")
Back to Journals » Cancer Management and Research » Volume 12
Knowledge and Attitude of Ethiopian Oncology Nurses About Cancer Pain Management: National Survey
Authors Admass BA , Endalew NS , Tawuye HY , Mersha AT
Received 7 May 2020
Accepted for publication 17 September 2020
Published 25 September 2020 Volume 2020:12 Pages 9045—9055
DOI https://doi.org/10.2147/CMAR.S261172
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Eileen O'Reilly
Biruk Adie Admass, Nigussie Simeneh Endalew, Hailu Yimer Tawuye, Abraham Tarekegn Mersha
Department of Anaesthesia, School of Medicine, College of Medicine and Health Science University of Gondar, Gondar, Ethiopia
Correspondence: Nigussie Simeneh Endalew Email [email protected]
Background: Cancer is becoming a leading cause of death worldwide. Pain is a common and devastating symptom of cancer patients that can significantly affect the patient’s quality of life. Optimal cancer pain control requires adequate knowledge and positive attitudes of nurses. Little is known about the knowledge and attitudes of oncology nurses towards cancer pain management in Ethiopia. The current study aimed to assess the knowledge and attitude of nurses and determinants of cancer pain management in all oncology centers in Ethiopia.
Methods: A nationwide cross-sectional survey was conducted on 138 nurses in all oncology centers in Ethiopia. Self-completed survey questionnaires were distributed using the ‘Knowledge and Attitudes Survey Regarding Pain (KASRP)’ tool. Both bivariable and multivariable logistic regression analyses were used. Both crude odds ratio and adjusted odds ratio with the corresponding 95% CI were calculated to show the strength of association. Variables with a p-value of < 0.05 were considered as statistically significant.
Results: Only 7.2% (95% CI: 2.9, 11.6) of oncology nurses had good knowledge and attitude about cancer pain management. Among 41 items, the mean number of correctly answered questions was 20.4 (SD = 5.13). Nurses who had a master’s degree in nursing were positively associated with good knowledge and attitude about cancer pain management.
Conclusion: In this nationwide study, the overall knowledge and attitude level of oncology nurses towards cancer pain management were poor. Nurses who had a master’s degree in nursing were significantly associated with good knowledge and attitude towards cancer pain management. Regular training and revision of the contents of pain management education in the academic curriculum of nursing education are recommended.
Keywords: pain management, nurses, cancer, knowledge, attitude
Background
Cancer is becoming a leading cause of death worldwide.1–3 Sub-Saharan Africa is predicted to have a greater than 85% increase in cancer burden by 2030.4 Currently, its burden overlaps with the magnitude of infectious diseases in these countries.5–8 In Ethiopia, it has been the second leading cause of death among non-communicable diseases.9 Despite this fact, it continues to receive low priority, largely because of the overwhelming burden of communicable diseases and limited resources.9,10
Pain due to cancer is a common and devastating symptom that affects a patient’s life more than the disease itself.11 It has a profound effect on all aspects of the quality of life, and may also affect the patient’s will to live or to cooperate in treatment.12,13 The cause of pain ranges from direct tumor invasion and metastasis to other sites.14,15
Despite advances in current pharmacology of cancer pain management and improvements in interventions; studies documented that many patients with cancer continued to experience high levels of pain worldwide. Approximately, 30% to 50% of cancer patients receiving treatment experience pain and 70% to 90% with advanced stages of cancer experienced moderate to severe pain16–20. Data regarding the status of cancer pain management in Ethiopia are limited. However, according to a study conducted in Gondar, Ethiopia, inadequate pain management accounts for 91% of patients with cancer.16 The high prevalence may be attributed to a lack of awareness of patients, limited treatment options, late presentation of patients with advanced malignancy, and inadequate knowledge and attitude of nurses.21–23
Globally nurses play a crucial role in assessing pain, administering medications, monitoring and reassessing patients’ responses.24–26 Despite they have different levels of training backgrounds, nurses have the same bedside responsibilities in Ethiopia, which requires an understanding of the nature of pain and individual attitude to a patient’s clinical condition to control the pain optimally.27 However, in Ethiopia, there is no cancer speciality training to nurse for palliative care rather general BSc and/or MSc nursing which contains some limited palliative care related courses in their curriculum. As a result, nurses most of the time gave the service through limited ongoing training and experience in palliative units.
Many barriers can make inadequate treatment of cancer pain, which might be provider related, system related or patient related. Unfortunately, poor knowledge and negative attitude of nurses towards cancer pain managements reported as one of the commonest hurdles in cancer pain management.15,28–33 Although data regarding the status of cancer pain management and knowledge and attitude of nurses towards cancer pain management is limited in Ethiopia, a survey conducted at selected oncology centers in Addis Ababa, Ethiopia showed that nurses had poor practice and negative attitudes towards cancer pain management. The main barriers were lack of courses related to pain in the undergraduate classes, lack of continuing training, role confusion, and lack of motivation.22 Therefore, the current study aimed to conduct a nationwide survey regarding nurses’ knowledge, and attitude of cancer pain management in all oncology centers in Ethiopia.
Methods
Design and Setting
A nationwide cross-sectional survey was conducted from February 15 to April 30, 2019, in all cancer centers in Ethiopia. Currently, there are seven functional oncology centers located in the northern, southern, west and central regions of Ethiopia. The oncology centers of Ayder Referral Hospital, University of Gondar Comprehensive Specialized Teaching Hospital, Felege Hiwot Referral Hospital, Hawassa Referral Hospital, Jimma Referral Hospital, St. Paul Referral Hospital and Black Lion Specialized Hospital were areas of the study. Information regarding the study participants was obtained from the human resource management of each institution. There was an average of twenty nurses and a few specialist oncologists dedicated to curative and palliative care during the study period (Figure 1). We included all nurses (bachelor degree and above) working in each oncology center in the survey to have an adequate sample size. Nurses who were on annual leave and not interested in giving consent to participate in the study were excluded.
