")
Back to Journals » Infection and Drug Resistance » Volume 14
Knowledge and Practice Toward Prevention of SARS-CoV-2 Among Healthcare Workers at Delghi Primary Hospital During a Massive Test Campaign in Northwest Gondar, Ethiopia: Institution-Based Descriptive Cross-Sectional Survey
Authors Shibabaw T , Teferi B
Received 2 November 2020
Accepted for publication 20 January 2021
Published 2 February 2021 Volume 2021:14 Pages 381—390
DOI https://doi.org/10.2147/IDR.S289965
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Suresh Antony
Tewodros Shibabaw,1 Banchamlak Teferi2
1Department of Biochemistry, School of Medicine, College of Medicine and Health Sciences, University of Gondar, Gondar, Ethiopia; 2Department of Clinical Pharmacy, School of Pharmacy, College of Medicine and Health Sciences, University of Gondar, Gondar, Ethiopia
Correspondence: Tewodros Shibabaw
Department of Biochemistry, School of Medicine, College of Medicine and Health Sciences, University of Gondar, P.O. Box: 196, Gondar, Ethiopia
Tel +251910162171
Email [email protected]
Background: Since December 29, 2019, severe acute respiratory syndrome coronavirus (SARS-CoV-2) has been spreading and is associated with notoriously increased morbidity and mortality of populations worldwide, including Ethiopia. Medicine and the healthcare system have been challenged by both first and second-waves of SARS-CoV-2. During this entire crisis, the main purpose of this study was to determine the current evidence on the level of awareness and prevention practice of healthcare workers (HCWs) at the district primary hospital, Delghi Primary Hospital (DPH) regarding COVID-19 in the overall effort to control the spread of the virus.
Methods: Institutional-based descriptive cross-sectional analysis was performed between late August and September 20, 2020. Participants of the study were HCWs with various occupations at DPH, North West Gondar, Ethiopia. In this study, among 112 health professions, we included a total of 104 HCWs. Written consent was obtained for willingness of the study participants from the DPH administrative office. Then, using a pre-tested, structured, and self-administered questionnaire, data were collected. The questionnaire included socio-demographics, sources of information, knowledge, and practice measures regarding COVID-19. The collected data were analyzed through IBM SPSS version 20. As a cut-off value, ≥ 8 out of 15 knowledge questions and ≥ 7 out of 14 practice questions were considered good knowledge and practice, respectively.
Results: The result of this study showed the majority of the respondents were male (71/104, (68.3%)), with a median age of 28 (minimum age 20 and maximum age 50) years. Thus, 94.2% (n=98/104) was the overall rate of correctly answered questions out of 15 knowledge questions. However, 40.6% of them had poor prevention practices. 73.1% of participants used regular hand-washing with soap and 64.4% used hand sanitizer and handshake avoidance equally for prevention purposes. Whereas, social distancing rule and mask-wearing were reported as impracticable by 55.8% and 44.2%, respectively.
Conclusion: 94.2% of HCWs had a good level of knowledge about COVID-19; in contrast, lack of preventive practice was observed. This implies that there is a gap between knowledge and implementation of preventive measures toward the disease.
Keywords: COVID-19, knowledge, practice, HCWs, DPH, Ethiopia
Introduction
A novel coronavirus (2019-nCoV) associated with human to human transmission and severe human infection has been reported since late December 2019 from Wuhan city, Hubei province in China.1,2 Researchers have detected SARS-CoV-2 on surfaces of objects in a symptomatic patient’s room and toilet area.3 Thus, a high fatality rate and rapid spread of the viruses from China to the world have attracted and diverted the intention of communities worldwide. Consequently, due to its worldwide spread and subsequent crisis, on February 11, 2020, and March 11, 2020 World Health Organization (WHO) named the disease caused by SARS-CoV-2 “COVID-19” and declared a pandemic.4–6 The extremely fast transmission capability of SARS-CoV-2 has aroused concern about its various transmission routes.5,7,8 Knowing the extent of environmental contamination of SARS-CoV-2 is critical for improving safety practices for HCWs and answering questions about SARS-CoV-2 transmission among the public.9 The ongoing capacity of viral spill-over from animals causing serious disease in humans has been demonstrated in this pandemic outbreak.10 It implies the need for close monitoring to find, isolate, test and treat every case, to break the chains of transmission routes through the population as well as in dental clinics and hospitals.10,11
From day one up to January 01, 2021, official figures released by the World Health Organization (WHO) at a glance, indicate over 84 million confirmed cases of COVID-19 worldwide with greater than 1.8 million death toll. Taking this a step further, from the total global confirmed cases, Africa accounts for >1.1 million confirmed COVID-19 cases and >24,000.00 deaths have been reported.14 In sub-Saharan Africa, Ethiopia has also been hit by this pandemic and the number of confirmed COVID-19 cases is increasing every single day. According to the Federal Ministry of Health and Ethiopia’s integrated COVID-19 control system, the present figure, ie, until first January 2021, is more than 124,000 confirmed cases of COVID-19, with more than 112,000 recovered and more than 1900 associated death toll. The current national statistics of COVID-19 indicates that the spread of the virus initially increased very slowly but is currently increasing at an alarming rate from the first confirmed COVID-19 case of Japanese citizens who came from Japan to Ethiopia (March 13, 2020). It is globally known that this newly emerged virus negatively affects not only human life and socio-economics but also the healthcare system. The pandemic primarily challenges the healthcare systems in almost every country around the world.16 The Ethiopian healthcare system faces a shortage of medical supplies such as personal protective equipment like face-covering masks and medical equipment like ventilators, and rapid diagnostic kits. HCWs are not only at the forefront of the fight against this highly contagious infectious disease but are also directly or indirectly affected by it and the likelihood of acquiring this disease is higher as compared to the general population. Most scholars assumed and believed that HCWs have sufficient knowledge and good prevention practice toward COVID-19.19
