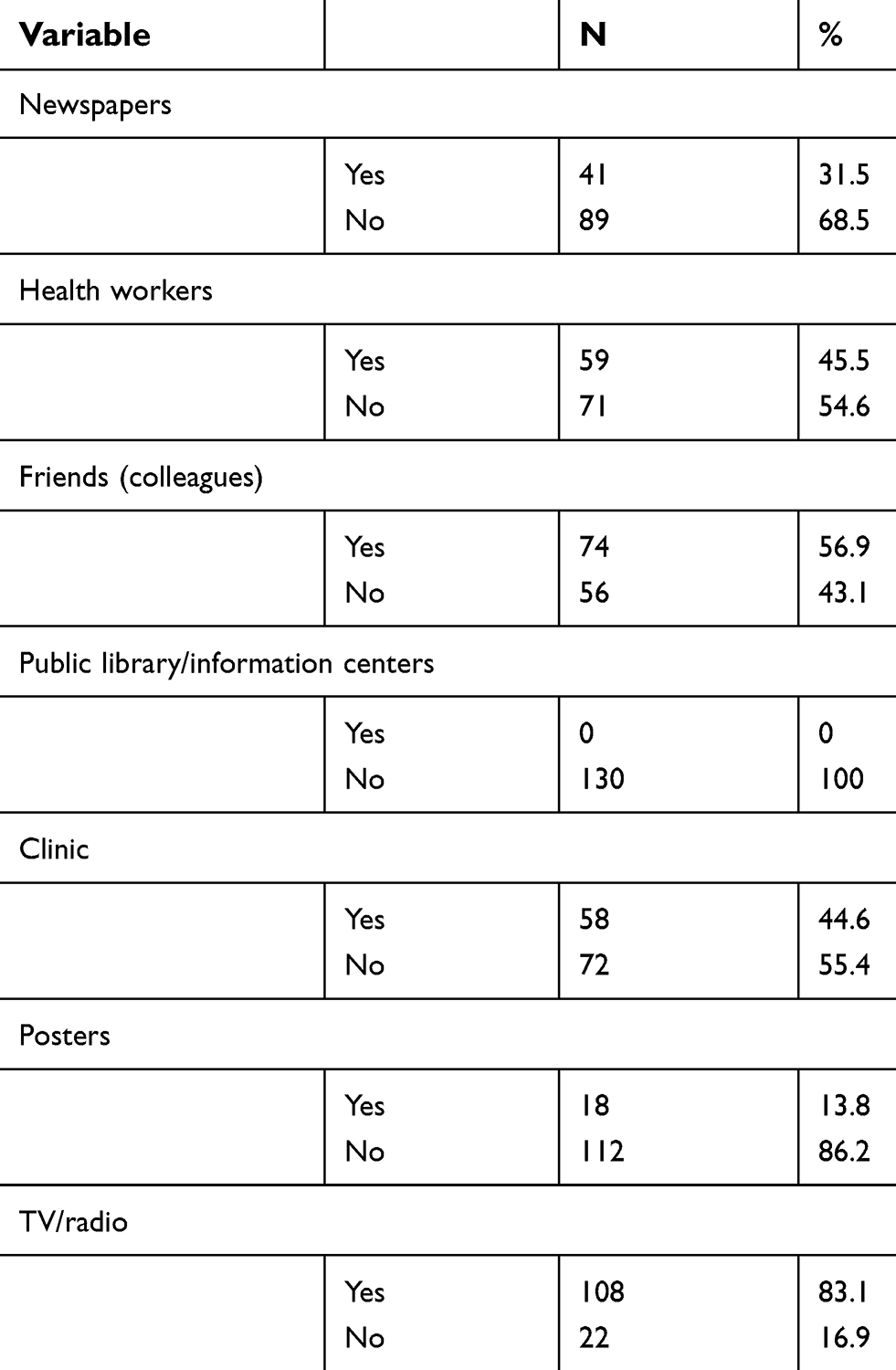 | Table 3 Sources of information used by the participants to get breast cancer information (N=130) |
Breast self-examination practices used by the participants in breast cancer detection
Respondents' knowledge and practice of BSE were described. Participants were asked about awareness and practices of this method. Things asked specifically were steps of BSE in detecting the signs and symptoms of breast cancer, such as looking at their breasts in the mirror with their arms at different positions (at the hips and raised above their shoulders) as well as feeling their breasts with their hands while in lying and sitting positions. The majority (73.8%, N=96) of the participants had never heard of this method, while 18.5% (N=24) of the participants who had knowledge about breast cancer practiced BSE occasionally (Table 4).
