")
Back to Journals » Journal of Experimental Pharmacology » Volume 12
Investigational and Experimental Drugs for Community-Acquired Pneumonia: the Current Evidence
Authors Sellarès-Nadal J , Burgos J, Falcó V, Almirante B
Received 30 September 2020
Accepted for publication 10 November 2020
Published 19 November 2020 Volume 2020:12 Pages 529—538
DOI https://doi.org/10.2147/JEP.S259286
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Bal Lokeshwar
Juilia Sellarès-Nadal, Joaquin Burgos, Vicenç Falcó, Benito Almirante
Infectious Diseases Department, Hospital Universitari Vall d’Hebron, Autonomous University of Barcelona, Barcelona, Spain
Correspondence: Benito Almirante
Infectious Diseases Department, Hospital Universitari Vall d’Hebron, Avda. Vall d’Hebron, 119-129, Barcelona 08035, Spain
Tel +34 274 60 90
Email [email protected]
Abstract: Community-acquired pneumonia (CAP) is a common infection with a constantly evolving etiological spectrum. This changing etiology conditions the adequate selection of optimal therapeutic regimens, both in empirical and definitive treatments. In recent years, new antimicrobials have been approved by regulatory authorities for use in CAP, although it is necessary to continue incorporating new antimicrobial agents that improve the activity profile in relation to the appearance of bacterial resistance in certain pathogens, such as pneumococcus, Staphylococcus aureus or Pseudomonas aeruginosa. Delafloxacin, omadacycline and lefamulin are the most recently approved antibiotics for CAP. These three antibiotics have shown non-inferiority to their comparators for the treatment of CAP with an excellent safety profile. However, in the 2019 ATS/IDSA guidelines, it has been considered that more information is needed to incorporate these new drugs into community-based treatment. New antimicrobials, such as solithromycin and nemonoxacin, are currently being studied in Phase III clinical trials. Both drugs have shown non-inferiority against the comparators and an acceptable safety profile; however, they have not yet been approved by the regulatory authorities. Several drugs are being tested in Phase I and II clinical trials. These include zabofloxacin, aravofloxacin, nafithromycin, TP-271, gepotidacin, radezolid, delpazolid, and CAL02. The preliminary results of these clinical trials allow us to assure that most of these drugs may play a role in the future treatment of CAP.
Keywords: community-acquired pneumonia, new antimicrobial drugs, fluoroquinolones, macrolides, tetracyclines, oxazolidinones
Introduction
Community-acquired pneumonia (CAP) continues to be an important challenge in the field of infectious diseases because is one of the most common infections that require hospitalization, especially in the elderly population and persons with co-morbid conditions.1–5
In the case of a patient with CAP, doctors have to decide which tests should be performed in order to determine the cause of pneumonia, which is the appropriate location to treat the patient and which is the best antibiotic therapy for this patient. Understanding the burden and the etiology of CAP is critical to making these decisions. Initial treatment of patients with CAP is empirical so the antibiotics chosen should cover the most common pathogens causing CAP but also those uncommon pathogens that may cause CAP in certain patients. This is one of the most important challenges in patients with CAP because the microbial etiology of CAP is constantly changing. The main features that have contributed to these changes in the last years are the widespread introduction of the pneumococcal conjugate vaccine, the emergence of resistant pathogens such as Pseudomonas aeruginosa or methicillin-resistant Staphylococcus aureus (MRSA) and the increased recognition of the role of viral pathogens.
Numerous antibiotics have been approved for the treatment of CAP by the Food and Drug Administration (FDA); however, it is necessary to continue the research of new drugs that are able to cover the entire etiological spectrum of CAP and with novel mechanisms of action that can overcome the increase of resistances and the emergence of resistant pathogens. In this article, we will perform a narrative review about the existing treatments for CAP and we will focus on the new drugs that are currently being investigated.
Etiology of CAP
Knowledge of the pathogens causing CAP is essential to select correct empirical treatments. The etiology of CAP is conditioned by several factors. The presence of underlying conditions, such as chronic lung disease or immunosuppression, local epidemiology or previous exposure to antibiotics is the most important.
