")
Back to Journals » International Journal of General Medicine » Volume 15
Is Travel Time Associated with Health Service Utilization in Northwest China? Evidence from Shaanxi Province
Received 30 January 2022
Accepted for publication 26 April 2022
Published 13 May 2022 Volume 2022:15 Pages 4949—4957
DOI https://doi.org/10.2147/IJGM.S360582
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Ruhai Bai,1 Jianmin Gao,2 Wanyue Dong3
1School of Public Affairs, Nanjing University of Science and Technology, Nanjing, People’s Republic of China; 2School of Public Policy and Administration, Xi’an Jiaotong University, Xi’an, People’s Republic of China; 3School of Elderly Care Services and Management, Nanjing University of Chinese Medicine, Nanjing, People’s Republic of China
Correspondence: Wanyue Dong, School of Elderly Care Services and Management, Nanjing University of Chinese Medicine, No. 138 Xianlin Road, Qixia District, Nanjing, 210023, People’s Republic of China, Tel +86 25 858 11301, Email [email protected]
Purpose: Northwest China has a large area, low population density, and few health resources, which makes the utilization of health resources in this region difficult. The objective of this study was to assess utilization of health services and its association with travel time in Shaanxi Province.
Patients and Methods: Data were obtained from the fifth Household Health Service Survey of Shaanxi Province conducted in 2013. Binary logistic regression was used to assess the relationship between travel time and health service utilization, and negative binomial regression was conducted to assess the relationship between travel time and the frequency of health service utilization.
Results: A total of 42.6% of patients used health services, with a higher use rate among rural residents than among urban residents (47.0% and 27.4%, respectively). A total of 30.9% of patients traveled more than 15 min to the nearest medical facility (33.3% in rural areas and 22.6% in urban areas). A total of 12.4% of patients traveled more than 30 min to the nearest medical facility (15.1% in rural areas and 3.0% in urban areas). Urban residents living farthest from health care facilities (more than 30 min) had a 2.12-fold higher probability of health service utilization and expected to have a health service utilization rate 1.77 times greater than that of residents with a travel time of less than 5 min. Among the rural population, there was no significant correlation between travel time and health service utilization.
Conclusion: Urban patients living farthest from hospitals were more likely to use health services and used health services more frequently. This suggests that more attention should be given to urban patients who live far away from health service providers in Shaanxi Province.
Keywords: health equity, accessibility, travel time, health service utilization
Introduction
Access to health care is a measure of human well-being that is limited by many factors of geographic variation.1,2 The most direct of these is the time it takes for individuals to travel to well-equipped and adequately staffed health care facilities. Due to the clustering of health care institutions in densely populated areas, individuals living in remote regions often experience increased health-related burdens, including travel times and related costs, when seeking health care.1
Many previous studies have assessed the correlation between travel time and health service utilization. In some developed countries, distance was not found to significantly influence the total number of routine or chronic care trips in older adults.3 However, in some developing countries, individuals living far away from health services have lower health care utilization rates.4
In China, the northwest part of the country has a large area, is not densely populated, and has relatively few health resources compared to areas in the eastern part with denser populations and adequate health resources.1,5 Even with the use of fast transportation, such as automobiles, the problem of accessibility of health resources remains prominent.1 Previous studies on distance and health care utilization in China have mostly focused on the eastern region.6,7 Considering the relatively low population density and the lack of health facilities in northwest China,8 the time and cost associated with accessing health care in this region may be increased.9 Exploring whether there are differences in health service utilization among residents with different travel times in this region not only reflects the accessibility of health services but also provides a certain basis for the optimal allocation of health resources, related policy formulation, and evaluation of expected effects. This study used data from the fifth Health Services Survey in Shaanxi province and aimed to explore health service utilization among residents with different travel times. Findings from this study may help provide policy insights for the balanced development of health resources in the region.
