")
Back to Journals » Local and Regional Anesthesia » Volume 7
Is there a difference in postdural puncture headache after continuous spinal anesthesia with 28G microcatheters compared with punctures with 22G Quincke or Sprotte spinal needles?
Received 4 June 2014
Accepted for publication 8 September 2014
Published 10 November 2014 Volume 2014:7 Pages 63—67
DOI https://doi.org/10.2147/LRA.S68828
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Stefan Wirz
Eberhard Albert Lux, Astrid Althaus
Fakultät für Gesundheit der Universität, Witten-Herdecke, Germany
Abstract: In this retrospective study, the question was raised and answered whether the rate of postdural puncture headache (PDPH) after continuous spinal anesthesia with a 28G microcatheter varies using a Quincke or a Sprotte needle. The medical records of all patients with allogenic joint replacement of the knee or hip or arthroscopic surgery of the knee joint undergoing continuous spinal anesthesia with a 22G Quincke (n=1,212) or 22G Sprotte needle (n=377) and a 28G microcatheter during the past 6 years were reviewed. We obtained the approval of the ethical committee. The rates of PDPH were statistically not different between both groups: 1.5% of patients developed PDPH after dura puncture with a Quincke needle and 2.1% with a Sprotte needle in women and men.
Keywords: continuous spinal anesthesia, postdural puncture headache (PDPH), Sprotte needle, Quincke needle
Introduction
Continuous spinal anesthesia (CSA) is a well-known anesthetic technique. Because of the possibility of titrating the anesthetic effect with small dosages of local anesthetics, the systemic toxic effects in comparison with epidural anesthesia are decreased. Additionally, the extension of the anesthetic effect by supplemental application of spinal local analgesics during surgery is possible.1–3
CSA can be realized today with small needles and catheters with different techniques (catheter applied over or through the needle).1–5 Postdural puncture headache (PDPH) is defined as a headache that begins 24–28 hours after puncturing the dura with frontal or neck pain and that continually grows over approximately 15 minutes after the patient sits up. Often, it is observed in combination with neck rigidity and rarely with tinnitus, photophobia, nausea, or defective hearing. Rates of PDPH are defined by diameter and architecture of the needles used.1,4,5
The pathophysiology of PDPH is characterized by the loss of cerebral fluid with the consequence for the CNS not being able to be sufficiently carried by the cerebral fluid. In a sitting posture, this can result in stress on the meninges, blood vessels, and nerves for the patient. The development of microcatheters (28G–32G) has significantly reduced the incidence of this complication.6–8 From single-shot spinal anesthesia it is well known that an optimized architecture of the needle tip can have a significant influence on the development of PDPH, whereas the way the dura is punctured is crucial.4
In how far this difference can come into effect during CSA, where the catheter is lodged into the dura causing a fast plugging of the puncture, has never been discussed in studies before. Only three large (n≥100 patients) studies on CSA with 28G microcatheters have investigated the problem of PDPH in orthopedic patients.7–9 These studies only referred to puncture needles with Quincke tips. Other needle types were not referred to.
The aim of the present retrospective study was to analyze the influence of the architecture of the needle tip (Sprotte versus Quincke 22G needle) by using CSA with 28G microcatheters (catheter through a needle) and the development of PDPH in a larger patient population.
Methods
Patients
The medical records of all our patients with allogenic joint replacement of the knee or hip or arthroscopic surgery of the knee joint undergoing CSA with a 22G Quincke (n=1,212) or 22G Sprotte needle (n=377) and a 28G microcatheter during the past 6 years were reviewed. We obtained the approval of the ethical committee. All patients were informed about potential complications, and written informed consent for anesthesia was obtained. Only three anesthesiologists experienced in CSA performed all CSAs. Contraindications for CSA were lack of patient compliance, pathological coagulation (Quick test <50%, partial thromboplastin time (PTT) >50 sec, platelets <50,000 gigaparticles/L), local infection in the area of puncture, and severe deformity of the spinal column with low expectancy of successful puncture of the spine.
