")
Back to Journals » Patient Preference and Adherence » Volume 16
“It Was Very Comforting to Find Out Right Away.” – Patient Perspectives on Point-of-Care Molecular SARS-CoV-2 Testing in Primary Care
Authors Matthes A , Wolf F, Bleidorn J, Markwart R
Received 26 April 2022
Accepted for publication 16 July 2022
Published 10 August 2022 Volume 2022:16 Pages 2031—2039
DOI https://doi.org/10.2147/PPA.S372366
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Johnny Chen
Anni Matthes,1,2 Florian Wolf,1 Jutta Bleidorn,1 Robby Markwart1,2
1Institute of General Practice and Family Medicine, Jena University Hospital, Friedrich Schiller University, Jena, Thuringia, Germany; 2InfectoGnostics Research Campus Jena, Jena, Thuringia, Germany
Correspondence: Anni Matthes, Institute of General Practice and Family Medicine, Jena University Hospital, Friedrich Schiller University, Bachstr. 18, Jena, Thuringia, 07743, Germany, Tel +49 3641 939 5824, Fax +49 3641 939 5802, Email [email protected]
Background: The use of point-of-care tests (POCTs) has been a central strategy to cope with the COVID-19 pandemic. Yet, evidence on the application and consequences of POCTs within medical settings is rare.
Purpose: To assess and understand patient perspectives on molecular point-of-care SARS-CoV-2 testing conducted in primary care.
Methods: We conducted a cross-sectional survey study among patients who were tested with a molecular SARS-CoV-2 rapid test (ID NOWTM COVID-19 rapid test, Abbott) in 13 primary care practices in the state of Thuringia (Germany) from February to April 2021. The following aspects were covered in the questionnaire through rating scales and open text formats: test characteristics, trust in test result, consequences of immediate result, cost amount willing to pay and expectations in the future. Open text answers were categorized; quantitative data were analyzed using descriptive statistics and a Mann–Whitney U-test to reveal differences in cost contribution depending on the test result.
Results: A total of 215 patients from nine family practices and one pediatric practice participated. The immediate availability of the test result was important to the majority of patients (94.3%). 95.7% of patients trusted in their test result. Personal consequences of the immediate test result referred to pandemic measures, certainty of action and reassurance. For further tests, patients were willing to pay between 0€ and 100€ (interquartile range = 10– 25€) for the molecular SARS-CoV-2 POCT, regardless of the test result. Expectations of being offered the test again in case of renewed cold symptoms were reported by 96.2%.
Conclusion: Patients highly appreciated molecular SARS-CoV-2 rapid testing conducted in primary care practices. The immediate availability of the test result led to adjustments in patients’ behavior and emotional wellbeing. However, potentially challenging for the implementation of POCTs in primary care practices may be the reimbursement of test costs and patients’ expectations in future situation.
Keywords: POCT, rapid test, COVID-19, acceptance, feasibility
Introduction
Point-of-care tests (POCTs), also known as rapid tests, are in-vitro diagnostic laboratory tests, which are performed in close proximity to the patient and yield test results usually within 30 minutes.1,2 During the COVID-19 pandemic, the public became accustomed to POCTs due to the use of SARS-CoV-2 rapid tests in healthcare facilities and home use. Since April 2021, the use of rapid SARS-CoV-2 antigen tests has been a cornerstone in the German national strategy to cope with the pandemic.3 Besides rapid antigen tests for detecting acute SARS-CoV-2 infections (usually lateral flow assays),4 molecular SARS-CoV-2 POCTs based on nucleic acid amplification techniques with superior diagnostic accuracy have been developed.5,6 However, laboratory testing using the real-time quantitative reverse transcription–polymerase chain reaction (RT-qPCR) technology remains the gold standard in the diagnosis of acute SARS-CoV-2 infection.7 A positive test result has far-reaching consequences for patients and their social network such as quarantine. The rapid availability of the test result could be of particular importance in the context of a disease like COVID-19, which possesses a significant public health relevance. In addition to the perspectives of medical professionals, the attitude of patients is one important factor in the successful implementation of medical intervention, including diagnostic procedures, in routine healthcare.
