")
Back to Journals » International Medical Case Reports Journal » Volume 15
Is It a Coincidence or Secondary Immune Thrombocytopenic Purpura? A Case of an 11-Year-Old Male Patient at Hawassa University Comprehensive Specialized Hospital, Hawassa, Sidama, Ethiopia
Authors Ketema W , Taye K , Tagesse N, Eifa A
Received 26 December 2021
Accepted for publication 24 February 2022
Published 5 March 2022 Volume 2022:15 Pages 85—90
DOI https://doi.org/10.2147/IMCRJ.S355892
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Ronald Prineas
Worku Ketema,1 Kefyalew Taye,1 Negash Tagesse,1 Aberash Eifa2
1Department of Paediatrics and Child Health, Hawassa University Comprehensive Specialized Hospital, Hawassa, Ethiopia; 2Department of Midwifery, Hawassa University Comprehensive Specialized Hospital, Hawassa, Ethiopia
Correspondence: Worku Ketema, Email [email protected]
Background: Isolated thrombocytopenia with normal levels of other cell lines in the absence of other reasons is referred to as “immune thrombocytopenic purpura” (ITP). Tuberculosis has been associated with a variety of hematologic abnormalities, although severe thrombocytopenia and tuberculosis presenting as immune thrombocytopenic purpura are extremely uncommon.
Case Presentation: We discuss a case of an 11-year-old male adolescent who came with epistaxis and petechial rash lasting one day, as well as severe thrombocytopenia. Following the clinical diagnosis of ITP, the patient was started on prednisone, transfused with platelets, and later started on antituberculosis (ATT) after confirmation of tuberculosis. The patient had a satisfactory response during the course of treatment, and the platelet level was fully recovered after 6 months.
Conclusion: Tuberculosis (TB) should be recognized as a cause of immunological thrombocytopenia in tuberculosis-endemic areas. Our patient’s platelet count improved after 1 week of ATT and 2 weeks of prednisolone, and it was entirely restored after 6 months of ATT treatment. Unfortunately, there are no clear guidelines for treating TB-related immune thrombocytopenia or determining the cause of TB-related immune thrombocytopenia. Tuberculosis-induced ITP resolves with the ATT, even though more investigation is warranted.
Keywords: immune thrombocytopenic purpura, tuberculosis, prednisolone
Introduction
Immune thrombocytopenia is an autoimmune illness defined by an isolated thrombocytopenia with or without mucocutaneous hemorrhage. It is an exclusionary diagnosis.1–3 In most cases, the origin of ITP is unknown, but it might be induced by a viral infection or other immunologic or environmental factors. Immune thrombocytopenia in tuberculosis is uncommon, with only a few cases reported to date.2,4,5
In ITP, thrombocytopenia is defined as a platelet count of 100,000/microL or below.4,6,7 However, in most case studies, the presenting platelet count is less than 30,000/microL, which is likely due to the fact that patients with mild illnesses are less likely to experience bleeding and may never seek medical help.5,8–11 At the time of presentation, approximately 80% of children with ITP had platelet counts of 20,000/microL, and around 45% had platelet counts of 10,000/microL. Anemia can occur in children who have had a lot of ITP-related bleeding (eg, epistaxis or vaginal). Microcytic anemia is common in this situation.6,7,12
Various hematologic abnormalities have been seen in tuberculosis, including anemia, leucocytosis, monocytosis, lymphopenia, leukopenia, thrombocytopenia, thrombocytosis, leukemoid reactions, and pancytopenia,5,13 but severe thrombocytopenia and tuberculosis presenting as immune thrombocytopenic purpura is rare.5,8,14 Several factors have been linked to infection-related bleeding, the most prevalent of which is thrombocytopenia. In most cases, thrombocytopenia appears to be caused by increased platelet destruction, such as from DIC or septicaemia without evidence of DIC, platelet adhesion to injured vascular surfaces, or direct platelet toxicity induced by the pathogen, or bone marrow involvement.15,16
ITP in tuberculosis is complex and can be explained by a variety of mechanisms:17,18 (A) antiplatelet antibodies may be shared by mycobacterium TB and platelets or platelet-associated immunoglobulin, resulting in immune-mediated platelet death, (B) reduced platelet production as a result of bone marrow infiltration, (C) tuberculosis-induced hemophagocytic syndrome, (D) antiplatelet antibodies can be generated by mycobacterium TB activating a clone of B-lymphocytes.19
Although the most important treatment for infection-related thrombocytopenia is to treat the underlying infection, treatment decisions for immune thrombocytopenic purpura are still debatable. They may include single or combination corticosteroid therapy, intravenous immunoglobulin (IVIg) therapy depending on the degree of thrombocytopenia or hemorrhage.20,21
There are varieties of corticosteroid dosing regimens. In a meta-analysis published in 2016, two of the most prevalent regimens were compared. The first treatment consists of one to three cycles of high-dose dexamethasone (40 mg/d for four days) with no tapering. Oral prednisone (1 mg/kg/d) for 2–4 weeks with a progressive taper is the second most popular treatment. The first regimen had a larger total platelet count response at 14 days, but there was no difference in long-term platelet count response between the two regimens.20,21
Tuberculosis associated ITP is one of the rarest clinical scenarios and we report a case of an 11-year-old male adolescent who came from Oromia region, Guji zone.