The eradication of COVID-19 appears to be virtually impossible, however, with a great trial and efforts of researchers, WHO on Thursday approved the Pfizer-BioNTech coronavirus vaccine for emergency use, a move aimed at helping the developing world gain access to the vaccine sooner.20 Besides this, a COVID-19 vaccine target product profile must address vaccinating at-risk human populations including frontline healthcare workers, individuals over the age of 60, and those with underlying and debilitating chronic conditions.21 Therefore, based on the WHO and CDC report, understanding its clear mode of transmission and taking appropriate preventive measures are the most essential and life-saving strategies for controlling the disease.22 Taking this a step further, to flatten the curve of the spread of SARS-CoV-2, ie, social isolation, appropriate face mask usage, following rules of social distancing, avoidance of “3C” (Closed, Crowded or involving Close contact),23 and proper hand washing practice or sanitization are among the most frequently recommended intervention measures.24,25 Hence, HCWs are at the forefront of infection prevention, and they are potentially at risk of getting the disease.26 Therefore, all possible actions must be taken to control the spread of the infection to HCWs. Currently, quarantine areas in Ethiopia are already occupied; transmission of the disease among HCWs is associated with overcrowding, absence of isolation room facilities. So far a multi-centric study showed that HCWs have adequate awareness about the multiple modes of viral transmission as well as infection prevention practices. However, particularly in Ethiopia, the healthcare system is dilapidated and very weak, due to politically assigned hospital administration and expanded corruption. Thus, from time to time, the government’s declining attention to the pandemic results in negligence and exhaustion of HCWs regarding containment of the pandemic.27,28 Scientific scholars suggest that if there is poor knowledge and practice toward a new epidemic disease, it will become worse and transform into the pandemic range.29,30 In order to achieve success against the spread of COVID-19, assessment of the awareness of HCWs and their practice is very important.7,8 Taken together, this research focused on understanding the current knowledge toward the pandemic and on evaluating HCWs’ practices to tackle the virus, avoid being infected, and protecting others at district primary hospital level.
Materials and Methods
Study Area, Design, and Period
The study was conducted in Takusa Woreda, Delghi Primary Hospital, which is located on the northwestern shore of Lake Tana, 152 km from Gondar town, Ethiopia. The hospital serves more than 1.5 million people who reside in Takusa Woreda and other neighboring woreda. The hospital has 68 beds and 4 wards for inpatients, emergency, surgery, and outpatient department (OPD). An institutional-based descriptive cross-sectional study from August to September 2020 G.C was conducted.
Source Population, Inclusion and Exclusion Criteria
All professional HCWs at DPH were included during the study period; while non-professionals (including cleaners), professionals who were not in the workplace or not willing to participate, and administrative staff who worked in the hospital were not included in this study.
Study Variables
Knowledge and practices toward COVID-19 disease were dependent variables; whereas socio-demographic details which included sex, age, religion, marital status, and profession were independent variables.
Operational Definition
HCWs: all people engaged in activities whose primary intention is to improve the quality of health.31 For the purpose of this study, all active and voluntary health professionals who work at DPH were enrolled. These included nurses, laboratory experts, midwives, medical doctors, environmental public health officers, health officers, and an anesthesiologist.
Knowledge was defined as having an adequate understanding of COVID-19.
Good knowledge: when the respondent answered or scored ≥ 8 of 15 knowledge assessment questions (≥53.3%).
Poor knowledge: when the respondent answered or scored < 8 of 15 knowledge assessment questions (<53.3%).
Practice was defined as an act of performing given procedure(s) according to a set standard of WHO and CDC.
Good practice: when respondent answered or scored ≥ 7 of 14 practice assessment questions (≥50%).
Poor practice: when respondent answered or scored < 7 of 14 practice assessment questions (<50%).
Sample Size and Sampling Methods
The total number of HCWs in this study was estimated to be around 112. The total number of willing participants and respondents in this study was 104 HCWs. Non-probability convenience sampling method was used in this study using a structured questionnaire to collect data from participants. This reflects a sample of HCWs that is proportionate to the number of HCWs within the district primary hospital in North West Gondar, Ethiopia.
Data Collection Tool
We used a questionnaire adapted from different current and past literature.32–39 Thus, all relevant data were collected by a pre-oriented and trained data collector at the DPH. The questionnaire covers socio-demographics, mediainformation about COVID-19, knowledge, and practice (KP) regarding COVID-19. The questionnaires regarding the assessment of knowledge regarding COVID-19 had 15 questions with Likert-type scale options such as likely, unlikely, and I do not know. The correct answer for each question scored one point and if incorrect zero points. Likewise, an assessment regarding their practices toward COVID-19 was composed of 14 questions and participants responded with Likert-type scale options ranging from always to never. Similar to knowledge score, the practices were assessed and scored one point for each question which was correctly answered, and zero for incorrect answers. Taken together, regarding both knowledge and practice, those who scored above the total average of the knowledge and practice question were considered as “good”, whereas, below the average value were labeled as “poor”, respectively. The questionnaire and the collected data were reviewed daily and coded before analysis for clarification, and completeness based on the pre-test.
Pilot Study
Pre-test phase was conducted to assess the validity and reliability of the questionnaire and confirmed by a pilot study on ten HCWs who worked nearby at primary Hospital, Kolladeba primary Hospital, in North West Gondar. Based on the pre-test, proper modifications were completed before the actual data collection and analysis commenced at DPH.
Data Processing and Analysis
After the data were collected, analysis was performed by using International Business Machines Corporation, Statistical Package for the Social Sciences (IBM SPSS) version 20. Descriptive analysis was done. Frequency distribution and percentage were used to describe data on knowledge as well as practice related to the pandemic. Data were presented in the form of tables and figure. The Pearson’s Chi-squared test was utilized to assess the either socio-demographic variables and source of information had an association with both knowledge and practice toward COVID-19. P-value < 0.05 was considered to be statistically significant. However, because we did not find any association and the survey had a limited sample size, we did not analyze both binary and multiple logistic regression.