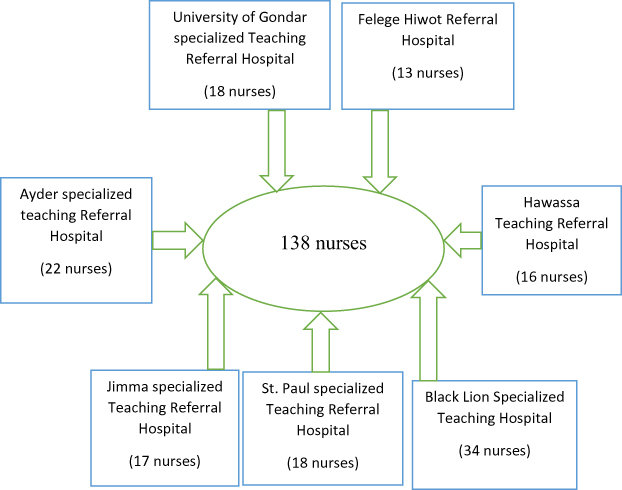 |
Figure 1 Flow diagram of study participant recruitment for the assessment of knowledge and attitude of Ethiopian nurses about cancer pain management. |
Study Variables
The outcome variable of this study was nurses’ knowledge and attitude about cancer pain management. The study participants who achieved a score of 80% or greater on nurses’ knowledge and attitude survey regarding pain survey were considered as having good knowledge and attitude whereas those who achieved a score of less than 80% on nurses’ knowledge and attitude survey regarding pain survey were considered as having poor knowledge and attitude.29,34,35
The independent variables were socio-demographic and work-related characteristics of nurses working in oncology centers.
Instrument
A self-administered questionnaire including socio-demographic variables and nurses Knowledge and attitude regarding pain survey (NKARP) tool was distributed to nurses working on all oncology units in Ethiopia. Even though English is a second language in Ethiopia, as the medium of instruction at all study areas of the institution was English. Therefore, the English version of a self-administered survey tool was used to collect data from the nurses. The importance and purpose of the study were stated on the first page of the questionnaire and further explanation was provided by the head nurse of each center. The questionnaire was handed to the head nurses of each oncology center, who undertake to give it to all nurses in the oncology wards who are starting the morning shift. They were instructed to keep the questionnaire anonymous. The questionnaire was completed quickly on the ward by the participants on their own, without consulting medical or nursing textbooks and then the questionnaire was returned to the head nurse.
The nurses’ knowledge and attitude survey regarding pain (NKASRP) tool developed by Ferrel, Betty and Mc Caffery which contained 22 true/false questions, 15 multiple-choice questions and two case studies with two questions each (a total of 41 questions).36 The content of the tool was established from standards of pain management from the American Pain Society (APS), World Health Organization (WHO), and Agency for Health Care Policy and Research (AHCPR). Construct validity of the original version was established by comparing scores of nurses at various levels of pain management expertise. Internal consistency for the English language version was reported at 0.70 and the test–retest reliability as 0.80.37
The scoring system of NKASRP is by analyzing the data in terms of the overall percentage of correct scores as well as in analyzing individual items. All items were equally weighted with the maximum possible score being 41. The correct responses were given a value of one and an incorrect or blank responses were given a value of zero.
Data Analysis and Interpretation
Epi-data and SPSS were used for data entry and analysis, respectively. Data were coded, entered, cleaned before statistical analysis. Descriptive statistics were carried out and the results were prepared using narrations, percentage and tables. Hosmer Lemeshow test was used for checking goodness of fit. Both bi-variable and multivariable binary logistic regression analyses were used to identify factors associated with knowledge and attitude level of nurses. Variables with a p-value of less than <0.2 in the bivariable analysis were fitted into the multivariable logistic regression analysis. Both crude odds ratio (COR) and adjusted odds ratio (AOR) with the corresponding 95% confidence interval were calculated to show the strength of association. In multivariable analysis, variables with a p-value of <0.05 were considered as statistically significant.
Results
Socio-Demographic and Work-Related Characteristics of Oncology Nurses
A total of 138 study participants were involved with the response rate of 99.3%. Only one participant was on annual leave during the study period and not included in the analysis of the study. The median age of the study participants was 28 years. 62.3% of the participants were female, and the majority (83.3%) of participants had a bachelor’s degree in nursing. 52.2% of the respondents had 1to 5 years of work experience. More than half (52.9%) of the study participants did not receive pain management training. Only 1.4% of study participants had personal cancer pain experience and 33.3% of participants had a friend or family member of the cancer pain experience. Most (81.9%) of study participants had a desire to attend pain management training in the future (Table 1).