In any textbook, the pathogen referred as the main cause of CAP is Streptococcus pneumoniae, accounting for up to two-thirds of bacteremic cases and for 30% of all CAP. Other pathogens include Haemophilus influenzae, which represents 12% and atypical microorganisms such as Mycoplasma pneumoniae, Chlamydiophila pneumoniae and Legionella spp. that account for 20% of CAP.1,6,7 Despite S. pneumoniae is the main bacterial microorganism isolated in CAP, in the latest studies its proportion is decreasing. This may partially be due to the introduction of the conjugated anti-pneumococcal vaccine in the United States and other countries.2
Moreover, recent studies point out that respiratory virus should also be taken into account. In these studies, viral isolates represent 20–30%, with influenza and rhinovirus in the head of viral pathogens.8 In fact, 2019 Infectious Diseases Society of America (IDSA) guidelines suggest that when influenza viruses are circulating, their presence should be investigated in patients with CAP.9 Such information has an impact, since a meta-analysis showed a higher risk of death in patients with viral-bacterial co-infection compared to patients with non-dual infection.10
On the other hand, with usual microbiological methods, pathogen detection is achieved in less than 50%.11 New diagnostic tools such as molecular techniques could contribute to the diagnosis of CAP, raising the level of microbiological diagnosis up to 85%. Therefore, these new methods have pointed out that mixed infections can represent 10–25% of all CAP.8,11 In the latest studies, etiologies of CAP include Gram-negative bacilli, such as Escherichia coli (11.5%), Klebsiella pneumoniae (4%) or P. aeruginosa (2.8%), and S. aureus (10.2%).12
Finally, multidrug-resistant organisms (MDRO), including MRSA and extended-spectrum beta-lactamase (ESBL) Enterobacteriaceae and P. aeruginosa, represent 6% of pathogens isolated in CAP, mostly in older patients with previous exposure to antibiotics, and they are associated with higher mortality.13 In North America, community-acquired MRSA, specially the USA300 clone, can cause a severe CAP presenting with rapid progression and hemoptysis.14
Current Treatment of CAP
Several guidelines for the diagnosis and treatment of CAP have been published, each one taking into account local epidemiology, health system particularities, drug side effects and cost-effectiveness. In this part, we assess general and most updated recommendations for the treatment of CAP in adults.
Most recommendations take into consideration the level of care (inpatient or outpatient) and severity of the disease. Severity can be assessed by scores, such as IDSA criteria, for severe pneumonia or by clinical judgment supported by CURB65, as recommended in British guidelines.9,15
The recommended treatment for healthy outpatients with CAP is amoxicillin, doxycycline or, in areas with low prevalence of macrolide-resistant S. pneumoniae, a macrolide. On the other hand, outpatients with co-morbidities, such as chronic lung disease, diabetes mellitus or alcoholism should be treated with amoxicillin-clavulanate acid plus a macrolide or with a respiratory fluoroquinolone.9
Treatment of hospitalized patients depends on severity. Patients with severe CAP should be treated with combined therapy with β-lactam plus macrolide or β-lactam plus fluoroquinolone. Several studies and meta-analysis support combined therapy for critically ill patients with CAP.16,17 In hospitalized patients with non-severe CAP, combination of a β-lactam plus a macrolide or a respiratory fluoroquinolone is recommended. Evidence of superiority of combined treatment with β-lactam plus macrolide over β-lactam monotherapy in non-critically ill patients with CAP is less robust and studies have drawn contradictory conclusions on this issue.18,19
Finally, previous guidelines defined “healthcare-associated pneumonia” (HCAP) as a pneumonia occurring in patients with higher risk of MDRO. Risk factors considered are residence in nursing homes, recent hospitalization, or chronic conditions, among others.20 The latest guidelines recommend avoiding the term as it leads to an increase in the use of broad-spectrum antibiotics without better results.21 Therefore, the current recommendation is to individually assess clinical probability of resistant-pathogens and to adjust treatment to local epidemiology.9
Do We Need New Antibiotics for CAP?