Results
Socio-Demographic Characteristics of the Study Participants
Among a total of 104 HCWs, 71 (68.3%) were male and 33 (31.7%) were female. The mean age of respondents was 30±5 years and ranged from 20 to 50 years (median age of 28). From the total of 104 interviewed HCWs, most of the participants, 94 (90.4%), were Orthodox followed by Muslim which accounted for 8 (7.7%). Regarding the profession of the study participants, 38 (35.7%), 20 (19.2%), 14 (13.5%), and 13 (12.5%) of the respondents were nurses, midwives, medical doctors, and pharmacists, respectively. Based on their marital status both married and unmarried were equivalent. However, only 3 (2.9%) were divorced (Table 1).
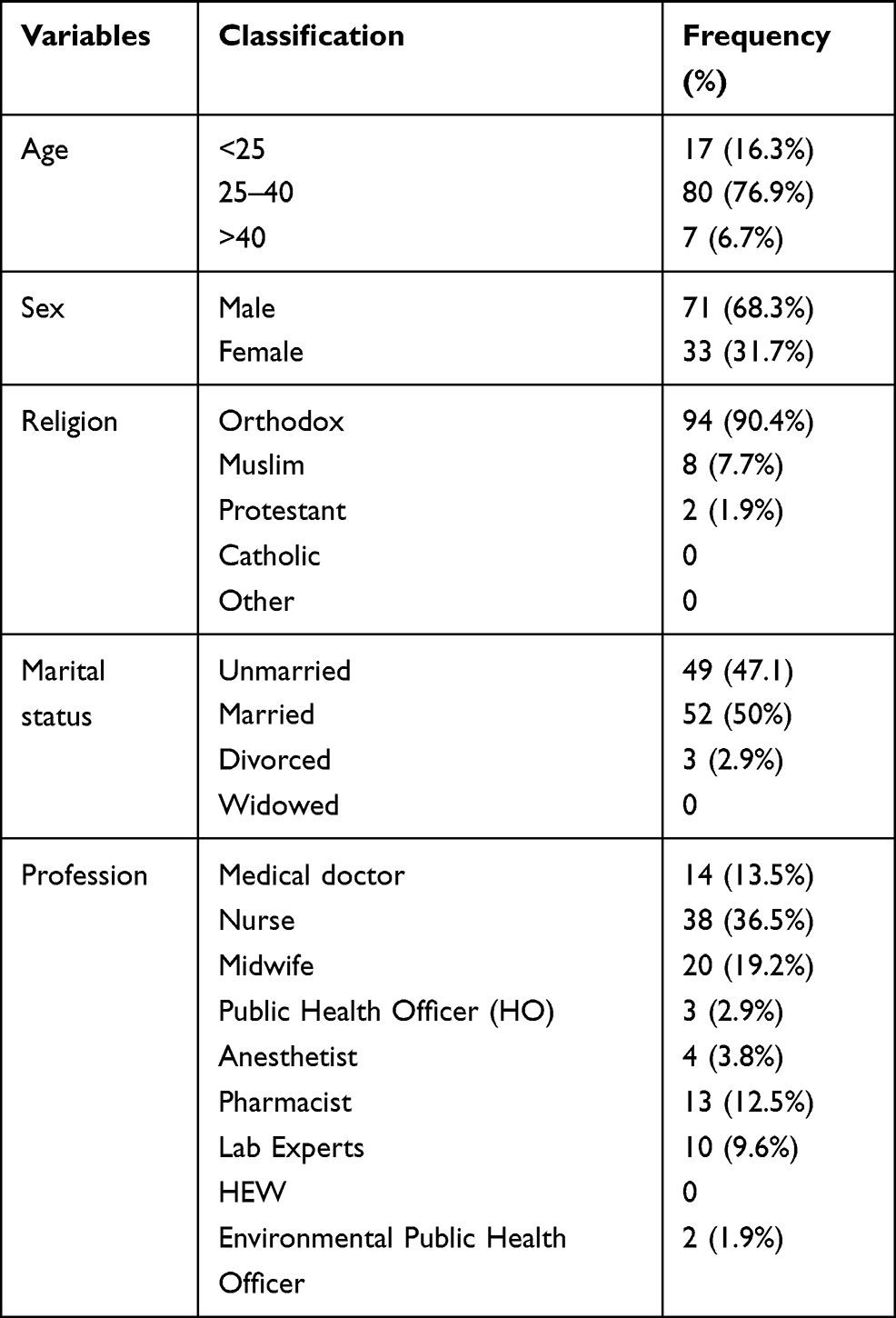 |
Table 1 Socio-Demographic Characteristics of Participants - HCWs, Delghi Primary Hospital, Northwest Ethiopia, 2020 (N=104) |
Source of Information About COVID-19 Among the Study Participants
Originally, knowledge about the pandemic was measured from various information sources with different preference as well as availability or access to the source of the information. This finding demonstrates that HCWs obtained information about this pandemic from social media such as Facebook, telegram, which comprised 45.2% followed by different television programs like ETV, BBC, and CNN comprising 35.6% (Figure 1). Of the total social media users, 93.3% of HCWs used it most frequently, and sometimes, whereas only 6.7% never used social media as a source of information. Similarly, Google search engine accounted for 27.9% as source of information regarding COVID-19 among HCWs. Of the total Google search users, 59.6% used it sometimes, but 12.5% of the participants never used it. Very surprisingly, only 7.7% of the participants used international journals like dove medical press or nature frequently as a source of information.