Ethical Review
After obtaining approval from the Hawassa University Institutional Review Board (IRB), the mother of the patient provided written informed consent for the publication of this case report.
Case Presentation
An 11-year-old male came to our hospital with a complaint of bilateral nasal bleeding of 1 day duration, which was of about 4 times, and it was massive as claimed by the family. He also has had associated history of skin rash which was noticed a day prior to the onset of nasal bleeding.
On further asking, the patient has had history of loss of appetite and significant but unquantified weight loss of one month duration but no history of fever or cough. He has no history of bleeding diseases, connective tissue disorders, autoimmune disorders, or cancer in himself or in his family. All vital signs were normal at the time of presentation, but there was a dry clot in the nostril bilaterally and no symptoms of anemia. A chest examination revealed scattered inspiratory crackles on both sides of the upper lung zone. Organomegaly, there was nothing. A petechial rash covered the chest and rear sides of the body, including the upper extremities.
Except for isolated thrombocytopenia, a complete blood count and serum chemistry, including the reticulocyte count, were unremarkable. A peripheral blood smear revealed isolated severe thrombocytopenia with normal blood cell morphology. Autoimmune screening (ANA, Coombs test), coagulation profile, viral screening including the COVID-19 test, blood cultures, urine cultures, were all non-revealing. The rate of erythrocyte sedimentation (ESR) was 70 mm/hr, which is suggestive of MTB. A smear for acid-fast bacilli was negative, but Gene expert from the sputum detected MTB with rifampicin sensitivity (Table 1).
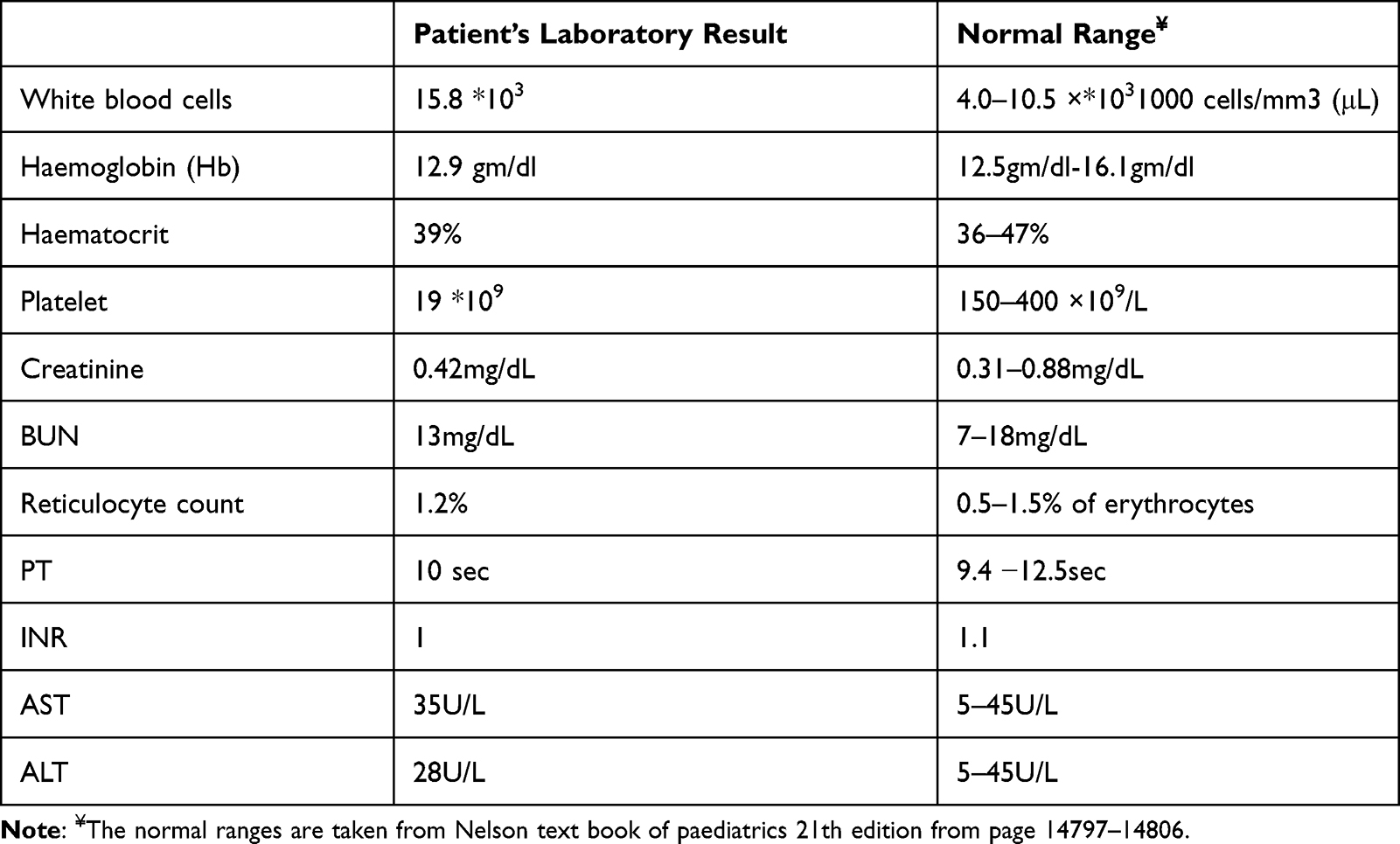 |
Table 1 The Laboratory Results of an 11-Year-Old Boy Patient Who Presented with a One-Day History of Bilateral Nasal Bleeding are Shown in the Table Below |
The ultimate outcome of the chest X-ray revealed bilateral diffusely dispersed nodular opacities all over the lung fields, which were commented on by three different radiologists(Figure 1).
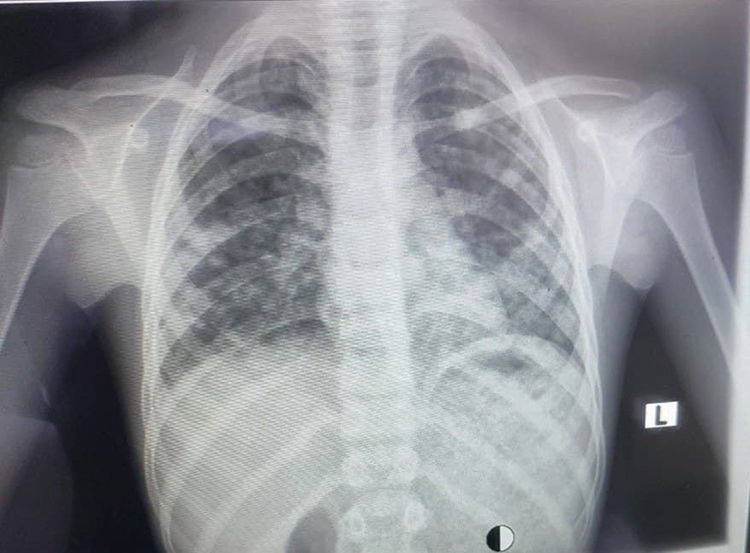 |
Figure 1 Depicts the patient’s chest X-ray feature, which was commented on by three independent radiologists; bilateral diffusely scattered nodular opacities all throughout the lung fields. |
With a presumptive diagnosis of immune thrombocytopenic purpura (ITP), the patient was hospitalised and began therapy with oral prednisolone 20 mg twice a day.
He was then managed with antituberculosis (ATT) RHZ (75/50/150) 4 tablets, and E100 mg (R stands for Rifampicin, H for Isoniazid, Z for Pyrazinamide, and E for Ethambutol in this order). Four tablets as per the national guideline, which was started after 1 week of admission because of late isolation of TB.22
Prednisolone 2mg/kg/day, ie 20 mg po bid (tapered over six weeks and stopped), and there were no reported problems of initial complaints after withdrawing the prednisolone.