The constant epidemiological changes have raised some issues that justify the research of new antibiotics for CAP. Although penicillin resistance has been a matter of concern for many years, currently we have learned that levels of β-lactam resistance in most settings generally do not result in treatment failure for patients with pneumococcal pneumonia when appropriate agents and doses are used.22–24 On the contrary, resistance of S. pneumoniae to macrolides is significant, with a prevalence of 20 to 40% in some settings.25,26 In the same way, resistance of M. pneumoniae to macrolides is also emerging worldwide.27 For these reasons, macrolide monotherapy, that was recommended for outpatients in the 2007 American Thoracic Society (ATS)/IDSA guidelines, has evolved to a conditional recommendation because of concerns on resistance levels to macrolides in the 2019 ATS/IDSA guidelines.9,28
On the other hand, the emergence of MDRO, including MRSA and P. aeruginosa, requires consideration in the empirical treatment coverage in some patients with risk factors for these etiologic agents.29 Although infection by S. aureus is still uncommon in most patients with CAP, its incidence is increasing in pediatric population and during the influenza season. Enterobacteriaceae and P. aeruginosa accounts in <2% of cases of CAP, but they are increasing in elderly patients with co-morbidities. So, appropriate therapy for these pathogens may be necessary for selected patients, since the impact of failing in initial treatment may be high, especially in critically ill patients.2
Finally, the description of adverse events related to the use of fluoroquinolones has raised concerns regarding its generalized use in all patients with CAP. While some of these adverse events, such as tendinopathy and tendon rupture were already known since years ago, others have become relevant more recently for their severity (severe hypoglycemia, adverse psychiatric events, QT prolongation or aortic rupture and dissection). For these reasons FDA has suggested that fluoroquinolones should be reserved for those patients who have no other treatment options.30
New Antimicrobials Recently Approved for CAP
Delafloxacin
Delafloxacin is a novel fluoroquinolone with a broad spectrum that includes Gram-positive and Gram-negative organisms, including MRSA and P. aeruginosa.31 It is also active against atypical microorganisms causing CAP. Delafloxacin differs from other fluoroquinolones in that delafloxacin exerts a minimal effect on cytochrome P450 enzymes and on the corrected QT interval so there does not seem to be a risk of QT prolongation. The efficacy of delafloxacin for CAP was demonstrated in a Phase 3, randomized double-blind trial.32 In this study iv delafloxacin, with potential to switch to oral delafloxacin, was compared to iv moxifloxacin, with potential to switch to oral moxifloxacin and potential to switch moxifloxacin to iv linezolid for confirmed MRSA. A total of 860 patients with CAP in PORT risk class of II to V were planned to be enrolled and finally 859 were included in the intention-to-treat (ITT) population. Overall, 88.9% of patients who received delafloxacin and 89.0% of patients who received moxifloxacin met the primary end-point of statistical non-inferiority for early clinical response at 96 hours. Delafloxacin was well-tolerated. The most common adverse events (≥2%) were diarrhea and increases in transaminase levels, which were generally mild and did not lead routinely to treatment discontinuation. As a consequence of these results, the FDA approved delafloxacin for the treatment of adults with CAP the past 10/24/2019.33
