")
Back to Journals » Vascular Health and Risk Management » Volume 15
Knowledge and Associated Factors of Blood Pressure Control Among Hypertensive Patients Attending Chronic Illness Follow-Up Clinic at University of Gondar, Comprehensive Specialized Hospital, Northwest, Ethiopia
Authors Mekonnen CK , Mekonnen BY, Mekonnen HS
Received 3 August 2019
Accepted for publication 21 November 2019
Published 13 December 2019 Volume 2019:15 Pages 551—558
DOI https://doi.org/10.2147/VHRM.S225910
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Daniel Duprez
Chilot Kassa Mekonnen,1 Bezenaw Yimer Mekonnen,2 Habtamu Sewunet Mekonnen1
1Department of Medical Nursing, School of Nursing, College of Medicine and Health Sciences, University of Gondar, Gondar, Ethiopia; 2Department of Emergency and Critical Care Nursing, School of Nursing, College of Medicine and Health Sciences, University of Gondar, Gondar, Ethiopia
Correspondence: Chilot Kassa Mekonnen Email [email protected]
Introduction: As hypertension is a chronic cardiovascular disease that contributes to a high proportion of morbidity and mortality worldwide, favorable knowledge is crucial to control it.
Objective: The objective of this study was thus to assess knowledge and associated factors of blood pressure control among hypertensive patients at the chronic illness follow-up Clinic of the University of Gondar comprehensive-specialized hospital, Gondar, Ethiopia.
Methods: An institution-based cross-sectional study was conducted from March to April 2018. A systematic random sampling technique was used to select participants. Bi-variable and multivariable logistic regressions were done to assess the relationship between dependent and independent variables. The adjusted odds ratio with a 95% confidence interval was used to determine the presence and strength of association between covariates and the outcome variable.
Results: A total of 404 participants took part in the study with a response rate of 97.3%. The overall good knowledge about blood pressure control was 51.7% (95% CI=46.3–56.8). Females were 3.79 (AOR= 3.79, 95% CI: (1.55, 9.28)) more knowledgeable about blood pressure control than males. In the multivariable analysis, the odds of being knowledgeable were 2.80 (AOR= 2.80, 95% CI (1.44, 5.46)), 8.05 (AOR=8.05, 95% CI (2.93, 22.10)), and 7.53 (AOR=7.53, 95% CI (2.52, 22.49)) for can read and write, secondary, preparatory and above education, respectively, compared to cannot read and write. Occupation was significantly associated with the knowledge of plod pressure control. For example, merchants 7.66 (AOR=7.66, 95% CI (3.01, 19.47)), government employee 6.33 (AOR=6.33, 95% CI (1.90, 22.07)), and self-employed 4.58 (AOR=4.58, 95% CI (1.80, 11.70)) times more likely to be knowledgeable than farmers, respectively. Participants with family history of hypertension were 2.36 (AOR=2.36, 95% CI (1.42, 3.92)) times more knowledgeable than their counterparts.
Conclusion: In this study, knowledge of blood pressure control was lower compared to the finding of a study done at Bishoftu hospital, Ethiopia. But it is higher than studies in other African countries. Both pharmacological and non-pharmacological awareness is vital for blood pressure control.
Keywords: blood pressure control, hypertension, knowledge, Ethiopia
Introduction
Hypertension or high or raised blood pressure is one of the most common public health problems which is exceeding the epidemics of communicable diseases. It has been rising due to changes in lifestyle and increasing urbanization.1 It is a chronic cardiovascular disorder that contributes to heart disease, stroke, kidney failure, and premature mortality and disability. The prevalence of hypertension exceeds 1.3 billion worldwide.2 In Ethiopia, the prevalence increased from 17.7% in 2010 to 19.6% in 2015.2,3
According to the global brief report 2015, there were 3 in 10 deaths due to CVD (cardiovascular diseases), and half of all of the deaths were related to uncontrolled BP (Blood pressure). The WHO (World Health Organization) action plan for the prevention and control of NCDs (non-communicable diseases) is the reduction of raised blood pressure by 25%. However, the prevalence is still projected to be 60% and will reach 1.56 billion by 2025, with the largest proportion in low and middle-income countries.4,5
Good knowledge of blood pressure control was reported from Southern Iran (25.2%), Armenia (50.23%), Saudi Arabia (54.7%), Pakistan (55%), Brazil (82.3%), and India (27.68%).6–11 A study in India showed 43.6% of good knowledge about lifestyle modification regarding blood pressure control.12 Similarly, it was 14% in Cameron,13 47.1% in Nigeria,14 8.9% in Egypt6 and 61.39% in Addis Ababa, Ethiopia.7 In Nigeria, 32.7% of the participants were knowledgeable about the use of exercise to control blood pressure.8
Studies in various parts of the world revealed the association between BP control knowledge and age, sex, marital status, educational level, occupation, income, presence of chronic disease and duration of hypertension.9–11,15 Good knowledge of blood pressure control was associated with the level of education, duration of follow-up, access to information and sometimes with socioeconomic status.12,16 In Nigeria, secondary or tertiary education was significantly associated with the knowledge of self-monitoring and lifestyle modification to control BP.17,18
Addressing the knowledge of behavioral risk factors, like unhealthy diet, smoking, harmful use of alcohol, and physical inactivity can be crucial to prevent and control raised blood pressure.1 Although there have been studies on the prevalence of hypertension in Ethiopia, knowledge about BP control and associated factors were not well studied. Therefore, this study will determine the knowledge level and associated factors towards blood pressure control among hypertensive patients.