He was transfused with Platelet 20 mg/kg, ie 400 mg, with post-transfusion CBC of almost the same, supporting the diagnosis of ITP.
This patient was discharged after 2 weeks of hospitalization, being taking ATT and Prednisolone, with the latest platelet count of 44,000*109, with appointment after 2 weeks or to come early if there are any complications. Fortunately, there were no complications related to the disease/or treatment, and on the day of appointment (after a total duration of 1 month of treatment and 31 days of the complaint), repeated CBC was done, and it showed Platelet count of 59,000*10*9 and the organ function test in search of ATT-related toxicities were also all in the normal range. The patient was again appointed after 2 months, and on return, the Platelet count was raised to 118,000*109 which is still below the normal value. Prednisolone was tapered over 6 weeks and stopped. After the total six months of therapy with ATT, platelet counts (204* 109) were became in the normal range after being successfully increased amid follow-up, and ATT was stopped as per the national guideline (Figure 2).
 |
Figure 2 Shows the trends of platelet count of an 11-year-old boy patient who presented with a one-day history of bilateral nasal bleeding. |
Discussion
The diagnosis of tuberculosis was initially dismissed since severe thrombocytopenia aggravating TB is unusual, making early detection difficult, and tuberculosis accompanied by secondary ITP is regarded extremely rare.8,14,23 Many secondary ITP cases caused by tuberculosis are treated with anti-tuberculosis drugs and corticosteroids, resulting in a platelet increase that lasts anywhere from a few days to three months. Within two weeks of starting prednisolone and one week of starting ATT, our patient’s platelets improved.5,8,24
In this case, there are numerous reasons to consider that thrombocytopenia is a result of tuberculosis, including positive gene expert with reasonable sensitivity and specificity, as well as typical tuberculosis chest x-ray findings and a supporting value of the erythrocyte sedimentation rate (ESR) of 70 mm/hr. The patient’s response to ATT, above all, confirms the tuberculosis diagnosis. The peripheral morphology, on the other hand, did not indicate chronic disease.9,22,25
Following test findings, this patient was started on prednisone right away and was transfused with platelets considering severe ITP,2,6,11,26 despite the fact that his platelet count did not improve. Steroids have been observed to treat patients with purpuric bleeding before their platelet count rises. This effect is caused by a decrease in vascular permeability.20,21
The prednisolone was discontinued after a 6-week taper, and the patient was regularly examined at an infectious clinic; no recurrence bleeding was discovered after the corticosteroid medication was discontinued. Finally, platelet levels recovered to normal after completing ATT, indicating that tuberculosis was the cause of thrombocytopenia in our instance.8,20,27
Because platelet transfusion was ineffective and there was no reduction in megakaryocytes and his bone marrow showed normal hematopoietic potential as seen by normal reticulocyte count, normal WBC, and normal hemoglobin, concomitant isolated ITP could be a possibility. In our opinion, TB bone marrow involvement did not play a substantial role in clinical thrombocytopenia. We also ruled out disseminated intravascular coagulation (DIC) due to normal prothrombin time and activated partial thromboplastin time.16,28
Furthermore, the lack of pancytopenia rules out bone marrow infiltration as a cause of thrombocytopenia, despite considerable evidence of tuberculosis as a cause of thrombocytopenia. The immunological roots of thrombocytopenia are revealed by the reaction to steroids. In the other cases that have been recorded thus far, steroids, intravenous immunoglobulin, and ATT have all been employed.16,29
There is no accepted standard of care for ITP caused by TB. Many cases described so far show that antituberculosis medication and corticosteroids are successful. ITP caused by tuberculosis usually has a fair prognosis. According to the literature, early detection and treatment of tuberculosis should be given high priority in order to reduce the use of immunosuppressive drugs, blood transfusions, and the danger of bleeding.5,10,16,20,30
According to the cases reported thus far, most patients respond to anti-tuberculosis treatment, corticosteroid, and IVIG,20,21 which is consistent with our case, despite the fact that IVIG was not used in our case because it was not available, and our patient responded to anti-tuberculosis treatment and corticosteroid, specifically Prednisolone. The time it takes for platelets to recover after starting treatment varies from a few days to a few months. In our case, no serious fetal bleeding occurred during the clinical course, and other sources support this.10,20,30–35
Generally, TB should be carefully considered in the ITP, and corticosteroids should be considered for inclusion in the ATT.
