")
Back to Journals » Open Access Surgery » Volume 13
Knowledge and Perception of Ethiopian Surgical Patients to Informed Consent Practice for Surgical Procedures
Authors Lemmu B, Megersa A , Abebe E, Abebe K
Received 27 June 2020
Accepted for publication 17 August 2020
Published 7 September 2020 Volume 2020:13 Pages 65—70
DOI https://doi.org/10.2147/OAS.S268009
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Luigi Bonavina
Befekadu Lemmu,1 Abebe Megersa,2 Engida Abebe,1 Kirubel Abebe1
1Department of Surgery, St. Paul’s Hospital Millennium Medical College, Addis Ababa, Ethiopia; 2Department of Surgery, Ambo University Referral Hospital, Ambo, Oromia, Ethiopia
Correspondence: Kirubel Abebe
Department of Surgery, St. Paul’s Hospital Millennium Medical College P.O. Box 1271, Addis Ababa, Ethiopia
Tel +251 92 1143772
Email [email protected]
Background: Surgical informed consent (SIC) is an established ethical and legal requirement for surgical treatment. Patient understanding of the process is essential for efficient surgical care. This study aimed to assess the knowledge and perception of operated patients towards surgical informed consent.
Methods: An institution-based cross‑sectional study of all adult surgical patients who signed informed consent and underwent surgery at St. Paul’s Hospital Millennium Medical College (SPHHMC) from February 1st to March 30th, 2018, was performed. Data were collected postoperatively before discharge using a pretested structured questionnaire.
Results: Of 420 patients identified, 385 (91.7%, M:F=2:1) agreed and interviewed. The mean age was 40.3 years (SD± 15.1), and many of the respondents (285, 74.0%) had some level of formal education. Even if most (336, 87.3%) knew the reason why they had surgery, less knowledge and awareness was reported regarding the options of alternative treatments (153, 39.7%), identifying the operating surgeon (129, 33.5%), the type of surgery (160, 41.6%), anesthesia-related risks (96, 24.9%), complications of surgery (69, 17.9%) and postoperative care (4, 1.0%). The legal requirement of surgical informed consent was reported by 267 (69.4%) subjects; however, more than half had no information on the right to change their mind after signed surgical informed consent (223, 57.9%) and whom it protects (224, 58.2%). Only 40 (10.5%) respondents had a good level of knowledge, and it was significant in those with some level of formal education (OR=4.8; 95% CI 1.45– 16.01; P=0.010) and in patients who live in an urban area (OR=4.7; 95% CI 1.81– 12.35; p=0.002) than their respective groups.
Conclusion: Our patients had limited knowledge and perception regarding surgical informed consent. Hence, the current consent process seems inadequate and needs a revisit.
Keywords: informed consent, knowledge, surgery, perception
Introduction
Surgical informed consent (SIC) is not an event or a signature on a piece of paper but an ongoing process of communication that begins when initial contact is made with the patient and continues through surgery and postoperative care.1–3 It is an established ethical and legal requirement for surgical treatment that serves to protect both the patient and the surgeon from unwanted procedures and accusations, respectively.1,2,4 Informed consent is aimed to shift the care from physician-centered to patient-centered care by promoting shared decision-making. SIC acknowledges patients’ autonomy and basic human rights of self-determination.1,2
According to the updated World Medical Association Declaration of Lisbon, the patient has the right to adequate and clear information regarding the purpose and result of any form of treatment/test. Information should be given in a way that the patient can understand taking into consideration the patient’s culture to make an informed and self-determined decision. Besides, the physician should also inform the patient about the consequences and implications of withholding consent. The declaration also stated that the consent process should respect the patient’s right to agree or refuse any diagnostic procedure or therapy provided that the patient is adult, mentally fit and competent.5
Patient awareness of legal and ethical issues related to the consent process is often limited which may lead to a feeling of powerlessness, vulnerability, and hopelessness.6 The information delivered is the major determinant of decision-making in the consent process. It should include at least the reason for surgery, the proposed surgery, the risks and benefits of the proposed surgery, alternative treatments, and their risks and benefits of declining treatment.2,4
Studies reported, only a little information is recalled by the patients during the informed consent process and their level of understanding is commonly overestimated. Several factors like patients’ age, educational level, intelligence, etc., are related to patient comprehension. The information given during the consent process assumed to help the patient to decide in autonomous and rational ways. However, some patients decide based on their instinct or something else like the hospital’s reputation, surgeon’s commitment, etc.2
Patients may change their minds and decline surgical care at any time in the process of treatment. Without a right to refuse, informed consent violates the principle of autonomy and self-determination. Prosecution is unlikely to be successful as far as the surgeon maintains good communication, mutual understanding and trust.1,2
Even if literature reported minimal attention and several misconceptions among surgical patients toward SIC, it is not well known and studied in most developing countries including Ethiopia.3,7 Conducting this cohort to assess the knowledge and perception of operated patients toward the SIC process provides data to improve the practice of patient-centered surgical care and decision-making.