Methods
Study Design and Period
An institutional-based cross-sectional study was conducted on hypertensive patients from March to April 2018.
Setting
The study was conducted at Gondar University comprehensive-specialized hospital, northwest Ethiopia. The hospital is found in Gondar town, Amhara National Region State 735 km from Addis Ababa (the capital of Ethiopia) and is one of the teaching hospitals in the country serving around 7 million people both in and outside of the town. It has a follow-up clinic, for the major chronic illnesses, including hypertension, in the Department of Internal Medicine staffed with internists, internal medicine residents, interns, and nurses. There were on average of 848 hypertensive patients on follow-up in the clinic during the study.
Study Population
All adult hypertensive patients attending at chronic care follow-up clinic at Gondar University comprehensive-specialized hospital and had at least one follow-up during data collection. Patients who were seriously ill and had difficulty in communication were excluded.
Sample Size Determination and Sampling Procedure
The sample size was determined using the single population proportion formula with the assumption of a 95% level of confidence and a 5% marginal error. Since there were no similar studies in Ethiopia about the knowledge of both medical and non-medical control of blood pressure, 50% was assumed and yielded the required sample size of 404 with a 5% nonresponse rate.
Using systematic random sampling, every other participant was interviewed based on their order of arrival. To avoid the recycling of data’s special marks were used in patients’ medical charts and it was strengthened by verbal confirmation whether they participate or not in the previous consecutive data collection time.
Data Collection Tools and Procedures
Data were collected by using a structured interviewer-administered questionnaire prepared by reviewing related published studies15,19–22 that included socio-demographic, knowledge, and clinical characteristics. Knowledge about blood pressure control was measured by eight interviewers administered questions collected by four trained BSc degree graduate nurses. The data collected in 25–30 mins were computed by coding the correct responses as “1” and the incorrect ones as “0”. Then, the correct answers were added up and participants who scored the mean and above were labeled as having good knowledge (Additional file 1).
Data Quality Control
The questionnaire was pre-tested on 21 hypertensive patients a week before the actual data collection. Based on the findings of the pretest modifications were made on vague questions and the flow of the items. A one-day training was given to data collectors and supervisors. The data were checked for completeness during collection, entry and analysis.
Operational Definition
Knowledge was measured by calculating the mean score and categorized as “knowledgeable” if individuals scored the mean and above or “not knowledgeable” if they scored less than the mean.7
Data Processing and Analysis
The data were checked for completeness and coded before entry and Epi info version7 and SPSS version 20 were used for analysis. Descriptive statistics, including frequencies, percentages, means and standard deviations were used to describe the data. The binary logistic regression analysis was used, and variables with < 0.2 p-values were entered into the multivariable logistic regression for final analysis. Variables with a ≤ 0.05 p-values were considered statistically significant.
Result
Socio-Demographic and Clinical Characteristics
In the study, 404 hypertensive patients participated with a response rate of 97.3%. The mean age of respondents was 59.1 years (SD=±12.773). Over half, 212 (53.9%) and 232 (59.0%), of the respondents were male and urban dwellers, respectively; more than two-thirds (71.2%) were married, and 34.1% classified low economic status according to the principal component analysis (PCA). The major sources of information for 332 (84.5%) participants about healthy lifestyle to control BP were health professionals, followed by the mass media for 206 (52.4%). More than half of the participants 205 (52.2%), had 1–5 years of follow up. Participants with comorbidity were 87 (22.1%) (Table 1).
