")
Back to Journals » International Journal of General Medicine » Volume 15
Is Vitamin B12 Level a Reliable Predictor of Psychosis Severity in Male Patients with Megaloblastic Anemia at a Single Tertiary Hospital?
Authors Wafaa H, Magadmi R , Hakami N , Al Sadoun H, Almaghrabi S, Mohammed N, Alrafiah A
Received 5 August 2022
Accepted for publication 23 September 2022
Published 4 October 2022 Volume 2022:15 Pages 7657—7668
DOI https://doi.org/10.2147/IJGM.S384432
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Scott Fraser
Hanaa Wafaa,1 Rania Magadmi,2 Nora Hakami,1 Hadeel Al Sadoun,1 Safa Almaghrabi,3 Nuha Mohammed,4 Aziza Alrafiah1
1Department of Medical Laboratory Sciences, Faculty of Applied Medical Science, King Abdulaziz University, Jeddah, Saudi Arabia; 2Pharmacology Department, Faculty of Medicine, King Abdulaziz University, Jeddah, Saudi Arabia; 3Department of Physiology, Medical School, King Abdulaziz University, Jeddah, Saudi Arabia; 4Department of Medical Laboratory, King Faisal Medical Complex, Taif, Saudi Arabia
Correspondence: Aziza Alrafiah, P.O Box 80200, Jeddah, 21589, Saudi Arabia, Tel +966 0126401000 Ext. 23495, Fax +966 0126401000 Ext. 21686, Email [email protected]
Background: Megaloblastic anemia (MA) occurs due to ineffective erythropoiesis, which results from impaired DNA synthesis in the hematopoietic precursors and intramedullary hemolysis. MA’s most common cause is nutritional deficiencies of either cobalamin (vitamin B12) or folate (vitamin B6). This study aims to determine the association between MA caused by vitamin B12 deficiency and psychosis among psychotic male patients in Mental Health Hospital at Taif, Saudi Arabia.
Methods: Fifty psychotic male patients, aged 48.58± 1.72, were recruited from the Mental Health Hospital at Taif, Saudi Arabia, in addition to 54 sex-matched healthy controls. The following tests were run: complete blood count (CBC), liver function tests (LFT), serum levels of vitamin B12, folate, and C-reactive protein (CRP).
Results: The CBC showed that RBCs count, haemoglobin, haematocrit, platelets count, mean platelets volume (MPV), and absolute lymphocyte count were significantly lower in psychotic patients versus healthy controls (P=0.007, P=0.002, P=0.001, P=0.004, P=0.0001, and P=0.005, respectively). In contrast, the eosinophil absolute count and basophil percentage were significantly higher in psychotic patients versus controls (P=0.009, P=0.0001, respectively). Vitamin B12 levels were insignificantly decreased in psychotic patients versus healthy group. There were significant negative correlations between serum levels of VitB12 and negative symptoms (r=− 0.381, P=0.006) and hallucination (r=− 0.297, P=0.036).
Conclusion: These findings indicate no link between MA induced by VitB12 insufficiency and psychosis among psychotic patients. However, low serum VitB12 can predict the severity of some psychosis signs, including hallucinations and negative symptoms. Therefore, monitoring VitB12 levels and its supplementation in psychotic patients is recommended to improve their symptoms.
Keywords: vitamin B12, complete blood count, megaloblastic anemia, psychosis
Introduction
Anemia is a condition where red blood cell (RBC) count and haemoglobin (HBG) concentration are lower than the reference range, resulting in decrease in the oxygen-carrying capacity, which is not meeting an individual’s physiological needs. Decrease HBG concentration and haematocrit (HCT) are the most common haematological parameters used to diagnose anemia. In addition, RBC count, mean corpuscular volume (MCV), reticulocyte count, examination of blood film, and HBG electrophoresis are considered significant parameters in anemia diagnosis.1
Megaloblastic anemia (MA) is a condition that occurs due to ineffective erythropoiesis (RBC production), which results from impaired DNA synthesis in the hematopoietic precursors and intramedullary hemolysis. The hallmark of MA is increased MCV, leading to macrocytosis features of RBCs. In addition, thrombocytopenia, as well as leukopenia, are presented frequently in MA.2 MA incidence has increased in the last two decades, particularly in underdeveloped countries.3 In India, megaloblastic anemia is a very common condition, with prevalence ranging from 2–40%.4
Megaloblastic anemia’s most common causes include nutritional deficiencies of either cobalamin (vitamin B12) or folate (vitamin B6).2
MA clinical symptoms include weakness, fatigue, dizziness, shortness of breath, tachycardia and pale skin. In addition, MA can cause gastrointestinal symptoms, including sore tongue, gum bleeding, weight loss, stomach upset, constipation, and diarrhea. Furthermore, MA results in nerve cell damage, which manifests as numbness or tingling in fingers and toes, walking difficulty, memory loss, mood swings, disorientation, depression, and dementia in severe cases.5 MA is considered the main feature of vitamin B12 deficiency, which is associated with psychosis, mood, cognitive, and neurologic symptoms.6,7 Psychosis is a condition that can be defined in one or more of five domains: hallucinations, delusions, abnormal motor behaviors including catatonia, disorganized speech, and thinking, and negative symptoms.8 Neuropsychiatric symptom incidence among individuals diagnosed with vitamin B12 deficiency is 4–50%. In addition, over more than a hundred years, many case reports and other studies have described an association between vitamin B12 and psychosis symptoms.7
A complete blood count (CBC) test is affordable and can be easily made. Leukocytes perform different tasks in immune system.9 Changes in leukocyte count reflect immune system reaction in inflammation.9 Neutrophil–lymphocyte ratio (NLR) is an important marker of chronic and low-grade inflammation and clinical outcomes in neuroimmune disorders.10–12 Monocytes are sources of several cytokines and directly affect platelets and endothelial cells, which induces prothrombotic and proinflammatory pathways. Inflammatory process may be part of schizophrenia etiology.13–15 Platelets are another structure included in proinflammatory secretion with leukocytes. Platelet–lymphocyte ratio (PLR) is used as simple indicator that correlates with inflammation, cardiovascular and chronic diseases.10–12,16 Peripheral platelet models are utilized as indicators of central serotonin (5-HT) metabolism, as they reflect central serotonergic functions.17 Serotonin is involved in the pathophysiology of psychotic disorders and plays pivotal roles in regulation of platelet aggregation and vascular tone.18 Abnormal platelet counts and mean platelet volume (MPV) parameters are determined in some psychiatric disorders, including bipolar disorder, unipolar depression, and schizophrenia.10,19,20 Patients with some psychiatric disorders have raised platelet counts.18,21 Varsak et al22 found that the NLR was significantly higher in first episode psychosis (FEP) versus control groups.