In the primary care setting, POCTs should support clinical decision-making, for both patients and physicians.8 While point-of-care measurement of certain laboratory markers is already established in primary care (eg C-reactive protein, D-Dimer, urine dipstick), the development of novel POCTs is omnipresent. Horvath et al9 defined key components that should be analyzed in the evaluation of diagnostic tests: analytical and clinical performances, clinical and cost-effectiveness and the broader impact of the test on social, psychological, or organizational consequences (such as patient scheduling, practice management, etc.) in a specific clinical setting. As shown by a review of 40 evaluation reports, the evaluation of novel POCTs targeted for primary care often focused on the diagnostic performance, while evidence gaps exist for the clinical effectiveness and the broader impact of POCTs (eg feasibility, acceptance, costs).10 In order to strengthen the evidence on social, psychological, or organizational consequences of POCTs, it is essential to investigate the perspectives of the actual test users (medical staff) and patients on whom the tests are performed.
The aim of this study was to assess and understand patient perspectives on molecular point-of-care SARS-CoV-2 testing performed in German primary care practices during a COVID-19 infection wave.
Methods
Study Design
We conducted a descriptive cross-sectional questionnaire-based survey study among patients on whom a molecular SARS-CoV-2 rapid test (ID NOWTM COVID-19 rapid test, Abbott Diagnostics Scarborough, Inc., USA) was performed. The study was conducted in 13 primary care practices in the German federal state of Thuringia from February 15th to April 26th 2021 when the 7-day incidence ranged between 100 and 200 new SARS-CoV-2 cases per 100,000 inhabitants.11 In our study, patients included all persons who presented at primary care practices with a suspected SARS-CoV-2 infection. The patients’ perspectives on the following aspects were evaluated: test characteristics, trust in test result, consequences of immediate result, cost amount willing to pay and expectations in the future. The Association of Statutory Health Insurance Physicians Thuringia (The Association of Statutory Health Insurance Physicians Thuringia is a body under public law and represents all outpatient physicians and psychotherapists in the German federal state of Thuringia. It is part of the medical self government and organizes all processes in outpatient medical care of patients insured by the statutory health insurances (Social Security Code (SGB V), § 77)) initiated the study and recruited primary care practices, which were known to be interested in research projects. The analyzer platform and test kits were provided by the manufacturer. By contract between manufacturer and the Association of Statutory Health Insurance Physicians Thuringia, the manufacturer was not involved in study design, implementation and analysis. Evaluation was performed independently without financial remuneration.
During the study period, the use of the molecular SARS-CoV-2 rapid test was restricted to diagnostic testing of patients with typical COVID-19 symptoms (eg cough, loss of taste or smell). Physicians had free choice whether SARS-CoV-2 testing was performed and if so, which test was used (laboratory PCR testing or POCT testing). Patients were informed about the nature of the molecular SARS-CoV-2 rapid test by the practice staff. After the test was performed and results were communicated to the patients, they were asked to participate in the study by answering the written questionnaire. The study complies with the declaration of Helsinki. Ethical approval was obtained from the Institutional Research Ethics Board of the Jena University Hospital (Registration No.: 2021–2108-Bef).
Molecular SARS-CoV-2 Rapid Testing
The used molecular SARS-CoV-2 rapid test (ID NOWTM COVID-19 rapid test) is based on the isothermal nucleic acid amplification technique for qualitative detection of viruses nucleic acids from nasopharyngeal swabs.12 According to the manufacturers’ information, the diagnostic sensitivity and specificity are 95.0% and 97.9%, respectively.13 However, an independent Cochrane review showed that the average sensitivity was 73.0%, while the specificity was 99.7%.14 As shown by several studies,15–17 the sensitivity of the ID NOW™ COVID-19 rapid test is particularly decreased in samples with low viral loads, but at high viral loads (corresponding to symptomatic patients), the diagnostic accuracy of the ID NOWTM is comparable to laboratory RT-qPCR testing. In January 2021, local health authorities in the federal state of Thuringia have officially approved the results of the ID NOWTM COVID-19 rapid test as confirmation/non-confirmation of SARS-CoV-2 infections in symptomatic patients without requesting a confirmatory PCR laboratory test.18 In consequence, patients with a positive ID NOWTM test result were granted the same status and faced equal consequences as patients with a positive laboratory test, such as quarantine orders from their local health authority, certificate of recovery from SARS-CoV-2, and contact tracing.
Sample
All patients who underwent molecular SARS-CoV-2 rapid testing in the participating primary care practices were eligible for participation. Practices represented a broad spectrum of the Thuringian practice landscape (small and large as well as rural and urban practices). Eleven family practices and two pediatric practices (including 4 single-handed practices, 6 group practices and 3 outpatient medical care centers) participated in the study and were equipped with the test system.