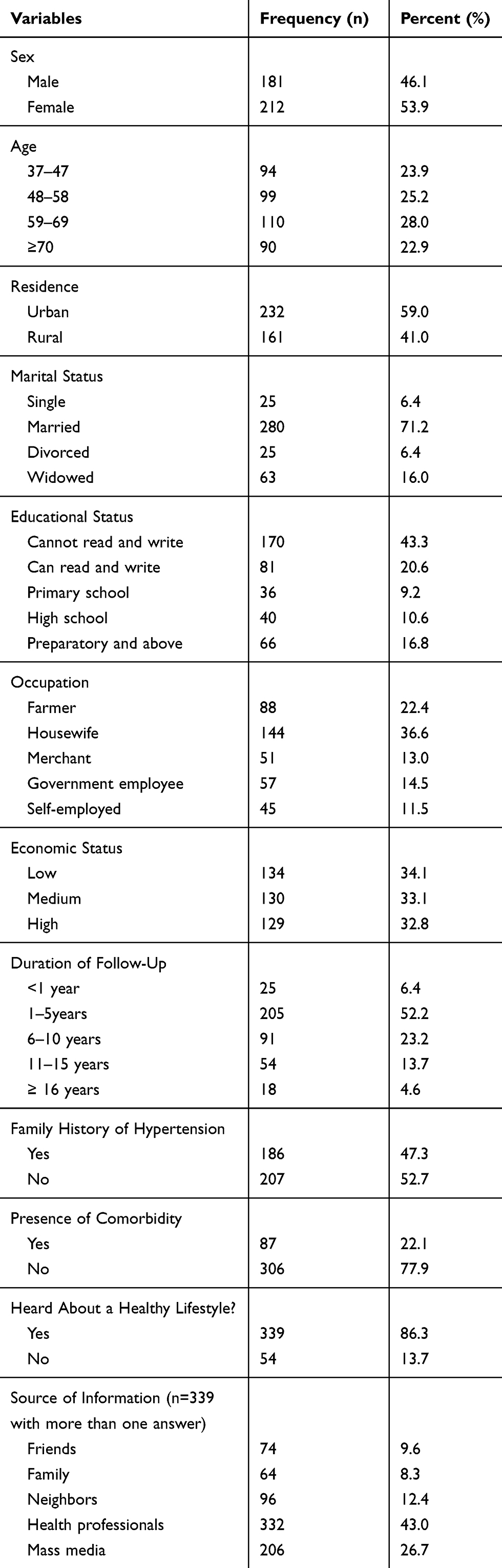 |
Table 1 Socio-Demographic and Clinical Characteristics of Participants Attending in Chronic Illness Follow-Up Clinic of Gondar University Comprehensive Specialized Hospital, Northwest, Ethiopia, 2018 (n=393) |
Knowledge About High Blood Pressure and Its Controls
Out of 393 participants, 203 (51.7%) of whom 125 (61.6%) had ≥ 5 years of follow-up were knowledgeable about the control. The mean (±SD) score for correctly answered knowledge questions was 17.695 (±6.261). Participants who correctly responded to the definition of increased blood pressure were 55.0%. Stress, smoking and alcohol consumption were identified as the risk factors for the problem by 78.8%, 45.7% and 44.6% of the respondents, respectively (Table 2).
