")
Back to Journals » Advances in Medical Education and Practice » Volume 13
Is Emergency Remote (Online) Teaching in the First Two Years of Medical School During the COVID-19 Pandemic Serving the Purpose?
Authors Arja SB, Fatteh S, Nandennagari S, Pemma SSK, Ponnusamy K, Arja SB
Received 5 December 2021
Accepted for publication 19 February 2022
Published 1 March 2022 Volume 2022:13 Pages 199—211
DOI https://doi.org/10.2147/AMEP.S352599
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Prof. Dr. Balakrishnan Nair
Sateesh B Arja, Samir Fatteh, Sailaja Nandennagari, Sai Sarath Kumar Pemma, Kumar Ponnusamy, Sireesha B Arja
Avalon University School of Medicine, Willemstad, Curacao
Correspondence: Sateesh B Arja, Tel +599 96965682, Email [email protected]
Purpose: COVID-19 pandemic and closure of campuses have required a significant and rapid shift in teaching and training methods across health professions education, including remote teaching replacing face-to-face teaching. This study aims to investigate if emergency remote teaching implemented in the first two years of the medical school at Avalon University School of Medicine served the purpose during the COVID-19 pandemic. The effectiveness of emergency remote teaching and on-campus teaching were compared using course evaluations (students’ feedback) and students’ performance in assessments.
Methods: This is a concurrent mixed research method. The quantitative data collected are course evaluations and students’ performance in assessments between the two semesters September 2019 (on-campus teaching) and May 2020 (emergency remote teaching). There are three semesters in the first year and two semesters in the second year of the medical program. Each semester has around 10– 20 students at any given time. Quantitative data were analyzed for p-values and statistical significance using a t-test. The qualitative data were analyzed using thematic analysis.
Results: Results have shown no statistically significant difference (p< 0.05) between two semesters (between on-campus teaching and emergency remote teaching) for course evaluations. Even if there is any difference, the mean values were better in May 2020 semester with emergency remote teaching. There was no statistically significant difference (p< 0.05) even on students’ performance in assessments between two semesters (between on-campus teaching and emergency remote teaching) except for two courses. The thematic analysis of interviews revealed the advantages and disadvantages of online teaching.
Conclusion: Emergency remote teaching served the purpose in the first two years of medical school during the COVID-19 pandemic. The advantages of online teaching are flexibility and comfort, and students can save time. The disadvantages are technical challenges, students lacking motivation, lack of personal interaction, and limitations on lab and hands-on experiences.
Keywords: COVID-19, medical education, basic science, teaching and learning, evaluation
Introduction
COVID-19 pandemic necessitated a significant and rapid shift in teaching and learning strategies across health professions education and educational programs worldwide. Significantly, the need for physical distancing severely constrained traditional face-to-face lectures and teaching strategies and encouraged a shift to be online and virtual teaching strategies.1–4 COVID-19 pandemic situation posed many challenges to healthcare worldwide and medical education. Rose observed that “The need to prepare future physicians has never been as focused as it is now in a global emergency”.5 The COVID-19 pandemic caused worldwide disruptions to the healthcare systems and medical education.5,6 Institutions of higher learning stopped operations physically, and most of the activities are online. Further, the response of medical schools to the COVID-19 pandemic was unprecedented.
Avalon University School of Medicine (AUSOM) is established in Curacao, the Caribbean region offering a Doctor of Medicine (M.D.) program. The M.D. program is of 4-year duration, with the first two years including basic science instruction and the next two years of clinical rotations/clerkships. The first two years of the program consist of basic science courses, including clinical skills. Basic science courses are spread over five semesters, which are from MD1 to MD5 semesters. Basic science courses are multi-disciplinary courses like Human Structure and Function (HSF) 1 and 2 (anatomy, histology, and physiology), Molecular Basis of Medicine (MBM) 1 and 2 (biochemistry and genetics), Mind, Brain, and Behavior (MBB) 1 and 2 (neuroscience and genetics), Diseases, Immunity, and Therapeutics (DIT) 1 and 2 (pharmacology, pathology and microbiology and immunology), epidemiology and biostatistics and clinical skills 1–4.
Face-to-face teaching is where the instructor and the learners meet in an established place for a scheduled time, for either one-on-one learning or, most commonly, in group classroom sessions. The advantages of face-to-face teaching are learners can concentrate better on learning because there’ll be fewer distractions, and learners can gain greater understanding, experiences, and real-world examples from teachers and other students. Learners have a greater chance of completing their course successfully in a classroom environment. (Completion rate of teacher-led classes is almost 5x higher than that of online learning). Learners may feel more comfortable and learn more efficiently in a familiar and traditional classroom environment. Learners can access more information. Learners have the opportunity to connect with, problem-solve, and socially interact with other diversified students from different backgrounds.
The Medical Education Unit (MEU) and dean’s office, in collaboration with the Information Technology (IT) department at AUSOM, provided training and resources for biomedical faculty to develop skills and expertise for delivering courses in virtual teaching methods. These actions were taken for the rapid transition to teaching and learning in virtual environments during the COVID-19 pandemic. In this context, drawing on faculty development program experiences and support during the COVID-19, which caused rapid teaching transition, we handled innovative teaching strategies in virtual environments. We designed and trained the faculty who are relatively new to virtual teaching and had no prior hands-on experience. Faculty with previous experience potentially benefit from new and different perspectives on the application and impact of education through technology presented below.
Online Teaching Platforms
Both content experts and the students needed to adapt to the new normal of using available tools on the internet to continue education.7 Popular platforms or software that are frequently used are WebEx®, Microsoft Teams®, Zoom®, and Google Meet® as these were provided free of charge. For example, Zoom® has forgone its time limit to use the Zoom® application widely. But these also have their limitations given vast usage around the globe as the whole world was being locked down.8 We have been using Google Meet® at AUSOM. All assessments were conducted using Examsoft software. Assessments were proctored using the Google Meet application (video-based proctoring).
Methods of Online Teaching
Methods of remote teaching and learning in medicine were primarily divided into two, which are synchronous and asynchronous teaching. Synchronous instruction is where the lecturer teaches and communicates with the students in real-time online using various video conference applications. Asynchronous teaching is where the lecturers record their lectures or hands-on clinical examinations or set up tasks and assignments for students to complete at a specified time. It is not on a real-time basis. These two methods also have limitations, mainly due to internet availability, connectivity, and time difference.9,10 At AUSOM, the main teaching method during this pandemic was synchronous teaching supplemented with recorded video libraries like “Lecturio.” AUSOM has adjusted the course learning objectives as per the requirement of Emergency Remote Teaching (ERT). AUSOM has given greater attention to students’ engagement during remote teaching. We focused on stimulating students’ interest, concepts around big ideas, required competencies and skills overarching the institutional learning objectives, and integrated multidisciplinary course modules. Different learning strategies, including small-group discussions, problem-based learning, and case-based discussions were employed.