A questionnaire (pain, vomiting, complaints lasting >24 hours postoperatively, and also postoperative headaches) for all patients undergoing anesthesia was personally dispensed on the third postoperative day and returned to anesthesiologists or pain nurses. If patients reported headache, the anesthesiologists were informed and examined the patients.
Devices
In this study we used needles and microcatheters from Kendall Inc., Neustadt, Germany. The Cospan Kit included a 22G Quincke needle (Group 1) and a 22G Sprotte needle (Group 2) and a 28G microcatheter.
Clinical procedure
For oral premedication, 50 mg of dikaliumclorazepat (Sanofi-Winthrop, Kent, UK) was given. The choice of median or lateral access for spinal puncture in a sitting position of the patients at L3/4 or L4/5 and the use of a Quincke or Sprotte needle was decided by the anesthesiologist. The dura was punctured with the cutting surface in a lateral direction by using the Quincke needle and by using the Sprotte needle with the needle opening pointed upward. Prior to the insertion of the catheter, the opening of the needle was turned in a cranial direction. The anesthesiologists advanced the catheter 2–4 cm into the intrathecal space. Cerebrospinal fluid was aspirated, and subsequently 0.5 mL bupivacaine 0.5% hyperbar to a maximum of 2.5 mL was given, with the patient in a horizontal position. To maintain sufficient anesthesia, operative single doses of 1.0 mL bupivacaine 0.5% isobar were injected if essential.
The postoperative pain therapy was organized for at least 24 hours with continuous infusion of 1.6–2.2 mL/h bupivacaine 0.08% isobaric, and the spinal catheter was removed on the second postoperative day by the anesthesiologist. In addition, pain was treated with metamizole sodium (Aventis Pharma, Strasbourg, France). Every patient was treated with medication to prevent PDPH, such as caffeine, gabapentin, or aminophylline. Patients with headache were interviewed and examined clinically to determine the type of headache (PDPH, migraine, tension headache, meningitis). To diagnose PDPH, the main criterion was an increase in intensity of ventral or nuchal headache in a standing or sitting position. Patients with PDPH were treated for 24 hours with bed rest, a nonsteroidal anti-inflammatory drug, and crystalloid infusions. If this treatment failed, the patients received a blood patch with 10 mL of autologous blood.
Data and statistics
The clinical data from records of 1,589 patients with CSA were analyzed. This study is a retrospective analysis with all of their limitations. Difficulties in the procedure of the puncture and positioning of the catheters are not commonly described in the records. A special severity scoring protocol for headaches was not used. Descriptive statistics were used to characterize the patient population and rates of PDPH. Statistical analysis (chi-squared test) was performed with Excel 2013 (Microsoft, Redmond, WA, USA).
Results
Patients
The patient population group with a Quincke needle included 825 females (68%) and 387 (32%) males. The patients had a median (interquartile range) age of 61 years (56–76 years), with a minimum–maximum range of 28–90 years. The types of operations performed were 843 hip prostheses, 264 knee prostheses, and 105 arthroscopic surgeries of the knee joint.
The patient population group with a Sprotte needle (Table 1) included 226 females (60.0%) and 151 (40.0%) males. The patients had a median (interquartile range) age of 57 years (52–70), with a minimum–maximum range of 20–82 years. The types of operations performed were 238 hip prostheses, 122 knee prostheses, and 17 arthroscopic surgeries of the knee joint.
