")
Back to Journals » Journal of Multidisciplinary Healthcare » Volume 14
Knowledge and Practice of Health Care Providers Towards Proper Face Mask Utilization to Minimize the Extent of COVID-19 Infection in Amhara Region Referral Hospitals, Ethiopia
Authors Seid Yimer T, Gebrehana Belay H
Received 10 May 2021
Accepted for publication 15 June 2021
Published 28 June 2021 Volume 2021:14 Pages 1583—1591
DOI https://doi.org/10.2147/JMDH.S306253
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Scott Fraser
Tigist Seid Yimer, Habtamu Gebrehana Belay
Department of Midwifery, College of Health Sciences, Debre Tabor University, Debre Tabor, Ethiopia
Correspondence: Tigist Seid Yimer Tel +251921430801
Email [email protected]
Introduction: The novel coronavirus disease (COVID-19) pandemic began in early 2020, causing tens of thousands of deaths, over a million cases, and widespread socioeconomic disruption.
Objective: The aim of the study was to assess health care workers’ knowledge and practice of proper face mask utilization to prevent the spread of COVID-19 infection in Amhara region referral hospitals, Ethiopia.
Methods: A cross-sectional institutional-based quantitative study design was conducted from May 15 to 30/2020 using pre-tested self-administrated questionnaire and analyzed by using SPSS version 20.0. The study included 422 health care providers, and the sample size was determined using a single population proportion formula with the assumption of a p value of 0.05. Data were collected using a consecutive sampling technique from all referral hospitals and were analyzed using descriptive statistics. Finally, the outcome was presented in the form of a text and a table.
Results: The overall knowledge and practice of health care providers regarding proper face mask utilization were 278 (65.8%) and 252 (59.5%), respectively. Of them, 284 (67.3%) knew that face masks were worn with the white side facing in, 264 (62.6%) knew that face masks had three layers, and 331 (78.4%) knew that surgical face masks were worn for up to 8 hours.
Conclusion and Recommendation: The respondent’s knowledge of proper face mask usage was high, in comparison with another studies but the proper utilization of face mask was relatively low. Ethiopian ministry of health in collaboration with Amhara region, zonal and woreda health institution works together to increase utilization of face mask and to alleviate scarcity of resource and provide training to the health care providers about the proper utilization of face mask to tackle COVID-19.
Keywords: knowledge, practice, proper face mask utilization, health care workers, COVID-19
Introduction
Coronavirus is still a communicable disease that has been exacerbated by a newly discovered coronavirus. It started in China in December 2019, and it is still a major public health issue around the world.1 Coronavirus infection is a highly communicable infection that threatens the lives of over 15 million people worldwide.2
The rapid spread of the virus has raised concerns that healthcare systems will lack sufficient resources and will be unable to cope with the issue of receiving COVID-19 patients, resulting in dramatically increased illness and death. It is critical to gain a better understanding of the efficacy of potential interferences in order to limit the spread of the disease, especially in the case of the setting supply limit. Many nations have imposed worldwide and national travel restrictions, closed universities and non-essential trades, and sharply restricted community gatherings in order to avoid irresistible nationwide health care capitals and relieve the weight of contagion.3 Coronavirus is spread primarily through airborne transmission and close contact with infected people. The World Health Organization and the Centers for Disease Control and Prevention (CDC) have developed new methods to combat the spread of COVID-19 infection. The virus has infected 3019 health care workers (HCWs) as of February 21, 2020, resulting in five morbidities.4
Many defensive activities are designed to reduce person-to-person interaction, lowering the successful replication number and, as a result, the spread degree. On an individual level, behavioral factors such as social distancing, self-isolation when symptomatic, hand washing, sanitizing surfaces, and following a clean protocol anywhere coughing and sneezing will help to reduce transmission. These interventions may provide protection (a lower risk of infection) to susceptible individuals as well as a lower risk of disease transmission to diseased people.5,6 WHO and CDC dose also not included covering of hair and wearing shoes,7 but study shows that covering of hair and shoes can prevent the spread of COVID-19 and other nosocomial infections.8 Face masks are required everywhere in the world for both healthy and symptomatic people in crowded public places.9 According to an Ethiopian ministry of health report, more than 100 health care workers were infected with coronaviruses within two weeks; this number may rise over time. Due to their close contact with patients, health care workers are at a higher risk.10 To reduce the spread of infection among health care providers, all likely practices must be engaged, and health care providers should follow the required infection prevention practice. It was recognized that the spread of disease among health care providers is linked to poor hand hygiene, congestion, a lack of separation area, and environmental contamination.11
Social distancing and regular use of a face mask are the first key infection prevention practices for health care workers, in addition to other infection prevention practices, such as hand hygiene. In resource-constrained countries, the prevalence of communicable diseases is high, and hospitals can rely heavily on face masks to protect medical personnel from coronavirus infection and prevent cross-contamination among patients, the general public, and health care workers.12,13 Different study shows wearing of face mask can reduce the risk of respiratory virus infection. A systematic review and meta-analysis in Chinese show wearing of face mask can prevent from influenza virus and SARS-CoV-2.14,15
The WHO, CDC, and the Ethiopian Ministry of Health all recommended using face masks to control the pandemic across countries, as standards and utilization of face masks is a current hot topic for the most front-line health care providers working at public health institutions at this time, along with other personal protective equipment. However, proper use of a face mask is critical to preventing the spread. According to the World Health Organization, improper use and inappropriate discarding of this mask increases the degree of spread. This is an indication that health care providers lack knowledge and practice in the proper use of face masks.16 The purpose of this study was to assess health care workers’ knowledge and proper face masks utilization to reduce the extent of coronavirus infection in Amhara region referral hospitals in Ethiopia.