Omadacycline
Omadacycline is a new aminomethylcycline, a derivate of tetracycline, with a mechanism of action based on its binding to the primary tetracycline site on bacterial 30S ribosomal subunit with high specificity. An advantage over older tetracyclines is that it is able to overcome the efflux and ribosomal protection mechanisms of tetracycline resistance. Omadacycline is active against pathogens that cause CAP, including S. pneumoniae, H. influenzae, S. aureus, and atypical pathogens.34 The efficacy of omadacycline was evaluated in the OPTIC trial, a double-blind trial in which once-daily omadacycline was compared to moxifloxacin for the treatment of adults with CAP in PORT risk class II to IV.35 The ITT population included 386 patients in the omadacycline group and 388 patients in the moxifloxacin group. Omadacycline showed non-inferiority to moxifloxacin for early clinical response (81.1% and 82.7%, respectively), and for the rates of investigator-assessed clinical response at the post-treatment evaluation (87.6% and 85.1%, respectively). The most frequent events were gastrointestinal side effects (10.2% and 18.0%, respectively). Although FDA approved omadacycline for CAP the 10/02/2018,36 recent ATS/IDSA guidelines state that omadacycline needs further validation in the outpatient setting.9
Lefamulin
Lefamulin is a semi-synthetic agent that belongs to the pleuromutilin class of antibiotics. The precise mechanism of action is based on the binding to the peptidyl-transferase center of the 50S ribosomal subunit of the bacteria. Lefamulin has a potent antimicrobial activity against Gram-positive microorganisms, including S. pneumoniae, and some Gram-negative pathogens (H. influenzae, Moraxella catarrhalis and Neisseria spp.), as well as against mycoplasmas and intracellular organisms, such as Chlamydia spp. and Legionella pneumophila.37 It has a good oral bioavailability and an excellent penetration into epithelial lining fluid of the lung. The clinical efficacy of lefamulin in patients with CAP was evaluated in two multicentre, randomized, double-blind, double-dummy, phase 3 trials, the Lefamulin Evaluation Against Pneumonia (LEAP 1 and 2) trials. The LEAP 1 study demonstrated the clinical efficacy and safety of iv-to-oral lefamulin compared to moxifloxacin ± linezolid in adult patients with moderate to severe CAP.38 The LEAP 2 study compared the safety and efficacy of oral lefamulin twice daily for 5 days versus oral moxifloxacin once daily for 7 days in 738 adult patients with moderate CAP, and also demonstrated non-inferiority between the two therapeutic options.39 On August of 2019, based on the results of these trials, the FDA announced the approval of lefamulin for the treatment of CAP.40 Despite this approval the ATS and the IDSA demand further validation in the outpatient setting.9
Investigational Drugs Currently in Phase III Clinical Trials
The phase III clinical trials including these drugs for patients with CAP are listed in Table 1.
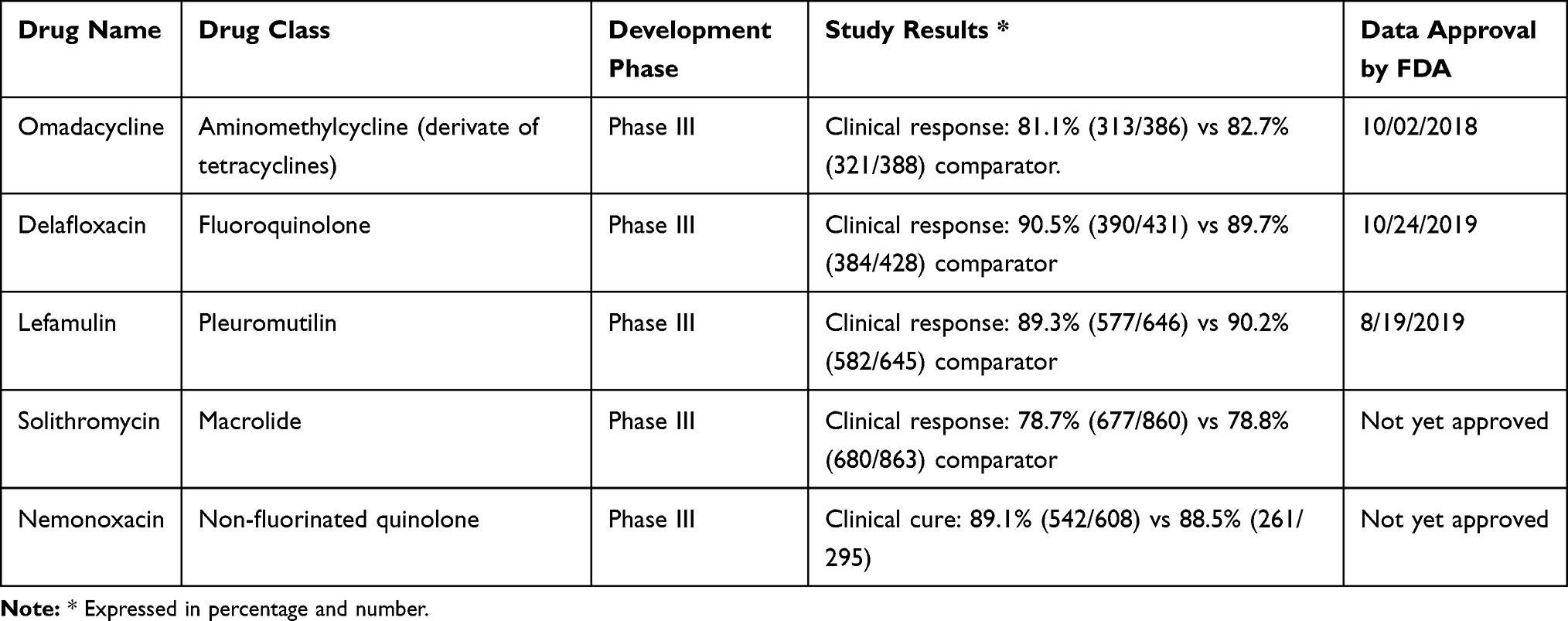 |
Table 1 Antimicrobials in Phase III Clinical Trials |
Solithromycin