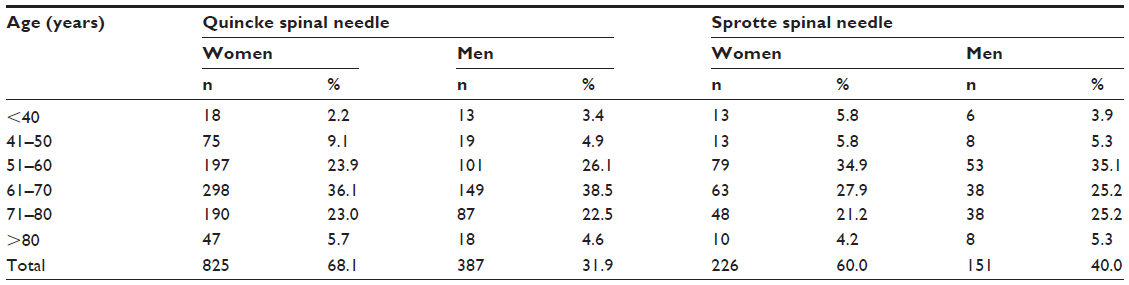 | Table 1 Age and sex of patients with continuous spinal anesthesia by 22G Quincke (n=1,212) or Sprotte spinal needles (n=377) and a 28G microcatheter |
In points of age, sex, and surgical procedure, the groups were not significantly different (Table 1).
PDPH
In the group with CSA with a Quincke needle, tension headaches were experienced by 190 (15.7%) patients, of whom 27 received therapy (2.2%). Postpuncture headaches were experienced by 18 (1.5%) patients – 14 women (1.6% of the women) and four men (1.0% of the men) (Table 2). Therapeutic intervention consisted of bed rest, infusions of crystalloids, and application of a nonsteroidal anti-inflammatory drug. If this treatment failed (n=4), patients received a blood patch with 10 mL of autologous blood and were immediately pain free.
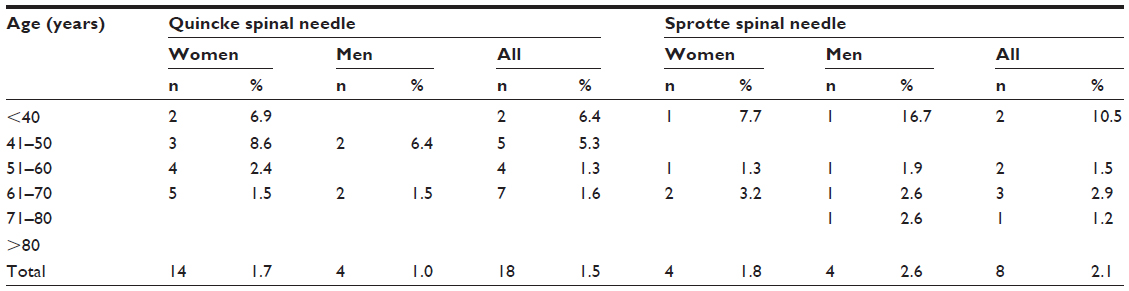 | Table 2 Postdural puncture headache in women and men after continuous spinal anesthesia (SPA) with 22G Quincke or Sprotte spinal needle and a 28G microcatheter (n=825) |
In the group with a Sprotte needle, we observed 60 (15.9%) patients with tension headaches, of whom 14 (3.7%) received therapy. Eight (2.1%) had typical PDPH – four women (1.8% of the women) and four men (2.6% of the men) (Table 2). One of them received a blood patch and was immediately pain free.
Between the patients treated with a “Quincke spinal needle” and treated with a “Sprotte spinal needle” there was not a significant difference regarding sex (chi-square <0.00, P=0.95) or age (chi-square <0.00, P=1.00).
There was no significant difference between the patients treated with a “Quincke spinal needle” and those treated with a “Sprotte spinal needle” regarding the number of patients who suffered from PDPH (chi-square <0.37, P=0.54).
Discussion
CSA provides a number of potential advantages over other forms of anesthesia.1–3 The use of microcatheters was restricted due to governmental concern on the risk of cauda equina syndrome. However, many anesthesiologists are also uncertain about the incidence of PDPH after CSA and in handling of CSA for anesthesia and postoperative pain management. PDPH is one of the most common complications after spinal anesthesia. Patients after spinal anesthesia often suffer headaches – men and women alike. Only a small number of them develop a typical PDPH.