Study Area and Period
A cross-sectional survey was conducted from May 15 to 30/2020 at Amara region referral hospitals in Ethiopia. Amhara regional state is one of eleven regional states in Ethiopia, located in the northwestern part of the country between 11° 30ʹ 00ʺ N latitude and 38° 30ʹ 00ʺ E longitude.
Amhara is Ethiopia’s largest region, with 12 zones, three city administrations, and 180 woreda (139 rural and 41 urban). According to the Ethiopian Central Statistics Agency, the region has a population of 21.5 million people, with rural agriculturalists accounting for roughly 80% of the population.17 Amara region had only nine public hospitals and 140 health centers two decades ago, which was insufficient to meet the region’s needs. Furthermore, facility coverage and excellence were lacking. The region now has 82 hospitals (7 referral hospitals, 2 general hospitals, and 73 primary care hospitals), 847 health centers, and 3342 health posts.
The region has seven referral hospitals: the University of Gondar Teaching Referral Hospital (UOGRH), Felege Hiwot Referral Hospital (FRH), Tibebe Ghion Referral Hospital, Dessie Referral Hospital (DRH), Debre Markos Referral Hospital (DMRH), Debre Tabor Referral Hospital, and Debre Berhan Referral Hospital (DBRH), all of which are expected to serve 5 million people. Each hospital had an average of 300 health care providers.
Sample Size Determination
The sample size was calculated using a single population proportion formula, assuming that 50% of health care workers are knowledgeable about and use face masks correctly, with a 5% margin of error (w) and a 95% (Za/2 = 1.96) confidence interval (CI). To compensate for the non-response rate, 10% of the calculated sample size was added, resulting in a final sample size of 422.
Population
The source population for this study was all health care professionals working at Amhara region referral hospitals, and the study population was all health care professionals working at Amhara region referral hospitals during the study period.
Sampling Technique and Procedure
Of seven referral hospitals, three referral hospitals were chosen through a lottery system: the University of Gondar Teaching Referral Hospital (UOGRH), Felege Hiwot Referral Hospital (FRH), Tibebe Ghion Specialized Hospital (TGSH), Dessie Referral Hospital (DRH), Debre Markos Referral Hospital (DMRH), Debre Tabor Referral Hospital, and Debre Berhan Referral Hospital (DBRH). The final sample size of 422 was assigned to the selected hospitals proportionally based on the average number of health care workers in each facility. Finally, the data was collected using the consecutive sampling method until the desired sample size was reached (Figure 1).
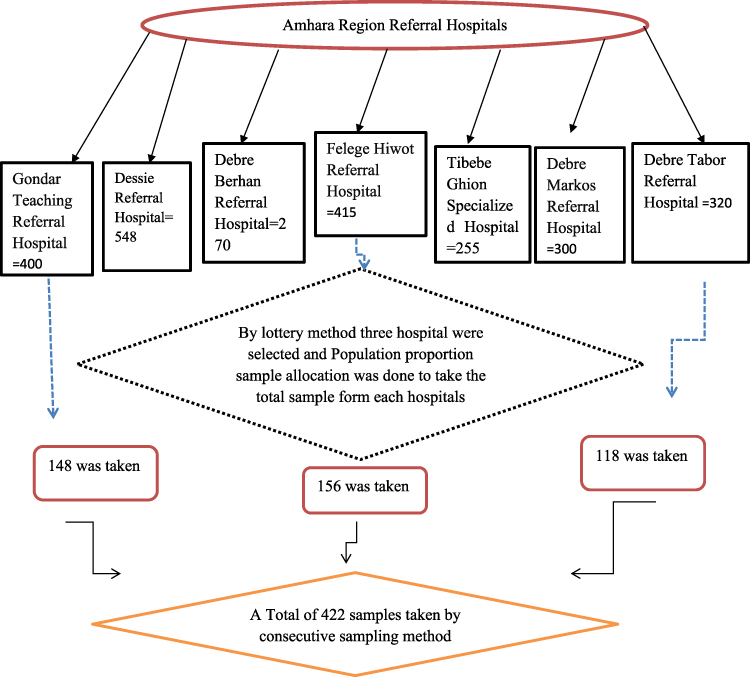 |
Figure 1 Schemes Presentation of the Sampling Procedure in Amhara Region Referral Hospital, Ethiopia, 2020. |
Inclusion and Exclusion Criteria
The study included health care providers who were willing to give informed consent, and was available at the time of the study.