Questionnaire
The questionnaire was designed with the expertise of an interdisciplinary research team consisting of two experienced primary care physicians (J.B., F.W.), a work and organizational psychologist (A.M.) and a biochemist with expertise in primary care laboratory testing (R.M.). To ensure comprehensibility and feasibility as well as to address validity, the questionnaire was piloted by three primary care physicians and five persons without scientific or medical background. The final questionnaire (see Supplementary File 1 for English translation) contained questions regarding patient characteristics (age group, sex, population size of place of residence) and the COVID-19 status (symptom intensity, test result), as well as eight statements on point-of-care SARS-CoV-2 testing to be rated on a five-point Likert scale19 and three statements to be completed in an open text format. These question formats were used in order to measure the degree of agreement for a series of statements (Likert scale) or to allow a broad range of answers (open text format). The questionnaire consisted of two DIN-A4 pages and could be completed in five to ten minutes. We sent printed questionnaires to the participating practices, with the request to hand them to all eligible patients. Only anonymous data were collected and patients were informed in a written statement that returning the questionnaire to the practice staff implied their consent for anonymous participation in the study.
Data Analysis
Raw data from the questionnaire were entered into Microsoft Excel 2010. Statistical analyses were performed using R.20 All rating items were answered by at least 96.3% of patients. Items in an open text format were answered by 20.0% (Finding out the test result right away, has the following consequences for me …) to 48.4% of patients (I would be willing to pay a maximum of the following amount for the test …). Missing values were excluded from the analysis. We used descriptive statistics to analyse the pattern of patient perspectives. Open text answers were categorized into subcategories in an inductive approach. To investigate the association between the variables test result (grouping variable) and cost amount willing to pay (dependent variable), a Mann–Whitney U-test was performed.
Results
In total, 215 patients from nine family practices and one pediatric practice returned completed patient questionnaires. The number of returned questionnaires per practice ranged from 3 to 42 (median = 20). An overview of the characteristics of the participants is provided in Table 1. In our study, 29 patients (15.2%) were tested positive for SARS-CoV-2 by molecular point-of-care testing. The majority of patients (116/198, 58.6%) reported none or mild symptoms, while 76 patients (38.4%) reported moderate or severe symptoms. Most patients (163/204, 79.9%) were between 18 and 65 years old, while 22 participants (10.8%) were older than 65 years. 55.2% of the respondents were female. 60.6% resided in villages or towns with less than 20,000 inhabitants.