Patients and Materials
Institution-based cross-sectional study design was employed from February 1st to March 30th, 2018, to assess knowledge, attitude and perception of adult surgical patients who signed and underwent a surgical procedure at SPHMMC. SPHMMC is a tertiary referral teaching hospital in Addis Ababa, Ethiopia serving a catchment area of more than 6 million people. The department of surgery is staffed with more than thirty surgeons from different specialties. On average 200 to 250 adult patients are operated every month.
As the p-value was not known, a value of 0.5 was used to calculate sample size which made it 384 patients. Of 420 surgeries done in the two months, 385 (91.7%) patients fulfilled the inclusion criteria (age 18 or above, conscious, mentally healthy and clinically stable) and were interviewed face to face after each patient gave written informed consent to participate in the study.
A pretested structured questionnaire which comprised sociodemographic profile and question on knowledge, attitude and perceptions towards surgical informed consent and their legal issues employed. Because the questionnaire was prepared in the English version it was translated to the local language which is Amharic and back to English to maintain its consistency. Data were collected prospectively after surgery but before discharge by trained Interns working in the department.
To evaluate the level of knowledge five questions were selected, which are the major components of SIC, and points allocated to their answers; 1 if they answered “Yes” and 0 if they answer “No”. The points were added and scored out of five. If a patient scored 0 to 1, he/she was said to have poor knowledge, 2 unsatisfactory, 3 satisfactory and 4 to 5 judged as good knowledge.
Data were checked for completeness, accuracy, consistency then coded and entered into SPSS version 20 for analysis. Results were shown using tables and central tendency statistics. Comparison of categorical variables was done using the Chi-Square test while P values of 0.05 or less was considered significant. A written ethical clearance letter was obtained from SPHMMC Institutional Review Board and confidentiality was kept throughout the study.
Results
Sociodemographic Characteristics
Of the 420 patients, 385 (91.7%) agreed to participate. Patients’ age ranged from 18 to 80 years with a mean of 40.3 years (SD ± 15.2). Males comprised two-third of the participants (256,66.5%) making male to female ratio 2:1. Three-fourth of the respondents were married (295,76.6%) and had some level of formal education (285,74.0%). Urban residents (241, 62.6%) and emergency surgeries (246, 63.9%) each made nearly two-thirds of the respondents (Table 1).