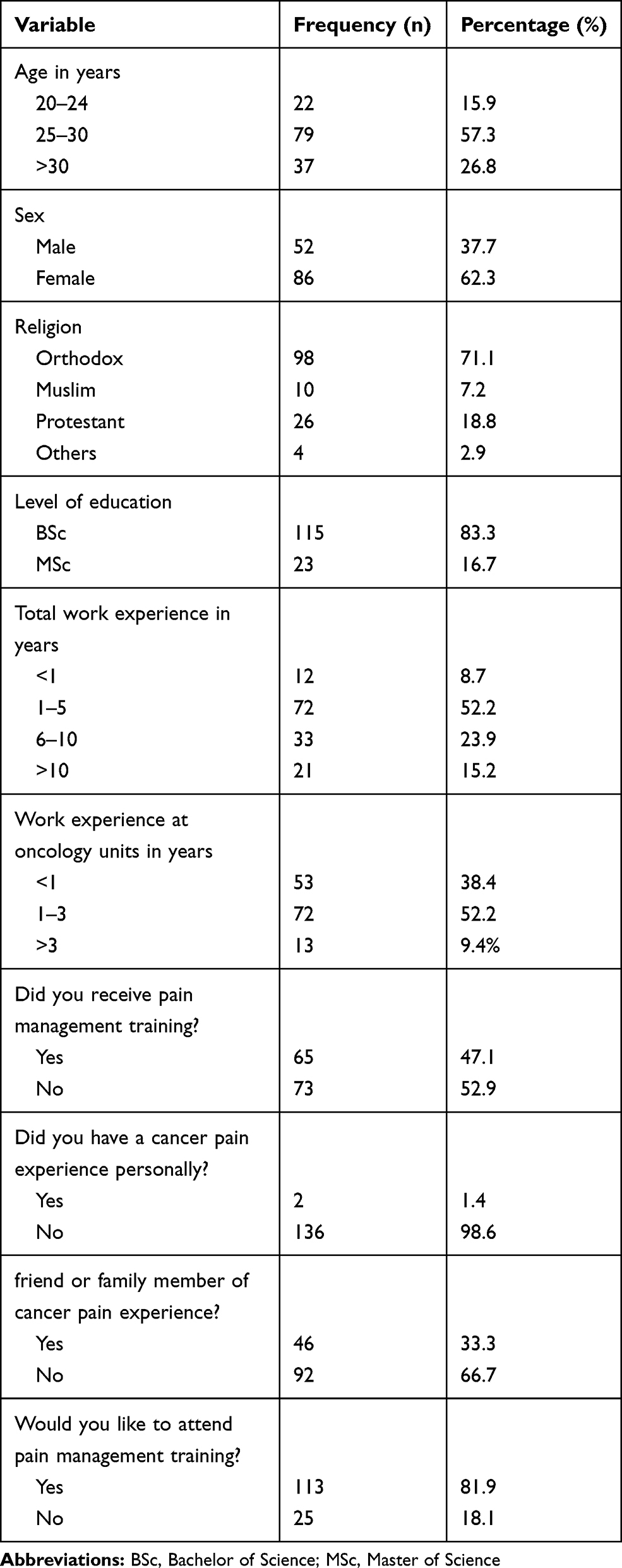 |
Table 1 Nurses’ Demographic and Work-Related Characteristics |
Knowledge and Attitude Level of Oncology Nurses About Cancer Pain Management
Overall, only ten of 138 (7.2%) oncology nurses scored above the cut-off point (80%) for good knowledge and attitude about cancer pain management. The mean (SD) knowledge and attitude score was 20.4 (5.13) and their correct item score ranged from 10.1% to 88.4% with an overall mean correct answer of 49.84%. The highest percentages of nurses responding to the correct answers were for items 21 (80.4%) and 25 (88.4%). Seven items had a correct answer rate of more than 70% of respondents. Nineteen items were correctly answered by less than 50% of the participants. 44.9% of nurses wrongly believed that placebo is a useful test to determine if the pain is real, and 77.5% of them were wrongly perceived that patients may develop a clinically significant respiratory depression if an opioid was administered. Only 51.4% of respondents knew that patients could request increasing doses of pain medication because of experiencing the increased intensity of pain, and 53.2% of them believed that the most accurate judge of the intensity of the patient’s pain is the patients themselves. Less than 25% of respondents correctly answered items 28 and 38 which are determinant of cancer pain management.