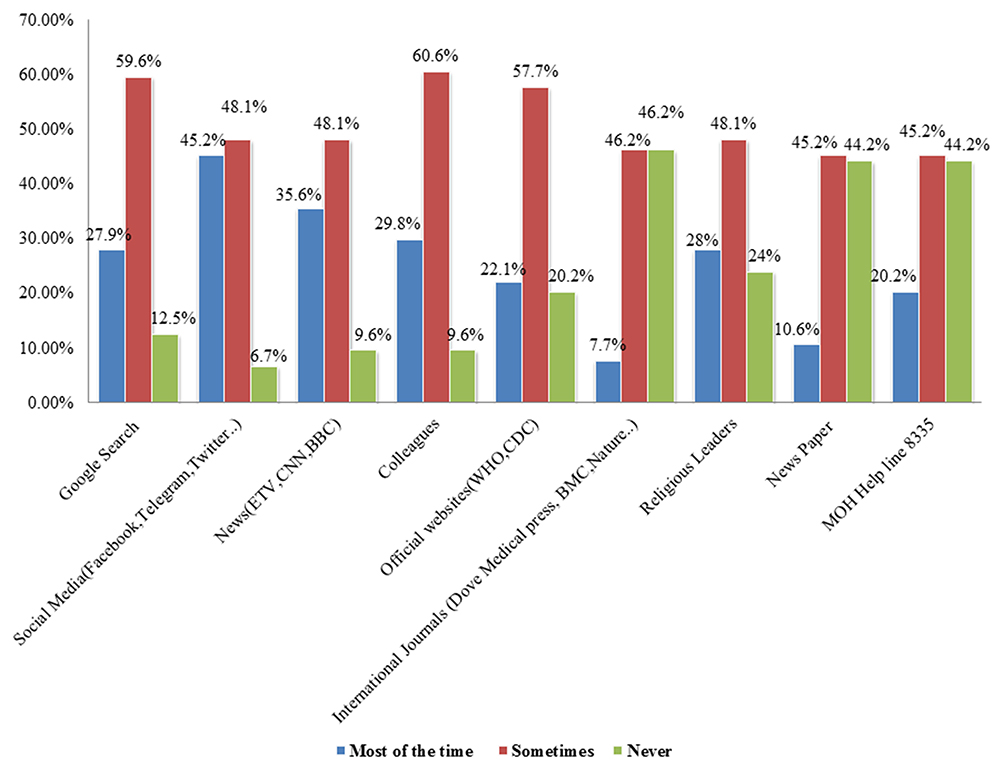 |
Figure 1 The most common sources of information related to COVID-19 among HCWs. The X axis: source of information about COVID and Y-axis: the frequency in percent. |
Knowledge of HCWs on COVID-19 Modes of Transmission
The present study also demonstrates the level of participants’ knowledge regarding mode of transmission and at-risk groups of the population regarding COVID-19. The result showed more than 50% of HCWs recognized that humans can get the virus from animal contact and contaminated food. On the other hand, greater than 90% of HCWs were aware that the novel corona virus can be transmitted through either inhalation from the nearby infected individuals with sneezing droplets, or physical contact, and hand shaking. Moreover, 87.5% of HCWs thought that this virus was transmissible and considered as airborne disease and kissing equally. Furthermore, HCWs suggested that the virus was not transmitted vertically from mother to fetus via placenta (51%), or mother to child via breast feeding (58.7%), sexual contact (40.4%) and feco-oral route (33.7%) (Table 2). Regarding risk factor assessment, majority of HCWs (>94%) assumed individuals with asthma, COPD, and hypertension (HTN) were more likely at risk of case fatality of the disease. In addition, more than 70% of the participants recognized that pregnant women and children were more susceptible to COVID-19.
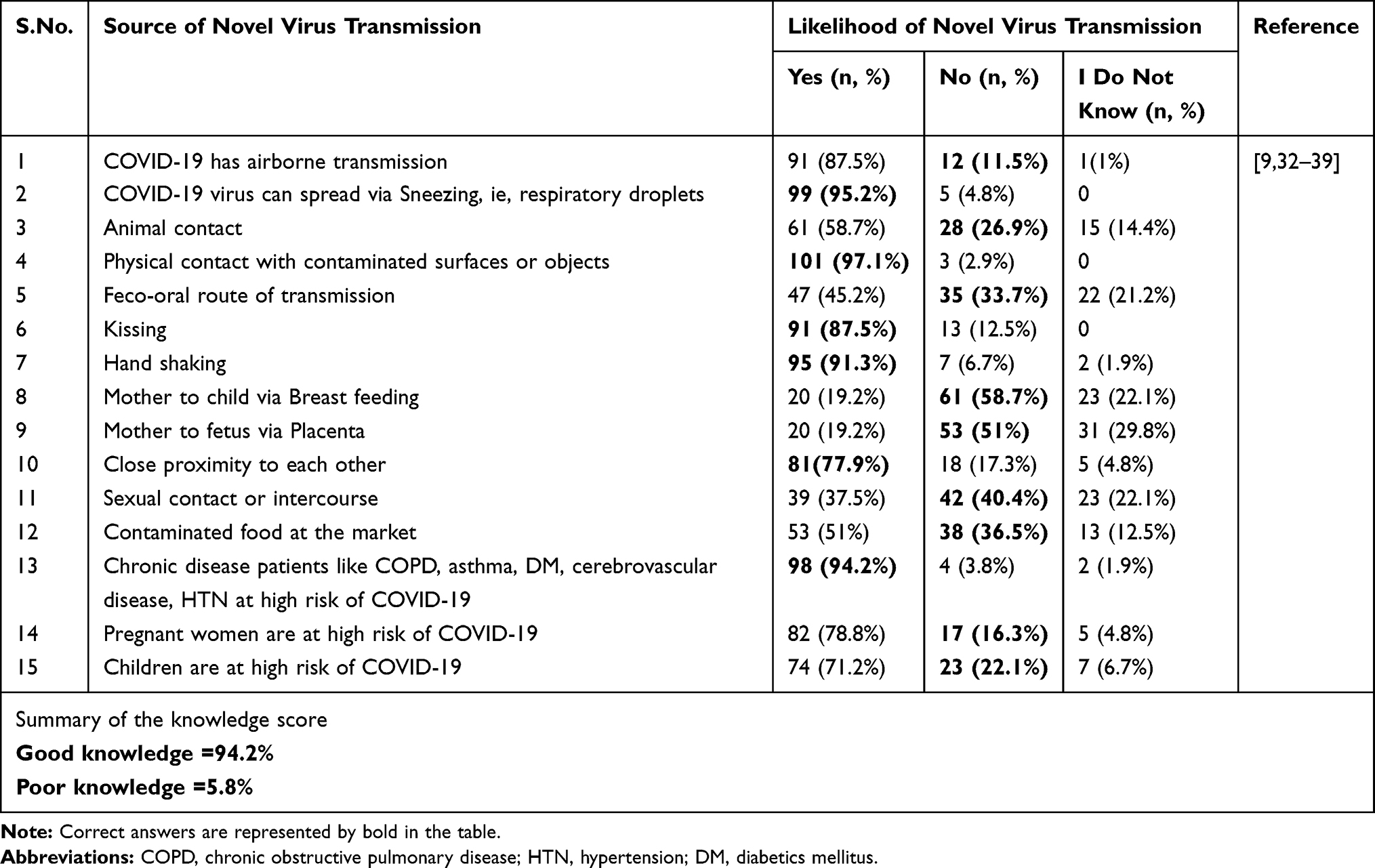 |
Table 2 Knowledge on the Potential Mode of Transmission and At-Risk Groups of COVID-19 Among the Study Participants at Delghi Primary Hospital Northwest Ethiopia, 2020. (N=104) |
COVID-19 Prevention Practice of Study Participants
This study also assessed the HCWs who used the types of preventive measures recommended by WHO or CDC to protect themselves or others from SARS-CoV-2. More than 50% of the HCWsalways practiced wearing surgical masks and avoiding hand to nose, eye and mouth contact. They also used hand sanitizer and avoided hand shaking while greeting friends with an equal proportion (64.4%). Surprisingly, around 11.5% never wore face covering masks even in hospital setup. However, more than 70.0% of the HCWs always wore surgical mask and used elbow cover while sneezing. Moreover, 44.2% of the participants frequently maintained the social distancing rule and avoided crowded areas (45%) where probability of getting the virus is high. However, greater than 45% of HCWs sometimes did not respectsocial distancing rule and visited crowded places during the pandemic (Table 3).
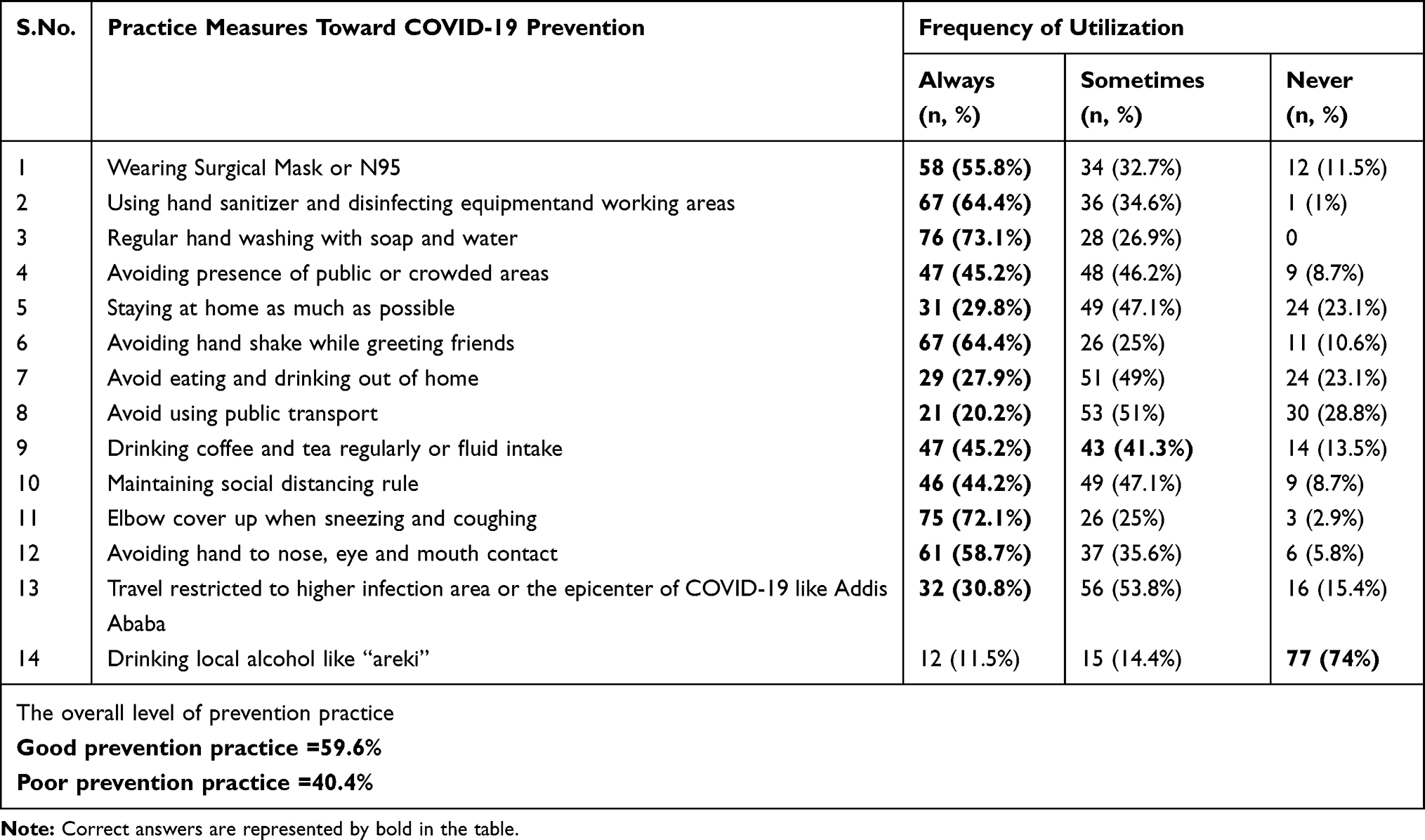 |
Table 3 Precautionary Measures Adopted by the HCWs in the Fight Against COVID-19 at Delghi Primary Hospital, 2020 (N=104) |
Discussion
In this study, out of 104 HCWs or health professionals, 94.2% had good levels of knowledge, which implies that the average knowledge score of the participants was 10.45 (SD=1.9, range 2–14) regarding transmission methods of the virus, and vulnerable or at-risk groups of the community. This knowledge score was comparatively higher than that of previously published articles from China (90%),33 Kenya (88%),32 Ethiopia (73.8%)35 (88.2%)34 and Egypt (80.4%).19 Another Chinese research study showed that 88% of the healthcare staff were aware of COVID-19 (knowledge score: 8.17 ± 1.30), which was again lower than the current study.40 The possible reason for the increment of knowledge is due to the accessibility of the information with different media sources in Ethiopia; telecommunication has a