Thus, the current study hypothesizes an association between MA caused by vitamin B12 deficiency and psychosis. Studying this association will help the psychiatric specialist improve the psychosis patient’s symptoms and raise the knowledge level of how poor diet and vitamin B12 deficiency could affect an individual’s mental health.
This study aims to determine the association between megaloblastic anemia and psychosis among psychotic male patients in the Mental Health Hospital at Taif.
Materials and Methods
Study Design and Population
The current study is a case-control study performed among inpatients showing psychosis symptoms in Mental Health Hospital at Taif, Saudi Arabia. The study followed the ethical standards of the Taif Ethics Research Committee at the hospital. The study was made in accordance with principles of the Declaration of Helsinki. Informed consent was obtained from the healthy control study participants prior to study commencement. Psychosis patients often lack insight into their medical condition and possible treatments and thus are unable to provide consent. It was therefore necessary to obtain written informed consent from the patients’ relatives. The study was approved by Taif Ethics Research Committee approval number (471–2021).
Fifty male adult inpatients were included, with their age range between 28–82 years, in addition to 54 age-matched healthy male controls. All inpatients and control participants in the present study are males from Saudi Arabia.
Inclusion criteria were being psychotic inpatients >18 years old showing psychosis symptoms diagnosed by a psychiatrist. Excluded from the study were inpatients taking vitamin B12 supplements, vegetarian, alcoholic, history of gastric surgery such as bariatric surgery. Also patients with chronic diseases that cause megaloblastic anemia like Crohn’s disease, celiac disease pancreatic insufficiency, congenital intrinsic factor deficiency, and patients on drugs that induce megaloblastic anemia, proton pump inhibitors, metformin, anticonvulsants, cytotoxic.
Method
Blood samples were collected from participants. Psychiatrist made a psychiatric diagnosis of psychosis and determined the severity of psychosis symptoms at the hospital. In addition, psychiatric specialists interviewed participants to determine the psychosis symptoms severity using the fifth edition of the Diagnostic and Statistical Manual of Mental Disorders (DSM-5). Clinician-Rated Dimensions of Psychosis Symptom Severity is an 8-item measure that assesses the severity of mental health symptoms that are important across psychotic disorders, including disorganized speech, cognitive impairment, negative symptoms, psychomotor activity abnormality, delusions, hallucinations, mania, depression. Each domain scale ranges from 0 to 4: 0 = not present; 1 = equivocal (occasionally elevated, expansive or irritable mode or some restlessness); 2 = present but mild (frequent periods of somewhat elevated expansive or irritable mood or restlessness); 3 = present but moderate (frequent periods of extensively elevated, expansive, or irritable mood or restlessness); and 4 = present and severe (daily and extensively elevated expansive or irritable mood or restlessness). Negative symptoms include loss of interest in or enjoyment of daily activities, loss of motivation, withdrawal from social life, difficulty showing emotions, difficulty functioning normally.
Inpatients’ blood samples were collected in two tubes: EDTA tubes for CBC analysis and lithium heparin tubes for clinical chemistry analysis as liver function tests, C- eactive protein, vitamin B12 and folic acid level measurements. Lithium heparin samples were centrifuged at 4000 rpm for five minutes, and then plasma was separated into two aliquots. Inpatients’ EDTA samples and LH aliquots were transported on ice to keep the sample temperature between 2–8 °C from Mental Health Hospital in Taif to King Faisal Medical Complex in Taif City. Both inpatients’ EDTA samples and LH aliquots were analyzed within two hours of collection.
Statistical Analysis
The data were analyzed utilizing IBM SPSS Statistics for Windows, version 23 (IBM SPSS, IBM Corp., Armonk, N.Y., USA). Shapiro–Wilk test was utilized to evaluate normal value distribution. The collected values were presented as mean±standard deviation (SD), minimum and maximum. Statistical comparisons of parametric data were made by unpaired student t-test for normally distributed data and Mann–Whitney test for abnormally distributed data. Correlations between components of DSM-5 and serum levels of vitamin B12 were made using Spearman correlation. P <0.05 was considered statistically significant.
Results
Sociodemographic Data
The mean age of patients and controls was 48.58±1.72 and 48.58±1.72 years. The mean BMI of patients and controls was 27.66±0.83 and 26.22±0.64 (kg/m2), respectively. All inpatients included in the study were schizophrenic, showing psychosis symptoms. The psychiatric disorder percentages of those showing psychotic symptoms were as follows: schizophrenia (98.0%) and schizo-affective disorder (2.0%). Intellectual disability was confirmed in 12.0% of the inpatients included in the study along with schizophrenia. Medical disorders were ischemic heart diseases (14.0%), hypertension (14.0%), hyponatremia (12.0%), diabetes mellitus (10.0%), epilepsy (10.0%), hypothyroidism (4.0%) and others (40.0%).
Medications Used by the Patients
Psychotic medications used by the patients are shown in Table 1. The most used medications were Aripiprazole (32%) then Olanzapine (30%), Lorazepam (28%) and Haloperidol (24%).
