")
Back to Journals » International Journal of General Medicine » Volume 13
Isolation Compliance and Associated Factors Among COVID-19 Patients in North-West Iran: A Cross-Sectional Study
Authors Foroozanfar Z , Zamanian M, Moradzadeh R , Hajiabadi F, Ahmadzadeh J , Hosseinkhani Z
Received 23 May 2020
Accepted for publication 14 September 2020
Published 31 December 2020 Volume 2020:13 Pages 1697—1703
DOI https://doi.org/10.2147/IJGM.S264227
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Scott Fraser
Zohre Foroozanfar,1 Maryam Zamanian,2 Rahmatollah Moradzadeh,2 Fatemeh Hajiabadi,1 Jamal Ahmadzadeh,3 Zahra Hosseinkhani4,5
1Children Growth Research Center, Research Institute for Prevention of Non-Communicable Diseases, Qazvin University of Medical Sciences, Qazvin, Iran; 2Department of Epidemiology, School of Health, Arak University of Medical Sciences, Arak, Iran; 3Social Determinants of Health Research Center, Urmia University of Medical Sciences, Urmia, Iran; 4Metabolic Diseases Research Center, Research Institute for Prevention of Non-Communicable Diseases, Qazvin University of Medical Sciences, Qazvin, Iran. School of Health, Qazvin University of Medical Sciences, Qazvin, Iran; 5School of Health, Qazvin University of Medical Sciences, Qazvin, Iran
Correspondence: Zahra Hosseinkhani
Metabolic Diseases Research Center, Research Institute for Prevention of Non-Communicable Diseases, Qazvin University of Medical Sciences, Qazvin, Iran
Tel +98-9127801064
Fax +98- 2833355162
Email [email protected]
Introduction: Coronavirus disease 2019 (COVID-19) has now turned into a public health emergency. Isolation of patients is a possible solution for controlling epidemic infectious diseases. We assessed the compliance of isolation and associated factors among patients with COVID-19.
Methods: This cross-sectional study was conducted on 320 COVID-19 patients discharged from hospitals of Qazvin province. Patients’ isolation, self-care health behaviors, reference to public health services and possible related factors were assessed. Data were analyzed using multiple logistic regression.
Results: In this study, 320 patients were enrolled, including 175 men (54.7%). Two hundred and eighty-six patients (89.4%) had complete isolation. Factors such as phone tracking by health center (OR = 1.30; 95% CI: 1.01 to 1.75) and dry cough (OR = 2.36; 95% CI: 1.09 to 5.09) increased odds of complete isolation in COVID-19 patients, but having a COVID-19 patient in the family (OR = 0.32; 95% CI: 0.15 to 0.71) and symptoms of disease like shortness of breath (OR = 0.39; 95% CI: 0.18 to 0.85) and muscle pain (OR = 0.43; 95% CI: 0.20 to 0.95) decreased odds ratio for these patients.
Conclusion: Phone tracking by the health center was the most important factor to increase the odds of patient isolation. Thus, the health system should consider improving health workers’ knowledge and skills through education.