Operational Definition
Health Care Providers
A person who has graduated from a recognized institution of higher learning and meets the Ethiopian Ministry of Health’s criteria for classifying, preventing, or treating disease.
Knowledgeable
Each correct answer in the information category was given a score of 1 and each incorrect response was given a score of 0. The final score was determined, and the labels were assigned based on the results (out of 9). A correct answer of >7 out of 9 questions (>80%) was considered good knowledge, while an incorrect response of ≤ 7 (≤80%) was considered poor knowledge.16
Proper Practice of Face Mask Utilization
The survey included 14 questions based on the World Health Organization (WHO) guidance on the correct use of face masks.18
The level of proper practice of face mask utilization was measured based on correct response using 14 questions. Each correct response scored 1 and each incorrect response was scored 0. The correct response of >11 out of 14 questions (>80%) was considered as good practice and (≤ 80%) was considered as poor practice.16
Data Collection Materials and Process
The questionnaire was adapted after reviewing different literatures, which had been developed for similar purpose by different authors. To meet the objective of the study, the questionnaires was carefully modified slightly in line with the context without changing the original meaning and it consisting of information on socio-demographic characteristics, knowledge and practice of health care providers regarding face mask towards COVID-19 prevention. The data were collected by using pre-tested self-administered questionnaire.
Data were collected by six Bachelors of Science midwives and supervised by 2 senior Bachelors of Science midwives.
Data Quality Control
The data quality was maintained by using several methods. First, a standard questionnaire was adapted from different literatures. Second, before the actual data collection pre-test was done on 5% of the total sample size out of the study area that is assumed to have similar characteristics of the targeted population. Based on the feedback received during the pre-test necessary amendment were done and the questions were assessed for its clarity; completeness, content and modified accordingly. Third, daily close supervision was made during the data collection and appropriate feedback was provided. Fourth, orientation was provided for the data collectors for one day by the principal investigator. The orientation was focus on the objective of the study and keeping confidentiality of the information they gathered. The collected data was checked for its completeness every day before the following day of data collection by supervisors and principal investigator.
Data Processing and Analysis
The collected data were coded, cleaned, and entered into SPSS Version 20 for analysis. All required variable recoding and transformation were completed prior to the final data analysis. A narrative and a graph were used to describe the variable under the study’s frequency distribution.
Ethical Review
The ethical approval was obtained from Debre Tabor University’s ethical review board, and a supporting letter was written to each referral hospital. Written informed consent was obtained from each health care provider after informing the purpose of the study. The study participants were informed that they had the right to refuse or discontinue participation in the study at any time during the data collection period.
Result
Socio Demographic Information
A total of 422 health care workers participated in the study, resulting in a 100% response rate. The respondents’ mean age was 31 years with 5.5 SD. More than two-thirds of the participants 284 (67.3%) were males, and approximately half of the participants were currently married. 225 (53.3%) and 410 (97.2%) were orthodox religious followers. More than half of health care professionals 232 (55%) are experienced 5–10 years. More than half 219 (52%) of respondents were nurses followed by midwives 149 (35%) (Table 1).