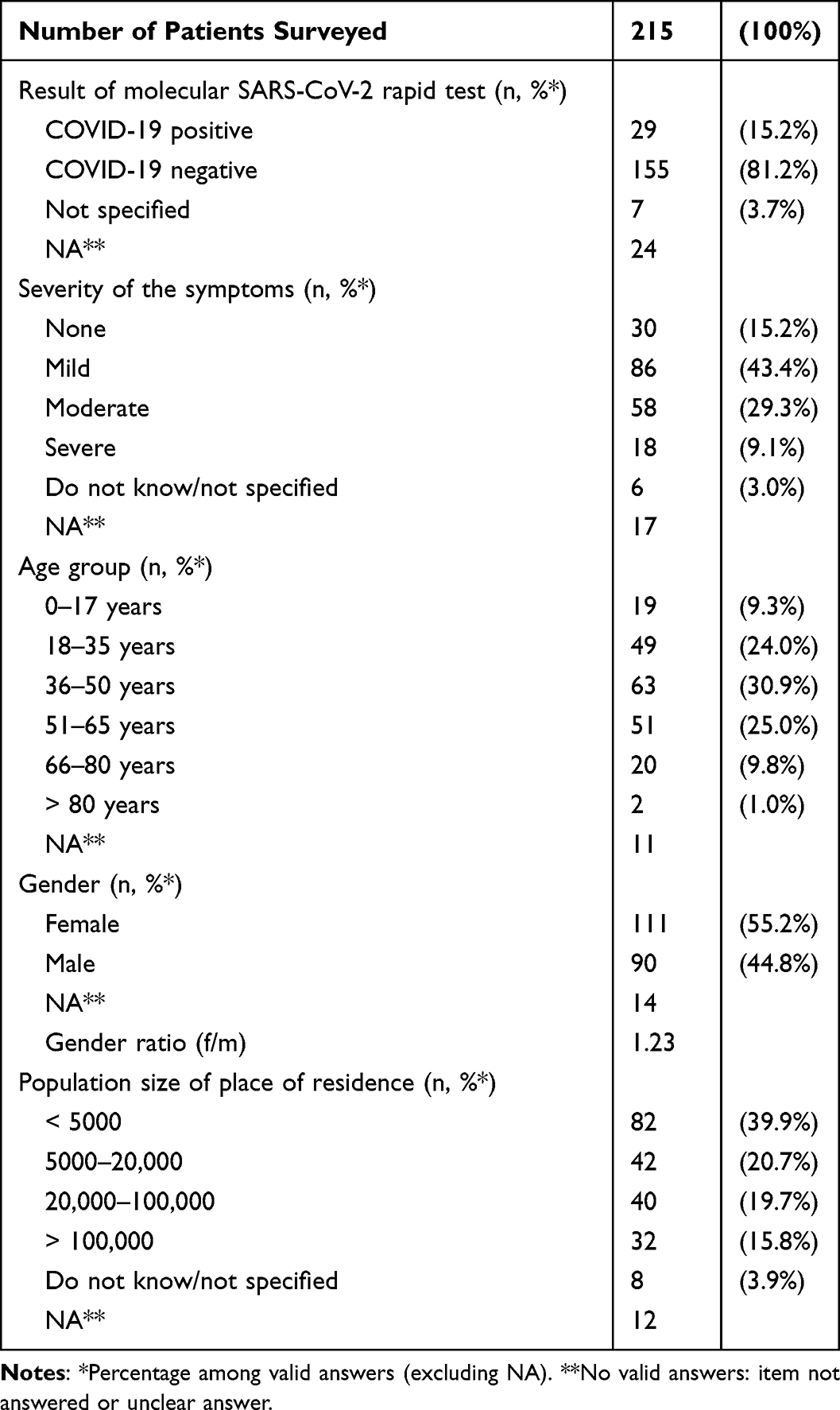 |
Table 1 Characteristics of Patients Surveyed |
General Rating of Molecular Point-of-Care Testing for SARS-CoV-2 in Primary Care Practices
The immediate availability of the test result was of importance for 200 of 212 patients (94.3%) (Figure 1A; see Supplementary File 2 for descriptive results in detail). For 93.4% (197/211) of the participating patients it was important that the rapid test was performed in the primary care practice. A higher reliability compared to other (ie antigen-based) rapid tests was of importance for 89.0% (186/209). 201 of 210 (95.7%) trusted the test result. The great majority (202/212, 95.3%) of patients agreed that they would recommend the molecular point-of-care test for SARS-CoV-2 used in this study to others with symptoms of a cold.
 |
Figure 1 Patient’s rating of molecular SARS-CoV-2 rapid testing conducted in primary care practice. (A) Importance rating on test characteristics. (B) Approval rating on aspects concerning implementation of molecular SARS-CoV-2 rapid testing in primary care. Percentages within the bars are only presented if ≥3%. |
Consequences of Immediate Test Result
For the majority of patients surveyed (208/212, 98.1%) it was of importance to have certainty about potential consequences such as quarantine/self-isolation or informing contact persons immediately (Figure 1B). Forty-three patients provided information on the specific consequence the immediate test result had for them personally. Answers were given in short open comments and were clustered in four categories and nine subcategories (Table 2). Statements referred to pandemic-specific aspects such as knowing whether to self-isolate or notifying others. Patients also reported that molecular point-of-care SARS-CoV-2 testing has consequences on their certainty of action either in a general or context-specific (eg work, family) manner: “I can decide not in 2 to 3 days, but immediately, how to behave in my surrounding.” or “I know if my child can go to kindergarten tomorrow – and if I can go to work.” Respondents reported that they had certainty if they could attend COVID-19 vaccination appointments the following day – at the time of the study period (beginning of 2021) vaccination appointments were difficult to get in Germany. Another consequence that patients reported was the reassurance they felt after the test result.