Keywords: COVID-19, isolation, self-care, compliance, Iran
Introduction
In early December 2019, the first case of coronavirus disease 2019 (COVID-19) was reported in Wuhan city, which is the capital of Hubei province in China. After that, the virus quickly became a pandemic disease of undefined origin.1 Although coronaviruses have been mostly reported in animals, other types of coronavirus have caused pandemics of severe acute respiratory syndrome (SARS) and Middle East respiratory syndrome (MERS) in the world within the past two decades.2–8 The mortality rates of SARS and MERS were respectively reported at 10% and 37%, which are higher in comparison to COVID-19.9,10
Symptoms of COVID-19 in 80% of infected people are mild, and common symptoms include, fever, dry cough and shortness of breath.11 Studies have reported that older age and chronic diseases such as cardiovascular disease, hypertension, diabetes, chronic respiratory disease, and cancer were all associated with mortality rates of COVID-19.12
The World Health Organization (WHO) has recently declared COVID-19 as a public health emergency.13 According to the latest reports by WHO, by 19 may 2020, a total of 4,894,278 laboratory-confirmed cases and 320,189 deaths in 215 countries have been documented globally.14,15 In Iran, the first cases were reported on February 2020 in Qom. Currently, 122,492 confirmed cases and 7057 deaths owing to COVID-19 have been reported in Iran.15,16
There are several similarities and differences between COVID-19 and SARS or MERS, such as in transmissibility and severity pyramids; however, many COVID-19 patients have mild symptoms and COVID-19 has a higher transmissibility than SARS, which contributes to rapid spread of COVID-19.17 Due to the lack of sufficient information about COVID-19, self-care behaviors should be based on recommendations for other types of coronavirus such as SARS and MERS.18,19
Self-care behaviors are of importance to decrease the transmission of COVID-19. Also, the emergency committees have stated that early diagnosis, isolation of confirmed or suspected cases, prompt treatment, and identification of contacts may help reduce transmission.13 According to recent WHO recommendations and also due to the fast spread of COVID-19, people should avoid traveling to high risk areas and contact with patients or people who are symptomatic as well as staying at home and following self-care guidelines.13,18
Prompt identification of laboratory-confirmed cases and their isolation in a medical center or at home is currently an approach to control COVID-19. Also, people who have been in contact with patients having laboratory-confirmed COVID-19 should be quarantined for 14 days after the last time they were exposed to the patient. After the quarantine period, respiratory samples should be taken from quarantined individuals regardless of presence or absence of symptoms.20
Staying at home and observing self-care behaviors have been introduced as the best strategies for controlling the COVID-19 pandemic18,21 and isolation is an important type of self-care behavior.22 According to the definition of WHO, isolation is the separation of patients from other persons in the family and community to prevent the spread of the disease.20
The present study was performed on patients with laboratory-confirmed test (PT-PCR) of COVID-19 who were isolated at home after discharge from the hospital. The aim of this research was to determine the compliance of complete insolation as well as factors associated with the complete isolation at home among patients with COVID-19.
Methods
Sampling and Procedure
In this epidemiological investigation, patients with laboratory confirmed test (PT-PCR) of COVID-19 who were hospitalized in Qazvin province from Feb 23, 2020 to Apr 28, 2020 were studied. We used simple random sampling method and selected 320 patients. Inclusion criterion was living in Qazvin province. We called the patients by phone and collected data after obtaining oral consent for participation in the study and informing them about the purpose of the study. Ethics Committee of Qazvin University of Medical Sciences approved this research (IR.QUMS.REC.1399.007).
Measurements
In this study, self-care behaviors, signs and symptoms of COVID-19 were assessed using government services and facilities after discharge of patients from the hospital and the demographic characteristics of patients were collected.
We assessed patients’ self-care behaviors by asking questions about their isolation. Isolation at home includes refusing to visit relatives during illness, avoiding close contact for 10 days and having a single room at home. Observance of all the three mentioned conditions is defined as complete isolation. People who did not follow at least one of the above conditions were considered as incomplete isolation.
Moreover, the patients’ health behaviors including public transport use before onset of symptoms or in the early days of the disease, history of exposure to a patient in the last 14 days, travel history from 14 days before onset of symptoms, starting home quarantine, seeking medical care early after onset of signs, as well as symptoms such as fever, dry cough, muscle pain, chill, shortness breath, digestive disorders (vomiting, diarrhea, anorexia), taste and smell disorders, and headache were assessed.
From the time the Iranian Ministry of Health prepared several equipment and services for combating COVID-19 epidemic, data about using government services and facilities after discharge from the hospital were collected. These services include disinfection by the government, phone tracking by the health center and home visits. We asked about the patients’ receipt of services and equipment. People who reported receiving at least one of the government services were considered as consumer. We used a checklist for assessing patients’ health behaviors and their use of government services and facilities.
We also inquired patients’ demographic characteristic such as age, gender, education, job, residence, number of family members and comorbidity with non-communicable diseases (diabetes, cancer, pulmonary, cardiovascular disease and immunodeficiency), cigarette and hookah smoking.
Statistical Analyses
Descriptive analysis for quantitative and qualitative variables was done using mean (standard deviation) or median (IQR) and number (percentage), respectively. We used Mann–Whitney U-test, Chi-square or Fisher’s exact test, independent t-test, bivariate and multiple logistic regression analysis. Variables showing P≤0.2 in bivariate analysis were entered into multiple logistic regression model to measure the association between variables with outcome. Complete isolation was considered as the outcome variable in regression models. Independent variables consisted of age, gender, education, job, residence, number of family members, comorbidity with non-communicable disease, cigarette and hookah smoking, signs and symptoms of COVID-19 at admission, health behaviors and receipt of public health services. Data were analyzed using STATA software version 14 with 95% confidence interval.