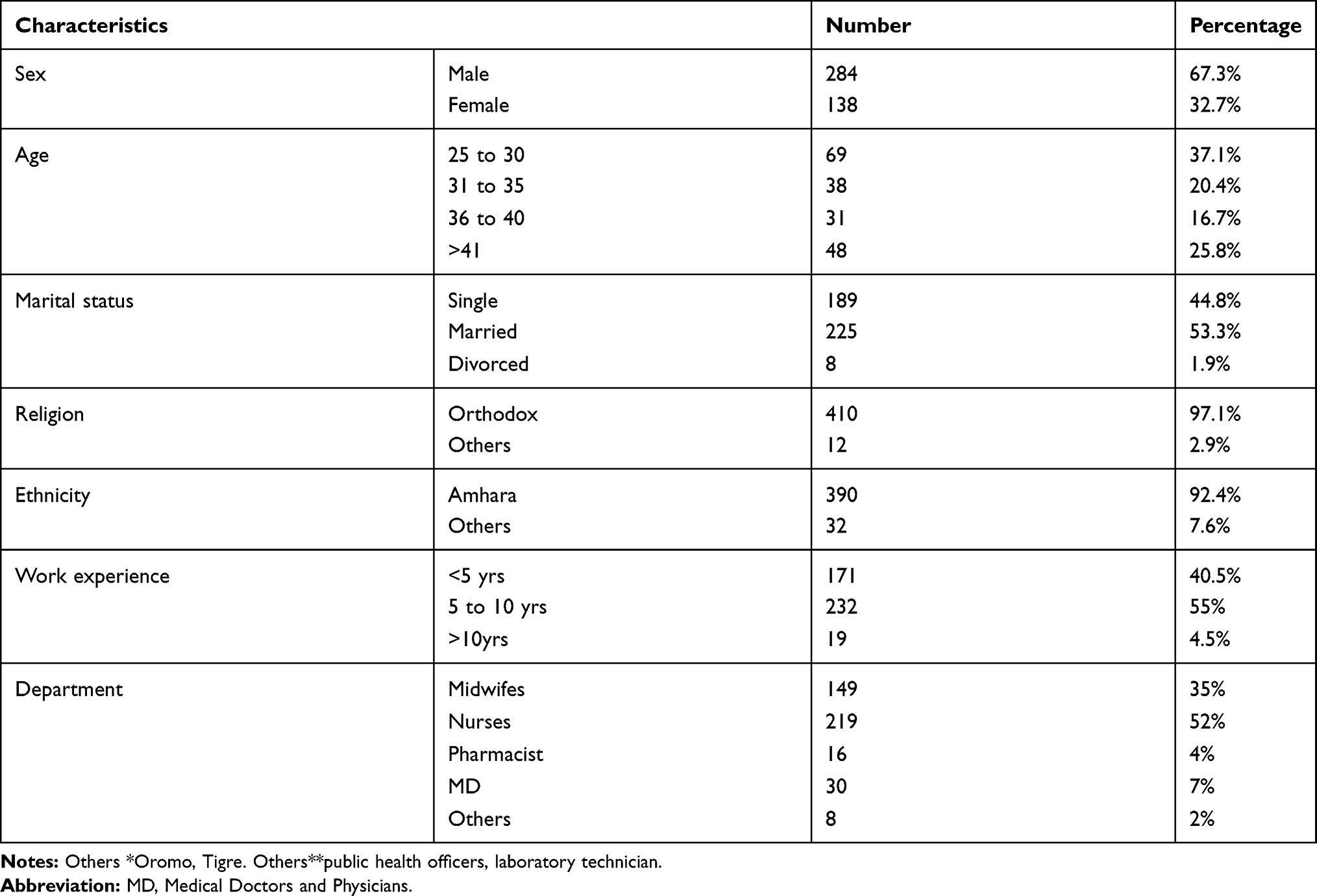 |
Table 1 Socio Demographic Characteristics of the Study Participants in Amhara Region Referral Hospitals (n= 422), 2020 |
Respondent Knowledge About Face Mask
Of the total of 422 respondents, 278 (65.8%) of the total participants were well-versed in the use of face masks. More than two-thirds of the 284 respondents (67.3%) correctly identified the proper technique for wearing a face mask. Almost all health care providers 405 (96%) knew that wearing a face mask properly prevents coronavirus infection, and 264 (62.2%) respondents knew surgical face masks had three layers, 64 (62.5%) knew that the middle layer act as a filter media barrier, 383 (90.8%) knew face masks should be covered nose, mouth and chin, 331 (78.4%) knew 8 hours the maximum recommended duration of wearing surgical mask and more than half of respondents 228 (54%) knew a close face mask is not effective as a surgical face mask. 6 out of ten health providers 257 (60.9%) knew the purpose of the metal strip was to fit the nose (Table 2).