In contrast to single-shot anesthesia, we could not show that an optimized architecture of the needle tip has an influence on the rate of PDPH. Needles with pencil point architecture of the tip cut the dura fibers less when separating the tissue, and this allows the tissue to close after retraction of the needle.4 This hypothesis was confirmed in a human postmortem thoracolumbar dura mater model. There was a leak reduction of 46% when using a Whitacre needle compared with a Quincke needle.10
Schmittner et al11 found in 363 patients with comparison puncture of the dura with a 27G Quincke versus a 27G pencil point needle a difference in PDPH from 6.6% to 1.7%. Flaatten et al12 found a similar result. They observed 301 patients – 153 with a pencil point needle and 148 with a Quincke needle. There were three cases (2.0%) of PDPH in the first group and 12 (8.1%) in the second group. Santanen et al13 confirmed these results.
Mihic14 found out that the incidence of PDPH was lower when a cutting Quincke needle was inserted parallel to the longitudinal dural fibers than if it was at a right angle to them. This was also our method in using Quincke needles.
In our patients, we found a rate of PDPH from 1.6% to 1.5% in the Quincke needle group and 2.1% in the Sprotte needle group. This result is not different from PDPH after single-shot anesthesia with 27G pencil point needles. Hence, the typical rate of developing a PDPH seems less when using spinal catheters than with single-shot spinal anesthesia with a 22G needle.11–13
The theory of Denny et al15 was that an inflammatory reaction develops in the surrounding area of the puncture site. When the catheter is removed, the edema or fibrous exudate reduces the leaking into the dura. Culling et al16 could not show a reduction of PDPH after puncture of the dura mater with an 18G Quincke needle and insertion of a microcatheter for surgical, rather than obstetrical, procedures, where the catheter was removed postoperatively after 3 hours. They observed a typical PDPH in eight out of 36 patients aged 63 years (32–77 years), on average. The headache rate was even higher than the PDPH rate expected after single-shot anesthesia.4
Standl et al,8 in contrast, concludes that the temporary sealing of the dural hole by the microcatheter may additionally reduce the risk of a PDPH where the spinal catheter was removed 24 hours postoperatively. Out of 100 patients aged, on average, 62.5 years, only one patient developed a PDPH. The theory of Denny et al15 is assisted by Yang et al,17 who showed that PDPH is increased after treatment with dexamethasone.
It has been shown that the application of the stylet into the spinal needle prior to the drawback out of the cerebral spinal fluid space can reduce the rate of PDPH. It is supposed that the arachnoidea is drawn less into the needle and hence is damaged less. This mechanism can also be possible with the use of CSA.5
The use of a Sprotte needle has no advantages. In contrast, the puncture with a Sprotte needle is more difficult for the untrained physician, and Van den Berg et al18 found more iatrogenic response using the pencil point needle versus a cutting-edge needle. Attempts in performing the CSA were interesting to discuss, but in the records these data were not commonly noted, so we cannot discuss this interesting fact with our data.
The rates of PDPH in using CSA – also with microcatheters – for anesthesia in cesarean section17,18 are clearly higher than in other fields of surgery. It has long been known that CSA is particularly beneficial for elderly patients. In elderly age groups, PDPH occurs only very seldom in CSA or single-shot spinal anesthesia.9,19 We recorded no cases of PDPH in patients aged >80 years.
Our data show no difference in the use of CSA with 28G microcatheters after puncture of the dura with a 22G Quincke or Sprotte needle with regard to PDPH. The rate of PDPH was comparable with use of single-shot anesthesia and needles with an optimized tip (27G) in men and women as they are commonly used today. To provide CSA, puncture with a Sprotte needle is more difficult for the untrained physician and has no advantages in the field of PDPH. There is no difference in PDPH after CSA with Quincke or Sprotte needles, but it may cause inflammation in the puncture region of the dura mater. Future structured studies have to confirm this theory.
Disclosure
Lecture fee sponsored by Almirall, Beta-Pharm, Grünenthal, Hexal, Mundipharma, OMT, and TEVA. The authors report no conflicts of interest in this work.