Materials and Methods
Source of Data
The data used in this study were obtained from the fifth Household Health Service Survey of Shaanxi Province in 2013, which was part of the National Health Service Survey (NHSS) in China.10 To obtain representative data of the whole population, multistage stratified cluster random sampling was used. In the first stage, 32 districts (counties) were randomly selected in Shaanxi Province according to their geographical and urban or rural distributions. In the second stage, five townships (streets) were randomly selected in each district (county). In the third stage, two villages (in rural areas), or committees (in urban areas) in each township or on each street were selected. The fourth stage randomly selected 60 households in selected villages or committees, and all residents of the sample households were included.10 For each household, face-to-face interviews were conducted by well-trained local investigators by using a structured household questionnaire developed by the Center for Health Statistics and Information of the Ministry of Health of China.10 The questionnaire covers general information, such as the socioeconomic and demographic characteristics of family members, self-reported diseases and injuries, and the utilization of health services. Informed consent was obtained by the surveyors before data collection. To ensure the quality of the data, 5% of the sampled households were revisited, and fourteen main questions were re-asked by survey supervisors. The consistency rate between the first and second visits exceeded 95%.10
In this study, we included individuals with a demonstrated need for health care services who reported an illness within the last 2 weeks before the survey. We excluded individuals who were <15 years old, with missing information, and with illogical answers. Finally, 9648 individuals were included in the empirical analysis.
Considering the substantial socioeconomic gap between rural and urban areas in China, rural residents are more likely to encounter obstacles (long distance from medical institutions, inconvenient transportation, and insufficient supply of specific experts),11 therefore, we analyzed rural and urban samples.
Measurement Indicators of Health Service Utilization by Patients
According to previous studies12,13 and our experience, we used the two-week health service utilization rate to reflect health service utilization. The two-week health services utilization rate is the number of health service utilizations in two weeks/the number of patients in two weeks. In addition, we also used the number of health service utilizations to reflect the frequency of health service utilization.
Travel Time to Health Services
In this study, we used the travel time to measure the accessibility to health services.14 Travel time was an independent question in the questionnaire: “What is the travel time to the nearest hospital (using the fastest method, such as walking or mechanical transportation)?”. We divided the answers into four different groups: less than 5 min, 5–14 min, 15–29 min, and more than 30 min.
Other Covariates
Four groups of factors were used in this study. Demographic characteristics included sex, age (15–44, 45–59, ≥ 60), marital status (unmarried, unmarried, divorced or widowed), family size (1–2, 3–4, or no less than 5 family members), employment status (employed, retired, or unemployed), and education level (illiterate, elementary, middle school, or high school and above). Health status characteristics included a history of chronic disease and the self-reported health condition. The self-reported health condition was reflected by the self-reported health score, which ranged from 0 to 100. According to a previous study,14 we divided self-reported health scores into three subgroups (<60, 60–79, 80–100). Health insurance status was divided into two categories according to any type of health insurance or not. Household economic status was reflected by self-reported annual household income. Annual household income was grouped into three quintiles (less than 20,000, 20,000–40,000, no less than 40,000 Yuan).
Statistical Analyses
We first analyzed health services utilization rates by travel time groups in the residents who reported illness in the 2 weeks before the survey. Then, we conducted binary logistic regression to examine the association between travel time and health service utilization. In addition, we conducted negative binomial regression to examine the association between travel time and the frequency of health services utilization.15
All statistics were performed by the R programming language (Version 4.0.5; R Foundation for Statistical Computing, Vienna, Austria). Binary logistic regression and negative binomial regression models were constructed using the “stats” and “MASS” packages, respectively. The criterion for statistical significance was P < 0.05.
Ethics Statement
This study was approved by the Ethics Committee of Xi’an Jiaotong University Health Science Center (approval NO. 2014–204) and conformed to the ethics guidelines of the Declaration of Helsinki. All data accessed complied with relevant data protection and privacy regulations.