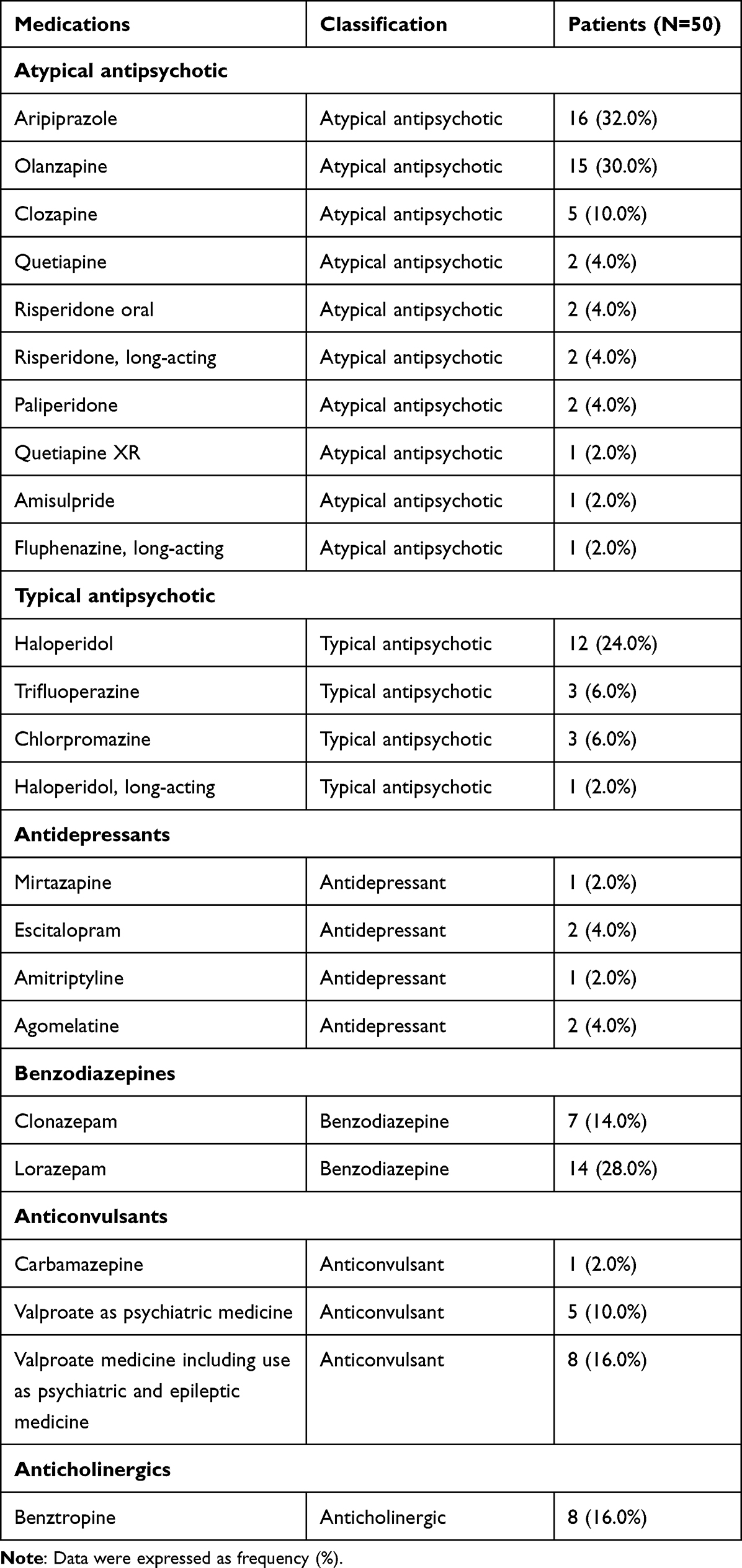 |
Table 1 Medications Used by the Patients |
Clinician-Rated Dimensions of Patients’ Psychosis Symptom Severity (DSM-5)
Clinician-rated dimensions of patients’ psychosis symptom severity (DSM-5) was shown in Table 2. The highest score was for disorganized speech (1.64±0.21 [0–4]), followed by cognitive impairment (1.38±0.17), negative symptoms (1.22±0.15), psychomotor activity abnormality (1.06±0.16), delusions (0.86±0.15), hallucinations (0.78±0.13), mania (0.52±0.13) and, lastly, depression (0.26±0.09). The total score ranged from 0 to 25, with a mean score of 8.02±0.70.
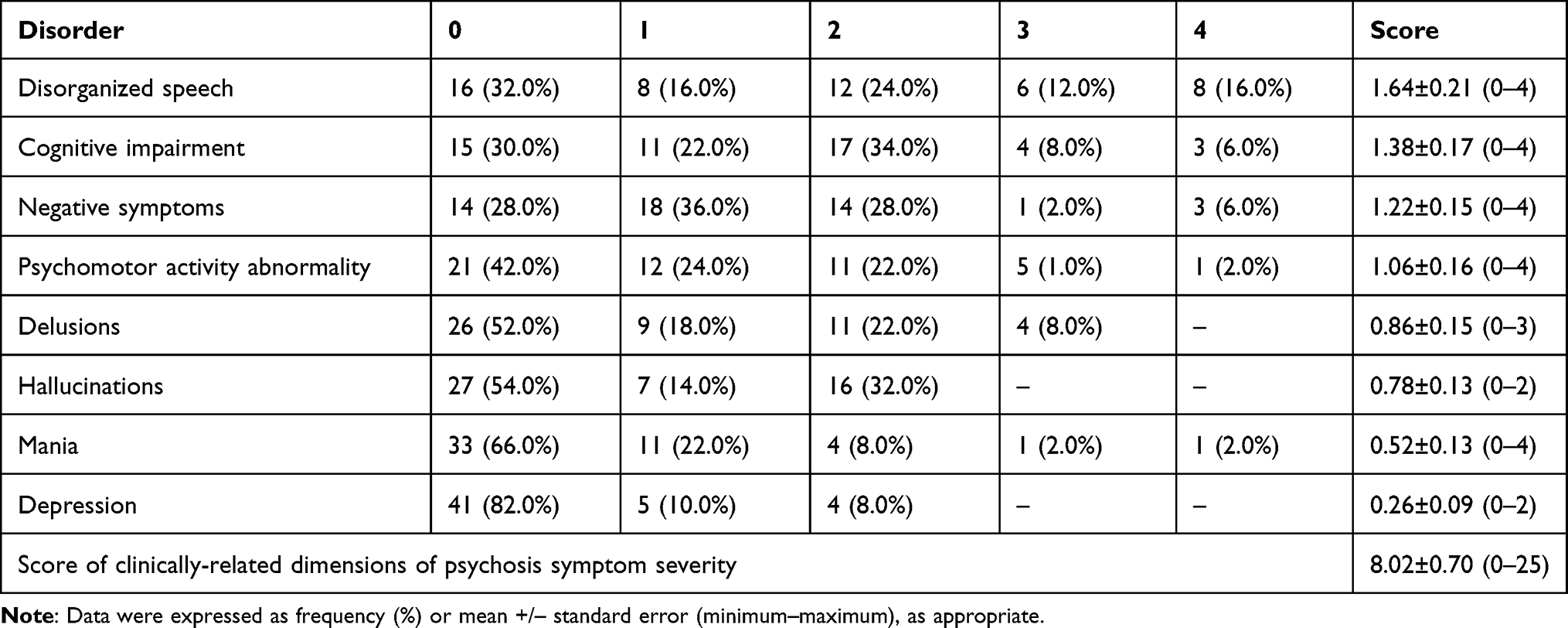 |
Table 2 Clinician-Rated Dimensions of Patients’ (N=50) Psychosis Symptom Severity (DSM-5) |
Complete Blood Count (CBC)
The CBC of patients and controls is shown in Figure 1. In the current study, patients’ LYM×103/µL, RBC (×106/µL), HGB (g/dL), HCT (%), MPV (Fl) and PLT (×103/µL) were significantly decreased versus those of controls (p=0.005, p=0.007, p=0.002, p=0.001, p=0.0001 and p=0.004). Meanwhile, EOS (×103/µL), BASO (%) were significantly increased in patients versus controls (p=0.009, p=0.0001).