default mobile phone sound message during calls about COVID-19 transmission and prevention measures.15 Despite this, individuals with respiratory disorders are more at risk of developing the disease. This may be due to the respiratory microbiome, which contributes to the host’s local immune education and to the development of respiratory diseases, including allergies, asthma and others.41 Their understanding related to at-risk groups of the population, 94.2% of HCWs believed that individuals with asthma or chronic obstructive pulmonary disease and hypertension were at higher risk of morbidity and mortality associated with COVID-19. This finding was in agreement with previously conducted studies in Vietnam (79.2%).40 Therefore, HCWs in different hospitals as well as healthcare system should be very conscious of patients with asthma, COPD, and other chronic diseases since those multi-morbidity patients are associated with highest hospital admission and case fatality rate with severe course of COVID‐19.42 Thus, we need to increase adequate understanding of participants from time to time about this pandemic. About 40.4% of the participants had poor prevention practice to tackle the pandemic in this study. As compared to the current study, a previous research article in Ethiopia showed a relatively lower level of knowledge (88.2%) with higher level of practice (63.5%) toward COVID-19.34 Similarly, in Zambia about 84.1% and 75% of the study participants had good knowledge, and good practice toward COVID-19 respectively.43 On the other hand, particularly for prevention practice, the current study is relatively higher than research done in NW Ethiopia, Gondar (38.73%).44,45 This difference may be due to the fact that this study was conducted in a single district primary hospital with limited number of study participants, whereas previously conducted research was in general hospital, teaching hospital, multicenter institution and large sample size. Moreover, due to the time gap, ie, participants’ awareness about COVID-19 increasing from first day of confirmed case (March to May 2020) to October 2020. Regarding the main source of information of the participants to get information related to this novel virus, it was revealed that except for 6.7% of participants who never used social media, 93.3% of HCWs used social media either “mostly” or “sometimes” as primary source of information followed by their colleagues (90.4%). In fact, this finding is lower than that of a study conducted in Ethiopian34 HCWs where social media was a major information source for COVID-19. In contrary, previous studies in Ethiopia35 showed that News media (82.8%) and social media (64%); United Arab Emirates,39 social media (61%), news media like TV (60%), and friends (31%) were the major sources of information related to COVID-19. The possible reason for the discrepancy of such result might be due to the fact that this study was only single institute based with limited sample size as well as limited facilities whereas the previous one was done in a multicenter hospital or more than three intuitions with large sample size. This should alert policy makers to the importance of social media in disseminating information to the public, especially in cases of pandemics. We also found that official sites such as the CDC, WHO website, newspaper and international journal like Dove medical press, BMC, or Nature which should reflect reliable sources of information, were less commonly used than social media (Facebook, Telegram, Twitter …) and news channels such as ETV, BBC, and CNN to obtain information.