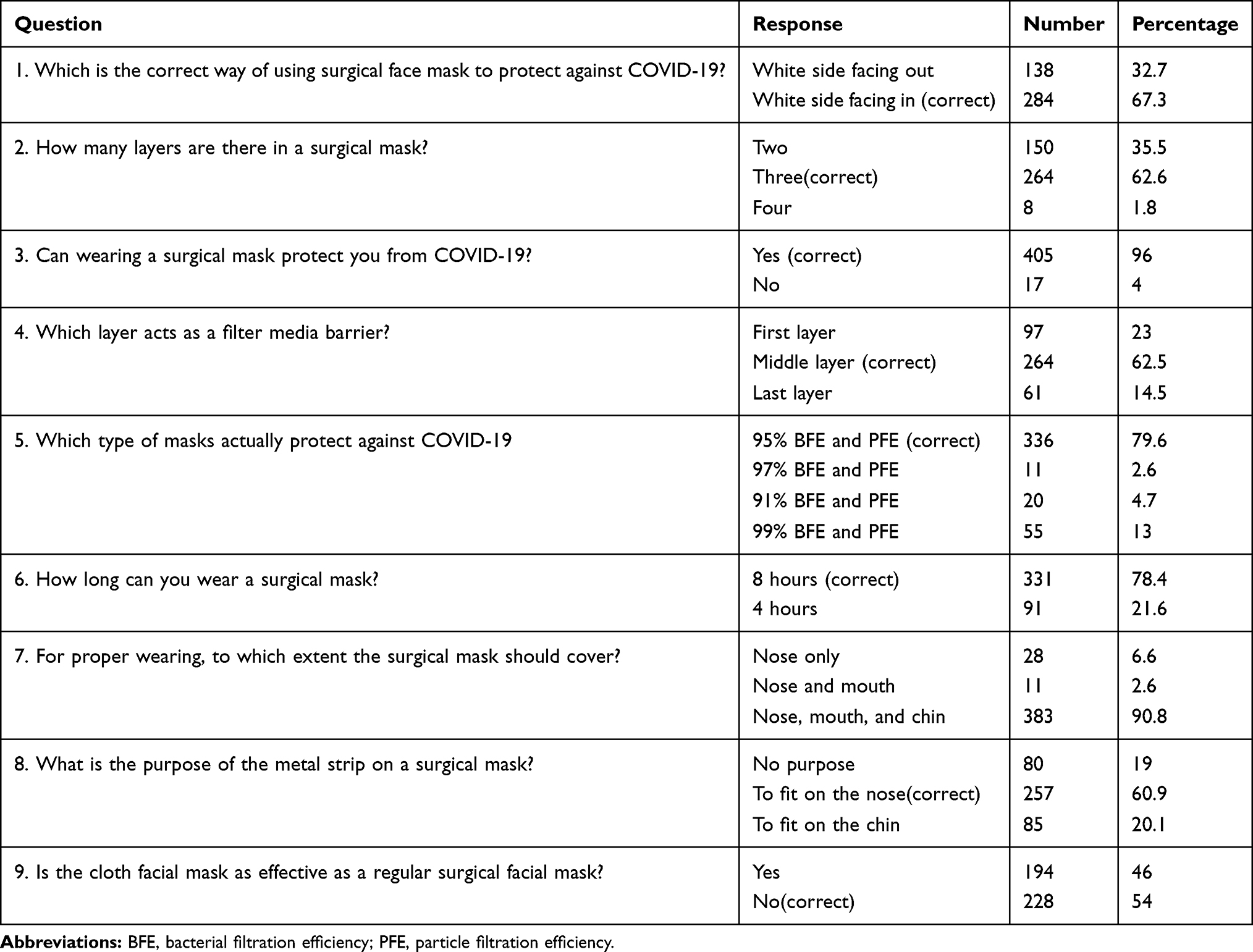 |
Table 2 Knowledge of the Respondents About Mask Utilization to Prevent COVID-19 Among Health Care Providers at Amhara Region Referral Hospitals (N= 422), 2020 |
Proper Practice of Face Mask Utilization Among the Respondents
Of the 422 total respondents, 251 (59.5%) of health care professionals had good practice of face mask utilization to prevent COVID-19 infection or to minimize the spread of the infection. Good practice of face mask utilization was higher among nurses and poor practice of face mask utilization was higher among specialist’s doctors. Of the total respondents 319 (75.6%) wearing face mask starting from home and 96 (22.7%) of them wearing face mask always at working time, 258 (61.1%) of the study participants do not wear face mask in public places. Use of face masks according to the WHO guidance criteria, this result revealed that only 188 health care professionals (43.4%) do not removed their face mask if there is a need to talk to the patient, 178 (42.2%) clean their hands before wearing their face masks and almost three-fourth 312 (74%) of them check the inside and outside of the mask before wearing, 94 (22.3%) clean their hands after taking off their masks or touching, almost two-third 270 (64%) confirm the metal nose band on the top,35 (8.3%) avoidance of touching the mask with hands,146 (34.6%) taking off the mask properly without touching the anterior surface and 405 (96%) re-used a single-use face mask (Table 3).