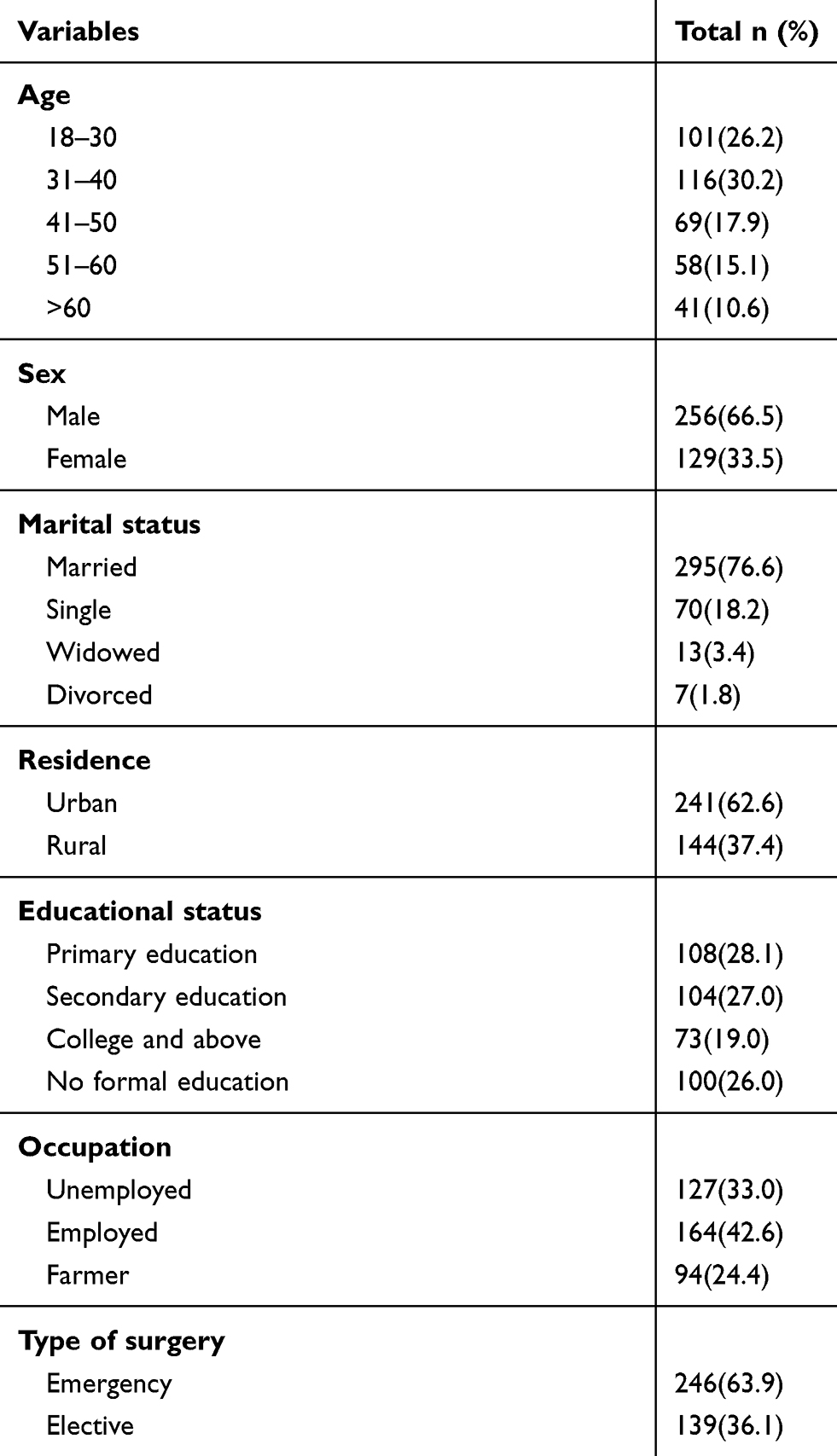 |
Table 1 Sociodemographic Characteristics of Respondents, St. Paul’s Hospital Millennium Medical College, Addis Ababa, Ethiopia, 2018 |
Knowledge
Of the responders, 199 (51.7%) signed Informed consent previously at least once. Even if most (336, 87.3%) knew the reason why they had surgery, less knowledge and awareness was reported regarding the type of surgery (160, 41.6%), its complications (69, 17.9%) and options of alternative treatment (153,39.7%) (Table 2).