Conclusion
Tuberculosis (TB) should be recognized as a cause of immunological thrombocytopenia in tuberculosis-endemic areas. Our patient’s platelet count improved after 1 week of ATT and 2 weeks of prednisolone, and it was entirely restored after 6 months of ATT treatment. Unfortunately, there are no clear guidelines for treating TB-related immune thrombocytopenia or determining the cause of TB-related immune thrombocytopenia. Tuberculosis-induced ITP resolves with the ATT, even though more investigation is warranted.
Data Sharing Statement
The data used to support the findings of this study will be available from the corresponding author upon request.
Acknowledgment
We thank all individuals who were involved in the management of this case.
Author Contributions
All authors made a significant contribution to the work reported, whether in the conception, study design, execution, data acquisition, analysis, and interpretation, or all of these areas; took part in drafting, revising, or critically reviewing the article; gave official approval to the version to be published; agreed on the journal to which the article has been submitted; and agreed to be accountable for all aspects of this work.
Disclosure
The authors declare no conflicts of interest for this work.
References
1. Liebman HA, Pullarkat V. Diagnosis and management of immune thrombocytopenia in the era of thrombopoietin mimetics. Hematology Am Soc Hematol Educ Program. 2011;2011:384–390. doi:10.1182/asheducation-2011.1.384
2. Zeller B, Rajantie J, Hedlund-Treutiger I, et al. Childhood idiopathic thrombocytopenic purpura in the Nordic countries: epidemiology and predictors of chronic disease. Acta Paediatr. 2005;94(2):178. doi:10.1080/08035250410025294
3. Ozsoylu Ş. Idiopathic thrombocytopenic purpura. Acta Haematol. 1994;92(1):55. doi:10.1159/000204143
4. Kühne T, Berchtold W, Michaels,LA, et al. Newly diagnosed immune thrombocytopenia in children and adults: a comparative prospective observational registry of the Intercontinental Cooperative Immune Thrombocytopenia Study Group. Haematologica. 2011;96(12):1831. doi:10.3324/haematol.2011.050799
5. Ghobrial MW, Albornoz MA. Immune thrombocytopenia: a rare presenting manifestation of tuberculosis. Am J Hematol. 2001;67(2):139–143. doi:10.1002/ajh.1093
6. Rosthøj SH, Hedlund-Treutiger I, Rajantie J, et al. Duration and morbidity of newly diagnosed idiopathic thrombocytopenic purpura in children;A prospective Nordic study of an unselected cohort. J Pediatr Hematol Oncol. 2003;143:302.
7. Rodeghiero F, Stasi R, Gernsheimer T, et al. Standardization of terminology, definitions and outcome criteria in immune thrombocytopenic purpura of adults and children: report from an international working group. Blood. 2009;113(11):2386. doi:10.1182/blood-2008-07-162503
8. Khan AA, Shahzad A, Javid H, et al. Immune thrombocytopenia associated with tuberculosis – a case report. IDCases. 2021;23:e01012. doi:10.1016/j.idcr.2020.e01012
9. Kliegman RM, St Geme J. Nelson Text Book of Pediatrics. Elsevier; 2020:715–722.
10. Akyildiz B, Uzel N, Yanni D, et al. Immune thrombocytopenic purpura associated with pulmonary tuberculosis. Turk J Pediatr. 2009;51:271–274.
11. Neunert C, Noroozi N, Norman G, et al. Severe bleeding events in adults and children with primary immune thrombocytopenia: a systematic review. J Thromb Haemost. 2015;13:457. doi:10.1111/jth.12813
12. Kühne T, Buchanan GR, Zimmerman S, et al. A prospective comparative study of 2540 infants and children with newly diagnosed idiopathic thrombocytopenic purpura (ITP) from the Intercontinental Childhood ITP Study Group. J Pediatr Hematol Oncol. 2003;143:605.
13. Mert A, Bilir M, Tabak F, et al. Miliary tuberculosis: clinical manifestations, diagnosis and outcome in 38 adults. Respirology. 2001;6(3):217–224. doi:10.1046/j.1440-1843.2001.00328.x
14. Al-Majed SAA, Al-Momen AK, Al-Kassimi A, Al-Zeer AM, Kambal AM, Baaqil H. Tuberculosis presenting as immune thrombocytopenic purpura. Acta Haematol. 1995;94(3):135–138. doi:10.1159/000203995
15. Kashyap R, Mohan A. Haematological Manifestations of Tuberculosis. Hindawi; 2006:370–379.
16. Wada H, Sakashita T. A case of immune thrombocytopenia due to miliary tuberculosis effectively treated with eltrombopag. Resp Med Case Rep. 2020;31:1–5.