The analysis of the two case studies (38Aand39A) showed that 63% and 35.5% of nurses underestimated the patients’ pain in each case, respectively, and 33.3% of them underestimated the pain in both cases. Only 10.1% and 20.3% of respondents administered the correct dosage of morphine to relieve the pain, respectively (Table 2).
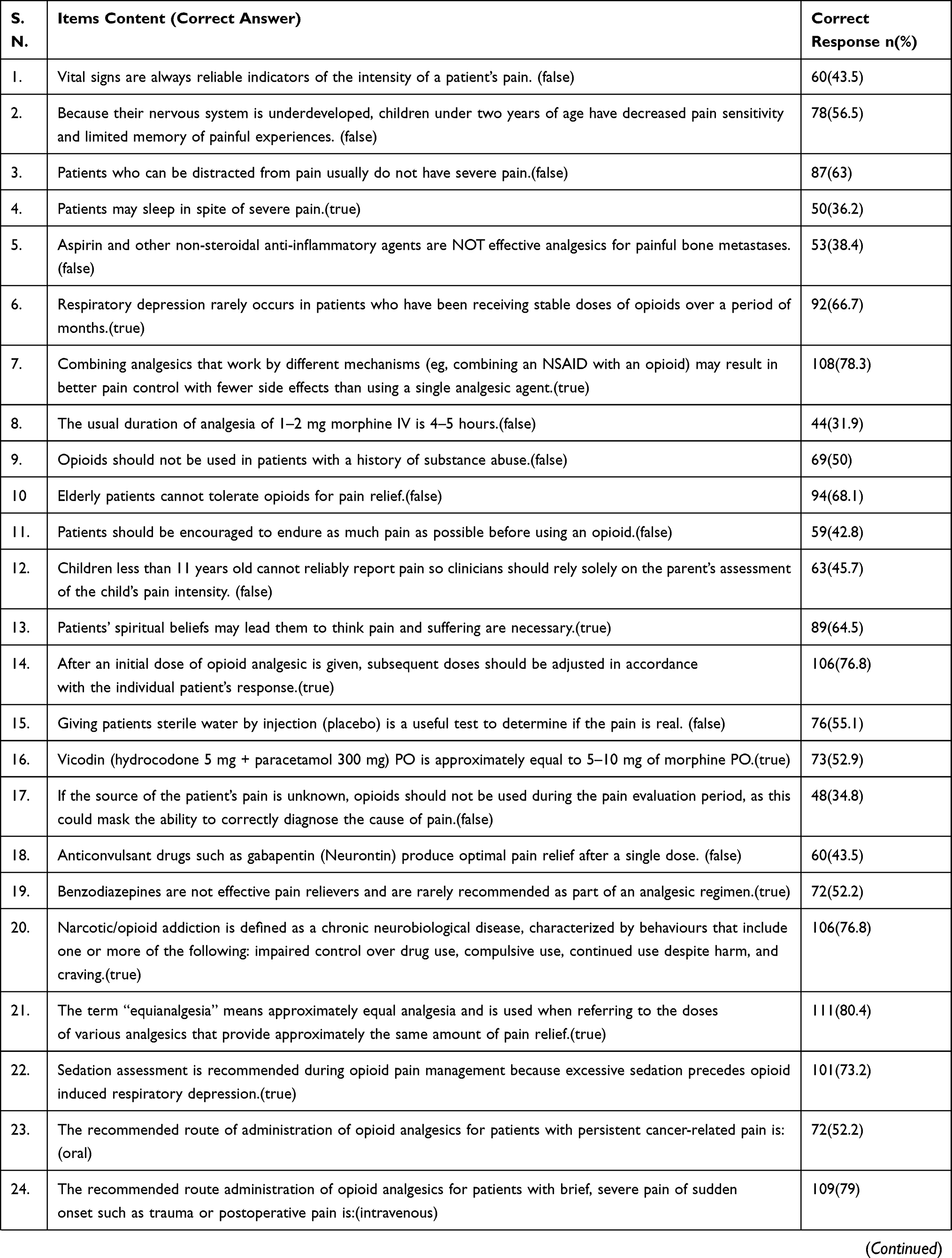 | 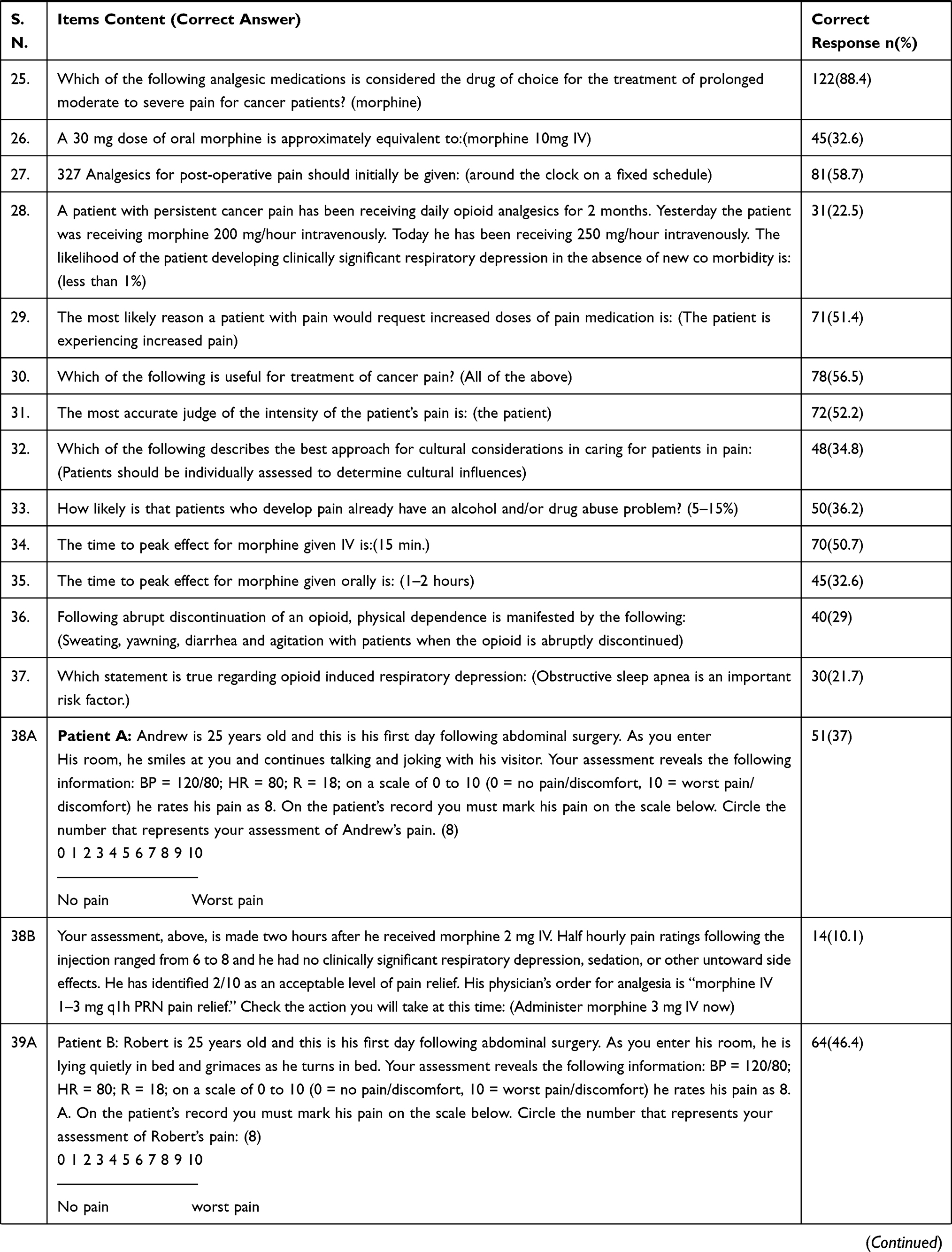 | 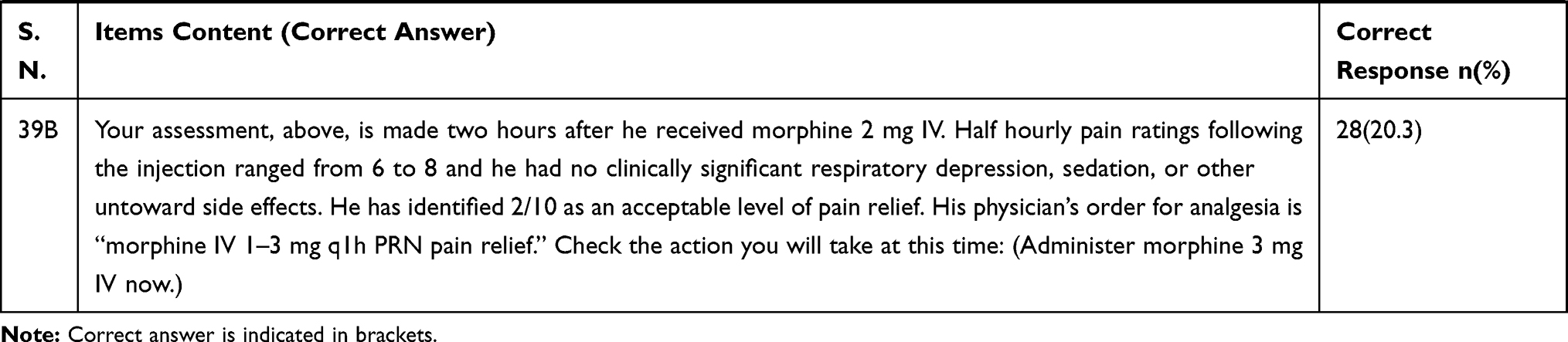 |
Table 2 Correct Answers for 41 Knowledge and Attitude Questions (N=138) |
Factors Associated with the Knowledge and Attitude of Oncology Nurses About Cancer Pain Management
On the bi-variable logistic regression analysis the level of education, sex of the respondent, and previous pain training were associated with the knowledge and attitude of nurses towards cancer pain management. In the multivariable logistic regression analysis, a significant association (AOR=5.57; CI = 1.12–19.73; P = 0.034) were found among nurses with their level of education. Those who had MSc in nursing were 4.7 times more likely to have good knowledge and attitude as compared to those who had a BSc degree. However, there was no significant knowledge and attitude level differences between male and female participants and those who had previous pain training in the multiple logistic regression analysis (Table 3).