Results
In the current study, 320 patients with COVID-19 were enrolled, of whom 175 (54.7%) were male and 145 (45.3%) were female. The mean age of subjects was 52.25 ± 17.36 years, which was 52.14 ± 17.44 in males and 52.38 ± 17.33 in females.
Health behaviors, demographic and clinical information of patients and use of public health services based on isolation status are reported in Table 1. Thirty-four patients (10.6%) had incomplete isolation and other patients observed complete isolation. According to the results, most patients were housewives, urban dwelling and in ≤ 39 years old age group. The most common symptoms of disease were fever 209 (65.3%), chills 165 (51.6%) and dry cough 167 (52.2%), and 143 patients (44.7%) had chronic diseases. Also, thirty-five patients (10.9%) were hospital staff.
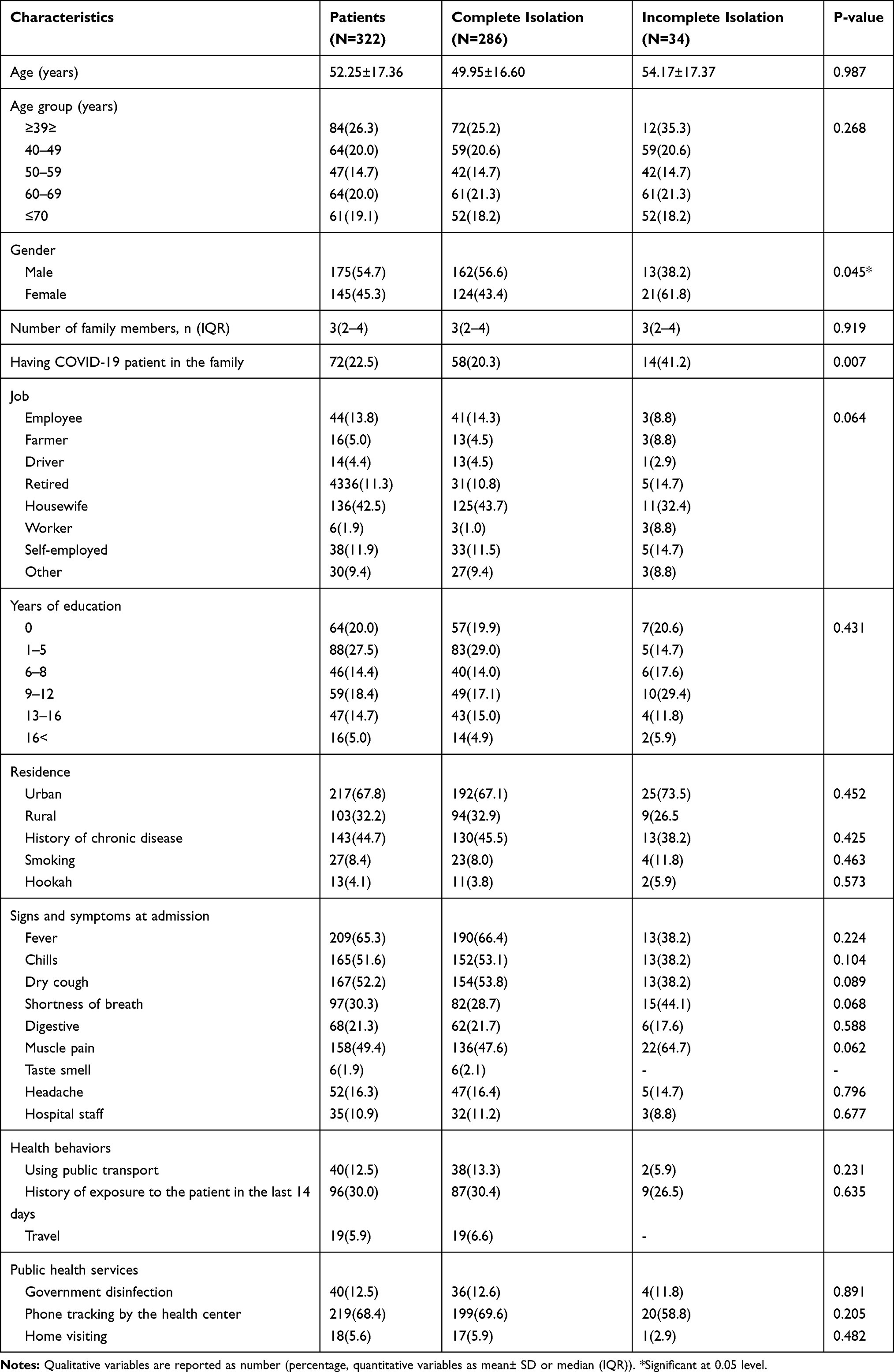 |
Table 1 Characteristics of the Patients with COVID-19 in Qazvin Province |
The results of bivariate analysis showed that gender and having a COVID-19 patient in the family were associated with complete or incomplete isolation. Females and patients who had a COVID-19 patient in the family were less likely to adhere to their isolation.