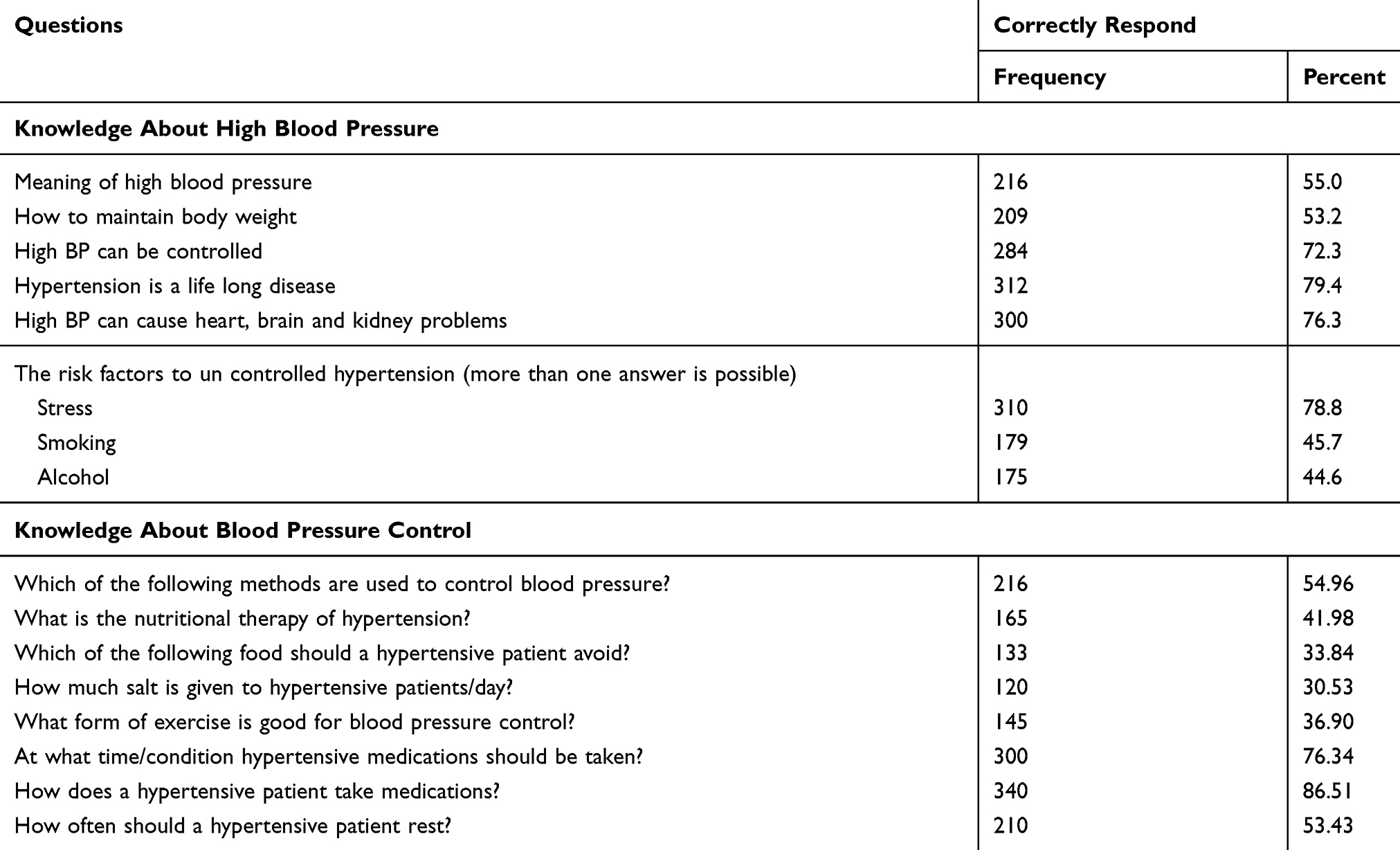 |
Table 2 Frequency Distribution of Knowledge Response About Blood Pressure and Its Control Among Hypertensive Patients Attending Chronic Illness Follow-Up Clinic, Gondar University Comprehensive Specialized Hospital, Northwest Ethiopia, 2018 (n=393) |
Knowledge About Signs and Symptoms
In the study, 76.9%, 53.8%, 53.1%, and 54.4% of the participants pointed out headache, dizziness, blurring of vision and fatigue as the signs and symptoms of high blood pressure, respectively. Only 9.5% of the participants failed to know the signs and symptoms of raised BP (Figure 1).
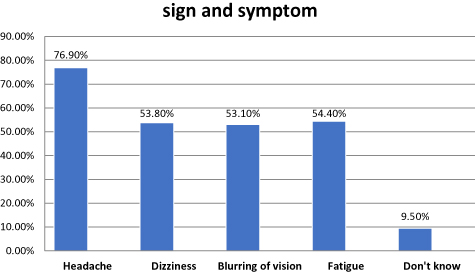 |
Figure 1 Knowledge of participants about signs and symptoms of high blood pressure (n=393). |
Factors Associated with Participant’s Knowledge of Blood Pressure Control
Sex, residence, level of education, occupation, family history of hypertension showed significant associations with knowledge of blood pressure control. Female participants were 3.79 (AOR= 3.79, 95% CI (1.55, 9.28)) more knowledgeable than males. Rural dwellers were 82% (AOR=0.18, 95% CI (0.11–0.98)) less knowledgeable than urban dwellers. The odds of being knowledgeable were 2.80 (AOR= 2.80, 95% CI (1.44, 5.46)), 8.05 (AOR=8.05, 95% CI (2.93, 22.10)), and 7.53 (AOR=7.53, 95% CI (2.52, 22.49)) more likely among participants who had read and write, secondary school, and preparatory and above educational status compared to cannot read and write group, respectively. In this work, occupation was significantly associated with knowledge. Merchants 7.66 (AOR=7.66, 95% CI (3.01, 19.47)), government employees 6.33 (AOR= 6.33, 95% CI (1.90, 22.07)), and the self-employed were 4.58 (AOR=4.58, 95% CI (1.80, 11.70)) times more likely to be knowledgeable compared with farmers, respectively. Respondents with family history of hypertension were 2.36 (AOR=2.36, 95% CI (1.42, 3.92)) times more likely to be knowledgeable than their counterparts (Table 3).