Results
Description of the Study Sample
Among the 9648 patients who reported illness in the 2 weeks before the survey, 42.6% utilized health services, and the health service utilization rate was higher in rural areas than in urban areas (47.0% and 27.4%, respectively; significant P<0.05). The travel time to the nearest medical service exceeded 15 min for 30.9% of the patients, and this proportion was higher in rural than in urban residents (33.3% and 22.6%, respectively; significant P<0.05). In 12.4% of the patients, travel time to the nearest medical service exceeded 30 min, and this proportion was higher in rural than urban residents (15.1% and 3.0%, respectively; significant P<0.05) (Table 1).
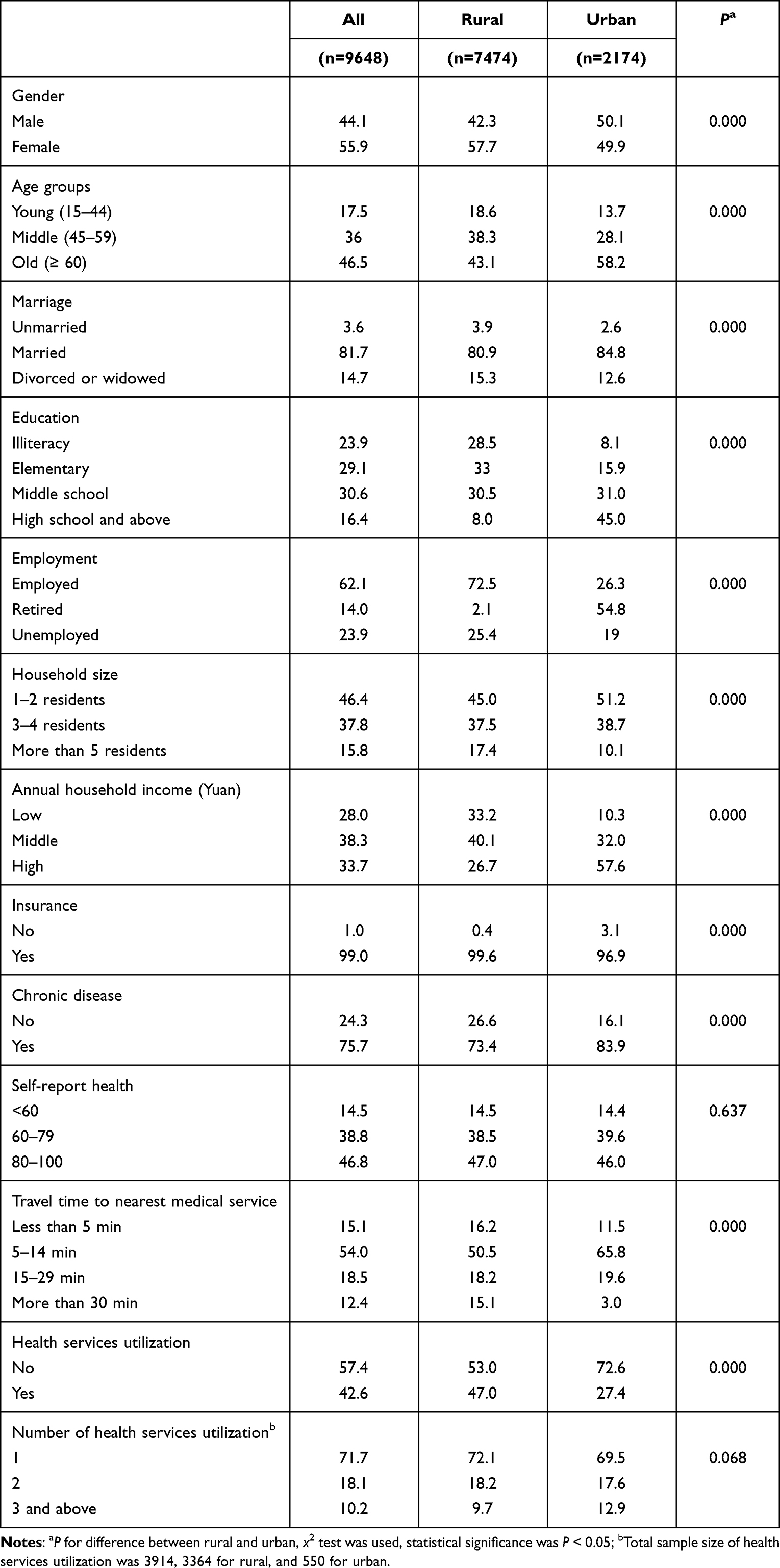 |
Table 1 Sample Characteristics of Survey Respondents Who Reported Illness in the 2 Weeks Before the Survey (%) |
Health Service Utilization by Travel Time
Figure 1 shows the health service utilization rate by travel time for rural and urban residents. As the travel time to the nearest medical service increased, the health service utilization rate decreased, but this decreasing tendency was reversed at a travel time ≥30 min. The health service utilization rate was highest in patients whose travel time to the nearest medical service exceeded 30 min.