For pre-clinical teaching, which is integrated with the United States Medical Licensing Examinations (USMLE) preparatory curriculum, usually requires clinical exposure and clinical skills right from the beginning. Online teaching posed a moderate challenge to this. Many universities evolved into eliminating lectures and using technology to replace face-to-face interaction, the so-called “active learning” strategy even before the pandemic. They moved towards promoting individualized teaching and enhancing interprofessional education11,12 through active learning strategies. The significant bulk of pre-clinical subjects can be conducted by various platforms, mostly through online, distance, or electronic learning without the face-to-face method. Subjects like physiology, neuroscience, biochemistry, and medical genetics and pharmacology can be taught online. According to Miller’s pyramid,13 most of the skills needed for these subjects are up to understanding the concepts. Hence, the need for face-to-face interaction is not as essential and manageable without face-to-face interactions and hands-on experiences. But it is not the same case for courses like anatomy, clinical skills, microbiology, histology, and pathology, which require labs and hands-on experiences. We aimed to identify advantages and difficulties with this new approach as a necessary replacement for traditional face-to-face lectures. The changes implemented at AUSOM in the first two years of the medical school’s education during the pandemic can be summarized as follows.
- Basic science instruction- Online didactic live lectures, small group activities, and virtual labs
- Basic science assessments- being conducted with video-based remote proctoring
- National board of medical examiners (NBME) comprehensive basic science exams- continuing with video-based proctoring by Zoom
Online teaching has existed for quite some time in a few medical schools, especially during the preclinical period, and there is literature on online teaching and effectiveness. This study aims to study the effectiveness of emergency remote teaching (ERT), which was implemented during the pandemic at AUSOM. This study examines whether online instruction implemented during unprecedented times (ERT) was equally effective as on-campus teaching. This manuscript also explores the stimulators, obstacles, advantages, and disadvantages of remote teaching, which was implemented not as a normal change process but as an emergency change. The effectiveness of ERT and on-campus teaching were compared using course evaluations (student feedback) and students’ performance on assessments. The outcomes that were compared between on-campus instruction and online teaching were course evaluations and students’ performance on assessments (final grades). This is one of the studies comparing on-campus teaching and emergency online (remote) teaching outcomes.
Null Hypothesis- Emergency online (remote) teaching is not effective as on-campus teaching at AUSOM.
Alternate Hypothesis: Emergency online (remote) teaching is equally effective as on-campus teaching at AUSOM.
Methods
This is a mixed concurrent quantitative and qualitative research study. In September-December 2019 semester, the basic science instruction was completely on-campus. In January- April 2020 semester, the basic science instruction was on-campus till March 2020, but it became virtual from March 17th due to lockdown implemented on the island. We did not use the outcomes of the January-April semester to compare with September-December 2019 semester as the January-April semester had both on-campus and online teaching. The outcomes of the May-August 2020 semester which was completely online were compared with outcomes of the September-December 2019 semester. Same faculty members were involved in teaching the same courses between September-December 2019 semester and May-August 2020 semester. The admission criteria and the attributes like grade point average (GPA) remain the same for students of the September-December 2019 and May-August 2020 semesters. There were no changes in the admissions criteria for the selection process of students. The curriculum, including learning objectives, teaching methods, and assessments, were aligned to achieve Bigg’s constructive alignment.
We evaluated the knowledge, skills, and attitudes of students throughout the semester. The students’ “knows” and “knows how” levels (13) were assessed using multiple-choice questions (MCQs). MCQs were employed to assess knowledge, application, and analysis of students. The students’ “shows” level (13) was assessed using standardized patient-based assessments, which were also done virtually. We assessed students’ attitudes and professional behaviors during all sessions, including group activities like small-group discussions, PBL, and case-based discussions. The assessments based on MCQs were standardized using the compromised Hofstee method before the pandemic and during the emergency remote teaching. Clinical skills were assessed using virtual SP-based assessments using Google Meet software. Virtual SP-based assessments by Google Meet replaced the original SP-based assessments. Because we cannot conduct the face-to-face exam format, the students were conducting a telemedicine interview with the standardized patient. Then students type out the encounter after each telemedicine interview. Students will have to verbalize to the Standardized Patients (SPs) the maneuvers they would do if they were in a face-to-face encounter for the virtual exam. The SPs will listen, and after students have finished describing the maneuver, they will report to the student if the findings are normal or any other findings. The borderline group method was used to standardize for performance-based assessments like SP-based assessments before the pandemic and during the emergency remote teaching.
The Research and Ethics committee of AUSOM approved this study.
Quantitative data: Comprised of two components
- Course evaluations- comparison of course evaluations between September-December 2019 (complete on-campus and face-to-face) and May-August 2020 semesters (complete online instruction)
- Comparison of students’ performance (Mean class average) in basic science courses between September-December 2019 and May-August 2020 semesters
Quantitative data were collected from the central IT department of AUSOM, where all course evaluations at the end of the semester was compiled using Survey Monkey. Dean’s office and MEU gathered this data every semester for analysis by the dean, quality assurance committee, and curriculum committee. The questionnaire (course evaluations) included a total of sixteen questions (Appendix 1). The responses to the questionnaire were gathered on the Likert scale of one to five. One is strongly disagreeing, two is disagreeing, three is neutral/no opinion, four is agreeing, and five is strongly agreeing. The values of mean and standard deviation were analyzed. SPPSS software was used to calculate p-values by using a t-test to determine any statistically significant difference. The p-values were adjusted to the nearest second decimal values. The students’ performance (grades) on assessments was collected from the Students Information System (SIS). The assessments included multiple-choice questions, oral examinations, objective structured practical examinations, and standardized patient-based assessments. The examinations were similar between September-December 2019 and May-August 2020 semesters. The class averages were calculated using SPSS software and calculated the p-value using a t-test to examine any statistically significant difference. During the collection of data, no personal data was identified.
The research methodology was mixed methodology. After the initial analysis of quantitative data, identified that ERT (online teaching) was equally effective as on-campus teaching. Then we wanted to take the experiential account of students and faculty members of their perceptions and experiences regarding emergency remote teaching using the phenomenology approach. We conducted individual interviews (qualitative data) with students and faculty members to gather their experiences and perceptions regarding emergency remote teaching. The sampling strategy was simple random sampling for students and purposive sampling for faculty as these faculty had experience with remote teaching during the pandemic. We did conduct a total of 19 interviews during September-October 2020. We randomly selected two students from each semester from MD1 to MD5 semesters, and a total of ten students were invited to participate in the interview. We invited all 12 faculty members teaching basic science courses to participate in the interview. All participants were required to sign the consent form. The interview schedule consists of five questions (Appendix 2). All interviews took time around 10–15 minutes. Interviews were audio-recorded. Interviews were conducted either by telephone or personally. Two students who were involved in this research study as authors conducted all interviews to avoid bias due to power relationships. Students were trained on how to run the interviews by the principal investigator. The faculty authors did the data analysis.