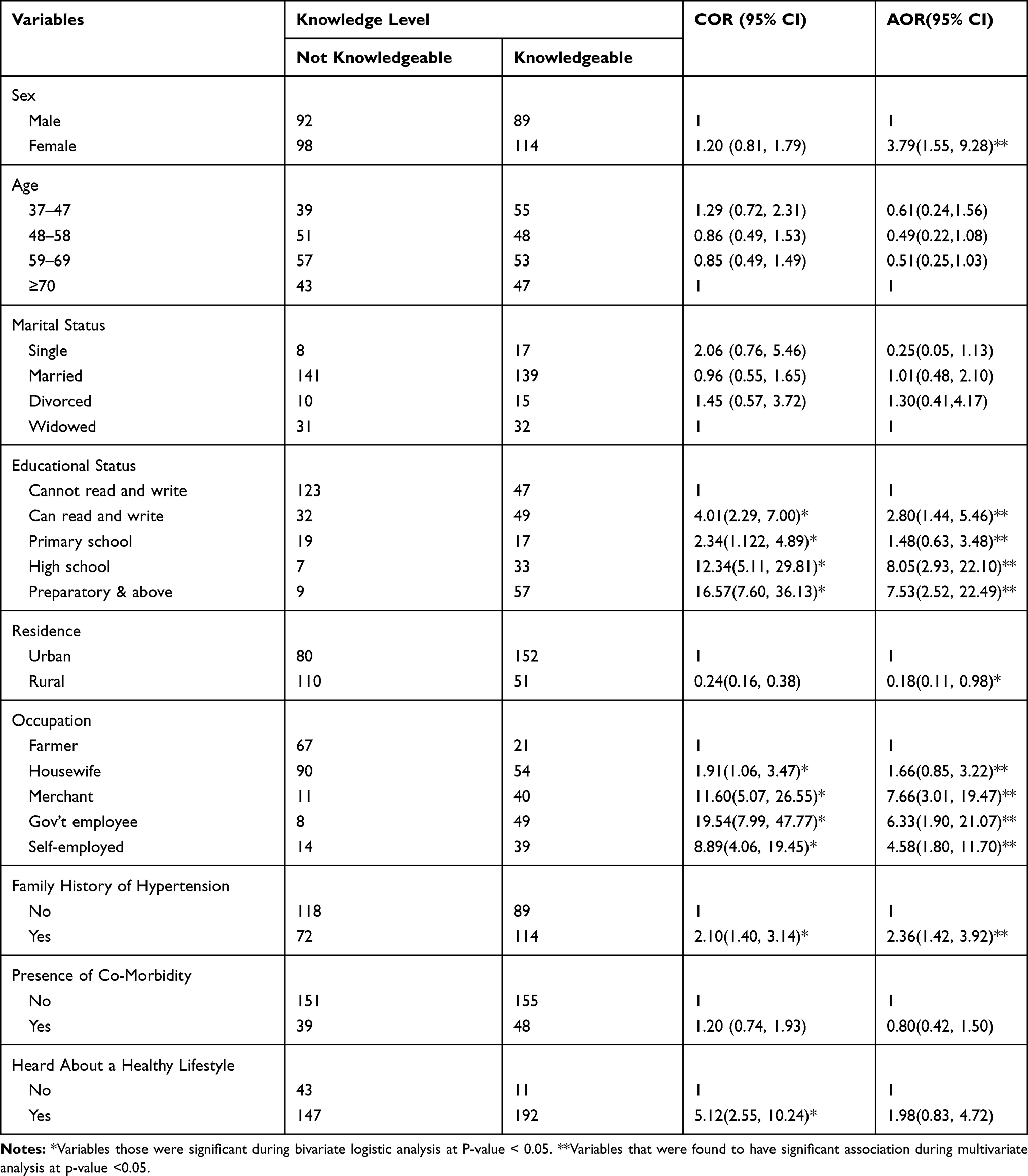 |
Table 3 Univariate and Multivariate Analysis for Knowledge Towards Blood Pressure Control Among Hypertensive Patients Attending Chronic Illness Follow-Up Clinic, Gondar University Comprehensive Specialized Hospital, Northwest Ethiopia, 2018 (n=393) |
Discussion
The current study showed that more than half of the participants, 51.7% (95% CI = 46.8–56.8), were knowledgeable about blood pressure control. This finding is in line with those of studies conducted in Saudi Arabia (52%), Armenia (50.23%), India (52.5%), and Pakistan (55.0%).15,21,23,24
The finding was lower than those of studies done in Bishoftu (72.27%), and Brazil (82.3%).7,25 The difference might be that the study in Bishoftu was only on non-pharmacological blood pressure control, and the majority of the participants were urban dwellers. On the other hand, the study in Brazil was community-based with a convenient sampling. Our finding is higher than the results of studies done in Iran (25.6%), Karnataka (41.61%), another study in India (27.7%), Nigeria (47.1%), Cameroon (14.0%), and another study in Nigeria (43.6%).13,14,20,26,27 The difference might be due to variations in sociodemographic characteristics of participants and the type of health facilities. The current study was done in a compressive-specialized hospital, but the comparative studies were carried out in health facilities including the health centers.