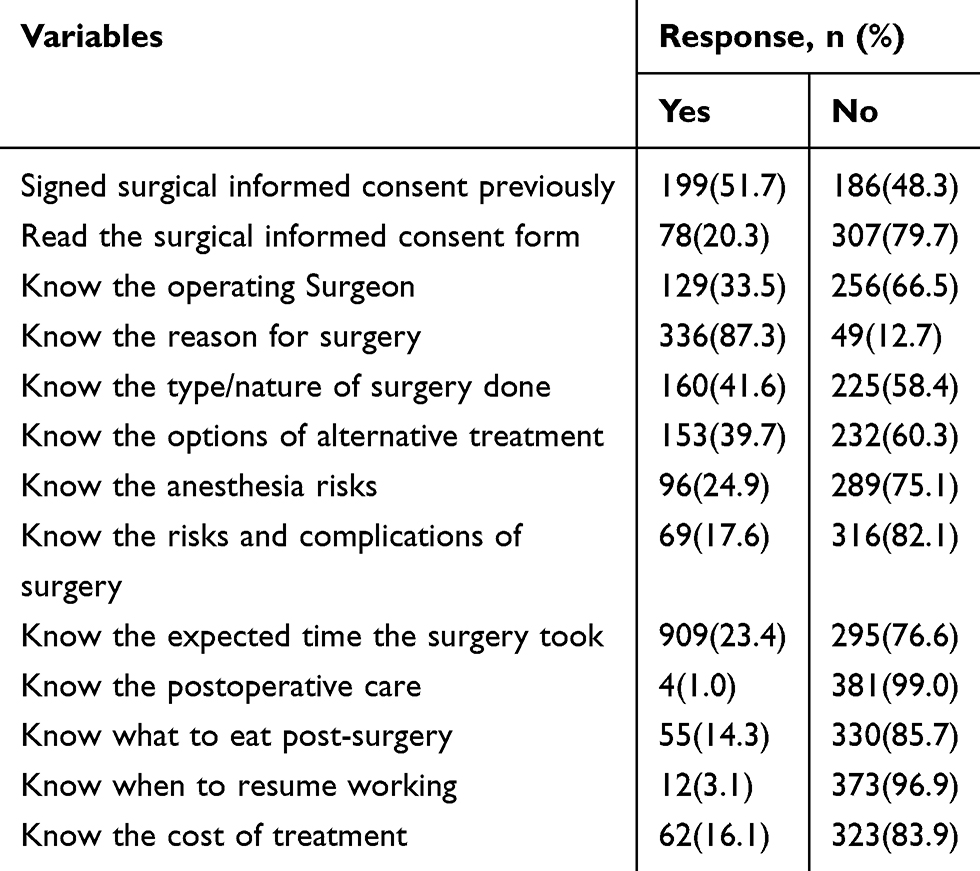 |
Table 2 Respondents Knowledge and Understanding Towards Surgical Informed Consent, St. Paul’s Hospital Millennium Medical College, Addis Ababa, Ethiopia,2018 |
Overall, the level of knowledge towards SIC was good only in 40 (10.5%), satisfactory in 94 (24.4%). One-third, 133 (34.5%), of the patients’ knowledge regarding SIC was poor. Of the patients with a poor level of knowledge, 52 (40%) signed SIC and undergone surgery in the past.
Perception
The majority (316, 82.1%) of the patients think that SIC was necessary and it was their obligation to sign (340, 88.3%), otherwise they will not be operated. The legal requirement of SIC was understood by 267 (69.4%) subjects. However, one-third (120, 31.2%) of patients perceived that the informed consent would remove their compensation and the hospital/operating surgeon would not be asked and sued if the wrong procedure were done and costs the life of a patient (126, 32.7%). More than half (223, 57.9%) of the respondents had no information regarding the right to change their mind once they signed the SIC. The right to sign on their behalf was given to relatives in a condition that the patients could not do by themselves (349, 90.6%) Table 3.