All interviews were recorded and transcribed using Happy Scribe software. After verification of its content, we read the transcript carefully, line by line, for familiarization. The transcribed texts were shared with all interview participants for word member checking and validation. We used thematic analysis. The thematic analysis included familiarization, identifying a thematic framework, indexing, charting, and mapping and interpretation. Thematic analysis was done manually. Certain ideas cropped up in the transcript readily, and we gave these a preliminary code. The coding was done by two authors (SBA1 and SBA2). Both SBA1 and SBA2 are physicians by training, and SBA1 completed his master’s in health professions education. Once we generated codes, we shared them with all authors. If there was a disagreement on any of the codes, it was resolved after discussing with other authors. Then we began to identify themes or emergent concepts and engaged in re-coding to develop more well-defined categories.
Results
The response rate for course evaluations was as follows. The response rate for Mind, Brain, and Behavior 2 in September 2019 was eight out of 11 (73%), and in May 2020 semester was 11 out of 13 (85%). The response rate for Diseases, Immunity, and Therapeutics 1 in September 2019 semester was nine out of 11 (82%), and in May 2020 semester was 10 out of 14 (71%). The response rate for Human Structure and Function 1 in September 2019 semester was 12 out of 12 (100%), and in May 2020 semester was 19 out of 19 (100%). The response rate for Human Structure and Function 2 in September 2019 semester was eight out of 10 (80%), and in May 2020 semester was 10 out of 13 (77%). For Clinical Skills I (CS 1), in September 2019 semester, the response rate was eight out of 10 (80%), and in May 2020 semester was 17 out of 19 (89.4%). The response rate for Clinical Skills 2 (CS-2) in September 2019 semester was nine out of nine (100%), and in May 2020 semester, 16 out of 16 (100%). Students’ responses for most of the questions, mean values have no statistically significant difference (p<0.05) between on-campus teaching and online teaching (Tables 1–Table 4). The t-test