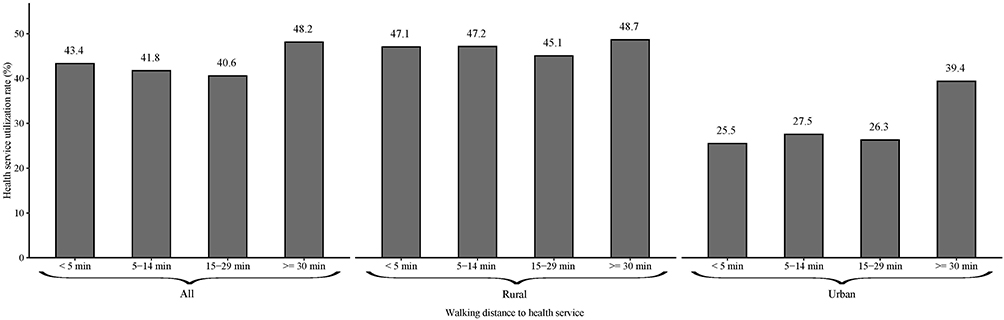 |
Figure 1 Health services utilization rate in different travel time. |
Association Between Travel Time and Health Service Utilization
Among the residents who reported illness in the 2 weeks before the survey, urban residents living farthest from health care facilities (more than 30 min) had a 2.12-fold higher probability of health service utilization than those with a travel time of less than 5 min. There was no significant correlation between travel time and health service utilization among rural residents (Table 2).
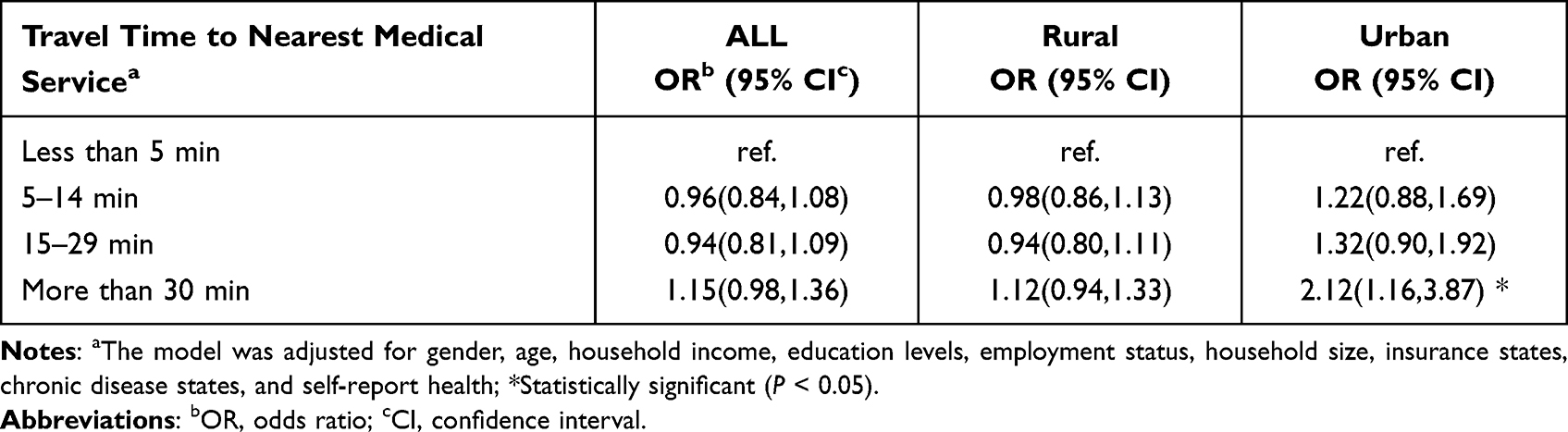 |
Table 2 Binary Logistic Regression for the Association Between Travel Time and Health Service Utilization |
Association Between Travel Time and Frequency of Health Service Utilization
While holding the other variables constant in the model, distant urban residents (travel time of more than 30 min) are expected to have a rate 1.77 times greater for health service utilization compared to the reference group (travel time of less than 5 min) (Table 3).