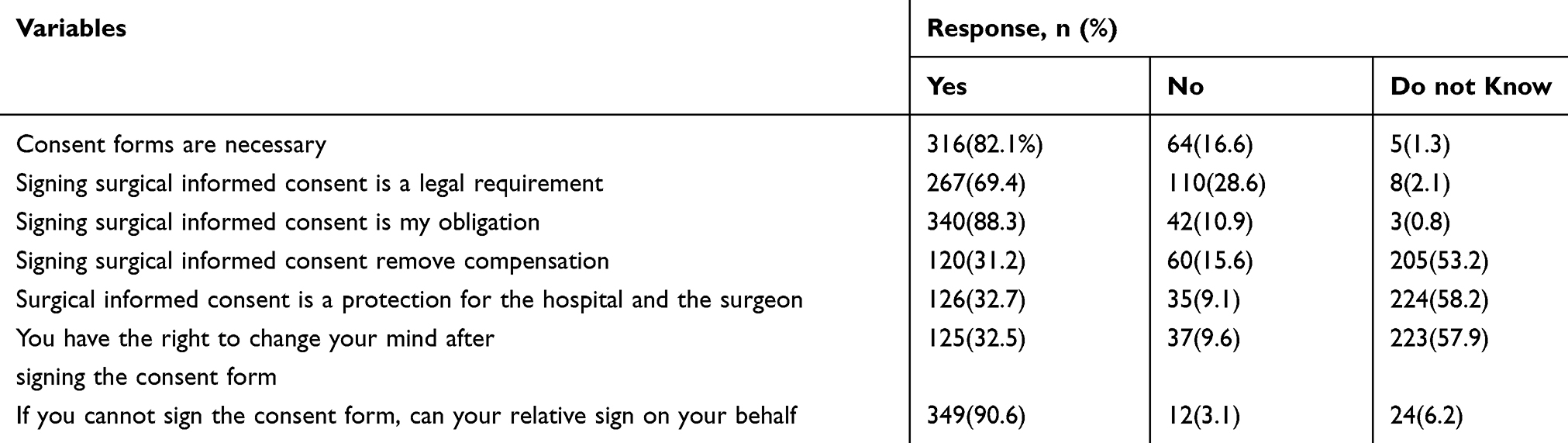 |
Table 3 Respondents Perception Towards Surgical Informed Consent, St. Paul’s Hospital Millennium Medical College, Addis Ababa, Ethiopia 2018 |
Factors Associated with the Level of Knowledge
A good level of knowledge towards SIC was significantly higher in patients with formal education (OR=4.8; 95% CI 1.45–16.01; P=0.010) and in those who live in an urban area (OR=4.7; 95% CI 1.81–12.35; p=0.002). Otherwise, sex, age and nature/mode of surgery had no statistically significant association with the level of knowledge (Table 4).
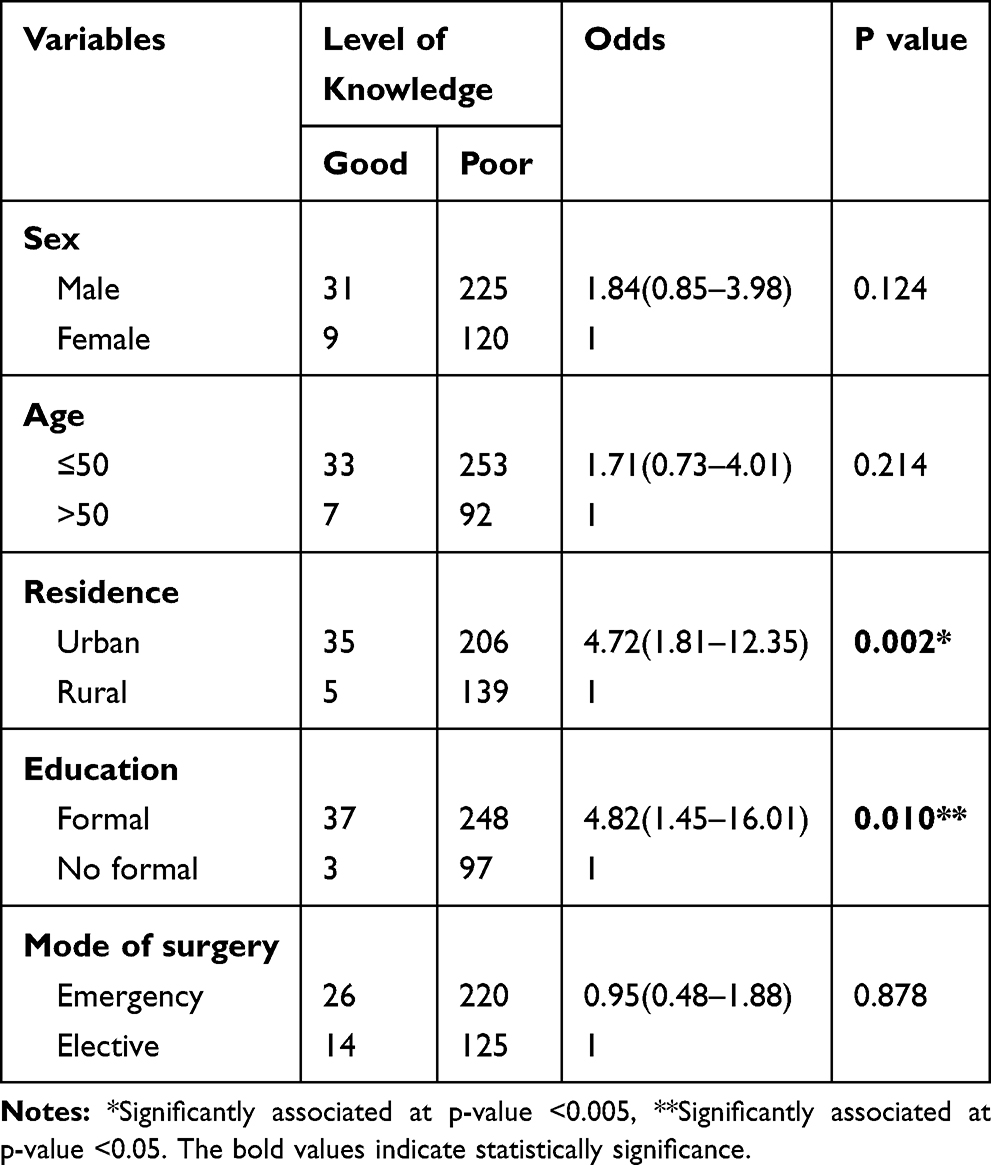 |
Table 4 Factors Associated with Level of Knowledge Towards Surgical Informed Consent, St. Paul’s Hospital Millennium Medical College, Addis Ababa, Ethiopia 2018 |
Discussion
SIC is meant to adequately inform the patient about the procedure to be carried out, benefits, alternatives and possible complications to enable appropriate decisions and to recognize the patient’s autonomy and dignity.8,9 It is also an opportunity for the surgeon to establish a relationship of openness and trust with the patient, and to promote mutual understanding to decrease unnecessary litigations if the unexpected occurs.9,10 The UK supreme court Montgomery judgement (2015) was a landmark event in reinforcing patient-centered care and shared-decision making (SDM) as the major part of valid consent. It also shifted from the thinking that considered SDM in consent as guidance to legal requirement.11 Literature reported that written information, with good patient education during the consent process, leads to better understanding and postoperative recall.8,10,12
Our study and others, demonstrated majority of the subjects knew that SIC was necessary and it was an obligation to undergo surgery.8,13,14 However, more than two-thirds of our respondents did not read the SIC before signing it; similar to findings of Leclercq et al.3 This is mainly related to the surgical care culture in the developing nations where the patient thinks the doctors decide what to do.7 Inadequate time allocation (though patients did not report it) for the consent process especially in emergency surgeries might have also contributed.