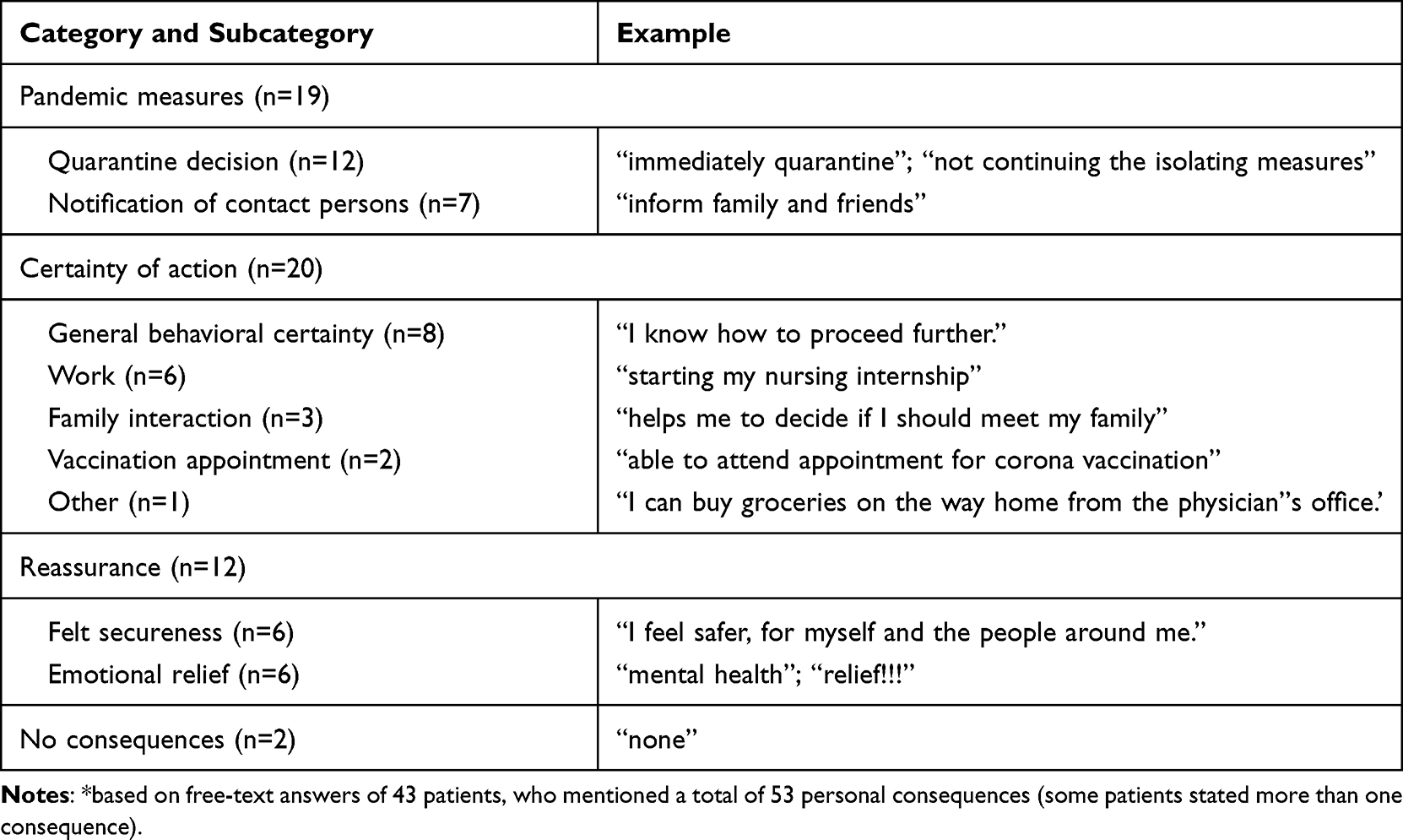 |
Table 2 Personal Consequences of Immediate Test Result for Exemplary Patients* |
Cost Contribution and Expectations in Similar Future Situations
Among the surveyed patients, 31.9% (66/207) agreed that they would pay the estimated costs of 40€ for the molecular SARS-CoV-2 rapid test, while 37.7% did not agree (78/207). Additionally, patients were asked for the maximum costs they were willing to pay. Answers ranged from 0€ to 100€ (median = 20€, interquartile range = 10–25€, n = 104). A Mann–Whitney test indicated that the amount willing to pay did not differ significantly between patients with a positive (median = 20) and patients with a negative (median = 15) COVID-19 test result (U = 483.5, p = 0.171). Expectations that a molecular SARS-CoV-2 rapid test will be used in the future if they have similar symptoms were reported by 96.2% (204/212) of patients.
Discussion
In this study, we surveyed 215 patients on molecular point-of-care SARS-CoV-2 testing performed in primary care practices during a SARS-CoV-2 infection wave in the State of Thuringia, Germany. The rapid test (ID NOWTM COVID-19 rapid test) was approved as equivalent to a PCR laboratory test by local health authorities.
Our study shows that patients accepted and appreciated the characteristics of the molecular SARS-CoV-2 POCT. The vast majority of patients valued the immediate availability of the test result during consultation in primary care practice and showed great confidence in the test result. Having immediate certainty about the potential consequences of the test result, instead of waiting for notification from a central laboratory or public health authority, made a difference for almost all patients. Despite these accepting patient perspectives, our study also identified two aspects that could be challenging for the implementation of a molecular SARS-CoV-2 rapid test in routine primary care: (i) financial aspects and (ii) patient expectations in future situations.