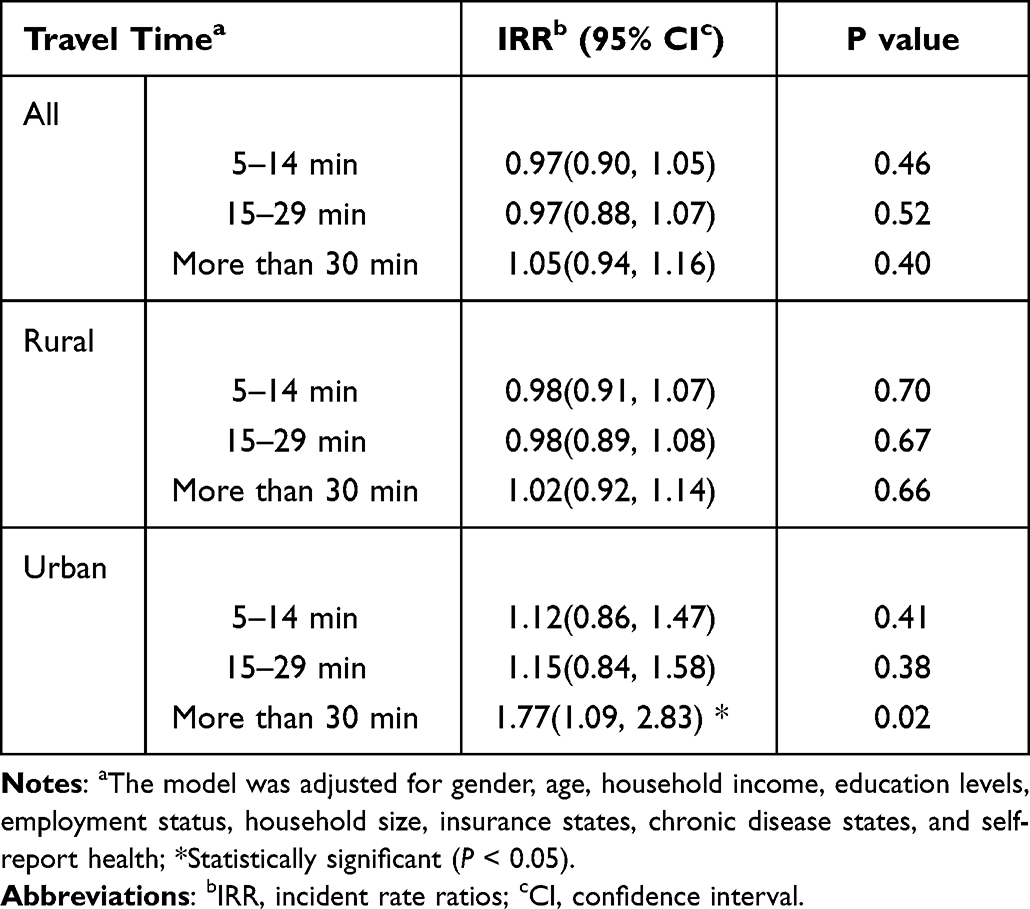 |
Table 3 Negative Binomial Regression of Association Between Travel Time and Frequency of Health Services Utilization |
Discussion
In this study, we analyzed health service utilization in a less developed area of China and the relationship between travel time to the nearest health care facility and the utilization of health services using population-representative data. The results showed that 42.6% of patients used health services (47.0% in rural areas and 27.4% in urban areas), and 30.9% of patients had a travel time longer than 15 min (33.3% in rural areas and 22.6% in urban areas). A total of 12.4% of the patients traveled more than 30 min to the nearest health care facility. Urban residents living farthest from health care facilities (travel time of more than 30 min) had a 2.12-fold higher probability of health service utilization and were expected to have a rate of health service utilization 1.77 times greater than those with a travel time of less than 5 min.