This study showed that 54.96% of the participants correctly answered the questions on blood pressure control methods. In Ghana, however, 87.0%, 64.2% and 54.0% of the participants correctly identified drugs, diets, and exercises as methods of blood pressure control, respectively.28 Similarly, in Samarkand State Medical Institute 71.3% and 51.7% of the participants knew that medicine was the most important factor in controlling BP and that eating less salt usually made BP lower, respectively.29
In this study, sex, family history of hypertension, education, occupation, and residence were factors associated with blood pressure control knowledge. Females were 3.79 (AOR= 3.79, 95% CI (1.55, 9.28)) times more knowledgeable about blood pressure control than males. In the cross-tabulation of sex and educational status, females had a higher educational status than males. Participants with more education could have a better understanding and can easily access information. So, the significant association of females with knowledge might be related to this fact. However, in Southern Iran, the level of knowledge about hypertension and its control was higher among males (27.1%) compared to females (23.9%).30 Respondents with family history of hypertension were 2.36 (AOR=2.36, 95% CI (1.42, 3.92)) times more knowledgeable compared to their counterparts. These findings were supported by studies conducted in Armenia and China and reported that family history had a high chance of making knowledgeable.9,15 This was however inconsistent with study conducted in South Iran and reported that family history was not a significant predictor of knowledge about blood pressure control.27
The odds of being knowledgeable about the control of blood pressure among the “can read and write”, and those who had primary, secondary, and preparatory school and above educational status were 2.8, 1.4, 8.05, and 7.53 times better, respectively, compared with the “can’t read and write”. Educated individuals could access information about blood pressure control mechanisms through content materials, like leaflets and manuals which might make them aware of BP control. They can also easily communicate with health care providers when they have doubts. The finding is supported by a study in Iran in which the proportion of the control of hypertension was higher among the educated compared with not educated.30
Rural residence decreased the chance of being knowledgeable by 82% (AOR=0.18, 95% CI (0.11–0.98)) compared to urban dwellings because rural dwellers had less access to the media and reading materials since most of them could not read and write. A study in India showed rural residence was associated with greater losses from hypertension follow-up care.31 Compared to farming, government employment increased the chances of being knowledgeable six-fold. This was supported by a study conducted in Ghana in which respondents who were employed scored better than the unemployed in knowledge.32
Conclusion and Recommendation
The knowledge of blood pressure control in this study was lower compared to the finding of a study done in Bishoftu, Ethiopia. But it was higher than those of studies in other African countries. Measures need to be taken to improve the pharmacological and non-pharmacological knowledge of participants so they could control their BP. Perhaps, future qualitative studies are necessary for detailed understanding of the problem and suggesting informed remedies.
Strengths and Limitations
To the best of our knowledge, the study has comprehensively evaluated HTN control knowledge among patients. However, it is an institution-based study that might not be generalized to the public. Besides, it has not assessed the blood pressure level of the participants in terms of their own knowledge.
Abbreviations
AOR, adjusted odds ratio; BP, blood pressure; CVD, cardiovascular disease; CI, confidence interval; COR, crude odds ratio; NCDs, non-communicable diseases; SD, standard deviation; SPSS, statistical package for social sciences; WHO, World Health Organization.