All the professionals on duty have to take protective measures in order not to infect themselves and their patients. Evidence shows that dentists, but also dental hygienists and dental assistants are potentially exposed to a high degree of contamination with SARS-CoV-2 virus during treatments that generate aerosols by using different devices, as airways-oral cavity, nostrils, and eye conjunctiva are the access routes of SARS-CoV-2.11 The present study demonstrated that more than half of the respondent HCWs showed good prevention practice against COVID-19. Approximately59.6% of the HCWs protected themselves and others from being infected with COVID-19 through wearing masks, frequent hand washing, using hand sanitizer, restricting travel,avoiding 3C or “zero C”, staying at home as much as possible and avoiding touching nose, eyes, and mouth, which was lower than studies reported from China (94%).33 The current practices toward COVID-19 were again lower than the practice of other countries including China, USA.33,39 Even though the majority of study participants had good knowledge of COVID-19, only 59.6% of the participants had good prevention practice. Maintaining of social distancing, hand hygiene and mask-wearing, as practiced in many countries, has proven to be effective to reduce the spread of COVID-19. Parallel to a study in Nigeria,27 social distancing (55.8%) and mask-wearing (44.2%) were not fully practicable. The possible reason for such poor practice was due to the type of HCWs or negligence of individual participants toward prevention practice, frequency of exposure, burden of the virus on that specific geographic area, frontline or non-frontline status of HCWs. Moreover, other factors such as availability of personal protective equipment (PPE) or PPE supply, water and soap supply to primary hospital were almost negligible. Apart from this, the existing “pandemic” scenario requires solid and reliable diagnostic tests in order to proceed with the required decision making and limiting the spread of this COVID-19 outbreak.
Limitations of the Study
The study design was institutional based cross-sectional, therefore causal modeling could not be attempted. Since the study took information at specified time-points, cause and effect association could not be studied. The other limitation was lack of sufficient similar study; which limits comparison with other studies. However, identifying knowledge gaps and practice can be used to develop effective and timely interventions. Moreover, the survey was conducted in only one district primary hospital in North West Gondar, Ethiopia so the results may not be generalizable to other hospital HCWs. Furthermore, the measurement of KP may be imprecise due to the limited number of study participants. Further study is needed with expanded sample size.
Conclusion
The findings of the present study suggested that the majority of the study participants at DPH have good knowledge; nevertheless, they have poor practice toward COVID-19. Since preventive practice is a critical step and measurement of COVID-19 control, maximum attention should be given to improving preventive measure practice toward COVID-19 by the responsible body and hospital administration. Therefore, in order to bring their knowledge into practice, multidisciplinary training, frequent education intervention platform, and campaigns with special emphasis on COVID-19 preventive measures are needed for HCWs.