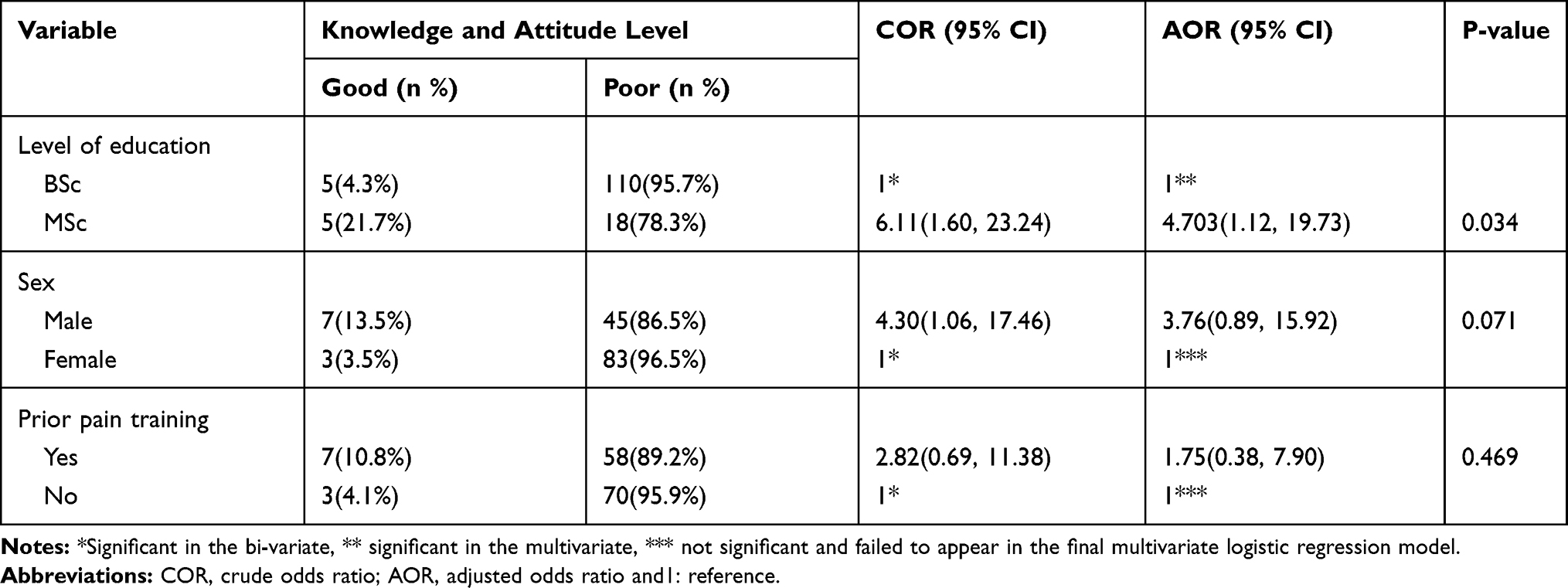 |
Table 3 Bivariate and Multivariate Logistic Regression Analyses of Factors Associated with Knowledge & Attitude of Oncology Nurses in Ethiopia, 2019 (N=138) |
Discussion
This study provides important evidence about the level of oncology nurses’ knowledge and attitude towards cancer pain management in Ethiopian oncology centers. Overall, there was inadequate knowledge and poor attitude about cancer pain management among nurses in Ethiopia. Only 7.2% (95% CI = 2.9–11.6) out of 138 oncology nurses had good knowledge and attitude about cancer pain management; indicating nurses continued to lack sufficient knowledge about pain management. This can be explained by the fact that lack of attention for pre-service and in-service pain education and training, as documented in previous literatures conducted in Ethiopia.38–41 For example, a study conducted among recently graduated paramedical students in Ethiopian universities reported that only 4.2% of the participants scored above the cutoff point (70%) for good knowledge regarding pain management with 49.8% mean score of correct answers.39 This shows an urgent need to start continuous quality improvement initiatives and include pain management training in the nursing curriculum to produce nurses who are competent to effectively control pain.
Among the 41 items examined, the mean knowledge and attitude score correctly answered was 20.43 (49.84% correct answer) in our study. This finding was consistent with similar studies conducted in Italy (21.4), Taiwan (18.52), and Jordan (19.3) which revealed that the total mean score of knowledge and attitude of nurses about cancer pain management was low.32,42,43 In contrast, studies conducted in the kingdom of Saudi Arabia and Turkey had lower mean scores (16.9 and 13.8) compared to our study.31,44 This difference probably indicates that the slight variation of assessment tools used. However, a similar study conducted using the same tool in Iran revealed that 18.9% of respondents had good knowledge and attitude with 28.5 correctly answered mean scores about cancer pain management which was higher than our findings. This discrepancy might be variation in the pain management education and training, sample size (62 participants), and overall experience of the study participants. A study conducted by Lewthwaite et al in Canada reported that nearly half of the nurses achieved a passing score of 80% or greater and there was a positive correlation between the knowledge and attitude score and educational level of study participants.35 This study did however use only the true or false item of nurses’ knowledge and attitude survey regarding pain tools, which made the score higher.