The results of this study showed that the rate of health service utilization among rural residents with an illness within two weeks before the survey was 47.0% in Shaanxi Province in 2013, which was higher than the previous national average (43.4%),16 but the rate of health service utilization among urban residents in Shaanxi Province with an illness within two weeks before the survey was lower than the national urban average (27.4% vs 32.3%).16 In recent decades, health service utilization in rural China has shown a significant increase,17 which may be attributed to the increasing income of rural residents. Additionally, the expansion of health insurance also played an important role in increasing health service utilization. Before 2003, more than 80% of the population in rural China was uninsured, but in 2008, more than 90% of the rural population was insured by a cooperative medical system/new rural cooperative medical system.17 For urban residents, previous studies have found that the health services utilization rate has declined in the last decade in China,16 and the decreased health service utilization rate in this region may be a result of that trend. In addition, the level of economic development in this region is lagging, and the utilization of health care resources is related to socioeconomic factors.18
Some studies have shown that dispersed populations and health care facilities inevitably cause some residents to spend more time accessing health services.19 This means that individuals have to travel a longer distance to access health services, and increases financial cost and time, which especially affects low-income groups who often bear more access costs because they often live in remote and poorly accessible areas.20 In this study, more than 30% of the residents who visited a doctor traveled for more than 15 min in Shaanxi Province; moreover, 15.1% of rural residents who visited a doctor travelled for more than 30 min. This indicator is not only higher than that of urban residents in Shaanxi Province but also much higher than that in large cities in eastern China.21 In the Healthy China 2030 Plan, the “15-min basic health service circle” is used as an evaluation index for healthy cities.22 Shaanxi Province also actively promotes the “15-min health service circle” in Guanzhong District and the mountain areas of Shannan and Shanbei districts. To reach these targets, more effective efforts are needed.
Although many studies have reported a negative correlation between distance/travel time to health services and health service utilization,4,23 some studies have shown that distance alone is not a sufficient measure of health care utilization among older adults.24 In addition, some studies found that health care utilization and disease burden increased as distance increased.25 In this study, we analyzed the correlation between travel time and health service utilization in Shaanxi Province. The results of this study showed that urban patients living far away from hospitals were more likely to use health services. To better understand the relationship between travel time and health care utilization behavior, this study also explored the relationship between travel time and the number of visits to health care facilities. The results of this study revealed that urban residents living farthest from health services (more than 30 min) had a 1.77 times greater health service utilization rate than urban residents living near health services (travel time less than 5 min). One possible explanation for this correlation is poor health outcomes for patients living far away from healthcare facilities. A previous study showed that the further a patient lived from health care facility they needed to attend, the worse health outcomes they experienced.26 Moreover, poor physical condition has been associated with a higher rate of health service utilization, which may result in a higher utilization rate among remote urban patients.