Abbreviations
BBC, British Broadcasting Corporation; CDC, Communicable Disease Control; CNN, cable news network; COPD, chronic obstructive pulmonary disease; COVID-19, coronavirus disease 2019; ETV, Ethiopia television; DPH, Delghi Primary Hospital; DM, diabetes mellitus; HCWs, healthcare workers; HEW, health extension worker; HTN, hypertension; KP, knowledge and practice; PPE, personal protective equipment; SARS-CoV-2, severe acute respiratory syndrome coronavirus; WHO, World Health Organization.
Ethical Approval
The study was approved by Delghi Primary Hospital ethics committee and administrative office for this institutional based survey about current knowledge and prevention practice experience of HCWs from prior to data collection (Ref. No DPH/342/2020). Furthermore, the study was conducted in accordance with the Declaration of Helsinki. Objective of the study was clearly explained to participants via email with the help of hospital administrative office before conducting the interview and verbal informed consent was obtained from each participant. All participants signed a written informed consent. Data were taken anonymously and kept confidential throughout the study period and kept locked in a cabinet.
Acknowledgments
We are very glad to acknowledge Delghi primary hospital for ethical approval. Special thanks to the hospital administration for material support such as duplication of questionnaires and facilitating the data collection process. We would like to thank all respondents for their willingness to participate in this study.
Author Contributions
All authors made a significant contribution to the work reported, whether in conception, study design, execution, acquisition of data, analysis, interpretation, or all those areas; took part in drafting, revising, or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was not funded by any of governmental or nongovernmental funders.
Disclosure
The authors report no conflicts of interest for this work.
References
1. Rothe C, Schunk M, Sothmann P, et al. Transmission of 2019-nCoV infection from an asymptomatic contact in Germany. N Engl J Med. 2020;382(10):970–971. doi:10.1056/NEJMc2001468
2. Hui DS, I Azhar E, Madani TA, et al. The continuing 2019-nCoV epidemic threat of novel coronaviruses to global health—The latest 2019 novel coronavirus outbreak in Wuhan, China. Int J Infect Dis. 2020;91:264–266. doi:10.1016/j.ijid.2020.01.009
3. Ong SWX, Tan YK, Chia PY, et al. Air, surface environmental, and personal protective equipment contamination by severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) from a symptomatic patient. JAMA. 2020;323(16):1610–1612. doi:10.1001/jama.2020.3227
4. Wang C, Horby PW, Hayden FG, et al. A novel coronavirus outbreak of global health concern. Lancet. 2020.
5. Guo Z-D, Wang Z-Y, Zhang S-F, et al. Aerosol and surface distribution of severe acute respiratory syndrome coronavirus 2 in hospital wards, Wuhan, China, 2020. Emerg Infect Dis. 2020;26(7):10–3201. doi:10.3201/eid2607.200885
6. Rothan HA, Byrareddy SN. The epidemiology and pathogenesis of coronavirus disease (COVID-19) outbreak. J Autoimmun. 2020;109:102433. doi:10.1016/j.jaut.2020.102433
7. Peng X, Xu X, Li Y, et al. Transmission routes of 2019-nCoV and controls in dental practice. Int J Oral Sci. 2020;12(1):1–6. doi:10.1038/s41368-020-0075-9
8. Zheng J. SARS-CoV-2: an emerging coronavirus that causes a global threat. Int J Biol Sci. 2020;16(10):1678. doi:10.7150/ijbs.45053
9. Charitos IA, Ballini A, Bottalico L, et al. Special features of SARS-CoV-2 in daily practice. World J Clin Cases. 2020;8(18):3920. doi:10.12998/wjcc.v8.i18.3920
10. Cantore S, Ballini A. Coronavirus disease 2019 (COVID-19) pandemic burst and its relevant consequences in dental practice. Open Dent J. 2020;14:111–112. doi:10.2174/1874210602014010111
11. Bordea IR, Xhajanka E, Candrea S, et al. Coronavirus (SARS-CoV-2) pandemic: future challenges for dental practitioners. Microorganisms. 2020;8(11):1704. doi:10.3390/microorganisms8111704
12. Zignol M, Dean AS, Falzon D, et al. Twenty years of global surveillance of antituberculosis-drug resistance. N Engl J Med. 2016;375(11):1081–1089. doi:10.1056/NEJMsr1512438
13. Baye K. COVID-19 prevention measures in Ethiopia: current realities and prospects. Intl Food Policy Res Inst. 2020.
14. Wu R, Wang L, Kuo H-CD, et al. An update on current therapeutic drugs treating COVID-19. Curr Pharmacol Rep. 2020:1. doi:10.1007/s40495-020-00216-7
15. Wahed WYA, Hefzy EM, Ahmed MI, et al. Assessment of knowledge, attitudes, and perception of health care workers regarding COVID-19, a cross-sectional study from Egypt. J Community Health. 2020;45:1–10. doi:10.1007/s10900-019-00710-0
16. WHO. 2020. Available from: https://wwwvoanewscom/covid-19-pandemic/who-approves-emergency-use-pfizer-vaccine.
17. Chen W-H, Strych U, Hotez PJ, et al. The SARS-CoV-2 vaccine pipeline: an overview. Curr Trop Med Rep. 2020:1–4. doi:10.1007/s40475-020-00201-6
18. Baloch S, Baloch MA, Zheng T, et al. The coronavirus disease 2019 (COVID-19) pandemic. Tohoku J Exp Med. 2020;250(4):271–278. doi:10.1620/tjem.250.271
19. Shimizu K, Wharton G, Sakamoto H, et al. Resurgence of covid-19 in Japan. Br Med J. 2020:m3221. doi:10.1136/bmj.m3221
20. Organization WH. Coronavirus disease (COVID-19) advice for the public: myth busters. 2020.
21. Matthews J. “Cultural exceptionalism” in the global exchange of (mis) information around Japan’s responses to Covid-19. Media Commun. 2020;8(2):448–451.