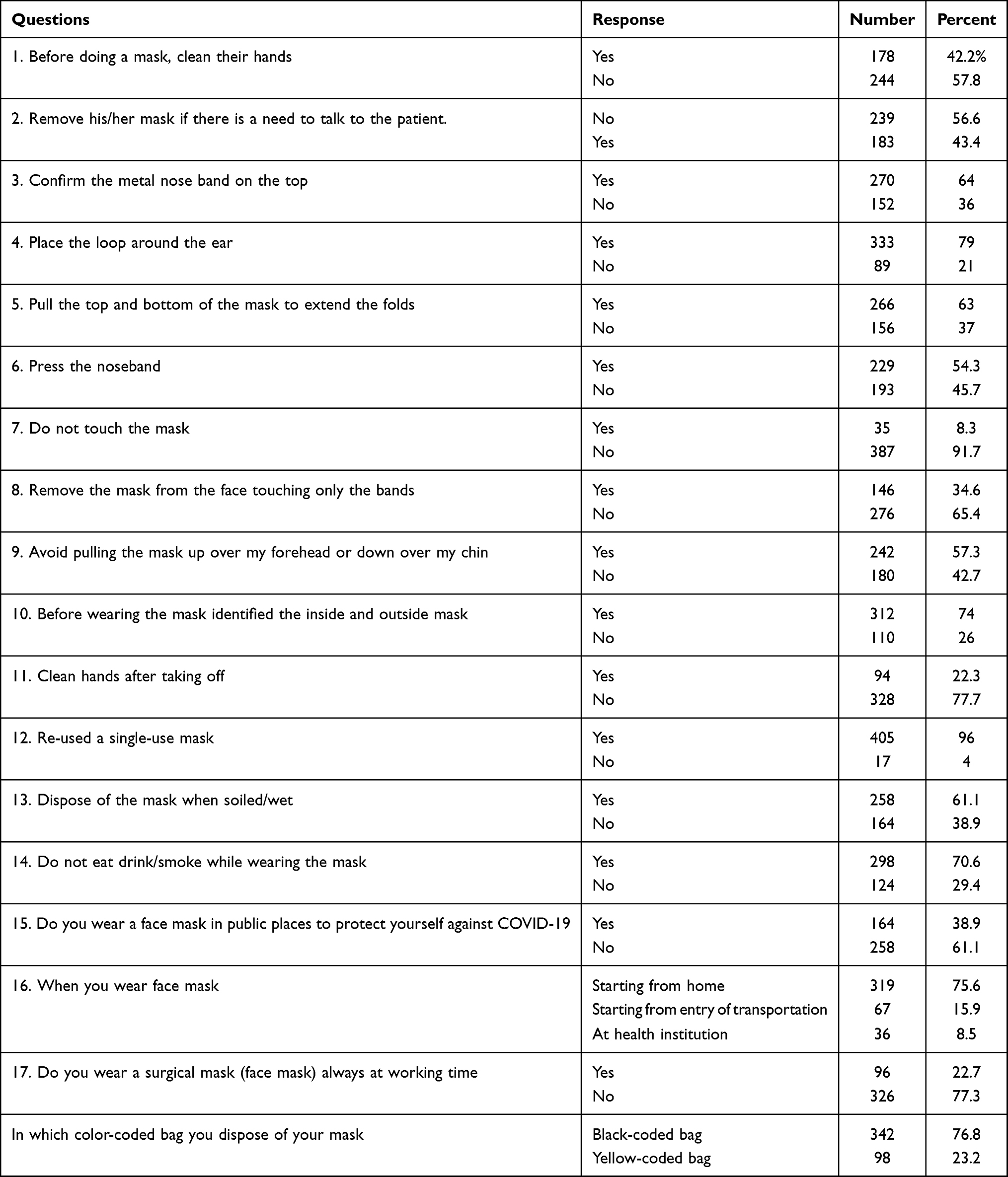 |
Table 3 Proper Practice of Face Mask Utilization of the Health Care Providers, in Amhara Region Referral Hospitals Ethiopia 2020 |
Discussion
This survey was conducted to assess knowledge and proper utilization of face mask to prevent the spread of COVID-19 infection among health care providers. Utilization of face mask is universally recommended infection prevention practice to reduce or to prevent the spread of COVID-19 throughout the world. Surgical masks are effective measures for preventing the transmission of SARS CoV-2. Wearing masks is strictly reserved for health care providers exposed to aerosol during invasive or specific procedures for patients suspected or confirmed as having COVID-19, although airborne transmission cannot completely be excluded. In this study, more than half 65.8% of the respondent has good knowledge about face mask.
The knowledge level in this study was higher than the knowledge level in Pakistan, which was 35%.16 This disparity could be attributed to differences in health coverage, disparities in COVID-19 awareness, and disparities in health system strategies among countries and difference in socio cultural and economic level.
More than two-thirds of the respondents 284 (67.3) knew correct method of wearing the face masks, around 264 (62.2%) knew there are three layers, and almost all of the respondents 405 (96%) knew wearing a face mask can protect against COVID-19, but only 54% knew close masks are not as effective as surgical masks. Another similar study conducted in Ethiopia backed up this finding.19
According to WHO guidance criteria, the proper use of a face mask in this finding was relatively low, accounting for 251 (59.5%). The finding of this study was lower than study conducted in Ethiopia about COVID-19 prevention practice among health care providers 67.3%20 and higher than another study conducted in Jimma University Medical Center visitors 35 (14.2%) and Addis Ababa, Ethiopia the proper utilization of face mask among the respondents were 33.3%19,21
This study’s findings were also higher than those of another study conducted in Ethiopia among chronic medical illness patients in Addis Zemen hospital, where only one-third (36.6%) of the study participants used a face mask.22 This difference might be due to difference in knowledge and awareness about face mask utilization and difference between the study populations. This finding is also lower than that of studies conducted in India and China.23,24 This might be due to difference in behavioral change or attitude of the respondents towards COVID-19 virus. When we compared male to female comparison of face mask utilization more than 75% out of the total usage or 42% of them were female. These indicate utilization of face mask in male participants were very low. This finding is supported by different research about the prevalence and death rate of men due to COVID-19 is relatively high.25 This might be due to low utilization of face mask and other infection prevention practice.