According to the results of multiple logistic regression, factors such as phone tracking by the health center, having a COVID-19 patient in the family as well as symptoms of disease such as dry cough, shortness of breath and muscle pain were associated with complete or incomplete isolation. Phone tracking by the health center and dry cough were related with the increase in complete isolation rates at home. Furthermore, having a COVID-19 patient in the family as well as symptoms of shortness breath and muscle pain were associated with complete isolation at home (Table 2).
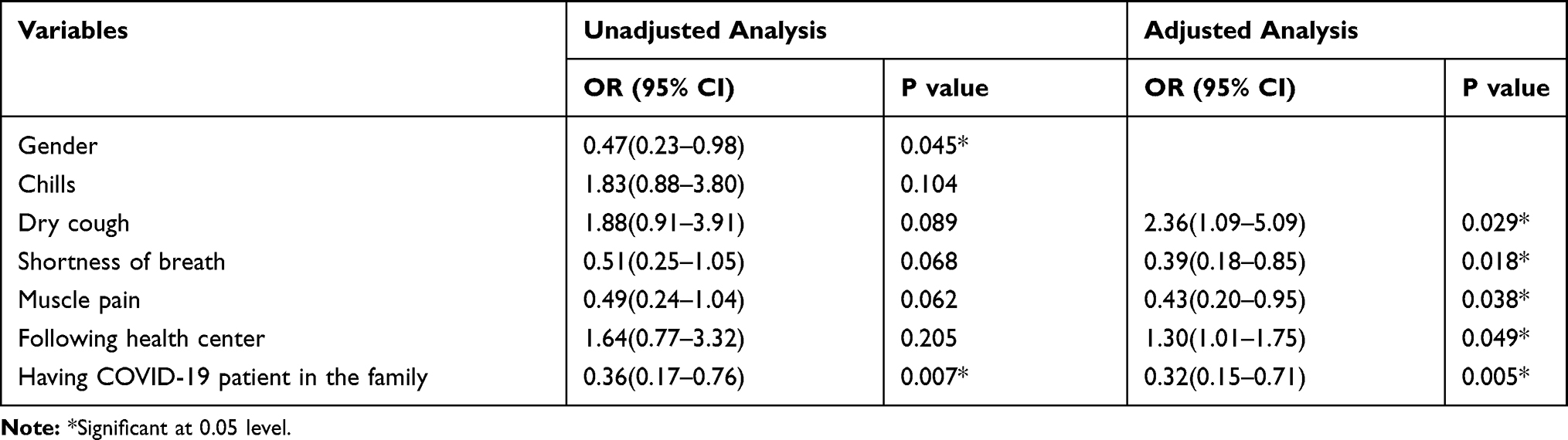 |
Table 2 Factors Associated with the Complete Isolation: Bivariate and Multiple Analysis |
Discussion
We assessed the determinant factors of isolation because it is an important factor to prevent infectious diseases in the community. Based on the results of the present study, government policy and activities for controlling COVID-19, family history of COVID-19 and symptoms of disease are the main factors for complete isolation.
The finding of this study showed that phone tracking by the health center increased odds of complete isolation in COVID-19 patients. In Iran, the health care system provides primary health care (PHC) for all people in the country.23 In the early stage of COVID-19 epidemic, health workers were trained to help people in combating the COVID-19 epidemic.24 As recommended by WHO, health care should be accompanied with social, educational and financial support, emphasizing increasing peoples’ participation in interventional plans, which should be used to consider educational programs and receive the highest level of cooperation.25,26 In Iran, beyond public education programs with national and local media on contagion and seriousness of COVID-19, health workers educate patients by tracking their phones, which is a useful approach improving patients’ knowledge and encouraging complete isolation.