was used to assess the statistical significance as the responses on course evaluations were normally distributed with homogeneous variance. Even if there is a difference, the mean values or students’ responses were better with emergency online (remote) teaching (Tables 1–4). Students’ performance in assessments in each course was compared between September 2019 and May 2020 semesters. Students’ grades were normally distributed with homogeneous variance, and the t-test was used to assess the statistical significance. There was no statistically significant difference (p<0.05) between the two semesters (Table 5) except for two courses, Mind, Brain, and Behavior 2 and clinical skills 2.
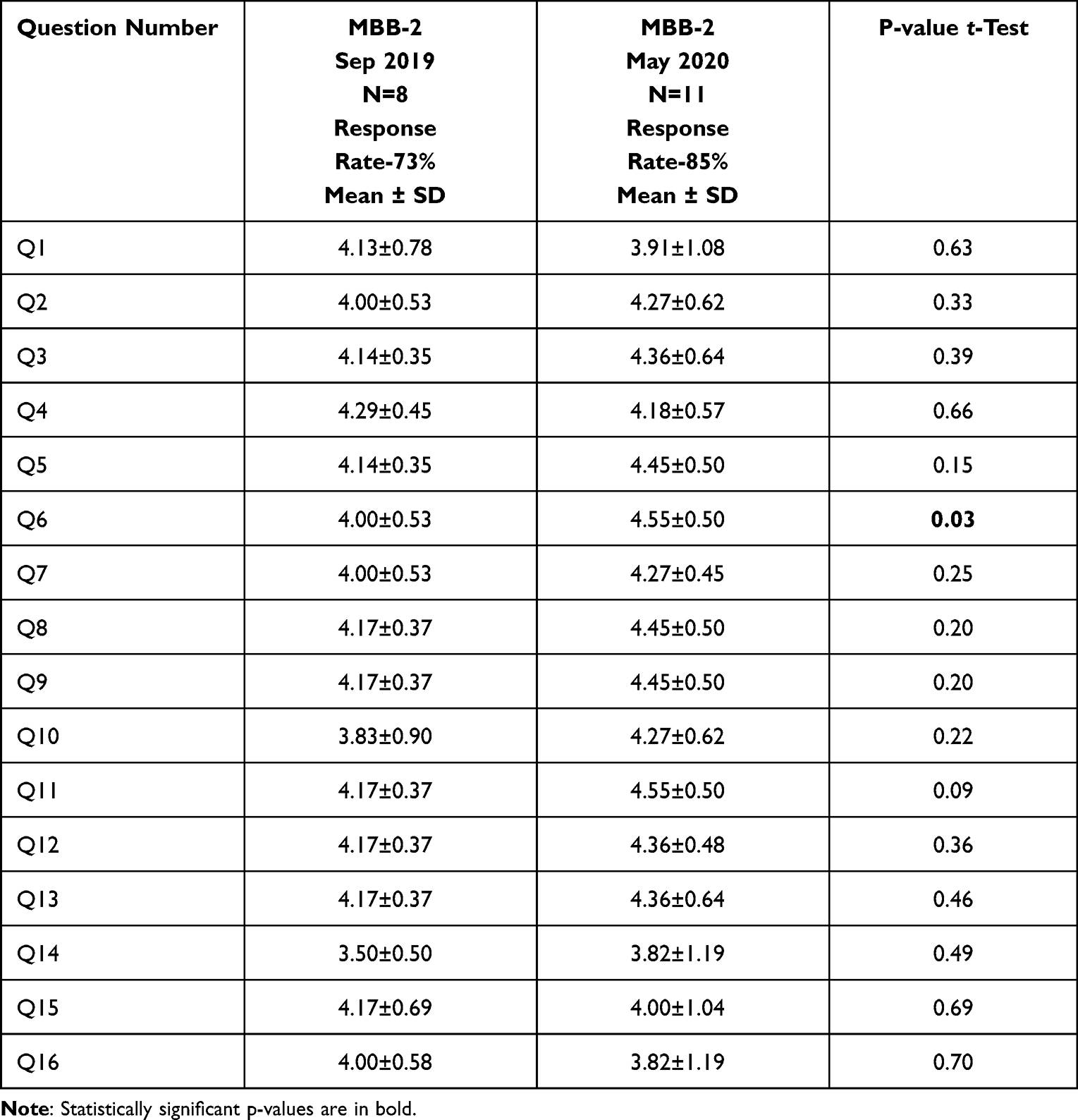 |
Table 1 Comparison of Course Evaluations for the Courses Mind, Brain, and Behavior (MBB) 2 |
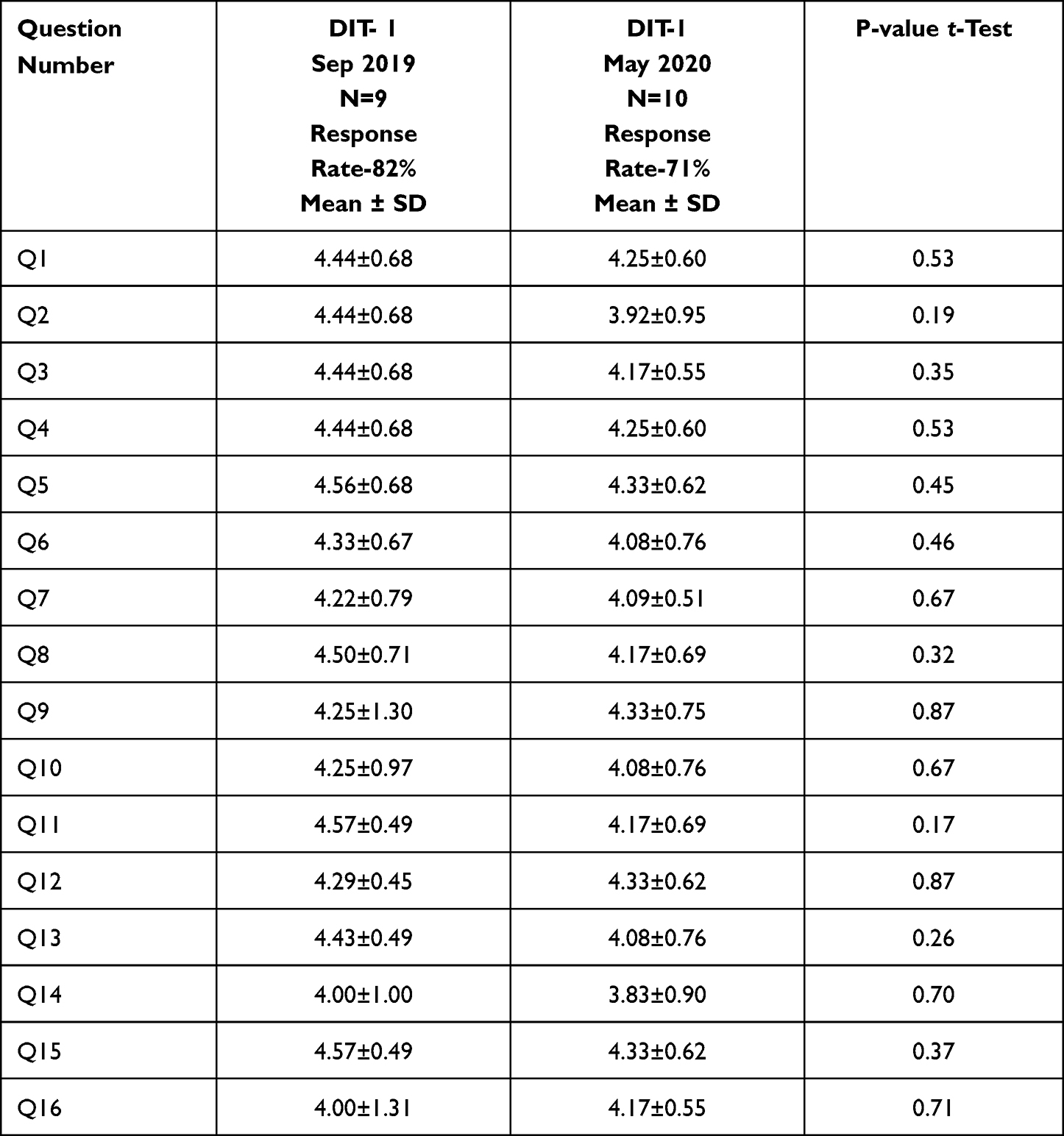 |
Table 2 Comparison of Course Evaluations for the Courses Diseases, Immunity and Therapeutics (DIT) I |
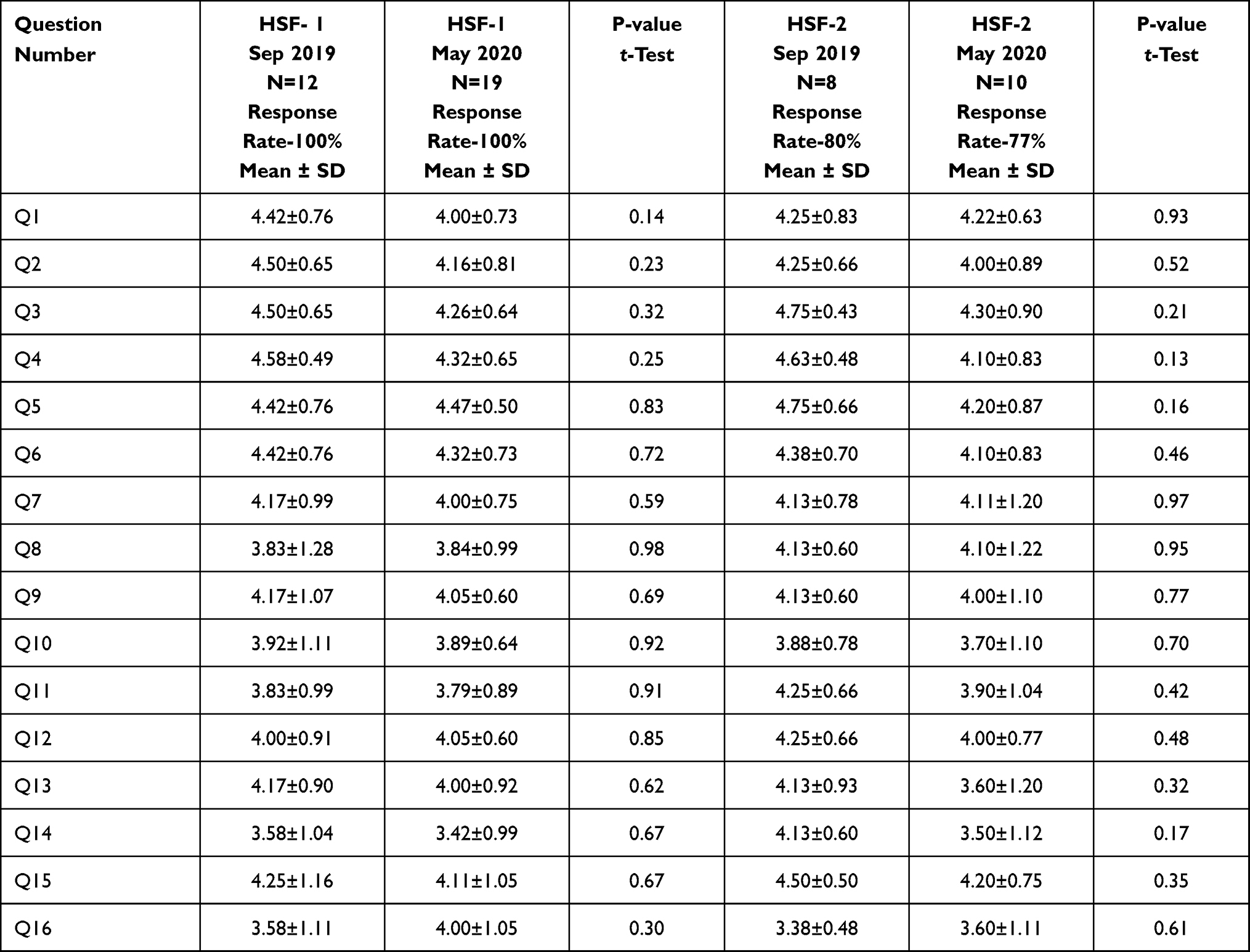 |
Table 3 Comparison of Course Evaluations for the Courses Human Structure and Function (HSF) 1 and 2 |
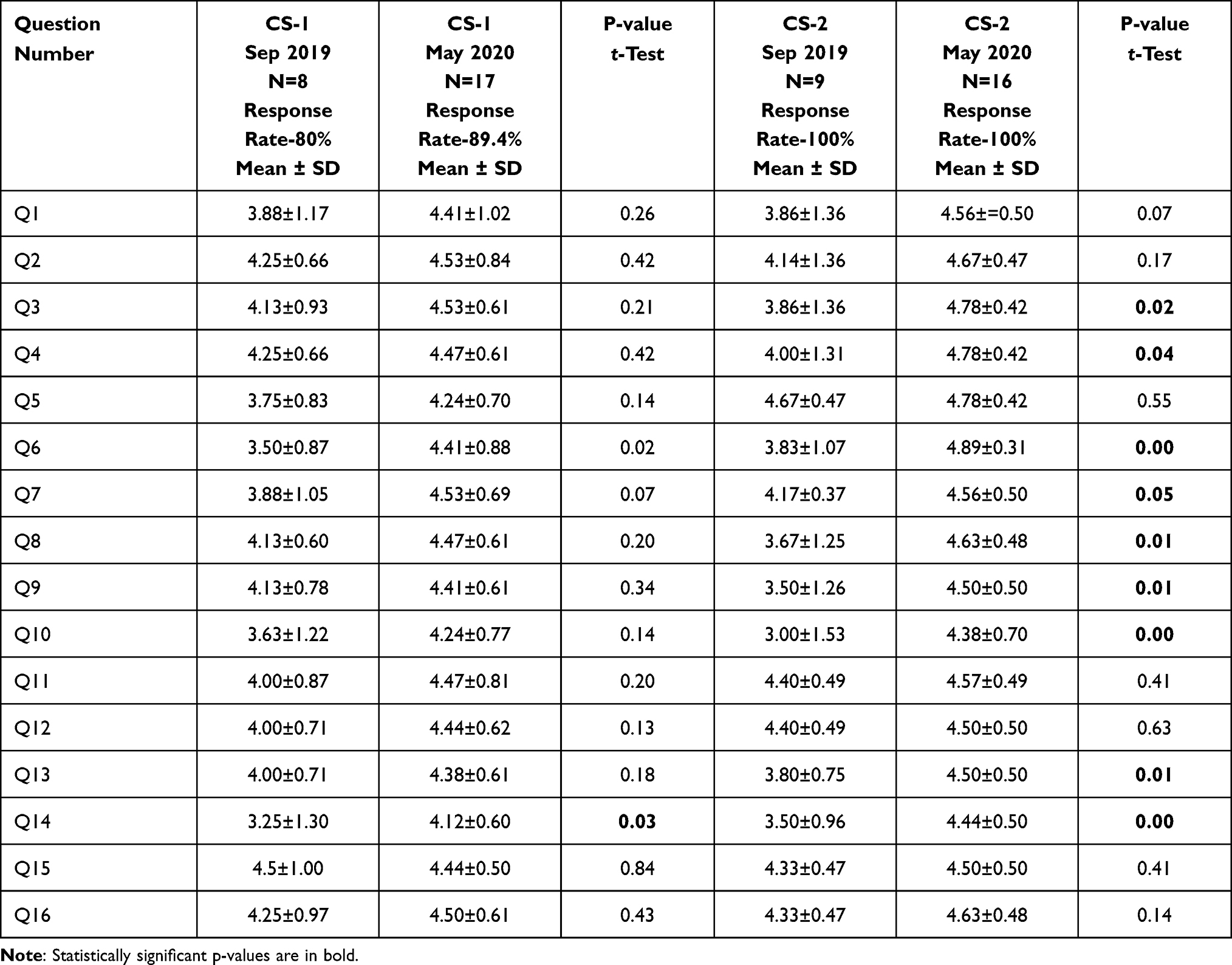 |
Table 4 Comparison of Course Evaluations for Clinical Skills 1 and 2 Courses |
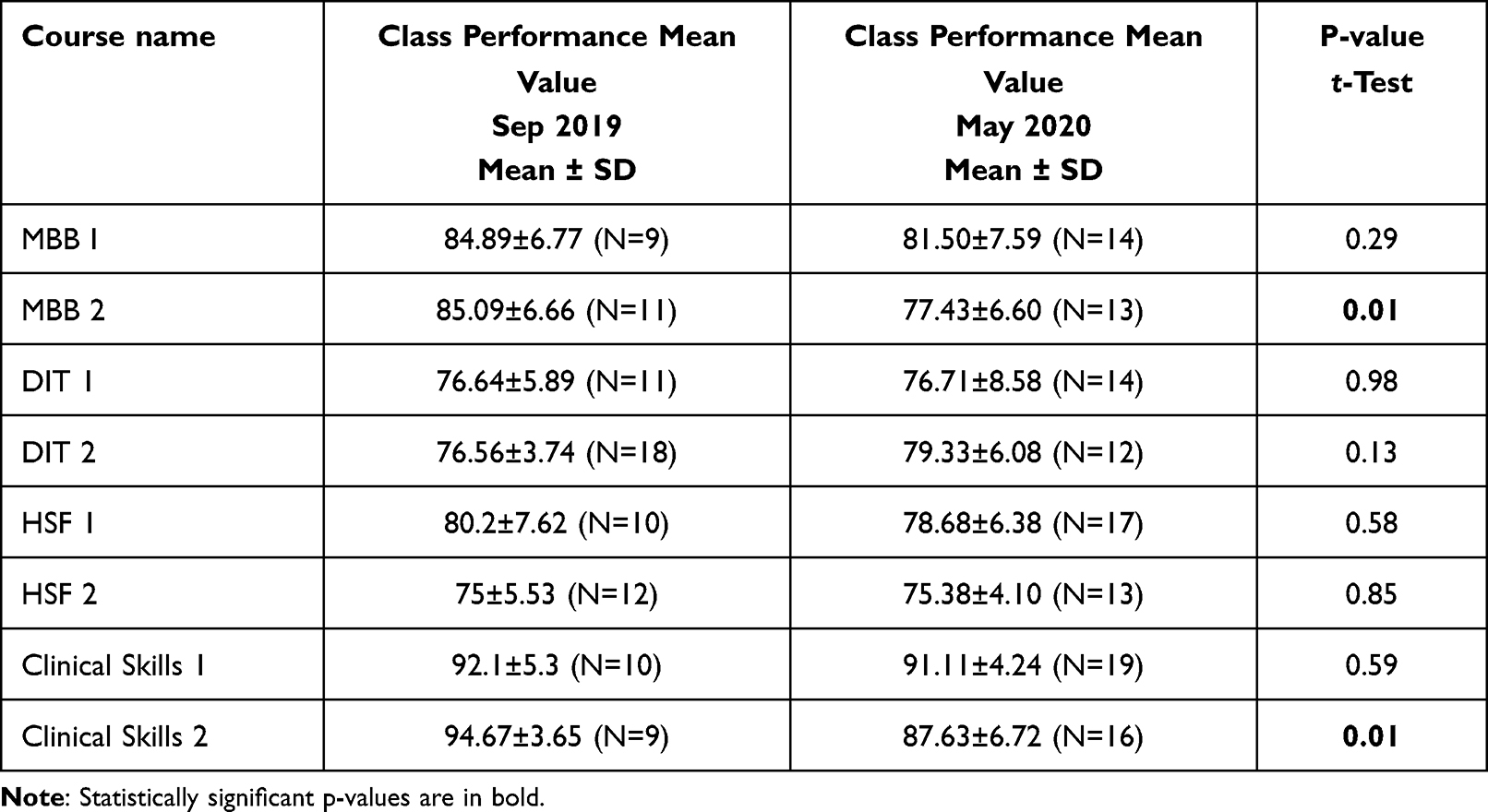 |
Table 5 Comparison of Students’ Performance in Different Courses Between Two Semesters |
We were able to interview all ten students out of ten students that were invited for the interviews (100% response rate). We were able to interview nine faculty members out of 12 faculty members that were invited for an interview (75% response rate). Thematic analysis of the qualitative data identified the following themes.
Earlier Experience with Online Teaching and Learning
Most faculty members said they did not have any previous experiences with online teaching. Four faculty members did distance learning programs for their education. All other faculty members felt that this online teaching and training were new. Few students did some online courses in the past but not in medical school. Before joining the medical school, the students who did online programs felt that it could help the students with part-time jobs. Most faculty members felt that they had never thought of online teaching in medical school before the pandemic.