Interestingly, in our study, we did not find an association either between travel time and health service utilization or between travel time and the number of visits to health care facilities among rural patients. The establishment of a network of rural health care systems, the availability of modern transportation, the establishment of a quality public transportation network, and a coverage rate of more than 90% by the cooperative medical system/new rural cooperative health system17 have all improved health care accessibility among rural residents and reduced the impact of distance to health services on utilization behavior.
This study explored health service utilization and the relationship between travel time and the utilization of health services in a less developed region of China by using representative data, and the findings may provide useful information for understanding health service utilization in this region. However, there are several limitations to this study. First, the travel time data in this study were self-reported and thus subject to recall bias. Second, this study was a cross-sectional study and cannot determine the causal relationship between travel time and health service utilization. Third, we did not include children under 15 years age in our study. To better understand the situation of health service utilization in Northwest China, future studies on frequent health service utilization among children are needed. Fourth, the data used in this study were collected in 2013, and they are now slightly out of date, future studies using the latest data are needed. Finally, although this study explored the relationship between travel time and the utilization of health services, it did not include different types of disease. To better understand the relationship between travel time and the utilization of health services, future studies considering different diseases are needed.
Conclusion
In conclusion, there is no correlation between travel time and health service utilization among rural residents in Shaanxi Province. However, urban patients living farthest from hospitals were more likely to use health services. In addition, these urban patients used health services more frequently. This suggests that urban residents living at a distance from hospitals in Shaanxi Province need more attention.
Data Sharing Statement
The data used in this study are available from Shaanxi Health and Family Planning Commission but restrictions apply to the availability of these data, which were used under license for the current study, and so are not publicly available. Data are however available from the authors upon reasonable request and with permission of the Shaanxi Health and Family Planning Commission.
Acknowledgments
This research was funded by National Natural Science Foundation of China, grant number 72104113. The funder had no role in the design of the study; the collection, analysis, and interpretation of data; or the writing of the manuscript. We are grateful to the individuals who participated in the study.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Weiss DJ, Nelson A, Vargas-Ruiz CA, et al. Global maps of travel time to healthcare facilities. Nat Med. 2020;26(12):1835–1838. doi:10.1038/s41591-020-1059-1
2. GBD 2016 Healthcare Access and Quality Collaborators. Measuring performance on the Healthcare Access and Quality Index for 195 countries and territories and selected subnational locations: a systematic analysis from the Global Burden of Disease Study 2016. Lancet. 2018;391(10136):2236–2271.
3. Mattson J. Transportation, distance, and health care utilization for older adults in rural and small urban areas. Transp Res Rec. 2011;2265(1):192–199. doi:10.3141/2265-22
4. Girma F, Jira C, Girma B. Health services utilization and associated factors in Jimma zone, South west Ethiopia. Ethiop J Health Sci. 2011;21(Suppl 1):85–94.
5. Zhang T, Xu Y, Ren J, Sun L, Liu C. Inequality in the distribution of health resources and health services in China: hospitals versus primary care institutions. Int J Equity Health. 2017;16(1):42. doi:10.1186/s12939-017-0543-9
6. Tao Z, Yao Z, Kong H, Duan F, Li G. Spatial accessibility to healthcare services in Shenzhen, China: improving the multi-modal two-step floating catchment area method by estimating travel time via online map APIs. BMC Health Serv Res. 2018;18(1):345. doi:10.1186/s12913-018-3132-8
7. Liu J, Yin H, Zheng T, et al. Primary health institutions preference by hypertensive patients: effect of distance, trust and quality of management in the rural Heilongjiang province of China. BMC Health Serv Res. 2019;19(1):852. doi:10.1186/s12913-019-4465-7
8. Zhu J, Zhang Q, Jia C, et al. Epidemiological characteristics and clinical outcomes of coronavirus disease patients in northwest china: high-volume research from low population density regions. Front Med. 2020;7:564250. doi:10.3389/fmed.2020.564250
9. Love D, Lindquist P. The geographical accessibility of hospitals to the aged: a geographic information systems analysis within Illinois. Health Serv Res. 1995;29(6):629.