17. Das S, Jana P, Bhattacharya SK, et al. Immune thrombocytopenic purpura associated with pulmonary tuberculosis. J Glob Infect Dis. 2012;4(3):175–177. doi:10.4103/0974-777X.100580
18. Comstock D, Khorolsky C, Galbraith,R. Severe rifamycin-induced immune thrombocytopenia in a patient with extra-pulmonary tuberculosis. Int J Tuberc Lung Dis. 2018;22(10):1243–1244. doi:10.5588/ijtld.18.0197
19. Boots RJ, Roberts AW, McEvoy D. Immune thrombocytopenia complicating pulmonary tuberculosis: case report and investigation of mechanisms. Thorax. 1992;47(5):396–397. doi:10.1136/thx.47.5.396
20. Godeau B, Chevret S, Varet B, et al. Intravenous immunoglobulin or high-dose methylprednisolone, with or without oral prednisone, for adults with untreated severe autoimmune thrombocytopenic purpura: a randomised, multicentre trial. Lancet. 2002;359(9300):23–29. doi:10.1016/S0140-6736(02)07275-6
21. Mithoowani S, Gregory-Miller K, Goy J, et al. High-dose dexamethasone compared with prednisone for previously untreated primary immune thrombocytopenia: a systematic review and meta-analysis. Lancet Haematol. 2016;3(10):e489–e496. doi:10.1016/S2352-3026(16)30109-0
22. Federal Democratic Republic of Ethiopia. Guidelines for management of TB,DR-TB and leprosy in Ethiopia sixth edition; 2018.
23. Srividya G, Nikhila GP, Kaushik AV, Jayachandran K. Immune thrombocytopenia in tuberculosis: causal or coincidental? J Glob Infect Dis. 2014;6(3):128. doi:10.4103/0974-777X.138512
24. Madkaikar M, Jijina F, Gupta M, Rajpurkar M, Mohanty D:. Tuberculosis and immune thrombocytopenia. Haematologica. 2002;87:8.
25. Kasper DL, Fauci AS, Hauser SL, Longo DL, Jameson JL, Loscalzo J. Harrison’s Principles of Internal Medicine.
26. Neunert C, Terrell DR, Arnold DM. American Society of Hematology 2019 guidelines for immune thrombocytopenia. Blood Adv. 2019;3(23):3829–3866. doi:10.1182/bloodadvances.2019000966
27. George JN, Rizvi MA. Thrombocytopenia. In: Williams Hematology. ClinMed; 2001:1495–1540.
28. Ali R, Özkalemkas F, Özöelik T, et al. Idiopathic thrombocytopenic purpura in pregnancy: a single institutional experience with maternal and neonatal outcomes. Ann Hematol. 2003;82(6):348–352. doi:10.1007/s00277-003-0665-6
29. Sunara AP, Shelgikar KM, Melinkeri S, et al. Immune thrombocytopenia (ITP): a rare association of lymph node tuberculosis. J Assoc Physicians India. 2014;62:74–76.
30. Stork CM. Toxicology of Antituberculosis Drugs. Springer; 1996:829–841.
31. Weber SF, Bélard S, Rai S, Reddy R, Belurkar S, Saravu K. Immune thrombocytopenia secondary to tuberculosis: a case and review of literature. Int J Tubercul Lung Dis. 2017;21(4):466–470. doi:10.5588/ijtld.16.0515
32. Yee DVC, Valiquette C, Pelletier M, Parisien I, Rocher I, Menzies D. Incidence of serious side effects from first-line antituberculosis drugs among patients treated for active tuberculosis.. Am J Respir Crit Care Med. 2003;167(11):1472–1477. doi:10.1164/rccm.200206-626OC
33. Krishna MR, Gottam US, Mahendra N. Disseminated tuberculosis with severe immune thrombocytopenia. Respir Med Case Rep. 2019;25:27.
34. Nasa P, Juneja D, Sehra S, Singh HK, Prasad D. Immune thrombocytopenic purpura in a patient with disseminated tuberculosis: an unusual presentation. Int J Mycobacteriol. 2019;8(1):107–109. doi:10.4103/ijmy.ijmy_169_18
35. Panda S, Meher LK, Dalai SPet al. A case of immune thrombocytopenic purpura secondary to pulmonary tuberculosis. J Clin Diagn Res. 2019;10:OD12.
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.