The main reasons given by respondents for not using a face mask were negligence, followed by a lack of resources. Almost all of the participants reused their face masks, which could be due to a scarcity of face masks; this finding is supported by other studies. Only 38.9% of the respondents were use face mask to prevent COVID-19 infection in public place. N95 type face mask utilization also very low. It was around 7% this might be due to its cost specially for African countries. It is very expensive but N95 type face mask is the most effective type of face mask to prevent the spread of COVID-19.26
In order to properly dispose of biomedical waste in hospitals, the WHO created a color-coded bin scheme.27 In this study, 342 respondents (76.8%) disposed of their used face mask in a black color-coded bag, while only 98 (23.2%) disposed in a yellow color-coded bag. This result is consistent with results from a Pakistan survey, which found that 44.9%of respondents disposed of their masks in a yellow-coded bag.16 However, this finding is lower than that of an Indian study, which revealed that 80.1% of respondents disposed of the mask in the yellow-coded bag.23
Of study participants, 67 (15.9%) of study participants were wearing face masks from the time they entered the transportation, indicating that infection prevention practices were very low. However, wearing a face mask is the recommended infection prevention practice.
Conclusion and Recommendation
Knowledge of the respondent was high in comparison with another studies but the proper utilization of face mask to prevent the spread of COVID-19 infection was relatively low. Ethiopian ministry of health in collaboration with Amhara region, zonal and woreda health institution works together to increase utilization of face mask and to alleviate scarcity of resource and it is better to provide training to the health care providers about the proper utilization of face mask to tackle the spread of COVID-19 infection.
Strength of the Study
The survey was conducted in selected referral hospitals so it can be representative for other hospitals.
Limitation of the Study
Due to scarcity of literature, it was very difficult to compare and contrast the finding of this study with other similar studies.
Abbreviation
CDC, Center for disease control and prevention; COVID-19, Coronavirus disease 2019; SARS CoV-2, severe acute respiratory syndrome coronavirus 2; WHO, World Health Organization.
Data Sharing Statement
The data used to support the findings of this study are available from the corresponding author upon formal request.
Ethical Approval and Consent to Participate
The Ethical clearance was obtained from the ethical review board of the Debre Tabor University and supporting letter was written to each Hospitals. Written Informed consent was obtained from each health care provider who is targeting after informing them the benefit, the confidentiality of the information and the voluntary nature of the participation of the study. The respondent was informed they have the right to refuse or stop at any time of the data collection.
Acknowledgment
We are highly thanks to Debre Tabor University for approval of ethical clearance. We would also like to extend our appreciation to the study participants, supervisors, data collectors and health extension workers.
Author Contributions
All authors contributed to data analysis, drafting or revising the article, have agreed on the journal to which the article will be submitted, gave final approval of the version to be published, and agree to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Sohrabi C, Alsafi Z, O’Neill N, et al. World Health Organization declares global emergency: a review of the 2019 novel coronavirus (COVID-19). Int J Surg. 2020;76:71–76. doi:10.1016/j.ijsu.2020.02.034
2. Burrer SL, de Perio MA, Hughes MM, et al.; Covid C, Team R. Characteristics of health care personnel with COVID-19 — United States, February 12–April 9, 2020. Morb Mortal Wkly Rep. 2020;69(15):477. doi:10.15585/mmwr.mm6915e6
3. Organization WH. Clinical Management of Severe Acute Respiratory Infection (SARI) When COVID-19 Disease is Suspected: Interim Guidance, 13 March 2020. World Health Organization; 2020.
4. Organization WH. nCoV Outbreak is an Emergency of International Concern. World Health Organization; 2020:31.
5. Anderson RM, Heesterbeek H, Klinkenberg D, Hollingsworth TD. How will country-based mitigation measures influence the course of the COVID-19 epidemic? Lancet. 2020;395(10228):931–934. doi:10.1016/S0140-6736(20)30567-5
6. Su Z, McDonnell D, Ahmad J. Article type: letter to the editor.
7. Control CfD, Prevention. Interim infection prevention and control recommendations for healthcare personnel during the coronavirus disease 2019 (COVID-19) pandemic. Accessed July 22, 2020.