In the present study, items related to knowledge of pharmacologic pain medications (such as right dose, effect, and duration of drugs), preferred route of administration, and fear of addiction were incorrectly answered. These results are consistent with findings reported by earlier studies.45,46
Further analysis of the two case studies (38Aand39A) showed that nurses had inadequate knowledge of pain relief medication, particularly morphine. Sixty-three percent (n=87) and 35.5% (n=49) of nurses underestimated the patient’s pain in each case, respectively; and 33.3% (n=46) of nurses underestimated the pain in both cases. Only 10.1% (n=14) and 20.3% (n=28) of respondents, administered the correct dosage of morphine to relieve the pain of the two patients, respectively. This finding is very comparable with the result of similar study conducted in Italy42 which indicated that nurses underestimated the intensity of a patient’s pain and they did not believe in the pain reported by the patients. This shows nurses’ clinical reasoning about pain is complicated and may be highly influenced by the patient’s expression, position, and even by individual pain experiences.47
According to an experimental study done by Lavigne et al, pain perception remains active throughout all sleep stages.48 Therefore, patients may continue to experience pain despite being in sleep. In this study, only 36.2% of nurses correctly recognized that patients may sleep despite experiencing severe pain.
In this study, 44.9% of nurses could use a placebo to check whether the pain is real. This practice might indicate that nurses still devalued the patient’s self-reporting of pain and the application of nurses’ wrong attitude in their clinical practice. This result is in line with a study done in Jordan in which 46.4% of nurses may use a placebo during the clinical assessment of pain.43
Even though there are concerns regarding the safe administration of opioid analgesics to elderly patients, it can be tolerated in lower doses by geriatric patients. However, in this study, 31.9% of respondents, wrongly, believed that elderly patients cannot tolerate opioids for pain relief. This result is comparable with studies done in Iran and Jordan of which 32.2% and 35.1% of nurses, respectively, believed that elderly patients could not tolerate opioid analgesics.29,43
Even though children’s pain is affected by constant development, relatively limited cognitive ability, limited verbal skills, and limited behavioral competencies; they can report their pain. In this study, only 45.7% of oncology nurses believed that children can state their pain. This response was lower than studies conducted in Iran and Italy which were 63.7% and 74.9%, respectively.29,42 This showed that nurses do not believe that pain can be reported by children because they might think that children’s understanding of pain is limited and leads to under-treatment of pain.
In this study, 77.5% of nurses had an exaggerated concern about opioid-induced respiratory depression and in Taiwanese study, 84%32 and in Italy, 72.5%42 of respondents were concerned about opioid-induced respiratory depression which was comparable to the result of this study. This fear or concern, wrongly, may lead to the inadequate relief of patients from cancer pain.
One of the purposes of this study was to identify predictors of oncology nurses’ knowledge and attitude about cancer pain management. Age and sex of respondents, level of education, total work experience, oncology work experience and those who had the experience of cancer pain with a family member were analysed. Among all parameters, there was significant relationship between only knowledge and attitude and level of education. This finding was supported with the study done in Taiwan.32
The present study demonstrates that nurses who received previous pain training and those who had more work experience had not got significantly higher knowledge and attitude scores than those who did not receive previous pain training and those who had more work experience. This was inconsistent with results reported by earlier studies done in Taiwan, Italy and Jordan.32,42,43 This indicated that the more the nurses are educated through advanced training, the more they know about pain and its management. This discrepancy might be because of the difference in the number of study participants, duration of pain training and the tool they used.
A similar study conducted in Canada, with only true or false item of NKASRP, nurses having MSc holders had a high score and no significant correlations were found with nurses’ desire to learn more about pain which was in line with our study result. However, in contradiction to the result of our study; age, years of professional experience and BSc degree had a positive correlation with the knowledge and attitude level of nurses.35 This could be due to the differences in the number of study participants and they used only the true or false item of the tool.
The relationship between number of years working in oncology center on knowledge and attitude of nurses to manage cancer pain is unclear.49 Our study revealed that number of years working in oncology unit had no influence on the knowledge and attitude of nurses on cancer pain management. This was consistent with results reported by Bernardi et al and Wilson28,50 but it contradicts the findings of one study that reported years of working in oncology unit is influencing factor on nurses’ knowledge and attitudes regarding pain.46 However, the small sample size might not be enough to detect such a difference with the use of regression analysis. Further studies with larger samples that control for possible confounding variables (eg, training) might be required to explain this contradiction.
To the best of our knowledge, this is the first nationwide survey of all oncology nurses' pain knowledge and attitude in Ethiopia. The NKASRP is reliable and valid questionnaire that has been used by researchers in many countries. This study has high response rate, the findings really reflect the current status of oncology nurses’ knowledge and attitude towards cancer pain management in Ethiopia. However, there is some limitation in this study. The sample size was relatively small to effectively measure the knowledge and attitude level. Despite this limitation, the findings support that cancer pain and pain management issues should be further considered in nursing curriculum and continuing education program should further include contents about these issues to provide effective pain management.
Conclusion
In this survey study, the knowledge and attitude level of the majority of oncology nurses towards cancer pain management was poor which augments the universal concern of inadequate knowledge and attitudes regarding pain management. Nurses who had a master’s degree were significantly associated with good knowledge and attitude towards cancer pain management. Thus, regular cancer pain management training and revision of the academic curriculum of nursing education are necessary to enhance their knowledge and attitude.
Abbreviations
AHCPR, Agency for Health Care Policy and Research; AOR, adjusted odds ratio; APS, American Pain Society; BSc, Bachelor of Science; CI, confidence interval; COR, crude odds ratio; EAA, Ethiopian Association of Anesthetists; IQR, interquartile range; MSc, Master of Science; NKASRP, nurses’ knowledge and attitude survey regarding pain; PMP, pain management program; SD, standard deviation; SPSS, Statistical Packages for Social Science; WHO, World Health Organization.
Data Sharing Statement
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Ethics Approval and Consent to Participate
To conduct the current research, the ethical approval was obtained from Ethical Review Board of School of Medicine, College of Medicine and Health Sciences, University of Gondar (Ref.No. SOM/1182/2019). Permission letter from each institution and informed consent from each study participant were obtained. Potential ethical issues were addressed accordingly during the study period.