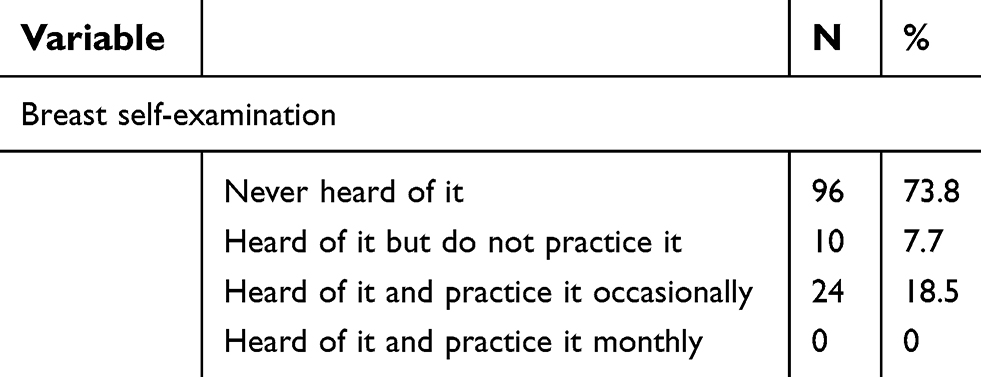 | Table 4 Breast self-examination practices used by the participants in breast cancer detection (N=130) |
Challenges in breast cancer screening
Participants were asked about the challenges they face in breast cancer screening/early detection methods, BSE method to be more specific. The majority (73.8%, N=96) reported lack of knowledge as the main challenge in breast cancer screening. More than half (56.2%, N=73) of the participants did not think of BSE as an important practice to adhere to, while a third (34.6%, N=45) of the participants did not consider themselves to be at risk of getting breast cancer, hence did not think of BSE as an important practice (Table 5).
 | Table 5 Challenges faced by the participants in breast cancer screening (N=130) |
Discussion
It was shown in this study that all of the participants have heard of breast cancer, but only 37.7% knew about the signs and symptoms such as breast lump, increase in size of the breast and an ulcer on the breast, while over two-thirds (71.5%) knew about its effects such as breast amputation and death. Fatty diet was reported to be the commonest risk factor (17.7%) for breast cancer, while women who have never breast-fed were considered to have low risk (7.7%). These findings differ slightly from previous studies done in Dar es Salaam and Saudi Arabia in which alcohol was mentioned as the highest risk factor for breast cancer by 52.9% and 52.7% respectively.5,6 These differences could be due to the differences in the socioeconomic status and culture of the participants between the study populations.
In the present study, putting money under the brassiere (30.8%) was reported as the most frequent cause for breast cancer among the study participants. This coincides with the study in Dar es Salaam, Tanzania, where it was pointed out as the highest cause by the majority (82.2%) of the participants.6 This may be explained by the similarity in the belief system and culture among people in the two populations as they are all located along the same zone within the country.
With regard to the source of information about breast cancer, the majority (83.1%) of the participants in our study reported radio and television programs to be their source of information. These results agree with a study in Nigeria.15 This could be explained by the similarity in the economic status of the participants in the studied population whereby all are from a rural setting in which there is scarce availability of public libraries and/or information centers. However, our results are slightly different from the study done in Saudi Arabia,5 where the authors in the latter study found that press media and television were the highest source of information (83.2% vs 68.2%, respectively).
In this study, the majority of the participants had never heard of BSE and among those who have heard about it, 70.6% practiced it occasionally. These results are different from the study done in Dar es Salaam, Tanzania in which 44% of the participants were aware of BSE.6 Similar findings were reported in Nigeria by15, where at least 19% of the participants practiced BSE monthly. A study in India showed that 55.3% of the urban population were aware of BSE but only 8.9% practiced it.1 These differences may probably be due to the difference in the study settings, the current study being in a rural area and the latter being in urban areas more likely to know about BSE and practice it regularly than those in the rural setting.
Furthermore, this study also showed lack of knowledge on breast cancer to be the main challenge in breast cancer screening. This is in agreement with a study in Zambia7 in which 55% of the participants in an urban setting and 65% in a rural setting reported lack of knowledge as the main challenge for breast cancer screening. The similarity in findings between these studies indicates that lack of knowledge in this matter is a problem in various African societies, therefore, more effort should be made to educate women in these areas.