The COVID-19 epidemic has imposed a lot of responsibility for Iranian health workers,21,27 including disinfection and home visiting. It is noteworthy that non-governmental organization (NGO) health centers helped to perform public health services, especially in contaminated areas. Although such activities are not significantly associated with patient isolation they can be effective for implementation of health instructions and control of the disease.28
The current study showed that symptoms of disease are related with isolation. Dry cough, a symptom of more than half of the patients, was a strong predictor for patients’ isolation. In contrast, patients with muscle pain and shortness of breath paid less attention to isolation. It seems that patients with shortness of breath receive more attention and care from their family members because of experiencing severe illness, so that isolation of them has been neglected. Given that fever, cough and shortness of breath are common symptoms of COVID-19 disease, patients should be educated with the most suitable accepted measures,18 It should be noted that all patients with each of the mentioned symptoms have to be isolated.
Despite the fact that patients having a history of COVID-19 disease in the family should be more considerate to isolation, the result of the present study showed just the opposite. It seems that isolation is not important for family members after contamination of more than a person in the family. As isolation and quarantine are of high importance in managing the spread of COVID-19 infection,22 negligence of isolation can be a warning for beginning clusters of the disease and spread of it in the community.
An important limitation of this study was unsatisfactory cooperation of patients with researchers, which could be due to patients’ difficulty in recalling illness days as well as frequent calls from health centers to educate and follow up people’s health behaviors. Another limitation was small sample size in the group not complying with isolation, which could have affected the results of the current study. Also, information on the severity of the disease was not available.
Conclusion
The COVID-19 pandemic is a great concern in the world and isolation is one of the most effective measures for controlling the pandemic. In this study, the association between patients’ isolation with different factors was assessed. Phone tracking by the health center was a main factor to increase the odds of patient isolation. Thus, health systems should consider improving health workers’ knowledge and skills in educating people. Since the patients’ isolation behaviors were heterogeneous in different symptoms, educational protocols should be provided based on educational needs of the community. Certainly, improving effective interventions can help to control the COVID-19 pandemic.
Acknowledgments
We thank all patients involved in the study. The authors express special gratitude to Qazvin University of Medical Sciences for supporting this study.
Funding
This study was supported by the Qazvin University of Medical Sciences (grant: 28/20/18865).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Chen N, Zhou M, Dong X, et al. Epidemiological and clinical characteristics of 99 cases of 2019 novel coronavirus pneumonia in Wuhan, China: a descriptive study. Lancet. 2020;395(10223):507–513. doi:10.1016/S0140-6736(20)30211-7
2. Mobaraki K, Ahmadzadeh J. Current epidemiological status of Middle East respiratory syndrome coronavirus in the world from 1.1. 2017 to 17.1. 2018: a cross-sectional study. BMC Infect Dis. 2019;19(1):1–5. doi:10.1186/s12879-019-3987-2
3. Ahmadzadeh J, Mobaraki K, Mousavi SJ, Aghazadeh-Attari J, Mirza-Aghazadeh-Attari M, Mohebbi I. The risk factors associated with MERS-CoV patient fatality: A global survey. Diagn Microbiol Infect Dis. 2020;96(3):114876. doi:10.1016/j.diagmicrobio.2019.114876
4. Salamatbakhsh M, Mobaraki K, Sadeghimohammadi S, Ahmadzadeh J. The global burden of premature mortality due to the Middle East respiratory syndrome (MERS) using standard expected years of life lost, 2012 to 2019. BMC Public Health. 2019;19(1):1523. doi:10.1186/s12889-019-7899-2