Stimulators for Emergency Remote Teaching
Current Circumstances and Ongoing Pandemic
All faculty members and students felt that the major stimulator for remote teaching in the current circumstances is the ongoing pandemic of COVID-19. All of them felt that this pandemic forced us to do remote teaching. Online instruction for basic science courses is the only option to complete education, especially in this tough and unprecedented time. One of the faculty members quoted that,
we have all kinds of resources and technologies and this can be simulated on devices like laptops, mobiles, and then the students can learn and practice using those technologies that are available. (faculty interviewee 1)
Saving Time
The other major stimulator mentioned by students is saving time. One student quoted that, “I think it’s
Time, even before if I wake up at 6 am, I will spend most of the time in getting dressed up for school and getting ready and now even though I wake up at 6 am I will spend 15 min for fresh up, and I can use the rest of the time to pre-read (student interviewee 1)
Students also felt that online education could be helpful for students with financial issues and physical disabilities.
Obstacles for Emergency Remote Teaching
Technological Difficulties and Technical Challenges
The major barriers mentioned by faculty members and students are technological difficulties, power issues, and network problems, sometimes. Some of the faculty members might not understand or acknowledge the technical challenges that students are going through. The other obstacle is time differences (different time zones). This is especially an issue with synchronous remote instruction.
Online Fatigue and Lack of Personal Interactions
The other obstacle for synchronous remote instruction is that faculty members get fatigued with online education as they must spend more time explaining the same concept. It could have been done in less time in on-campus teaching. One student felt that some of the faculty members were not ready for remote classes. One student felt that class could be very monotonous in remote education when no personal interaction between the students and faculty members.