Ethics Statement
The study was approved by the University of Gondar College of Medicine and Health Sciences School of nursing Research and Ethical Review Committee. Permission and supportive letters were obtained from the head of each health center. Each study participant was informed about the purpose, method, expected benefit, and risk of the study. They were also informed about their full right not to participate or withdraw from the study at any time, and deciding not to participate had no impact on their services. Written informed consent was obtained from study participants and anonymity was employed to maintained confidentiality. For participants who could not read and write, a thumbprint was used in place of participants' signature. The study has been performed following the ethical standards laid down in the 1964 Declaration of Helsinki.
Acknowledgment
The authors would like to express our gratitude to the University of Gondar College of Medicine and Health Science School of Nursing Research and Ethical Review Committee for the approval of the ethical clearance. The authors would like to thank data collectors and supervisors for their commitment and the study participants for their valuable information.
Author Contributions
CKM wrote the proposal, participated in data collection, analyzed the data and drafted the manuscript. BYM and HSM approved the proposal with revisions, participated in data collection, data analysis and revised subsequent drafts of the manuscript. All authors contributed to data analysis, drafting or revising the article, gave final approval of the version to be published, and agree to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Demaio AR, Otgontuya D, de Courten M, et al. Hypertension and hypertension-related disease in mongolia; findings of a national knowledge, attitudes and practices study. BMC Public Health. 2013;13(1):194. doi:10.1186/1471-2458-13-194
2. Adeloye D, Basquill C. Estimating the prevalence and awareness rates of hypertension in Africa: a systematic analysis. PLoS One. 2014;9:8.
3. Kibret KT, Mesfin YM. Prevalence of hypertension in Ethiopia: a systematic meta-analysis. Public Health Rev. 2015;36:14. doi:10.1186/s40985-015-0014-z
4. Adler AJ, Prabhakaran D, Bovet P, et al. Reducing cardiovascular mortality through prevention and management of raised blood pressure. Glob Heart. 2015;10(2):111–122. doi:10.1016/j.gheart.2015.04.006
5. Whelton PK, Carey RM, Aronow WS, et al. 2017 Guideline for the prevention, detection, evaluation, and management of high blood pressure in adults: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines.J Am Coll Cardiol. 2018;71:e127–e248.
6. Seham A AE-H, El Mezayen SE. Knowledge and perceptions related to hypertension, lifestyle behavior modifications and challenges that facing hypertensive patients. IOSR J NursHealth Sci Ver I. 2015;4(6):15–26.
7. Daniel D, Rathore Kamal S. Assessment of knowledge, attitude and practice of hypertensive patients towards the non- medical management of hypertension in Bishoftu General Hospital. Pharm Chem J. 2017;4(1):48–59.
8. Awotidebe T, Adedoyin R, Rasaq W, et al. Knowledge, attitude and practice of exercise for blood pressure control: a cross-sectional survey. J Exerc Sci Physiol. 2014;10(1):1. doi:10.18376/2014/v10i1/67243
9. Li X, Ning N, Hao Y, et al. Health literacy in rural areas of China: hypertension knowledge survey. Int J Environ Res Public Health. 2013;10(3):1125–1138. doi:10.3390/ijerph10031125
10. Bakhsh LA, Adas AA, Murad MA, et al. Awareness and knowledge on hypertension and its self- care practices among hypertensive patients in Saudi Arabia. Ann Int Med Dent Res. 2017;2(5). doi:10.21276/aimdr.
11. Zinat Motlagh SF, Chaman R, Ghafari SR, et al. Knowledge, treatment, control, and risk factors for hypertension among adults in Southern Iran. Int J Hypertens. 2015;2015:1–8. doi:10.1155/2015/897070
12. Patnaik L, Paul KK, Pattnaik S, Sahu T. Lifestyle pattern and hypertension related knowledge, attitude and practices among diagnosed patients of hypertension attending a tertiary care hospital. J Cardiovasc Dis Res. 2017;8(4):108–111. doi:10.5530/jcdr
13. Akoko BM, Fon PN, Ngu RC, Ngu KB. Knowledge of hypertension and compliance with therapy among hypertensive patients in the Bamenda Health District of Cameroon: a cross-sectional study. Cardiol Ther. 2017;6(1):53–67. doi:10.1007/s40119-016-0079-x
14. Busari OA, Oluyombo R, Fasae AJ, Gabriel E, Ayodele LM, Agboola SM. Prescribing pattern and utilization of antihypertensive drugs and blood pressure control in adult patients with systemic hypertension in a rural tertiary hospital in Nigeria. Am J Inter Med. 2014;2(6):144–149.