In line with our findings, Adisa et al and Nnabugwu et al reported that many of their patients (93.7% and 78.3%) knew the reason for surgery, and less knowledge was noted regarding options of alternative treatment, risks of the planned surgery and anesthesia.9,15 In contrast, a study from the UK revealed high knowledge concerning the risks of surgery.16 This discrepancy may reflect the difference in the level of literacy among the study subjects and consent process which gave more emphasis for the diagnosis.9 As compared with other studies our patients recall less information about the type and nature of the operation.9,15,17,18 Another Ethiopian study also showed most of the patients were not informed about alternative treatment and complications of the procedure.19 Similar with our analysis, a study from Uganda reported less than a quarter (22.4%) of their patients knew the surgeon who conducted the procedure.18 Such lower values are mainly related to not only the patient’s knowledge on SIC but also the poor practice of the surgeons and residents in charge. This in turn might reflect the lack of formal teaching of bioethics and communication skills in the surgical residency program of our country. According to Jarayedi Z and Asghari F, the surgical residents in Iran acquire such skills from their professors and senior residents rather than formal courses.20 A study from Nigeria and Uganda suggested incorporating biomedical ethics in medical education improves consent practice.18,21
The legal requirement of SIC was reported by more than two-thirds (69.4%) of our patients. Comparable observations were also made by studies from Egypt 69.18%, Kuwait 69.9%, India 75% and the United Kingdom 88%.6,8,16,22 However, 16% of clients of the UK study believed that it will remove their right to compensations. The figure is much lower than ours’ and other studies from Africa and Asia.6,8,13,16,22 Educational status may contribute to this difference as educated patients tend to be conscious regarding their right and are more likely to understand information on the consent.23
Authors showed that more than half of clients/patients perceived that SIC aims, mainly, to protect the hospital and the surgeon from litigation.8,13,22 A study from the UK demonstrated 46% of their patients reported that the main goal of SIC is to protect the hospital.16 In contrast with this, our analysis reported a lower number of clients had this impression. This is a paradoxical reflection because more than half (58.2%) of our patients signed the consent without knowing whom it protects.
Literature reported that 8.7% to 20% of patients did not know whether they could change their minds after they had signed SIC.6,8,13,16,22 This is much lower than our finding which could be due to inadequate consent process and the urgency of surgery as most of our patients underwent emergency procedures. Many of our and other participants thought that their relative could sign on their behalf if they cannot sign the consent.8,13,16
Factors associated with the level of knowledge and understanding:
Patient knowledge and understanding of the SIC process can be influenced by factors; patient’s age, educational level, intelligence, cognitive function and anxiety.2 It is also associated with the health profession age, years of experience and duration of training.19 The current study identified that level of knowledge and understanding was higher in patients with some level of formal education (OR=4.8; 95% CI 1.45–16.01; P=0.010) than patients with no formal education. A similar finding was also demonstrated in studies from Nigeria and India.6,7,15,23 Moreover, patients’ who reside in an urban area (OR=4.7; 95% CI 1.81–12.35; p=0.002) had a better level of Knowledge. This may be due to more access to different sources of information in urban settings than rural. Avoiding technical words, using patient’s language, allocating sufficient time and addressing patients’ concerns during the consent process plays a vital role in understanding the information for decision-making.7,17,19 Furthermore, different authors advocate the use of audio-visual information and leaflets improves patient understanding and recall.2,9,10
The main limitations in this study include recall bias, since the questions were entirely dependent on patients recalling capacity, and failure to include some important data concerning the consent process such as the health-care provider who obtained the informed consent, the time spent and timing of counseling. Despite these limitations, the study assessed our patient’s knowledge and perception towards SIC and provided data to evaluate our practice.
In conclusion, our patients had limited knowledge and perception regarding SIC. Hence, the existing consent process and form deserve re-evaluation to serve its purpose. In addition, the hospital needs to design awareness creation measures towards SIC.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Bernat JL, Peterson LM. Patient-centered informed consent in surgical practice. Arch Surg. 2006;141(1):86–92.
2. Hall DE, Prochazka AV, Fink AS. Informed consent for clinical treatment. CMAJ. 2012;184(5):533–540. doi:10.1503/cmaj.112120
3. Leclercq WK, Keulers BJ, Scheltinga MR, Spauwen PH, van der Wilt GJ. A review of surgical informed consent: past, present, and future. A quest to help patients make better decisions. World J Surg. 2010;34(7):1406–1415.