The finding that patients value the immediate test result and the opportunity to discuss implications with their primary care physician within the same consultation has been demonstrated for other indications as well, eg lower respiratory tract infection,21,22 diabetes23–25 and anticoagulant therapy.26,27 Yet, a new and so far COVID-19-specific finding is the difference it made for patients to have immediate certainty about the test result and its consequences. These include self-isolation and informing contact persons, as well as consequences regarding continuation of work and family interaction. With the COVID-19 pandemic being of great public health relevance, consequences of a SARS-CoV-2 test result do not only have an impact on an individual level but also directly affect the society as a whole. Another aspect is the emotional burden that patients face. It has been demonstrated that the waiting period and uncertainty for health-related diagnosis is often provoking anxiety.28 Patients therefore reported great emotional relief and security after having certainty about their SARS-CoV-2 test result. Thus, the time gain due to the rapid testing had a great impact on patients’ emotional wellbeing as well as their behavioral adjustments.
Considering the implementation of a molecular SARS-CoV-2 rapid test in German routine primary care, the aspect of cost reimbursement may be challenging. In German primary care, relatively few POCT diagnostics are reimbursed and do not routinely include molecular rapid SARS-CoV-2 testing. While expenditures were covered within the study setup, a molecular SARS-CoV-2 test should be reimbursed with 40€ in order to be cost-efficient for the primary care physician. Yet, only 31.9% of patients were willing to cover these costs. Most patients reported that they would pay between 10€ and 25€. It is important to note that in Germany patients are not used to paying for medical services beyond monthly insurance rates. While it remains a challenge for the implementation of molecular SARS-CoV-2 rapid tests, it is still remarkable that participating patients were willing to pay for the test at least to some degree.
At the same time, we anticipate the challenge that POCTs for SARS-CoV-2 might be seen as a new standard and that a rapid test result is expected in similar future medical situations. Even though this aspect has not well been studied so far, Wood et al21 conclude for patients from Norway where a POCT is regularly used for managing patients with acute cough that “it appeared to be simply accepted as part of common practice […]” (p.667).
The great acceptance among patients and the rapid detection of SARS-CoV-2 in symptomatic patients advocates for the implementation of molecular SARS-CoV-2 rapid tests in primary care. However, besides costs/reimbursement, many other factors are important for general physicians in the decision to implement a POCT in practice, such as user-friendliness, technical accuracy, frequency of use (disease incidence), clinical guidelines, as well as support, training and quality control.29,30 Further studies addressing these aspects are necessary to fully understand the feasibility and utility of molecular SARS-CoV-2 rapid testing in primary care from a clinician’s perspective.
Strengths and Limitations
Our study is the first that evaluated patient perspectives on a molecular point-of-care SARS-CoV-2 testing in German primary care. One strength of our study is that the test was evaluated in a clinical routine. While existing evidence and evaluation processes of POCTs often solely focus on their diagnostic performance (sensitivity and specificity), we were able to gain insights into the application and consequences of a SARS-CoV-2 rapid test within the medical setting. Patients answered the written questionnaire immediately after rapid SARS-CoV-2 testing, which minimizes the risk of recall bias.
However, the generalizability of our study is limited to some extent since we only analyzed perspectives of patients in Thuringia. Yet, the included practices represent a certain degree of heterogeneity observed in German primary care because they are located in both rural and urban regions and represent different types of practices. Studies in other countries are necessary to confirm the transferability of our results to other countries. Differences in the healthcare system as well as in culture-specific attitudes toward healthcare should be considered. Additionally, it is likely that patient perspectives on a SARS-CoV-2 test are affected by the pandemic situation and testing regulations at the time. In the beginning of 2021, when our survey took place, only few people (mostly >80 years and/or high-risk populations) in Germany had been vaccinated against COVID-19. Accordingly, the influence of a partial or complete vaccination status on the participants’ perspectives cannot be determined. As of June 2022, 78% of the German population has been vaccinated,31 but rigorous testing (incl. rapid tests and laboratory tests) remains a cornerstone of the German COVID-19 strategy. Although there is no evidence that vaccination status affects patient’ attitudes towards molecular SARS-CoV-2 testing in primary care practices, further research on this topic is needed.
Conclusion
Based on the perspectives of the surveyed patients, we found a relatively homogenous response pattern for molecular point-of-care SARS-CoV-2 testing in primary care practices: an immediate COVID-19 test result that is equivalent to a PCR laboratory test is of high relevance for patients. It made a difference for patients “to find out right away” and resulted in immediate adjustments of patients’ behavior and emotional wellbeing. Although patients in Germany commonly do not pay for standard healthcare besides insurance fees, patients would, at least partly, pay for a molecular SARS-CoV-2 rapid test. However, the requested cost contribution should not be above 25€. Before implementing molecular SARS-CoV-2 rapid testing in primary care, the question of cost reimbursement as well as perspectives’ of clinicians and clinical stakeholder must be addressed.