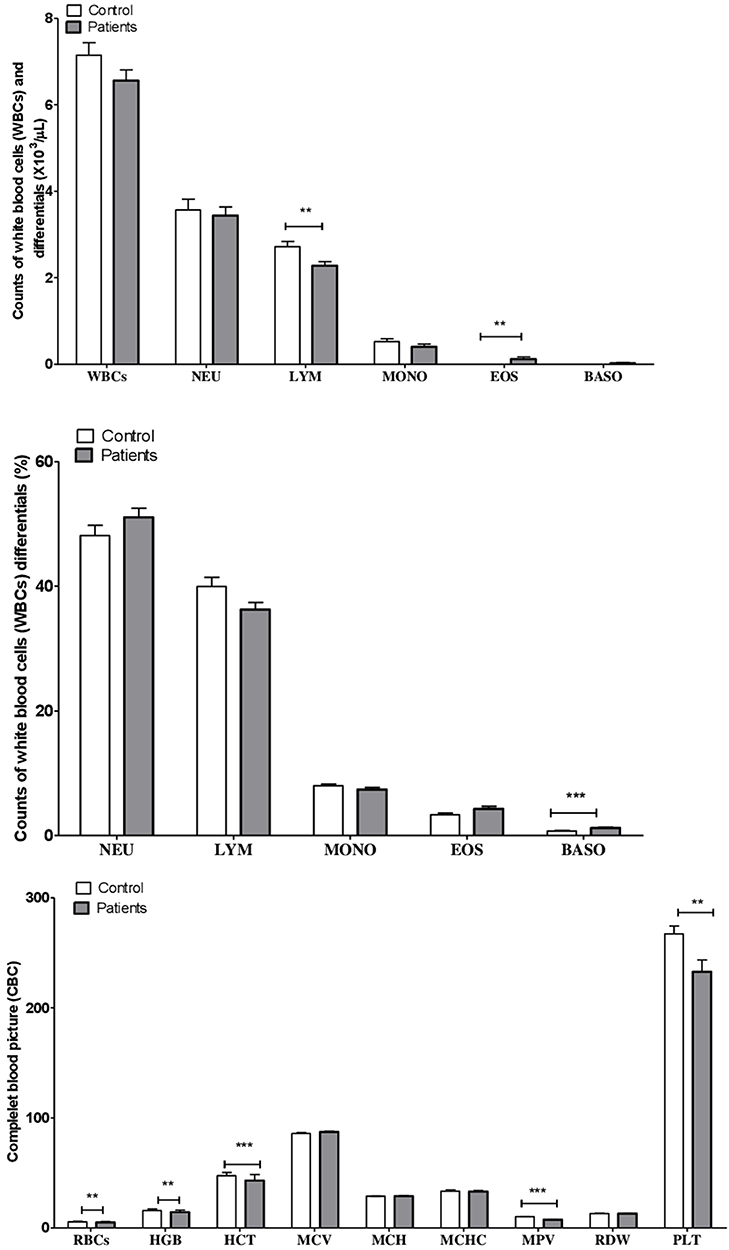 |
Figure 1 Complete blood count (CBC) in patients and controls. Data are expressed as mean +/– standard mean error. **P <0.010; ***P <0.001. |
Liver Function Test (LFT)
The results of the liver function tests of patients and controls are shown in Figure 2. Serum levels of albumin were significantly decreased in patients versus controls (p=0.0001).
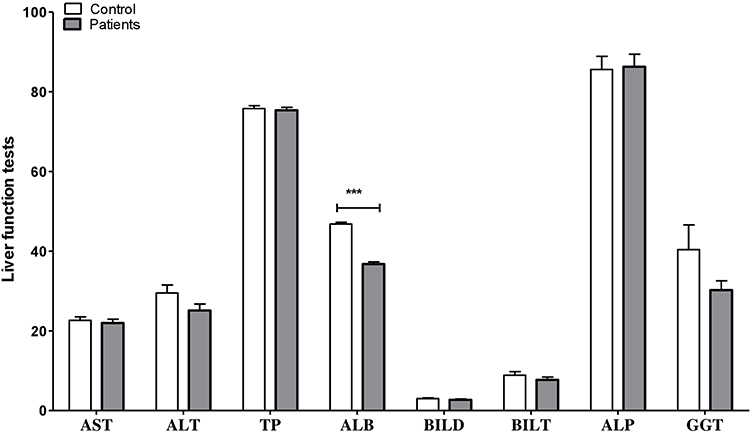 |
Figure 2 Liver function tests of patients and controls. Data are expressed as mean +/– standard mean error. ***P <0.001. |
C-Reactive Protein (CRP), Vitamin B12, and Folic Acid Levels
Serum levels of CRP were significantly increased in patients versus controls (p=0.003). Vitamin B12 levels were slightly lower in psychotic patients when compared to healthy controls. However, there was no statistical significance (p=0.103). There were insignificant changes regarding folic acid levels between patients and controls (p=0.761) (Figure 3).