8. Sun C, Ahmed MA, Cheng C. Is it wise not to include hair and shoe covers in personal protective equipment (PPE) recommendations? Infect Control Hosp Epidemiol. 2020;1–3. doi:10.1017/ice.2020.1306
9. Ma T, Heywood A, MacIntyre CR. Travel health seeking behaviours, masks, vaccines and outbreak awareness of Australian Chinese travellers visiting friends and relatives–implications for control of COVID-19. Infect Dis Health. 2021;26(1):38–47. doi:10.1016/j.idh.2020.08.007
10. Sun C, Ahmed MA, Kim NH, et al. Do we put frontline health care workers at more risk with the current CDC and WHO recommendation for ending isolation and precautions? Infect Control Hosp Epidemiol. 2021;1–5.
11. Molla KA, Abegaz SB, Tu W-J. Community knowledge, attitude and practices to SARS-CoV-2 disease 2019 (COVID-19): a cross-sectional study in Woldia town, Northeast Ethiopia. PLoS One. 2021;16(4):e0250465. doi:10.1371/journal.pone.0250465
12. Shen M, Zu J, Fairley CK, et al. Projected COVID-19 epidemic in the United States in the context of the effectiveness of a potential vaccine and implications for social distancing and face mask use. Vaccine. 2021;39(16):2295–2302. doi:10.1016/j.vaccine.2021.02.056
13. Zhao T, Hu C, Ahmed MA, Cheng C, Chen Y, Sun C. Warnings regarding the potential coronavirus disease 2019 (COVID-19) transmission risk: vaccination is not enough. Infect Control Hosp Epidemiol. 2021:1.
14. Liang M, Gao L, Cheng C, et al. Efficacy of face mask in preventing respiratory virus transmission: a systematic review and meta-analysis. Travel Med Infect Dis. 2020;36:101751. doi:10.1016/j.tmaid.2020.101751
15. Li Y, Liang M, Gao L, et al. Face masks to prevent transmission of COVID-19: a systematic review and meta-analysis. Am J Infect Control. 2020. doi:10.1016/j.ajic.2020.12.007
16. Kumar J, Katto MS, Siddiqui AA, et al. Knowledge, attitude, and practices of healthcare workers regarding the use of face mask to limit the spread of the new coronavirus disease (COVID-19. Cureus. 2020;12(4).
17. Fantahun M, Degu G. Health service utilization in Amhara region of Ethiopia. Ethiop J Health Dev. 2003;17(2):140–147.
18. World Health Organization. Rational use of personal protective equipment (PPE) for coronavirus disease (COVID-19): interim guidance. 2020. Available from: https://apps.who.int/iris/handle/10665/331498.
19. Tadesse T, Tesfaye T, Alemu T, Haileselassie W. Healthcare worker’s knowledge, attitude, and practice of proper face mask utilization, and associated factors in police health facilities of Addis Ababa, Ethiopia. J Multidiscip Healthc. 2020;13:1203. doi:10.2147/JMDH.S277133
20. Jemal B, Ferede ZA, Mola S, et al. Knowledge, attitude and practice of healthcare workers towards COVID-19 and its prevention in Ethiopia: a multicenter study. 2020.
21. Kebede Y, Yitayih Y, Birhanu Z, Mekonen S, Ambelu A, Tu W-J. Knowledge, perceptions and preventive practices towards COVID-19 early in the outbreak among Jimma University Medical Center visitors, Southwest Ethiopia. PLoS One. 2020;15(5):e0233744. doi:10.1371/journal.pone.0233744
22. Akalu Y, Ayelign B, Molla MD. Knowledge, attitude and practice towards COVID-19 among chronic disease patients at Addis Zemen Hospital, Northwest Ethiopia. Infect Drug Resist. 2020;13:1949. doi:10.2147/IDR.S258736
23. Singh AP, Agrawal P, Gautam A, Kumar D, Garg R, Pursnani N. Knowledge, attitude, and practices of healthcare workers in non-COVID areas of hospital regarding the use of face mask to limit the spread of the novel Coronavirus Disease (COVID-19): an Institutional Cross-sectional Online Survey. J South Asian Fed Obstet Gynaecol. 2020;2.
24. Ho H. Use of face masks in a primary care outpatient setting in Hong Kong: knowledge, attitudes and practices. Public Health. 2012;126(12):1001–1006. doi:10.1016/j.puhe.2012.09.010
25. Dehingia N, Raj A. Sex differences in COVID-19 case fatality: do we know enough? Lancet Global Health. 2021;9(1):e14–e15. doi:10.1016/S2214-109X(20)30464-2
26. Smith JD, MacDougall CC, Johnstone J, Copes RA, Schwartz B, Garber GE. Effectiveness of N95 respirators versus surgical masks in protecting health care workers from acute respiratory infection: a systematic review and meta-analysis. CMAJ. 2016;188(8):567–574. doi:10.1503/cmaj.150835
27. Chartier Y. Safe Management of Wastes from Health-Care Activities. World Health Organization; 2014.
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.