Abbreviations
POCT, point-of-care test; real-time quantitative reverse transcription–polymerase chain reaction, RT-qPCR; PCR, polymerase chain reaction.
Data Sharing Statement
All data generated or analysed during this study are included in this published article and its supplementary information files (see Supplementary File 3 for Study data).
Ethics Approval and Informed Consent
All methods were carried out in accordance with relevant guidelines and regulations. Informed consent was obtained from all participants. The study protocol including all procedures concerning the study as well as the questionnaire was approved by the institutional research ethics board of the Jena University Hospital (Registration No.: 2021-2108-Bef).
Acknowledgments
We would like to thank all patients and physicians for their participation in the study. We would also like to thank the Kassenaerztliche Vereinigung Thueringen (Association of Statutory Health Insurance Physicians Thuringia) for the cooperative collaboration and our student assistant Yana Bender for the conscientious help with the data entry.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
The study is embedded in the project POCT-ambulant (POCT-ambulatory) within the InfectoGnostics Forschungscampus (InfectoGnostics research campus) which is funded by the Bundesministerium für Bildung und Forschung (Ministry of Education and Research) (grant no. 13GW0461). The funding source had no role in the design, conduct or reporting of this study; or in the decision to submit the manuscript for publication.
Disclosure
Ms Anni Matthes reports grants from the Ministry of Education and Research, during the conduct of the study. The authors report no other conflicts of interest in this work.
References
1. Junker R, Schlebusch H, Luppa PB. Point-of-care testing in hospitals and primary care. Dtsch Arztebl Int. 2010;107(33):561–567. doi:10.3238/arztebl.2010.0561
2. Luppa PB, Müller C, Schlichtiger A, Schlebusch H. Point-of-care testing (POCT): current techniques and future perspectives. Trends Analytical Chem. 2011;30(6):887–898. doi:10.1016/j.trac.2011.01.019
3. German Federal Ministry of Health. National Testing Strategy SARS-Cov-2 [in German]. Berlin, Germany: German Federal Ministry of Health; 2022.
4. Truong TT, Dien Bard J, Butler-Wu SM. Rapid Antigen Assays for SARS-CoV-2: promise and Peril. Clin Lab Med. 2022;42(2):203–222. doi:10.1016/j.cll.2022.03.001
5. Davies E, Farooq HZ, Brown B, et al. An Overview of SARS-CoV-2 Molecular Diagnostics in Europe. Clin Lab Med. 2022;42(2):161–191. doi:10.1016/j.cll.2022.02.005
6. Peeling RW, Heymann DL, Teo YY, Garcia PJ. Diagnostics for COVID-19: moving from pandemic response to control. Lancet (London, England. 2022;399(10326):757–768. doi:10.1016/s0140-6736(21)02346-1
7. Erbak Yılmaz H, Iscan E, Oz O, et al. Considerations for the selection of tests for SARS-CoV-2 molecular diagnostics. Mol Biol Rep. 2022;49:1–11. doi:10.1007/s11033-022-07455-5
8. Schols AMR, Dinant G-J, Hopstaken R, Price CP, Kusters R, Cals JWL. International definition of a point-of-care test in family practice: a modified e-Delphi procedure. Fam Pract. 2018;35(4):475–480. doi:10.1093/fampra/cmx134
9. Horvath AR, Lord SJ, StJohn A, et al. From biomarkers to medical tests: the changing landscape of test evaluation. Clin Chimica Acta. 2014;427:49–57. doi:10.1016/j.cca.2013.09.018
10. Verbakel JY, Turner PJ, Thompson MJ, et al. Common evidence gaps in point-of-care diagnostic test evaluation: a review of horizon scan reports. BMJ Open. 2017;7(9):e015760. doi:10.1136/bmjopen-2016-015760
11. Robert Koch Institute. 7-Tage-Inzidenzen nach Bundesländern und Kreisen. Robert Koch Institute; 2022. Available from: https://www.rki.de/DE/Content/InfAZ/N/Neuartiges_Coronavirus/Daten/Inzidenz-Tabellen.html.
12. Abbott. ID NOW COVID-19 PRODUCT INSERT. 2021.
13. Abbott. Releases ID NOW™ COVID-19 Interim Clinical Study Results from 1003 People to Provide the Facts on Clinical Performance and to Support Public Health. Abbott; 2020.