Acknowledgments
The authors would like to express their gratitude to oncology head nurses for support, and to the nurses who participated in the study. This study was fully funded by University of Gondar.
Author Contributions
All authors made substantial contributions to conception and design, acquisition of data, or analysis and interpretation of data; took part in drafting the article or revising it critically for important intellectual content; agreed to submit to the current journal; gave final approval of the version to be published; and agree to be accountable for all aspects of the work.
Disclosure
All authors declared that they have no competing interests.
References
1. Fitzmaurice C, Dicker D, Pain A, et al. The global burden of cancer 2013. JAMA oncol. 2015;1(4):505–527. doi:10.1001/jamaoncol.2015.0735
2. Fitzmaurice C, Allen C, Barber RM, et al. Global, regional, and national cancer incidence, mortality, years of life lost, years lived with disability, and disability-adjusted life-years for 32 cancer groups, 1990 to 2015: a systematic analysis for the global burden of disease study. JAMA oncol. 2017;3(4):524–548. doi:10.1001/jamaoncol.2016.5688
3. Torre LA, Bray F, Siegel RL, Ferlay J, Lortet‐Tieulent J, Jemal A. Global cancer statistics, 2012. CA Cancer J Clin. 2015;65(2):87–108.
4. Morhason-Bello IO, Odedina F, Rebbeck TR, et al. Challenges and opportunities in cancer control in Africa: a perspective from the African Organisation for Research and Training in Cancer. Lancet Oncol. 2013;14(4):e142–e51. doi:10.1016/S1470-2045(12)70482-5
5. Pisani P. The cancer burden and cancer control in developing countries. Environ Health. 2011;10(Suppl 1):S2. doi:10.1186/1476-069X-10-S1-S2
6. Li Z, Aninditha T, Griene B, et al. Burden of cancer pain in developing countries: a narrative literature review. Clinico Econ Outcomes Res. 2018;10:675. doi:10.2147/CEOR.S181192
7. Jemal A, Bray F, Forman D, et al. Cancer burden in Africa and opportunities for prevention. Cancer. 2012;118(18):4372–4384. doi:10.1002/cncr.27410
8. Stefan DC. Cancer care in Africa: an overview of resources. J Global Oncol. 2015;1(1):30–36. doi:10.1200/JGO.2015.000406
9. Memirie ST, Habtemariam MK, Asefa M, et al. Estimates of cancer incidence in Ethiopia in 2015 using population-based registry data. J Global Oncol. 2018;4:1–11. doi:10.1200/JGO.17.00175
10. Tigeneh W, Molla A, Abreha A, Assefa M. Pattern of cancer in Tikur Anbessa specialized hospital oncology center in Ethiopia from 1998 to 2010. Int J Cancer Res Mol Mech. 2015;1:1.
11. Nuland SB. Physician-assisted suicide and euthanasia in practice. Mass Medical Soc. 2000.
12. Kuuppelomäki M, Lauri S. Cancer patients’ reported experiences of suffering. Cancer Nurs. 1998;21(5):364–369. doi:10.1097/00002820-199810000-00008
13. Serlin RC, Mendoza TR, Nakamura Y, Edwards KR, Cleeland CS. When is cancer pain mild, moderate or severe? Grading pain severity by its interference with function. Pain. 1995;61(2):277–284.
14. Yaakup H, Eng TC, Shah SA. Does clinical experience help oncology nursing staff to deal with patient pain better than nurses from other disciplines? Knowledge and attitudes survey amongst nurses in a tertiary care in Malaysia. Asian Pac J Cancer Prev. 2014;15(12):4885–4891. doi:10.7314/APJCP.2014.15.12.4885
15. Eftekhar Z, Mohaghegh M, Yarandi F, et al. Knowledge and attitudes of physicians in Iran with regard to chronic cancer pain. Asian Pac J Cancer Prev. 2007;8(3):383.
16. Tegegn HG, Gebreyohannes EA. Cancer pain management and pain interference with daily functioning among cancer patients in Gondar University Hospital. Pain Res Manage. 2017;2017.
17. Harding R, Selman L, Agupio G, et al. The prevalence and burden of symptoms amongst cancer patients attending palliative care in two African countries. Eur J Cancer. 2011;47(1):51–56. doi:10.1016/j.ejca.2010.08.003
18. Bennett MI, Rayment C, Hjermstad M, Aass N, Caraceni A, Kaasa S. Prevalence and aetiology of neuropathic pain in cancer patients: a systematic review. Pain. 2012;153(2):359–365. doi:10.1016/j.pain.2011.10.028
19. Deandrea S, Corli O, Consonni D, Villani W, Greco MT, Apolone G. Prevalence of breakthrough cancer pain: a systematic review and a pooled analysis of published literature. J Pain Symptom Manage. 2014;47(1):57–76. doi:10.1016/j.jpainsymman.2013.02.015
20. Van Den Beuken-van MH, Hochstenbach LM, Joosten EA, Tjan-Heijnen VC, Janssen DJ. Update on prevalence of pain in patients with cancer: systematic review and meta-analysis. J Pain Symptom Manage. 2016;51(6):1070–90. e9. doi:10.1016/j.jpainsymman.2015.12.340
21. Getahun F, Mazengia F, Abuhay M, Birhanu Z. Comprehensive knowledge about cervical cancer is low among women in Northwest Ethiopia. BMC Cancer. 2013;13(1):2. doi:10.1186/1471-2407-13-2
22. Kassa RN, Kassa GM. Nurses’ attitude, practice and barrier s toward cancer pain management, Addis Ababa, Ethiopia. J Cancer Sci Ther. 2014;6(12):483–487.
23. Serawit Lakew HM, Shimeles T, Challinor J. Assessment of knowledge, accessibility and utilization of palliative care services among adult cancer patients at Tikur Anbesa Specialized Hospital, Addis Ababa, Ethiopia: a cross-sectional institution based study BMC Res Notes. 2015;8:657.