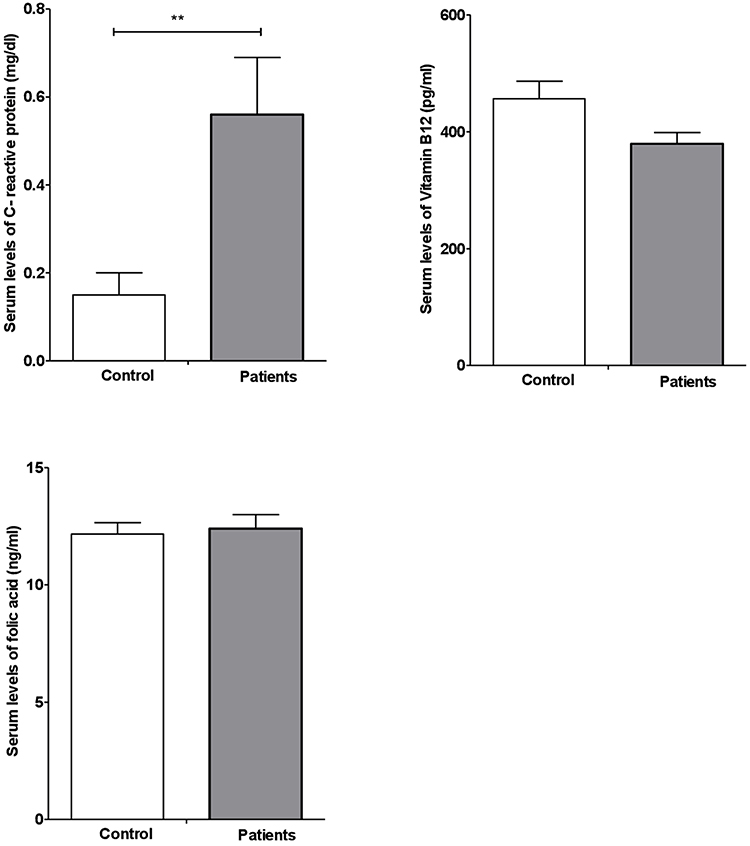 |
Figure 3 CRP, vitamin B12 and folic acid serum levels of patients and controls. Data are expressed as mean +/– standard mean error. **P <0.010. |
Correlations Between Serum Levels of Vitamin B12 and Clinician-Rated Dimensions of Psychosis Symptom Severity (DSM-5)
There were significant negative correlations between serum levels of vitamin B12 and negative symptoms (r=−0.381, p=0.006) and hallucinations (r=−0.297, p=0.036). Meanwhile, there were no significant correlations between other components of DSM-5 and serum levels of vitamin B12 (Figure 4).
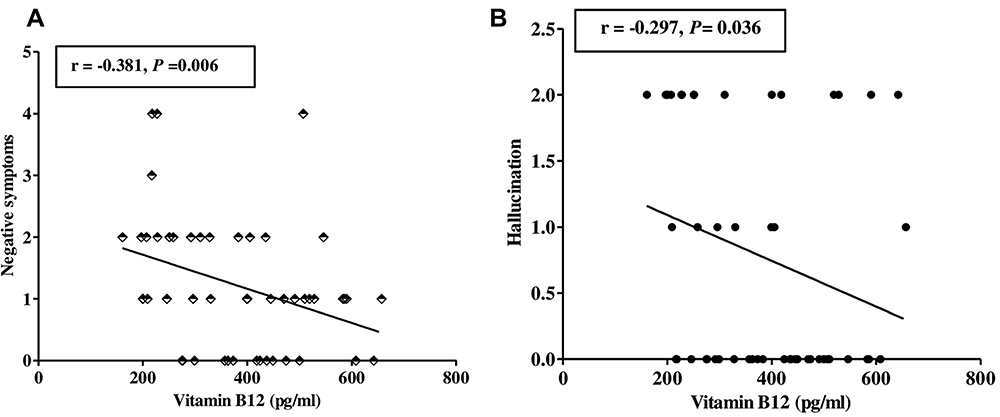 |
Figure 4 Correlations between patients’ (N=50) serum levels of vitamin B12 and negative symptoms (A) and hallucinations (B). |
Discussion
This study was designed to determine the association between megaloblastic anemia due to vitamin B12 deficiency and psychosis among psychotic patients in the Mental Health Hospital at Taif. The study findings show no association between MA induced by Vitamin B12 insufficiency and psychosis among psychotic patients. Dogan et al reported a case of psychotic patients who showed a deficient vitamin B12 level with no signs of MA.23 Payinda and Hansen published a case report of a 52-year-old patient diagnosed with psychosis and low serum vitamin B12 level without signs of anemia.24 Rajkumar and Jebaraj reported a case of a 31-year-old man who suffered from psychotic symptoms with deficient vitamin B12 and no anemia.25 Additionally, Ssonko et al published a study paper that included 280 inpatients at Mental Health Hospital in Uganda and they found that the majority of hospitalized psychiatric patients had deficient serum vitamin B12 with no haematological finding of MA.26 Lindenbaum et al performed on 141 patients at Harlem Hospital Centre and Columbia-Presbyterian Medical Center suffering from neuropsychiatric abnormalities caused by deficient vitamin B12. They conclude that neuropsychiatric disorders caused by low vitamin B12 occur commonly without anemia or abnormal elevated MCV.27 The current study finding shows that psychosis inpatients have an insignificant lower serum vitamin B12 level when compared to controls. In addition, the study findings show a significant negative correlation between the serum level of vitamin B12 and the severity of two symptoms of psychosis: hallucinations and negative symptoms. Consequently, vitamin B12 levels can predict the severity of some psychosis signs, including hallucinations and negative symptoms. Sabeen and Holroyd published a paper concluding that low to moderately normal levels of vitamin B12 can cause psychiatric symptoms.28 Lachner et al reported that establishing the normal serum vitamin B12 threshold range depends on population statistics. Active disease due to vitamin B12 deficiency may present, although the normal range of the metabolic requirements of individuals may vary. Another cause of a false negative result of the deficiency is that inactive Cbl form might be detected by radioimmunoassay and mimic the tissue deficiency of the active cobalamin. In addition, the concentration of vitamin B12 binding proteins may alter vitamin B12 level, causing a false negative result.29 Another cross-sectional study among schizophrenic patients, by Hussein et al, found a significant negative correlation between vitamin B12 level and negative symptoms.30 Engelborghs et al reported statistically significant negative correlations among frontotemporal dementia patients between hallucinations, levels of vitamin B12, and diurnal rhythm disturbances.31 Psychotic inpatients in current study are on antipsychotic drugs, antidepressants, anticonvulsants, and benzodiazepines to control their psychiatric symptoms, which might affect some laboratory results.