15. Tadevosyan A. knowledge, Attitude and Practice of hypertensive people in American University of Armenia. 2013;p13–17.
16. Shaikh MA, Dur-e-Yakta S, Kumar R. Hypertension knowledge, attitude and practice in adult hypertensive patients at LUMHS. J Liaquat Uni Med Health Sci. 2012;11(2):113–116.
17. Ambakederemo T, Ebuenyi I, Jumbo J. Knowledge and attitude to self-monitoring of blood pressure in a cardiology clinic in Nigeria. IOSR J Dent Med Sci. 2014;13(5):63–65.
18. Ike S, Aniebue P, Aniebue U. Knowledge, perception and practices of lifestyle—modification measures among adult hypertensive in Nigeria. Royal Soc Trop Med Hyg. 2010;104:55–60. doi:10.1016/j.trstmh.2009.07.029
19. Buda ES, Hanfore LK, Fite RO, Buda AS. Lifestyle modification practice and associated factors among diagnosed hypertensive patients in selected hospitals, South Ethiopia. Clin Hypertens. 2017;23(1):26. doi:10.1186/s40885-017-0081-1
20. Ahmad S, Ahmad T. Assessment of knowledge, attitude and practice among hypertensive patients attending a health care facility in North India. Indian J Basic Appl Med Res. 2015;4(3):501–509.
21. Bollampally M, Chandershekhar P, Kumar K, Surakasula A, Srikanth S, Reddy T. Assessment of patient’s knowledge, attitude and practice regarding hypertension. Int J Res Med Sci. 2016;3299–3304. doi:10.18203/2320-6012.
22. Rashidi Y, Manaflouyan H, Pournaghi Azar F, Nikniaz Z, Nikniaz L, Ghaffari S. Knowledge, attitude and practice of Iranian hypertensive patients regarding hypertension. J Cardiovasc Thorac Res. 2018;10(1):14–19. doi:10.15171/jcvtr.2018.02
23. Elkheshen A, Billah M, Shahbaz A, Zarghamravanbakhsh P, Nabi U, Sachmechi I. A rare case report of extra-adrenal pheochromocytoma with normal blood pressure: is that possible? Cureus. 2018;10(8):e3167.
24. Almas A, Godil SS, Lalani S, Samani ZA, Hameed A. Good knowledge about hypertension is linked to better control of hypertension; a multicentre cross sectional study in Karachi, Pakistan. BMC Res Notes. 2017;24(5):579.
25. Barreto MDS, Reiners AAO, Marcon SS. Knowledge about hypertension and factors associated with the non-adherence to drug therapy. Rev Lat Am Enfermagem. 2014;22(3):491–498. doi:10.1590/0104-1169.3447.2442
26. Binu K, Jose R, Sarfarz M, Doddayya H, Antin S. Assessment of knowledge, attitude and medication taking behaviour of hypertensive patients in a tertiary care teaching hospital. WJPPS. 2017;6(6):966–975.
27. Motlagh Z, Fazel S, Chaman R, et al. Knowledge, treatment, control, and risk factors for hypertension among adults in southern Iran. Int J Hypertens. 2015;2015.
28. Anowie F, Darkwa S. The knowledge, attitudes and lifestyle practices of hypertensive patients in the cape coast metropolis-Ghana. J Sci Res Rep. 2015;8(7):1–15. doi:10.9734/JSRR/2015/19891
29. Malik A, Yoshida Y, Erkin T, Salim D, Hamajima N. Hypertension-related knowledge, practice and drug adherence among inpatients of a hospital in samarkand, uzbekistan. Nagoya J Med Sci. 2014;76:255–263.
30. Fazel S, Motlagh Z, Chaman R, et al. Knowledge, treatment, control, and risk factors for hypertension among adults in Southern Iran. Int J Hypertens. 2015.
31. Prenissl J, Manne-Goehler J, Jaacks LM, et al. Hypertension screening,awareness, treatment, and control in India: a nationally representative cross-sectional study among individuals aged 15 to 49 years. PLoS Med. 2019;16(5):e1002801. doi:10.1371/journal.pmed.1002801
32. Anowie F, Darkwa S. The knowledge, attitudes and lifestyle practices of hypertensive patients in the cape coast metropolis-Ghana. J Sci Res Rep. 2016;8(7):1–15. doi:10.9734/JSRR
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.