24. Breuer B, Fleishman SB, Cruciani RA, Portenoy RK. Medical oncologists’ attitudes and practice in cancer pain management: a national survey. J Clin Oncol. 2011;29(36):4769–4775. doi:10.1200/JCO.2011.35.0561
25. Fishman SM, Young HM, Lucas Arwood E, et al. Core competencies for pain management: results of an interprofessional consensus summit. Pain Med. 2013;14(7):971–981. doi:10.1111/pme.12107
26. Abdalrahim MS, Majali SA, Stomberg MW, Bergbom I. The effect of postoperative pain management program on improving nurses’ knowledge and attitudes toward pain. Nurse Educ Pract. 2011;11(4):250–255.
27. Chow K, Chan JC. Pain knowledge and attitudes of nursing students: a literature review. Nurse Educ Today. 2015;35(2):366–372. doi:10.1016/j.nedt.2014.10.019
28. Bernardi M, Catania G, Lambert A, Tridello G, Luzzani M. Knowledge and attitudes about cancer pain management: a national survey of Italian oncology nurses. Eur J Oncol Nurs. 2007;11(3):272–279.
29. Shahriary S, Shiryazdi SM, Shiryazdi SA, et al. Oncology nurses knowledge and attitudes regarding cancer pain management. Asian Pac J Cancer Prev. 2015;16(17):7501–7506. doi:10.7314/APJCP.2015.16.17.7501
30. Oldenmenger WH, Sillevis Smitt PA, van Dooren S, Stoter G, van der Rijt CC. A systematic review on barriers hindering adequate cancer pain management and interventions to reduce them: a critical appraisal. Eur J Cancer. 2009;45(8):1370–1380. doi:10.1016/j.ejca.2009.01.007
31. Yildirim YK, Cicek F, Uyar M. Knowledge and attitudes of Turkish oncology nurses about cancer pain management. Pain Manage Nurs. 2008;9(1):17–25. doi:10.1016/j.pmn.2007.09.002
32. Lai Y-H, Chen M-L, Tsai L-Y, et al. Are nurses prepared to manage cancer pain? A national survey of nurses’ knowledge about pain control in Taiwan. J Pain Symptom Manage. 2003;26(5):1016–1025. doi:10.1016/S0885-3924(03)00330-0
33. Howell D, Butler L, Vincent L, Watt–Watson J, Stearns N. Influencing nurses’ knowledge, attitudes, and practice in cancer pain management. Cancer Nurs. 2000;23(1):55–63. doi:10.1097/00002820-200002000-00009
34. McCaffery M, Robinson ES. Your patient is in pain—here’s how you respond. Nursing2018. 2002;32(10):36–45. doi:10.1097/00152193-200210000-00042
35. Lewthwaite BJ, Jabusch KM, Wheeler BJ, et al. Nurses’ knowledge and attitudes regarding pain management in hospitalized adults. J Continuing Educ Nurs. 2011;42(6):251–257. doi:10.3928/00220124-20110103-03
36. Rushton P, Eggett D, Sutherland CW, editors. Knowledge and Attitudes About Cancer Pain Management: A Comparison of Oncology and Nononcology Nurses. Oncology Nursing Forum; 2003.
37. Ferrell BR, McGuire DB, Donovan MI. Knowledge and beliefs regarding pain in a sample of nursing faculty. J Prof Nurs. 1993;9(2):79–88. doi:10.1016/8755-7223(93)90023-6
38. Tilahun Y, Nasrabadi A, Alemayehu M, Teklu A, Charania N. The journey of ethiopian nursing education: a glimpse of past, present and future. Int J Current Res. 2016;8:02.
39. Eyob T, Mulatu A, Abrha H. Knowledge and attitude towards pain management among medical and paramedical students of an Ethiopian University. J Pain Relief. 2013;3(127):2167–0846.1000127.
40. Eshete MT, Baeumler PI, Siebeck M, et al. The views of patients, healthcare professionals and hospital officials on barriers to and facilitators of quality pain management in Ethiopian hospitals: a qualitative study. PLoS One. 2019;14:3.
41. Germossa GN, Sjetne IS, Hellesø R. The impact of an in-service educational program on nurses’ knowledge and attitudes regarding pain management in an Ethiopian University Hospital. Front Public Health. 2018;6:229. doi:10.3389/fpubh.2018.00229
42. Bernardi M, Catania G, Lambert A, Tridello G, Luzzani M. Knowledge and attitudes about cancer pain management: a national survey of Italian oncology nurses. Eur J Oncol Nurs. 2007;11(3):272–279.
43. Al Qadire M, Al Khalaileh M. Jordanian nurses knowledge and attitude regarding pain management. Pain Manage Nurs. 2014;15(1):220–228. doi:10.1016/j.pmn.2012.08.006
44. Eid T, Manias E, Bucknall T, Almazrooa A. Nurses’ knowledge and attitudes regarding pain in Saudi Arabia. Pain Manage Nurs. 2014;15(4):e25–e36. doi:10.1016/j.pmn.2014.05.014
45. M Cg B, Lambert A, Tridello G, Luzzani M. Knowledge and attitudes about cancer pain management: A national survey of Italian oncology nurses. Eur J Oncol Nurses. 2007;11:272–279.
46. Yasemin Kuzeyli Yildirim P, Cicek F, Uyar M. Knowledge and Attitudes of Turkish Oncology nurses about cancer pain management. Pain Manage Nurs. 2008;9.
47. McCaffrey M, Ferrell BR. Nurses’ knowledge of pain assessment and management: how much progress have we made? J Pain Symptom Manage. 1997;14(3):175–188. doi:10.1016/S0885-3924(97)00170-X
48. Lavigne G, Brousseau M, Kato T, et al. Experimental pain perception remains equally active over all sleep stages. Pain. 2004;110(3):646–655. doi:10.1016/j.pain.2004.05.003
49. Patiraki-Kourbani E, Tafas CA, McDonald DD, Papathanassoglou ED, Katsaragakis S, Lemonidou C. Personal and professional pain experiences and pain management knowledge among Greek nurses. Int J Nurs Stud. 2004;41(4):345–354. doi:10.1016/j.ijnurstu.2003.10.007
50. W B. Nurses’ knowledge of pain. J Clin Nurs. 2007;16:1012–1020. doi:10.1111/j.1365-2702.2007.01692.x
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.