Neuronal demyelination, which affects both the peripheral and central nervous systems, is another traditional pathophysiologic symptom of B12 insufficiency in addition to megaloblastic anemia. S-adenosylmethionine (SAM) shortage and subsequent suppression of methylation processes, which are necessary for membrane phospholipid metabolism and neurotransmitter metabolism, are one of the ideas behind demyelinating disease B12 deficiency-related myeloneuropathy possibly being brought on by a disruption in the metabolism of odd-chain fatty acids due to the suppression of the conversion of methylmalonyl CoA to succinyl CoA. B12 therapy corrects changes in cytokines and epidermal growth factor in cerebrospinal fluid and serum, which are linked to neurological symptoms of B12 deficiency in humans and rats and have been hypothesised to contribute to neuropathy.3
The only vitamin in the human body that contains cobalt is vitamin B12, which serves as a cofactor for enzyme methionine synthetase. Vitamin B12 deficiency is linked to a variety of neurologic, psychiatric, and neuropsychiatric disorders, including neuropathy, myelopathy, optic atrophy, cerebellar ataxia, and cognitive disorders like dementia, psychosis, and mood disorders.32 DNA and other molecules must be synthesised from nucleotides, which requires one-carbon metabolism (OCM). This cycle is a complex system that transfers a methyl group between several different conformations.32 Impaired folic acid and vitamin B12 levels are the main contributors to OCM changes.33
The present study findings show significantly elevated CRP level within the schizophrenia inpatient group consistent with a published study by Dickerson et al among schizophrenic patients. In Dickerson et al’s study, schizophrenia patients received the following medications: atypical antipsychotics (clozapine, risperidone, olanzapine), antidepressant medication, anti-cholinergic, and lithium.34 In addition, a retrospective study by Hefner et al among patients treated with antipsychotics including clozapine and risperidone shows a significant correlation between the percentage increase in serum concentration of clozapine and risperidone and the serum level of CRP.35 In the current study, CBC results show significant lymphocytopenia compared to the control subject. Moreover, psychosis inpatients show lower total WBC counts and neutrophil counts without statistical significance. Several case studies show that lymphocytopenia and neutropenia can be induced by combined risperidone and paliperidone treatment.36–39 Abanmy et al conducted a retrospective study in Saudi Arabia to report the incidence of clozapine-induced hematological toxicity. They reported that clozapine induces lymphocytopenia in 12.9% of their patients.40 Psychotic inpatients in the current study also have significantly elevated eosinophil count and basophil percentages compared to control subjects. Several case studies reported that olanzapine41–43 and valproate induce eosinophil.44 Tsamakis et al published a paper concluding that elevated eosinophil count might be associated with antipsychotics. In their study, elevated eosinophil count was noted in psychiatric patients treated with haloperidol, olanzapine, and aripiprazole.45 Lee et al reported a transient increase in basophil count after the first week of clozapine treatment.46 RBC count, HBG, HCT, platelet count, and MPV were significantly lower in the patient group than in controls, which is consistent with a cross-sectional study conducted by Jombo and Ekwere on 60 persons with schizophrenia treated with either typical or atypical antipsychotics except for MPV. In contrast, their study findings show significantly higher RBCS count, Hb, Hct, platelet count, and MPV in patients than in controls.47 Nasreddine and Beydoun indicate a negative correlation between valproate plasma level and platelet count.48 The current study’s findings show a significant decrease in the MPV of patients compared to controls. A study conducted by Ataoglu and Canan showed that patient platelet count and MPV results were significantly decreased following treatment with escitalopram.17 The liver function test finding of the current study showed a significant decrease in serum albumin level in inpatients. This agreed with the results of Zhai et al, which found a significant decrease in albumin following antipsychotic treatments.49 In addition, a study conducted by Garcia-Unzueta et al found that serum albumin was significantly lower in schizophrenic patients under antipsychotic treatment compared to healthy controls.50
Limitations
This study has some limitations. First, this is a case control study with a small sample size. Absence of data relating to duration of first-episode psychosis in psychotic patients is another limitation. Another limitation is that it was conducted in a single institution in Saudi Arabia and involved the male gender only, so the results obtained cannot be generalized.
Conclusions
This study was conducted to determine the association between megaloblastic anemia caused by vitamin B12 insufficiency and psychosis among psychotic patients in Mental Health Hospital in Taif. We aimed to find a causal relationship between MA and psychosis. Our study found no association between megaloblastic anemia and psychosis among psychotic patients in the Mental Health Hospital at Taif. However, psychotic inpatients had a low to moderate average vitamin B12 level, which might contribute to the psychosis symptoms. We found a significant negative correlation between the serum level of vitamin B12 and the severity of two symptoms of psychosis: hallucinations and negative symptoms. According to our study findings, monitoring VitB12 levels in psychotic patients is recommended to improve their symptoms.
For future studies, we recommend recording baseline vitamin levels and assessing psychosis symptom severity at admission, and then following patients’ symptoms after introducing vitamin B12 supplements. Moreover, increasing sample size and involving females in the study may obtain more accurate and precise results.
Data Sharing Statement
The data available are in the manuscript.
Institutional Review Board Statement
The study was approved by Taif Ethics Research Committee with approval number (471-2021). The study was executed in consensus with the guidelines followed by both Mental Health Hospital and King Faisal Medical Complex, Taif, Saudi Arabia, which were in accordance with Ministry of Health in Saudi Arabia.
Acknowledgments
The authors would like to acknowledge Mental Health Hospital and King Faisal Medical Complex for supporting this study. Also, we would like to thank Dr. Talal Mahfoz, Muna Al-Qethami, and Abdulrahman Al-Malki for their help.