Advantages of Emergency Remote Teaching
Convenience and Flexibility
The major advantages of remote teaching are the availability of many resources and technologies and complementing the didactic lectures with these technologies. Remote teaching is very convenient and flexible. The other advantage cited by the faculty members and students is that remote teaching can have sessions recorded, and recorded videos can be played again. Students can always go back to the point where there was a conclusion that, as in in-person lectures, we cannot do that. The other advantage mentioned was that faculty and students could be anywhere in the world.
Saving Time and Other Benefits
One of the most important advantages students mentioned is saving time with remote teaching, as they are not required to go to the school’s campus. The other advantage is that introverts and shy students became very communicative and interact well during online classes.
Disadvantages of Emergency Remote Teaching
Limited Hands-on Experience and Personal Interactions
Most of the faculty members and students felt that the major obstacle to remote teaching is the lack of hands-on experiences and personal interaction. Even though we were conducting virtual labs, some faculty members and students felt that they were missing labs and hands-on experiences, especially for courses like anatomy and clinical skills. Remote teaching lacks classroom experience, which is the major disadvantage of missing personal connection. One faculty member quoted that “there is verbal communication and there is nonverbal communication.
As a teacher, you can look into the students” eyes and ask them questions, and they can also look into the teacher’s eye and answer or ask questions (faculty interviewee 3)
Professional training requires visual, auditory, tactile, and every part of your faculties to be ministering to the student. Sometimes students can switch off the camera and disappear from the class. Some faculty members quoted that it is very difficult to track students’ attendance during class hours.