References
Hurley RJ, Lambert DH. Continuous spinal anaesthesia with a micro catheter technique: preliminary experience. Anesth Analg. 1990;70(1):97–102. | |
Moore JM. Continuous spinal anesthesia. Am J Therapeutics. 2009;16(4):289–294. | |
Maurer K, Bonvini JM, Ekatodramis G, Serena S, Borgear A. Continuous spinal anaesthesia/analgesia vs single-shot spinal anaesthesia with patient-controlled analgesia for elective hip arthroplasty. Acta Anaesthesiol Scand. 2003;47(7):878–883. | |
Hess JH. Postdural puncture headache: a literature review. AANA J. 1991;59(6):549–555. | |
Radke K, Radke OC. Post-dural puncture headache. Anaesthesist. 2013;62(2):149–159. | |
Peyton PJ. Complications of continuous spinal anaesthesia. Anaesth Intens Care. 1992;20(4):417–438. | |
Poulakka R, Haasio J, Pitkänen MT, Kallio M, Rosenberg PH. Technical aspects and postoperative sequelae of spinal and epidural anaesthesia: a prospective study of 3230 orthopedic patients. Reg Anesth Pain Med. 2000;25(5):488–497. | |
Standl T, Eckert S, Schulte am Esch J. Micro catheter continuous spinal anaesthesia in the post-operative period: a prospective study of its effectiveness and complications. Eur J Anesthesiol. 1995;12(3):273–279. | |
Döhler S, Klippel A, Richter S. Kontinuierliche Spinalanästhesie bei Patienten in hohem Lebensalter und mit hohem Anästhesierisiko bei traumatologisch-orthopädischen und allgemeinchirurgischen Eingriffen. Anaesthesiol Reanimat. 1999;24(6):157–163. | |
Cruickchank RH, Hopkinson SM. Fluid flow through dural puncture sites. Anaesthesia. 1989;44:415–418. | |
Schmittner MD, Urban N, Janke A, et al. Influence of the pre-operative time in upright sitting position and the needle type on the incidence of post-dural puncture headache (PDPH) in patients receiving a spinal saddle block for anorectal surgery. Int J Colorectal Dis. 2011;26:97–102. | |
Flaatten H, Felthaus J, Kuwelker M, Wisborg T. Postural post-dural puncture headache. A prospective randomised study and a meta-analysis comparing two different 0.40 mm OD (27 g) spinal needles. Acta Anaesthesiol Scand. 2000;44:643–647. | |
Santanen U, Rautoma P, Luurila H, Erkola O, Pere P. Comparison of 27-gauge (0.41-mm) Whitacre and Quincke spinal needles with respect to post-dural puncture headache and non-dural puncture headache. Acta Anaesthesiol Scand. 2004;48:474–479. | |
Mihic DN. Postspinal headache and relationship of needle bevel to longitudinal dural fibers. Reg Anest. 1985;10:76–81. | |
Denny N, Masters D, Pearson J, Read M, Sikota M, Selander D. Postdural puncture headache after continuous spinal anesthesia. Anesth Analg. 1987;66(8):791–794. | |
Culling RD, Baxter G, Menk EJ. Incidence of postdural puncture headache after continuous spinal anaesthesia. Anesthesiology. 1989;71:A723. | |
Yang B, Li DL, Dong P, Zhang XY, Zhang L, Yu JG. Effect of dexamethasone on the incidence of post-dural puncture headache after spinal anesthesia: a randomized, double-blind, placebo-controlled trial and a meta-analysis. Acta Neurol Belg. Epub May 28, 2014. | |
Van den Berg AA, Ghatge S, Armendariz G, Cornelius D, Wang S. Response to dural puncture puncture during institution of combined spinal-epidural analgesia: a comparison of 27 gauge pencil-point and 27 gauge cutting-edge needles. Anaesth Intensive Care. 2011;39:247–251. | |
Kumar CM, Corbett WA, Wilson RG. Spinal anaesthesia with a micro-catheter in high-risk patients undergoing colorectal cancer and other major abdominal surgery. Surg Oncology. 2008;17(2):73–79. |
 © 2014 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2014 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.