14. Dinnes J, Deeks JJ, Berhane S, et al. Rapid, point-of-care antigen and molecular-based tests for diagnosis of SARS-CoV-2 infection. Cochrane Database Sys Rev. 2021;3(3):CD013705–CD013705. doi:10.1002/14651858.CD013705.pub2
15. Krause E, Puyskens A, Bourquain D, et al. Sensitive on-site detection of SARS-CoV-2 by ID NOW COVID-19. Mol Cell Probes. 2021;58:101742. doi:10.1016/j.mcp.2021.101742
16. Mitchell SL, George KS. Evaluation of the COVID19 ID NOW EUA assay. J Clin Virol. 2020;128:104429. doi:10.1016/j.jcv.2020.104429
17. Procop GW, Brock JE, Reineks EZ, et al. A Comparison of Five SARS-CoV-2 Molecular Assays With Clinical Correlations. Am J Clin Pathol. 2021;155(1):69–78. doi:10.1093/ajcp/aqaa181
18. Kassenärztliche Vereinigung Thüringen. Für ID NOW (Abbott) kein zusätzlicher PCR-Test erforderlich. ÖGD-Ticker – wöchentlicher Newsticker der KV Thüringen. 26; 2021. Available from: https://www.kv-thueringen.de/fileadmin/media2/Corona/OEGD-Ticker/210126_OEGD-Ticker_-_woechentlicher_Newsticker_der_KV_Thueringen_-_KW_04.pdf.
19. Likert R. A technique for the measurement of attitudes. Arch Psychol. 1932;22(140):55.
20. Team RC. R: A Language and Environment for Statistical Computing; 2013.
21. Wood F, Brookes-Howell L, Hood K, et al. A multi-country qualitative study of clinicians’ and patients’ views on point of care tests for lower respiratory tract infection. Fam Pract. 2011;28(6):661–669. doi:10.1093/fampra/cmr031
22. Kaman WE, Andrinopoulou ER, Hays JP. Perceptions of point-of-care infectious disease testing among European medical personnel, point-of-care test kit manufacturers, and the general public. Patient Prefer Adherence. 2013;7:559–577. doi:10.2147/ppa.S44889
23. Patzer KH, Ardjomand P, Göhring K, et al. Implementation of HbA1c Point of Care Testing in 3 German Medical Practices: impact on Workflow and Physician, Staff, and Patient Satisfaction. J Diabetes Sci Technol. 2018;12(3):687–694. doi:10.1177/1932296818759690
24. Schnell O, Crocker JB, Weng J. Impact of HbA1c Testing at Point of Care on Diabetes Management. J Diabetes Sci Technol. 2017;11(3):611–617. doi:10.1177/1932296816678263
25. Stone MA, Burden AC, Burden M, Baker R, Khunti K. Near patient testing for glycated haemoglobin in people with Type 2 diabetes mellitus managed in primary care: acceptability and satisfaction. Diabet Med. 2007;24(7):792–795. doi:10.1111/j.1464-5491.2007.02175.x
26. Laurence CO, Gialamas A, Bubner T, et al. Patient satisfaction with point-of-care testing in general practice. Br J Gen Pract. 2010;60(572):e98–104. doi:10.3399/bjgp10X483508
27. Barcellona D, Mastino D, Marongiu F. Portable coagulometer for vitamin K-antagonist monitoring: the patients’ point of view. Patient Prefer Adherence. 2018;12:1521–1526. doi:10.2147/ppa.S164680
28. Sweeny K, Cavanaugh AG. Waiting is the hardest part: a model of uncertainty navigation in the context of health news. Health Psychol Rev. 2012;6(2):147–164. doi:10.1080/17437199.2010.520112
29. Lingervelder D, Koffijberg H, Kusters R. Point-of-care testing in primary care: a systematic review on implementation aspects addressed in test evaluations. International Journal of Clinical Practice. 2019;73(10):e13392. doi:10.1111/ijcp.13392
30. Kip MMA, Hummel JM, Eppink EB, et al. Understanding the adoption and use of point-of-care tests in Dutch general practices using multi-criteria decision analysis. BMC Fam Pract. 2019;20(1):8. doi:10.1186/s12875-018-0893-4
31. Robert Koch Institute. Digitales Impfquotenmonitoring zur COVID-19-Impfung. Robert Koch Institute. Available from: https://www.rki.de/DE/Content/InfAZ/N/Neuartiges_Coronavirus/Daten/Impfquoten-Tab.html.
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.