Lack of Motivation
Another disadvantage associated with remote teaching is the lack of motivation for students. Procrastination is one of the problems in online learning and training. Students must be kept motivated, and communication between faculty and students is the key. One of the faculty members quoted that,
The main obstacle for online teaching is the students” self-motivation might be missing. In face-to-face interactions, they learn from group studies and with the faculty interaction and then the personal experiences they have and then hands-on experiences. They are missing like a lot of group interaction (faculty interviewee 7)
.Discussion
The COVID-19 pandemic is continuing and will remain to disrupt medical teaching and training. COVID-19 has caused unprecedented interruption to the medical education process and healthcare across the globe.14 The current COVID-19 pandemic presented various challenges like challenges to faculty in shifting from face-to-face to online teaching challenges to students in moving to remote learning, challenges in conducting the assessment, challenges in accessing the internet and using digital technology, and challenges to an institution in organizing online teaching and learning activities during the lockdown. It is said that challenges bring opportunities. COVID-19 may also bring opportunities. Medical educators have initiated the process of transforming education and improving quality before the COVID-19 outbreak. The COVID-19 pandemic has, however, changed the landscape of medical education. The situation has forced medical educationalists to think “out of the box” and act innovatively using advanced digital technology. The existing COVID-19 pandemic has motivated us to transform education methods, modalities, and processes, initially requiring greater effort. Still, it provides teachers, faculty, and facilitator impetus to keep pace with current technology trends, eg, digital gadgets, programs, and software, modified forms of media with innovative audiovisual aids. This is a new experience or opportunity to learn, understand, and update unique needs and new modes of delivery of medical education for all stakeholders involved. It may also have a long-lasting impact on healthcare.
The attitude and readiness of educators running or engaging in remote education are crucial. As key stakeholders, educators should be seen as educators and be supported and developed, including the faculty development in both delivery and design of online teaching.15 This could be evident in our efforts to emphasize the requirement of faculty development activities for our biomedical educators. We did a few faculty development activities just before the transformation to emergency remote (online) teaching. These faculty development activities were focused on how to use digital technologies for online teaching. This led to successful emergency online (remote) teaching for our basic science courses, which is evident in course evaluations.
The literature on remote learning in medical students before the COVID-19 pandemic has found that though students feel it complements their education, they do not see it as an acceptable replacement for in-person learning.16,17 By now, many medical schools due to COVID-19 have created online coursework so that students can continue education and training from home.18,19 In most medical institutions, alternative virtual coursework was adopted, such as e-learning modules, video vignettes, and virtual reality simulators.20 Although the significant amount of time in the medical curriculum in pre-clerkship is allotted for didactic lectures, anatomy labs (Grant’s Dissector Videos), clinical skills lab sessions (telemedicine/telehealth concepts), small group sessions, problem-based Learning (PBL) sessions, and other labs (virtual labs like virtual microscopy in histology and pathology) at AUSOM also implemented and incorporated in emergency remote (online) teaching and training. This allowed students’ active engagement and participation during online instruction, which was done during these emergent times. This could be evident from course evaluations. The last but one question on the survey (courses evaluations) is that if students contribute constructively to in-class activities, there is no statistically significant difference between on-campus teaching and remote teaching (Tables 1–4). We recommend adapting interactive remote learning lectures using highly sophisticated technologies and virtual clinical case-based discussions. Such measures would help students adjust to this way of medical teaching even during emergent times.
Emergency remote (online) teaching could be successful if learning objectives, teaching methods, and assessment methods are in alignment, which is referred to as constructive alignment.21 The other important key factor is students’ engagement in classroom activities. This was achieved by emphasizing the pedagogy of adult learning principles. Adult learning principles were implemented using various teaching-learning strategies, including small group discussions, self-directed learning, pre-reading assignments, and hands-on experiences, including labs employed during our emergency online (remote) teaching. This led to sufficient satisfaction of learners, which could be evident in course evaluations.
Students’ satisfaction with feedback was satisfactory because of providing effective and specific feedback provided on time,22 even during the emergency remote (online) teaching. The feedback was provided to all students using the Google Meet platform. All departments were instructed to give feedback at least twice a semester. In addition, students can request an appointment and meet with the faculty member to receive feedback and academic guidance using the Google Meet platform. Students’ responses for most of the questions, mean values have no statistically significant difference (p<0.05) between on-campus teaching and remote teaching (Tables 1–4). Even if there is a difference, the mean values or students’ responses were better with remote teaching (Tables 1–4). Students’ were satisfied, and they felt they were achieving course learning objectives, and they were actively engaged in classroom activities because of innumerable opportunities for them. This was achieved due to small group activities, including case-based discussions and PBL, virtual labs, and clinical skills teaching using standardized patients. Students practiced history taking and interviewing skills with standardized patients using Google Meet, verbalizing physical examination, and physical examination videos.
Students’ performance in assessments in each course was compared between September 2019 and May 2020 semesters. There was no statistically significant difference (p<0.05) between the two semesters (Table 5) except for two courses, Mind, Brain, and Behavior 2 and clinical skills 2. AUSOM has given greater importance to Bigg’s constructive alignment (21) during this emergency remote teaching. The course learning objectives, instructional methodologies, student involvement in classroom activities, and assessments are aligned. This could be evident in course evaluations (student feedback). Students were satisfied with course learning objectives, and students were aware of course learning objectives. Students were satisfied with teaching methods, and they felt that they were achieving course learning outcomes and involved in classroom activities. Students also felt that the assessments were in support of course learning objectives.
Even though the quantitative data have shown no statistically significant difference between on-campus teaching and remote teaching, we did interviews to investigate whether quantitative and qualitative data complement each other. The data analysis of interviews has shown both advantages and disadvantages to emergency remote (online) teaching. The advantages include the availability of different technologies, resources, and platforms for online teaching. The other advantage is remote teaching is flexible and convenient. The other most important advantage is saving time for students as they do not need to get prepared and travel to the campuses. Students and faculty are well adopted during difficult and unprecedented times. All students and faculty agreed that emergency remote (online) teaching is the only option to teach basic science courses during this pandemic as campuses are not open. This change in medical education is seen as an emergency change rather than as a standard change process.
But most of the faculty members and students also have expressed their dissatisfaction with emergency remote (online) teaching. The main disadvantage of remote teaching is the lack of classroom experience and personal interaction. The other disadvantage is limitations on labs and hands-on experiences even though virtual labs are conducted. This was of major concern for anatomy and clinical skills courses. The biggest challenge for students is not having study groups as they are not on campus and lacking motivation. This can be rectified if students contact their peers using social media and online platforms and adequate communication with their faculty members. The other difficulties with online teaching are technical challenges and network issues.
Limitations
This study was conducted at a single institution. Another limitation is the cross-sectional nature of the study design. This necessitates the requirement of conducting longitudinal studies in different institutions. Another limitation of our study is the small sample size that was used for quantitative data. But the sample size for qualitative data is adequate as we were able to do 19 interviews, and there was no further new information added after some interviews.