Funding
This research was self-funded.
Disclosure
The authors declare that they have no competing interests.
References
1. Romain M, Sviri S, Linton D, Stav I, van Heerden PV. The role of vitamin B12 in the critically ill—a review. Anaesth Intensive Care. 2016;44(4):447–452. doi:10.1177/0310057X1604400410
2. Watanabe F, Bito T. Vitamin B12 sources and microbial interaction. Exp Biol Med. 2018;243(2):148–158. doi:10.1177/1535370217746612
3. Allen LH, Miller JW, De Groot L, et al. Biomarkers of Nutrition for Development (BOND): vitamin B-12 review. J Nutr. 2018;148(suppl_4):1995S–2027S. doi:10.1093/jn/nxy201
4. Kaur N, Nair V, Sharma S, Dudeja P, Puri P. A descriptive study of clinico-hematological profile of megaloblastic anemia in a tertiary care hospital. Med J Armed Forces India. 2018;74(4):365–370. doi:10.1016/j.mjafi.2017.11.005
5. Hariz A, Bhattacharya PT. Megaloblastic Anemia. StatPearls [Internet]; 2020.
6. Goossen LH. Anemias caused by defects of DNA metabolism. In: Rodak’s Hematology-E-Book: Clinical Principles and Applications. Elsevier Health Sciences; 2019:282.
7. Koury MJ, Ponka P. New insights into erythropoiesis: the roles of folate, vitamin B12, and iron. Annu Rev Nutr. 2004;24:105–131. doi:10.1146/annurev.nutr.24.012003.132306
8. Obeagu EI, Babar Q, Obeagu GU. Megaloblastic anaemia-a review. Int J Curr Res Med Sci. 2021;7(5):17–24.
9. Zahorec R. Ratio of neutrophil to lymphocyte counts-rapid and simple parameter of systemic inflammation and stress in critically ill. Bratisl Lek Listy. 2001;102(1):5–14.
10. Özdin S, Sarisoy G, Böke Ö. A comparison of the neutrophil-lymphocyte, platelet-lymphocyte and monocyte-lymphocyte ratios in schizophrenia and bipolar disorder patients–a retrospective file review. Nord J Psychiatry. 2017;71(7):509–512. doi:10.1080/08039488.2017.1340517
11. Akıl E, Bulut A, Kaplan İ, Özdemir HH, Arslan D, Aluçlu MU. The increase of carcinoembryonic antigen (CEA), high-sensitivity C-reactive protein, and neutrophil/lymphocyte ratio in Parkinson’s disease. Neurol Sci. 2015;36(3):423–428. doi:10.1007/s10072-014-1976-1
12. Rembach A, Watt AD, Wilson WJ, et al. An increased neutrophil–lymphocyte ratio in Alzheimer’s disease is a function of age and is weakly correlated with neocortical amyloid accumulation. J Neuroimmunol. 2014;273(1–2):65–71. doi:10.1016/j.jneuroim.2014.05.005
13. Abacioglu OO. Monocyte to high-density lipoprotein ratio: a prognostic factor for mitral valve prolapse? Bratisl Lek Listy. 2020;121(2):151–153. doi:10.4149/BLL_2020_021
14. Canpolat U, Çetin EH, Cetin S, et al. Association of monocyte-to-HDL cholesterol ratio with slow coronary flow is linked to systemic inflammation. Clin Appl Thromb Hemost. 2016;22(5):476–482. doi:10.1177/1076029615594002
15. Kaplan I, Kaplan M, Abacioglu O, Yavuz F, Saler T. Monocyte/HDL ratio predicts hypertensive complications. Bratisl Lek Listy. 2020;121(2):133–136. doi:10.4149/BLL_2020_018
16. Topal E, Celiksoy MH, Catal F, Karakoç H, Karadağ A, Sancak R. The Platelet Parameters as Inflammatory Markers in Preschool Children with Atopic Eczema. Clin Lab. 2015;61(5–6):493–496. doi:10.7754/Clin.Lab.2014.140930
17. Ataoglu A, Canan F. Mean platelet volume in patients with major depression: effect of escitalopram treatment. J Clin Psychopharmacol. 2009;29(4):368–371. doi:10.1097/JCP.0b013e3181abdfd7
18. Seidel A, Arolt V, Hunstiger M, Rink L, Behnisch A, Kirchner H. Major depressive disorder is associated with elevated monocyte counts. Acta Psychiatr Scand. 1996;94(3):198–204. doi:10.1111/j.1600-0447.1996.tb09849.x
19. Yüksel RN, Ertek IE, Dikmen AU, Göka E. High neutrophil-lymphocyte ratio in schizophrenia independent of infectious and metabolic parameters. Nord J Psychiatry. 2018;72(5):336–340. doi:10.1080/08039488.2018.1458899
20. Kirlioglu S, Balcioglu Y, Kalelioglu T, Erten E, Karamustafalioglu N. Comparison of the complete blood count-derived inflammatory markers in bipolar patients with manic and mixed episodes. Clin Study. 2019;195:199.
21. Ragolsky M, Shimon H, Shalev H, Weizman A, Rubin E. Suicidal thoughts are associated with platelet counts in adolescent inpatients. J Child Adolesc Psychopharmacol. 2013;23(1):49–53. doi:10.1089/cap.2012.0057
22. Varsak N, Aydin M, Ibrahim E. The evaluation of neutrophil-lymphocyte ratio in patients with first episode psychosis. Family Practi Palliative Care. 2017;1(3):65–69. doi:10.22391/920.287411
23. Dogan M, Ariyuca S, Peker E, et al. Psychotic disorder, hypertension and seizures associated with vitamin B12 deficiency: a case report. Hum Exp Toxicol. 2012;31(4):410–413. doi:10.1177/0960327111422404
24. Payinda G, Hansen T. Vitamin B12 deficiency manifested as psychosis without anemia. Am J Psychiatr. 2000;157(4):660–661. doi:10.1176/appi.ajp.157.4.660
25. Rajkumar A, Jebaraj P. Chronic psychosis associated with vitamin B12 deficiency. J Assoc Physicians India. 2008;56:115–116.