Study strengths and limitations
To our understanding this is the first study to be documented about knowledge and practices on breast cancer detection and the associated challenges among women in Mikese, Morogoro Rural. The methodology used provided an opportunity to follow up and clarify some issues to the respondents as well as including the illiterate candidates. In addition, the study targeted women of 35 years and above who are at a higher risk of developing breast cancer. Lastly this study has provided a basis for future research.
The present study also had some limitations: information was gathered by means of a questionnaire only. The results of this study were dependent on the accuracy and truthfulness of the participants’ responses. All these may lead to information bias. Furthermore, this study included only women from rural Tanzania, therefore, findings cannot be generalized to women from urban areas.
Conclusions
This study revealed that the majority of women have heard of breast cancer but they lack adequate knowledge on its risk factors, causes, symptoms, and effects. The majority of the women do not practice BSE citing lack of knowledge as the main reason. It is our opinion that in order to promote early detection of breast cancer, efforts should be made to improve womens’ knowledge of breast cancer. Furthermore women reported radio and television as their primary source of information, which provides a good opportunity for sharing information on breast cancer.
Availability of the data and materials
Data used in this work will be available for sharing with the scientific community, Mikese Ward executive officer for policy implementation and a copy will be sent to Kilimanjaro Christian Medical University College Library in case requested. Furthermore, this data will be available for use whenever requested.
Consent to publish
Participants consented for the data to be published to ensure that information they provided benefits the public.
Acknowledgments
The authors thank the Community Department of Kilimanjaro Christian Medical University College and the Morogoro Rural Municipal Director for organizing and making this work successful. This was a student work as partial fulfillment to accomplish the first author’s medical degree program, and it was purely self-sponsored.
Author contributions
All authors contributed to data analysis, drafting or revising the article, gave final approval of the version to be published, and agree to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Sehrawat JS, Mor S. Knowledge, beliefs and practices about breast cancer and its self examination procedure among urban and rural women of district Gurdaspur, Punjab, India: a cross sectional study. Int J Community Med Public Health. 2017;4(1):120–128. doi:10.18203/2394-6040.ijcmph20164723
2. Azubuike SO, Okwuokei SO. Knowledge, attitude and practices of women towards breast cancer in Benin City, Nigeria. Ann Med Health Sci Res. 2013;3(2):155–160. doi:10.4103/2141-9248.113653
3.
4.
5. Dandash KF, Al-Mohaimeed A. Knowledge, attitudes and practices surrounding breast cancer and screening in female teachers of Buraidah, Saudi Arabia. Int J Health Sci. 2007;1(1):61–71.
6. Morse EP, Maegga B, Joseph G, Miesfeldt S. Breast cancer knowledge, beliefs and screening practices among women seeking care at district hospitals in Dar es Salaam, Tanzania. Breast Cancer Basic Clin Res. 2014;8(10):73–79. doi:10.4137/BCBCR.S13745
7. Mukupo FC, Ngoma CA. Breast cancer knowledge and breast self examination practice among rural and urban women in Zambia. Afr J Nurs Midwifery. 2007;9(1):50–58.
8. Bi Suh MA, Atashili J, Fuh EA, Eta VA. Breast self-examination and breast cancer awareness in women in developing countries: a survey of women in Buea, Cameroon. BMC Res Notes. 2012;5(621):1.
9. Elsie KM, Gonzaga MA, Francis B, et al. Current knowledge, attitudes and practices of women on breast cancer and mammography at Mulago Hospital. Pan Afr Med J. 2010;3(9):9.
10. Akhigbe AO, Omuemu VO. Knowledge, attitudes and practice of breast cancer screening among female health workers in a Nigerian Urban City. BMC Cancer. 2009;9(203):203.
11. Heidari Z, Mahmoudzadeh-Sagheb HR, Sakhavar N. Breast cancer screening knowledge and practice among women in Southeast of Iran. Acta Med Iran. 2008;46(4):321–328.
12. Opoku SY, Benwell M, Yarney J. Knowledge, attitudes, beliefs, behavior and breast cancer screening practices in Ghana, West Africa. PanAfr Med J. 2012;11:28.
13.
14.
15. Gwarzo UMD, Sabitu K, Idris SH. Knowledge and practice of breast-self examination among female undergraduate students of Ahmafu Bello University Zaria, Northwestern Nigeria. Ann Afr Med. 2009;8(1):55–58.
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.