4. Wheeler R. Consent in surgery. Ann R Coll Surg Engl. 2006;88(3):261–264. doi:10.1308/003588406X106315
5. World Medical Association Declaration of Lisbon on the Rights of the patient. Available from: www.wma.net/policies-post/wma-declaration-of-lisbon-on-the-rights-of-the-patient/.
6. Singh R, Chopra M, Singh GP, Bhardwaj A, Kaur B, Aggarwal OP. Patient’s awareness, attitude, understanding and perceptions towards legal nature of informed consent. J Ind Acad Forensic Med. 2013;35(1):40–43.
7. Agu KA, Obi EI, Eze BI, Okenwa WO. Attitude towards informed consent practice in a developing country: a community-based assessment of the role of educational status. BMC Med Ethics. 2014;15(1):77. doi:10.1186/1472-6939-15-77
8. Alazmi S. Patients’ perception of informed consent for surgical operations in Kuwait. J High Inst Public Health. 2018;48(2):92–96. doi:10.21608/jhiph.2018.19915
9. Adisa AO, Onakpoya UU, Oladele AO, Lawal OO. Informed consent in surgery: an audit of practice in Ile-Ife, Nigeria. Niger J Clin Pract. 2008;11(3):206–210.
10. Anderson OA, Wearne IM. Informed consent for elective surgery—what is best practice? J R Soc Med. 2007;100(2):97–100.
11. Ward J, Kalsi D, Chandrashekar A, et al. Shared decision making and consent post-Montgomery, UK Supreme Court judgement supporting best practice. Patient Educ Couns. 2020;15.
12. Lewis PJ, O’Keefe L, Adcock S. Patients who were given information sheets have better postoperative recall of information. J R Coll Surg Edinb. 1991;36(3):206–207.
13. Parmar P, Rathod GB, Rathod S, Parikh A. Consent in medical practice–Perceptions of patients towards legal aspects of informed consent. IAIM. 2016;3(4):105–110.
14. Gong N, Zhou Y, Cheng Y, et al. Practice of informed consent in Guangdong, China: a qualitative study from the perspective of in-hospital patients. BMJ Open. 2018;8(10):e020658.
15. Nnabugwu II, Ugwumba FO, Udeh EI, Anyimba SK, Ozoemena OF. Informed consent for clinical treatment in low-income setting: evaluating the relationship between satisfying consent and extent of recall of consent information. BMC Med Ethics. 2017;18(1):69.
16. Akkad A, Jackson C, Kenyon S, Dixon-Woods M, Taub N, Habiba M. Patients’ perceptions of written consent: questionnaire study. BMJ. 2006;333(7567):528.
17. Ngim NE, Ndifon WO, Umoh MS, Ogunkeyede A. Informed consent for surgery in Nigeria: is the practice adequate? Global J Med Sci. 2008;7:1–2.
18. Ochieng J, Buwembo W, Munabi I, et al. Informed consent in clinical practice: patients’ experiences and perspectives following surgery. BMC Res Notes. 2015;8(1):765.
19. Teshome M, Wolde Z, Gedefaw A, Tariku M, Asefa A. Surgical informed consent in obstetric and gynecologic surgeries: experience from a comprehensive teaching hospital in Southern Ethiopia. BMC Med Ethics. 2018;19(1):38. doi:10.1186/s12910-018-0293-2
20. Jarayedi Z, Asghari F. From whom do physicians obtain consent for surgery? J Med Ethics. 2018;44(6):366–370. doi:10.1136/medethics-2017-104556
21. Ezeome ER, Marshall PA. Informed consent practices in Nigeria. Dev World Bioeth. 2009;9(3):138–148. doi:10.1111/j.1471-8847.2008.00234.x
22. Ahmed SA, Dewedar S. Obstetric patient perceptions of written consent forms: a middle east hospital study. Int J Acad Res. 2011;3(1):471–475.
23. Sulaiman AI, Ayyuba R, Diggol IG, Haruna IU. Knowledge, attitude and perception of patients towards informed consent in obstetric surgical procedures at Aminu Kano Teaching Hospital. Nigerian J Basic Clin Sci. 2015;12(1):45. doi:10.4103/0331-8540.156688
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.