5. Ahmadzadeh J, Mobaraki K. Epidemiological status of the Middle East respiratory syndrome coronavirus in 2019: an update from January 1 to march 31, 2019. Int J Gen Med. 2019;12:305. doi:10.2147/IJGM.S215396
6. Aghazadeh-Attari J, Mohebbi I, Mansorian B, et al. Epidemiological factors and worldwide pattern of Middle East respiratory syndrome coronavirus from 2013 to 2016. Int J Gen Med. 2018;11:121. doi:10.2147/IJGM.S160741
7. Mobaraki K, Salamatbakhsh M, Ahmadzadeh J. Standard expected years of life lost as a neglected index for calculating the burden of premature mortality due to Middle East respiratory syndrome. Health Security. 2019;17(5):407–409. doi:10.1089/hs.2019.0074
8. Salamatbakhsh M, Mobaraki K, Ahmadzadeh J. Syndromic surveillance system for MERS-CoV as new early warning and identification approach. Risk Manag Healthc Policy. 2020;13:93. doi:10.2147/RMHP.S239984
9. Huang C, Wang Y, Li X, et al. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. lancet. 2020;395(10223):497–506. doi:10.1016/S0140-6736(20)30183-5
10. Mobaraki K, Ahmadzadeh J. An update to Middle East respiratory syndrome coronavirus and risk of a pandemic in 2019. Clin Microbiol Infect Dis. 2019;50(8):
11. Hellewell J, Abbott S, Gimma A, et al. Feasibility of controlling COVID-19 outbreaks by isolation of cases and contacts. Lancet Global Health. 2020;8(4):488–496. doi:10.1016/S2214-109X(20)30074-7
12. Jordan RE, Adab P, Cheng K. Covid-19: risk factors for severe disease and death. British Med J Publishing Group. 2020;368:2.
13. Sohrabi C, Alsafi Z, O’Neill N, et al. World Health Organization declares global emergency: A review of the 2019 novel coronavirus (COVID-19). Int J Surgery. 2020.
14. pandemic CdC. Available from: https://www.who.int/emergencies/diseases/novel-coronavirus-2019.
15. COVID-19 CORONAVIRUS PANDEMIC. Available from: https://www.worldometers.info/coronavirus/.
16. http://corona.behdasht.gov.ir/.
17. Wilder-Smith A, Chiew CJ, Lee VJ. Can we contain the COVID-19 outbreak with the same measures as for SARS? Lancet Infect Dis. 2020;20:e102–e107. doi:10.1016/S1473-3099(20)30129-8
18. Mehraeen E, Hayati B, Saeidi S, Heydari M, Seyed Alinaghi S. Self-care instructions for people not requiring hospitalization for coronavirus disease 2019 (COVID-19). Archives Clin Infectious Diseases. 2020;15(COVID–19). doi:10.5812/archcid.102978
19. Murthy S, Gomersall CD, Fowler RA. Care for critically ill patients with COVID-19. JAMA. 2020;323(15):1499–1500. doi:10.1001/jama.2020.3633
20. Organization WH. Considerations for Quarantine of Individuals in the Context of Containment for Coronavirus Disease ( COVID-19): Interim Guidance. World Health Organization; 2020.
21. Mash B. Primary care management of the coronavirus (COVID-19). 2020. South African Family Practice 31;62(1):e1–e4. doi:10.4102/safp.v62i1.5115.
22. Salathé M, Althaus CL, Neher R, et al. COVID-19 epidemic in Switzerland: on the importance of testing, contact tracing and isolation. Swiss Med Wkly. 2020;150(11–12):w20225.
23. Takian A, Doshmangir L, Rashidian A. Implementing family physician programme in rural Iran: exploring the role of an existing primary health care network. Fam Pract. 2013;30(5):551–559. doi:10.1093/fampra/cmt025
24. Raoofi A, Takian A, Sari AA, Olyaeemanesh A, Haghighi H, Aarabi M. COVID-19 pandemic and comparative health policy learning in Iran. Arch Iran Med. 2020;23(4):220–234. doi:10.34172/aim.2020.02
25. Organization WH. Rational Use of Personal Protective Equipment for Coronavirus Disease ( COVID-19) and Considerations During Severe Shortages: Interim Guidance. World Health Organization; 2020.
26. Organization WH. Critical Preparedness, Readiness and Response Actions for COVID-19: Interim Guidance. World Health Organization; 2020.
27. Mash B. Primary care management of the coronavirus (Covid-19). South African Family Practice. 2020;62:1.
28. Ye G, Lin H, Chen L, et al. Environmental contamination of SARS-CoV-2 in healthcare premises. J Infection. 2020;81:e1–e5. doi:10.1016/j.jinf.2020.04.034
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.