Conclusions
We found that medical students had different knowledge, attitudes, and practices regarding the emergency remote (online) learning process. Our quantitative data results have shown no statistically significant difference in either course evaluations or students’ performance on assessments with a very few exceptions. This shows that emergency remote (online) education served the purpose in the first two years of medical school during the COVID-19 pandemic in terms of effectiveness regarding students’ performance in assessments and students’ feedback on course evaluations. The thematic analysis of interviews revealed the advantages and disadvantages of emergency remote (online) teaching. The advantages of online instruction are flexibility and comfort, and students are able to save time. The disadvantages are technical challenges, network issues, students lacking motivation, lack of personal interaction, and limitations on lab and hands-on experiences. The results may not be generalized to other institutions. Further studies in different institutions must validate them to see the remote learning platform’s utility as a teaching and learning mode, especially for basic science courses. Such replication studies in multiple institutions could help determine whether remote education can replace traditional medical lectures in the first two years of medical school. Medical schools might look at didactic lectures online either during urgent times or as a regular change process, and small group discussions, seminars, and labs require on-campus instruction. Remote education in the first two years of medical school can succeed if students and faculty are appropriately engaged and actively involved in in-class activities. Provide structure to the classroom activities, give students time, and provide feedback to students to make online education successful.
Abbreviations
AUSOM, Avalon University School of Medicine; M.D, Doctor of Medicine; HSF, human structure and function; MBB, Mind, Brain, and Behavior; DIT, Diseases, Immunity, and Therapeutics; MEU, medical education unit; IT, Information Technology; USMLE, United States Medical Licensing Examinations; NBME, National Board of Medical Examiners; GPA, grade point average; MCQ, multiple choice questions; PBL, problem-based learning; SIS, student information system.
Data Sharing Statement
Raw data and materials are available.
Ethical Approval and Consent to Participate
This study is approved by the Research and Ethics committee of Avalon University School of Medicine. Informed written consent was taken from all participants (students and faculty members) and they had a right to decline participation in this study.
Consent to Publish
We haven’t used any identifiable personal information or 3rd party images or videos.
Acknowledgments
The authors would like to acknowledge all faculty members and students who participated in the interviews.
Funding
No external or internal funding received.
Disclosure
The authors declare that they have no conflicts of interest for this work.
References
1. Carlson ER, COVID-19 and educational engagement. J Oral Maxillofac Surg. 2020;78(7):1049–1051. doi:10.1016/j.joms.2020.04.033
2. Collins B, Day R, Hamilton J, Legris K, Mawdsley H, Walsh T. 12 tips for pivoting to teaching in a virtual environment. MedEdPublish. 2020;4:1–11.
3. DeFilippis EM, Stefanescu Schmidt AC, Reza N. Adapting the educational environment for cardiovascular fellows-in-training during the COVID-19 pandemic. J Am Coll Cardiol. 2020;75(20):2630–2634. doi:10.1016/j.jacc.2020.04.013
4. Prem K, Liu Y, Russell TW, et al. The effect of control strategies to reduce social mixing on outcomes of the COVID-19 epidemic in Wuhan, China: a modelling study. Lancet Public Health. 2020;5:e261–e270. doi:10.1016/S2468-2667(20)30073-6
5. Rose S. Medical Student Education in the Time of COVID-19. JAMA. 2020;323(21):2131–2132. doi:10.1001/jama.2020.5227
6. Mian A, Khan S. Medical education during pandemics: a UK perspective. BMC Med Educ. 2020;18(1):100. doi:10.1186/s12916-020-01577-y
7. Moszkowicz D, Duboc H, Dubertret C, Roux D, Bretagnol F. Daily medical education for confined students during COVID-19 pandemic: a simple video conference solution [published online ahead of print, 2020 Apr 6]. Clin Anat. 2020. doi:10.1002/ca.23601
8. Rashid AA, Mohd Radzniwan AR, Yaman MN, Mohamad I. Teaching medicine online during the COVID-19 pandemic: a Malaysian perspective. Bangladesh J Medical Sci. 2020;19:e45.
9. Lowenthal P, Borup J, West R, Archambault L. Thinking beyond zoom: using asynchronous video to maintain connection and engagement during the COVID-19 pandemic. J Technol Teacher Educ. 2020;28(2):383–391.
10. Mukhtar K, Javed K, Arooj M, Sethi A. Advantages, limitations and recommendations for online learning during COVID-19 pandemic era. Pak J Med Sci. 2020;36(COVID19–S4):S27–S31. doi:10.12669/pjms.36.COVID19-S4.2785
11. Irby DM, Cooke M, O’Brien BC. Calls for reform of medical education by the Carnegie foundation for the advancement of teaching: 1910 and 2010. Academic Medicine. 2010;85(2):220–227. doi:10.1097/ACM.0b013e3181c88449
12. Skochelak SE, Stack SJ. Creating the medical schools of the future. Academic Medicine. 2017;92(1):16–19. doi:10.1097/ACM.0000000000001160
13. Miller GE. The assessment of clinical skills competence performance. Acad Med. 1990;65:S63–S67. doi:10.1097/00001888-199009000-00045
14. Woolliscroft JO. Innovation in response to the COVID-19 pandemic crisis. Academic Medicine. 2020;95(8):1140–1142. doi:10.1097/ACM.0000000000003402
15. Baran E, Correia AP. A professional development framework for online teaching. TechTrends. 2014;58:96–102. doi:10.1007/s11528-014-0791-0
16. Ruiz JG, Mintzer MJ, Leipzig RM. The impact of e-learning in medical education. Academic Medicine. 2006;81(3):207–212. doi:10.1097/00001888-200603000-00002
17. Huynh R. The role of E-learning in medical education. Academic Medicine. 2017;92(4):430. doi:10.1097/ACM.0000000000001596
18. Evans DJR, Bay BH, Wilson TD, et al. Going virtual to support anatomy education: a STOP GAP in the midst of the Covid-19 pandemic. Anat Sci Educ. 2020;13:279–283. doi:10.1002/ase.1963
19. Srinivasan DK. Medical students’ perceptions and an anatomy teacher’s personal experience using an e-learning platform for tutorials during the Covid-19 crisis. Anat Sci Educ. 2020;13:318–319. doi:10.1002/ase.1970
20. Lim EC, Oh VM, Koh DR, Seet RC. The challenges of “continuing medical education” in a pandemic era. Ann Acad Med Singapore. 2009;38(8):724–726. doi:10.1097/00152193-200601000-00041
21. Biggs J. The definitive guide to constructive alignment. Teaching for quality learning at University. Buckingham: SRHE and Open University Press; 1999.
22. Norcini J, Burch V. Workplace-based assessment as an educational tool: AMEE Guide No. 31. Med Teach. 2007;29(9):855–871. doi:10.1080/01421590701775453
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.