10. Xu Y, Gao J, Zhou Z, et al. Measurement and explanation of socioeconomic inequality in catastrophic health care expenditure: evidence from the rural areas of Shaanxi Province. BMC Health Serv Res. 2015;15:256. doi:10.1186/s12913-015-0892-2
11. Fan X, Su M, Zhao Y, Si Y, Zhou Z. Trends in equity of inpatient health service utilization for the middle-aged and elderly in China: based on longitudinal data from 2011 to 2018. BMC Public Health. 2021;21(1):1162. doi:10.1186/s12889-021-11203-y
12. Qian Y, Zhou Z, Yan J, et al. An economy-related equity analysis of health service utilization by women in economically underdeveloped regions of western China. Int J Equity Health. 2017;16(1):186. doi:10.1186/s12939-017-0667-y
13. Carrasquillo O. Health Care Utilization. In: Gellman MD, Turner JR, editors. Encyclopedia of Behavioral Medicine. New York: Springer New York; 2013:909–910.
14. Zhang Y, Zhou Z, Si Y. When more is less: what explains the overuse of health care services in China? Soc Sci Med. 2019;232:17–24. doi:10.1016/j.socscimed.2019.04.018
15. Trivedi PK. Models for Count Data. In: Culyer AJ, editor. Encyclopedia of Health Economics. San Diego: Elsevier; 2014:306–311.
16. Liu M, Zhang Q, Lu M, Kwon CS, Quan H. Rural and urban disparity in health services utilization in China. Med Care. 2007;45(8):767–774. doi:10.1097/MLR.0b013e3180618b9a
17. Zhou Z, Su Y, Gao J, et al. Assessing equity of healthcare utilization in rural China: results from nationally representative surveys from 1993 to 2008. Int J Equity Health. 2013;12(1):34. doi:10.1186/1475-9276-12-34
18. Zhang X, Wu Q, Shao Y, Fu W, Liu G, Coyte PC. Socioeconomic inequities in health care utilization in China. Asia Pac J Public Health. 2015;27(4):429–438. doi:10.1177/1010539514565446
19. Goodman DC, Fisher E, Stukel TA, Chang C. The distance to community medical care and the likelihood of hospitalization: is closer always better? Am J Public Health. 1997;87(7):1144. doi:10.2105/AJPH.87.7.1144
20. Chan L, Hart LG, Goodman DC. Geographic access to health care for rural Medicare beneficiaries. J Rural Health. 2006;22(2):140–146. doi:10.1111/j.1748-0361.2006.00022.x
21. Zhu L, Zhong S, Tu W, et al. Assessing spatial accessibility to medical resources at the community level in Shenzhen, China. Int J Environ Res Public Health. 2019;16(2). doi:10.3390/ijerph16020242
22. Chen J, Bai Y, Zhang P, et al. A spatial distribution equilibrium evaluation of health service resources at community grid scale in Yichang, China. Sustainability. 2020;12(1):52. doi:10.3390/su12010052
23. Raknes G, Hansen EH, Hunskaar S. Distance and utilisation of out-of-hours services in a Norwegian urban/rural district: an ecological study. BMC Health Serv Res. 2013;13(1):222. doi:10.1186/1472-6963-13-222
24. Nemet GF, Bailey AJ. Distance and health care utilization among the rural elderly. Soc Sci Med. 2000;50(9):1197–1208. doi:10.1016/S0277-9536(99)00365-2
25. Billi JE, Pai CW, Spahlinger DA. The effect of distance to primary care physician on health care utilization and disease burden. Health Care Manage Rev. 2007;32(1):22–29. doi:10.1097/00004010-200701000-00004
26. Kelly C, Hulme C, Farragher T, Clarke G. Are differences in travel time or distance to healthcare for adults in global north countries associated with an impact on health outcomes? A systematic review. BMJ Open. 2016;6(11):e013059–e013059. doi:10.1136/bmjopen-2016-013059
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.