26. Ssonko M, Ddungu H, Musisi S. Low serum vitamin B 12 levels among psychiatric patients admitted in Butabika mental hospital in Uganda. BMC Res Notes. 2014;7(1):1–9. doi:10.1186/1756-0500-7-90
27. Lindenbaum J, Healton EB, Savage DG, et al. Neuropsychiatric disorders caused by cobalamin deficiency in the absence of anemia or macrocytosis. N Engl j medi. 1988;318(26):1720–1728. doi:10.1056/NEJM198806303182604
28. Sabeen S, Holroyd S, Holroyd S. Vitamin B12 and psychiatric illness. Arch Gerontol Geriatr. 2009;51(1):6–8. doi:10.1016/j.archger.2009.06.002
29. Lachner C, Steinle NI, Regenold WT. The neuropsychiatry of vitamin B12 deficiency in elderly patients. J Neuropsychiatry Clin Neurosci. 2012;24(1):5–15. doi:10.1176/appi.neuropsych.11020052
30. Abd El Mawella SM, Hussein HA, Ahmed T. Folate, vitamin B12, and negative symptoms in schizophrenia. Egypt J Psychiatr. 2018;39(2):89. doi:10.4103/ejpsy.ejpsy_39_17
31. Engelborghs S, Vloeberghs E, Maertens K, et al. Correlations between cognitive, behavioural and psychological findings and levels of vitamin B12 and folate in patients with dementia. Int J Geriatr Psychiatry. 2004;19(4):365–370. doi:10.1002/gps.1092
32. Pedro Dos Reis F, Duarte L, Cartaxo T, Santos V. Folic acid, vitamin B12, and psychotic symptoms among young psychiatric inpatients. Nascer e Crescer. 2021;30(2):85–91.
33. Zhilyaeva T, Piatoikina A, Bavrina A, et al. Homocysteine in schizophrenia: independent pathogenetic factor with prooxidant activity or integral marker of other biochemical disturbances? Schizophr Res Treatment. 2021;2021:1–6. doi:10.1155/2021/7721760
34. Dickerson F, Stallings C, Origoni A, et al. C-reactive protein is elevated in schizophrenia. Schizophr Res. 2013;143(1):198–202. doi:10.1016/j.schres.2012.10.041
35. Hefner G, Shams ME, Unterecker S, Falter T, Hiemke C. Inflammation and psychotropic drugs: the relationship between C-reactive protein and antipsychotic drug levels. Psychopharmacology. 2016;233(9):1695–1705. doi:10.1007/s00213-015-3976-0
36. Raj V, Druitt T, Purushothaman S, Dunsdon J, Aust N. Risperidone/paliperidone induced neutropenia and lymphopenia. Aust NZJ Psychiatr. 2013;47(3):291–292. doi:10.1177/0004867412460594
37. Manfredi G, Solfanelli A, Dimitri G, et al. Risperidone-induced leukopenia: a case report and brief review of literature. Gen Hosp Psychiatry. 2013;35(1):102.e3–102. e6. doi:10.1016/j.genhosppsych.2012.03.009
38. Tseng -C-C. Neutropenia during risperidone treatment. J Neuropsychiatry Clin Neurosci. 2011;23(4):E19–E19. doi:10.1176/jnp.23.4.jnpe19
39. Woon LS-C, Tee CK, Gan LLY, Deang KT, Chan LF. Olanzapine-induced and risperidone-induced leukopenia: a case of synergistic adverse reaction? J. Psychiatr Pract. 2018;24(2):121–124. doi:10.1097/PRA.0000000000000292
40. Abanmy NO, Al-Jaloud A, Al-Jabr A, Al-Ruwaisan R, Al-Saeed W, Fatani S. Clozapine-induced blood dyscrasias in Saudi Arab patients. Int J Clin Pharm. 2014;36(4):815–820. doi:10.1007/s11096-014-9967-0
41. Evison M, Holme J, Alaloul M, et al. Olanzapine-induced eosinophilic pleuritis. Respir Med Case Rep. 2015;14:24–26. doi:10.1016/j.rmcr.2014.11.007
42. Huang J, Yu Y, Lin W, Zhang D, Deng Z, Ding Q. Olanzapine-induced peripheral eosinophilia and eosinophilic pleural effusion: a case report. Medicine. 2018;97(7):e9996.
43. Raz A, Eilam O, Hayek T, Bergman R, Yungerman T. A case report of olanzapine-induced hypersensitivity syndrome. Am J Med Sci. 2001;321(2):156–158. doi:10.1097/00000441-200102000-00008
44. Bullington W, Sahn SA, Judson MA. Valproic acid–induced eosinophilic pleural effusion: a case report and review of the literature. Am J Med Sci. 2007;333(5):290–292. doi:10.1097/MAJ.0b013e31805339ae
45. Tsamakis K, Mueller C, Hortis I, et al. Association of antipsychotic use with raised eosinophil count. Exp Ther Med. 2021;21(5):1–5. doi:10.3892/etm.2021.9944
46. Lee J, Takeuchi H, Fervaha G, et al. The effect of clozapine on hematological indices: a 1-year follow-up study. J Clin Psychopharmacol. 2015;35(5):510–516. doi:10.1097/JCP.0000000000000387
47. Jombo HE, Ekwere TA. A cross-sectional study of the impact of antipsychotic medications on the hematological profile of patients with schizophrenia in a tertiary health facility in Uyo, South-South, Nigeria. Int Neuropsychiatr Dis J. 2018;11(2):1–9. doi:10.9734/INDJ/2018/40894
48. Nasreddine W, Beydoun A. Valproate‐induced thrombocytopenia: a prospective monotherapy study. Epilepsia. 2008;49(3):438–445. doi:10.1111/j.1528-1167.2007.01429.x
49. Zhai D, Liu Y, Ma F, et al. Effects of the first exposure of antipsychotics on serum albumin in adolescents and young adults with first-episode schizophrenia. J Clin Psychopharmacol. 2018;38(1):103–105. doi:10.1097/JCP.0000000000000819
50. Garcia‐Unzueta MT, Herran A, Sierra‐Biddle D, Amado JA, Vázquez‐Barquero JL, Álvarez C. Alterations of liver function test in patients treated with antipsychotics. J Clin Lab Anal. 2003;17(6):216–218. doi:10.1002/jcla.10094
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.