22. Ran L, Chen X, Wang Y, et al. Risk factors of healthcare workers with corona virus disease 2019: a retrospective cohort study in a designated hospital of Wuhan in China. Clin Infect Dis. 2020;71(16):2218–2221. doi:10.1093/cid/ciaa287
23. Anyanwu MU, Festus IJ, Nwobi OC, et al. A perspective on Nigeria’s preparedness, response and challenges to mitigating the spread of COVID-19. Challenges. 2020;11(2):22. doi:10.3390/challe11020022
24. Lewis S, Mulla F. Diagnostic radiographers’ experience of COVID-19, gauteng south africa. Radiography. 2020. doi:10.1016/j.radi.2020.09.009
25. Shilpa K, Kumar BP, Kumar SY, et al. A study on awareness regarding swine flu (influenza A H1N1) pandemic in an urban community of Karnataka. Med J Dr DY Patil Univ. 2014;7(6):732. doi:10.4103/0975-2870.144862
26. Alkot M, Albouq MA, Shakuri MA, et al. Knowledge, attitude, and practice toward MERS-CoV among primary health-care workers in Makkah Al-Mukarramah: an intervention study. Int J Med Sci Public Health. 2016;5(5):952–959. doi:10.5455/ijmsph.2016.24012016345
27. Organization WH. The world health report 2006: working together for health. World Health Organization; 2006.
28. Austrian K, Pinchoff J, Tidwell JB, et al. COVID-19 related knowledge, attitudes, practices and needs of households in informal settlements in Nairobi, Kenya. 2020.
29. Zhong B-L, Luo W, Li H-M, et al. Knowledge, attitudes, and practices towards COVID-19 among Chinese residents during the rapid rise period of the COVID-19 outbreak: a quick online cross-sectional survey. Int J Biol Sci. 2020;16(10):1745. doi:10.7150/ijbs.45221
30. Jemal B, Ferede ZA, Mola S, et al. Knowledge, attitude and practice of healthcare workers towards COVID-19 and its prevention in Ethiopia: a multicenter study. 2020.
31. Kassie BA, Adane A, Tilahun YT, et al. Knowledge and attitude towards COVID-19 and associated factors among health care providers in Northwest Ethiopia. PLoS One. 2020;15(8):e0238415. doi:10.1371/journal.pone.0238415
32. Azlan AA, Hamzah MR, Sern TJ, et al. Public knowledge, attitudes and practices towards COVID-19: a cross-sectional study in Malaysia. PLoS One. 2020;15(5):e0233668. doi:10.1371/journal.pone.0233668
33. Khasawneh AI, Humeidan AA, Alsulaiman JW, et al. Medical students and COVID-19: knowledge, attitudes, and precautionary measures. A descriptive study from Jordan. Front Public Health. 2020;8. doi:10.3389/fpubh.2020.00253
34. Olum R, Chekwech G, Wekha G, et al. Coronavirus disease-2019: knowledge, attitude, and practices of health care workers at Makerere University Teaching Hospitals, Uganda. Front Public Health. 2020;8:181. doi:10.3389/fpubh.2020.00181
35. Bhagavathula AS, Aldhaleei WA, Rahmani J, et al. Novel coronavirus (COVID-19) knowledge and perceptions: a survey on healthcare workers. MedRxiv. 2020.
36. Huynh G, Nguyen TNH, Vo KN, et al. Knowledge and attitude toward COVID-19 among healthcare workers at District 2 Hospital, Ho Chi Minh City. Asian Pac J Trop Med. 2020;13(6):260. doi:10.4103/1995-7645.280396
37. Santacroce L, Charitos IA, Ballini A, et al. The human respiratory system and its microbiome at a glimpse. Biology. 2020;9(10):318. doi:10.3390/biology9100318
38. Sokolowska M, Lukasik ZM, Agache I, et al. Immunology of COVID‐19: mechanisms, clinical outcome, diagnostics, and perspectives—a report of the European Academy of Allergy and Clinical Immunology (EAACI). Allergy. 2020;75(10):2445–2476. doi:10.1111/all.14462
39. Chawe A, Mfune RL, Syapiila P, et al. Knowledge, attitudes and practices of COVID 19 among medical laboratory professionals in Zambia. medRxiv. 2020.
40. Kassie BA, Adane A, Abebe Kassahun E, et al. Poor COVID-19 preventive practice among healthcare workers in Northwest Ethiopia, 2020. Adv Public Health. 2020;2020:1–7. doi:10.1155/2020/7526037
41. Akalu Y, Ayelign B, Molla MD. Knowledge, attitude and practice towards COVID-19 among chronic disease patients at Addis Zemen Hospital, Northwest Ethiopia. Infect Drug Resist. 2020;13:1949. doi:10.2147/IDR.S258736
42. Zhou M, Tang F, Wang Y, et al. Knowledge, attitude and practice regarding COVID-19 among health care workers in Henan, China. J Hosp Infect. 2020.
43. Clements JM. Knowledge and behaviors toward COVID-19 among US residents during the early days of the pandemic: cross-sectional online questionnaire. JMIR Public Health Surveillance. 2020;6(2):e19161. doi:10.2196/19161
44. Kwok KO, Li KK, Chan HH, et al. Community responses during the early phase of the COVID-19 epidemic in Hong Kong: risk perception, information exposure and preventive measures. MedRxiv. 2020.
45. Pham V, Nguyen K, Le S, et al. Rapid and sensitive diagnostic procedure for multiple detection of pandemic Coronaviridae family members SARS-CoV-2, SARS-CoV, MERS-CoV and HCoV: a translational research and cooperation between the Phan Chau Trinh University in Vietnam and University of Bari” Aldo Moro” in Italy. Eur Rev Med Pharmacol Sci. 2020;24(12):7173–7191. doi:10.26355/eurrev_202006_21713
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.