Solithromycin is a fourth-generation macrolide and the first fluroketolide in development. Solithromycin acts binding to three different sites of 50S ribosomal unit, resulting in a potent antibacterial activity and a low tendency to select for resistant mutants.41 This drug has activity against the most common typical and atypical CAP pathogens, including fluoroquinolone-, macrolide-, and penicillin-resistant isolates.41 Two phase III trials, SOLITAIRE-ORAL and SOLITAIRE-IV, have evaluated the safety and efficacy of oral and iv solithromycin, respectively, for the treatment of CAP.42,43 Both trials have shown non-inferiority compared with moxifloxacin for the early clinical response meeting the FDA's primary end-point (SOLITAIRE-ORAL, difference = −0.19, 95% CI, −5.8 to 5.5, and SOLITAIRE-IV, difference = −0.46, 95% CI, −6.1 to 5.2). In SOLITAIRE-ORAL, side effects were comparable between both groups. However, in SOLITAIRE-IV more than 50% of patients in the solithromycin arm had drug-related adverse events, compared with 35% in the moxifloxacin arm. This difference was driven mainly by infusion reactions, more common in the solithromycin group (31.3%) compared to the moxifloxacin group (5.4%).43 Nevertheless, hepatic safety remains a concern, with 5–10% of patients experiencing mild asymptomatic transaminase elevations. Given the relatively small sample sizes (<1000 patients) in which solithromycin was studied, the FDA recommended that the company initiates a new clinical study with a greater number of patients to better evaluate its safety profile before formally granting approval.44
Nemonoxacin
Nemonoxacin is a recently developed non-fluorinated quinolone antibiotic. Nemonoxacin has a broad spectrum of activity against Gram-positive, Gram-negative, and atypical pathogens, and a reduced resistance profile compared with other fluoroquinolones. It displays good in vitro activity against MRSA, penicillin-resistant S. pneumoniae, and ertapenem-non-susceptible Enterobacteriaceae.45–47 This is achieved by its targeting to both topoisomerase II and IV.
Different Phase II and III clinical trials have investigated the clinical efficacy and safety of nemonoxacin in the treatment of CAP in comparison with levofloxacin.48–51 A recent meta-analysis of most recent phase III trial found that nemonoxacin and levofloxacin had similar clinical cure rates in the treatment of CAP (OR = 1.05, 95% CI, 0.67–1.64). Nemonoxacin also had a similar microbiologic response rate than levofloxacin (OR = 0.89, 95% CI, 0.44 to 1.81). The safety/tolerability of nemonoxacin was also comparable with levofloxacin, so no significant differences were found in adverse events between the two drugs (OR = 1.08, 95% CI, 0.81 to 1.43). In subgroup analysis of dose of nemonoxacin (500 or 750 mg) and individual pathogens, results remained unchanged.47 It has received priority review status by the FDA as a “qualified infectious disease product” once further phase III studies are available documenting its safety and efficacy.
Investigational Drugs in Phase I and II Clinical Trials
Several drugs for the treatment of CAP are currently being investigated in phase I and phase II clinical trials. Quinolone are the leading antibiotic class, with 6 compounds under clinical testing. Of this, ACH-702, WCK-771, WCK-2389 and KPI-10 are new quinolones with activity against common respiratory pathogens, including resistant isolates, and with potential to treat respiratory tract infections. Nevertheless, these drugs have not yet been studied in phase I clinical trials. The next groups of antibiotic are tetracyclines and ketolides, with three drugs in study. Oxazolidinones are also an important class, with two compounds currently in clinical trials. Finally, a non-antibiotic drug with antitoxin activity completes the compounds under investigation. The targets of most of these drugs are not only patients with CAP but also patients with other types of infections. The phase I and II clinical trials including these drugs for patients with CAP are listed in Table 2.
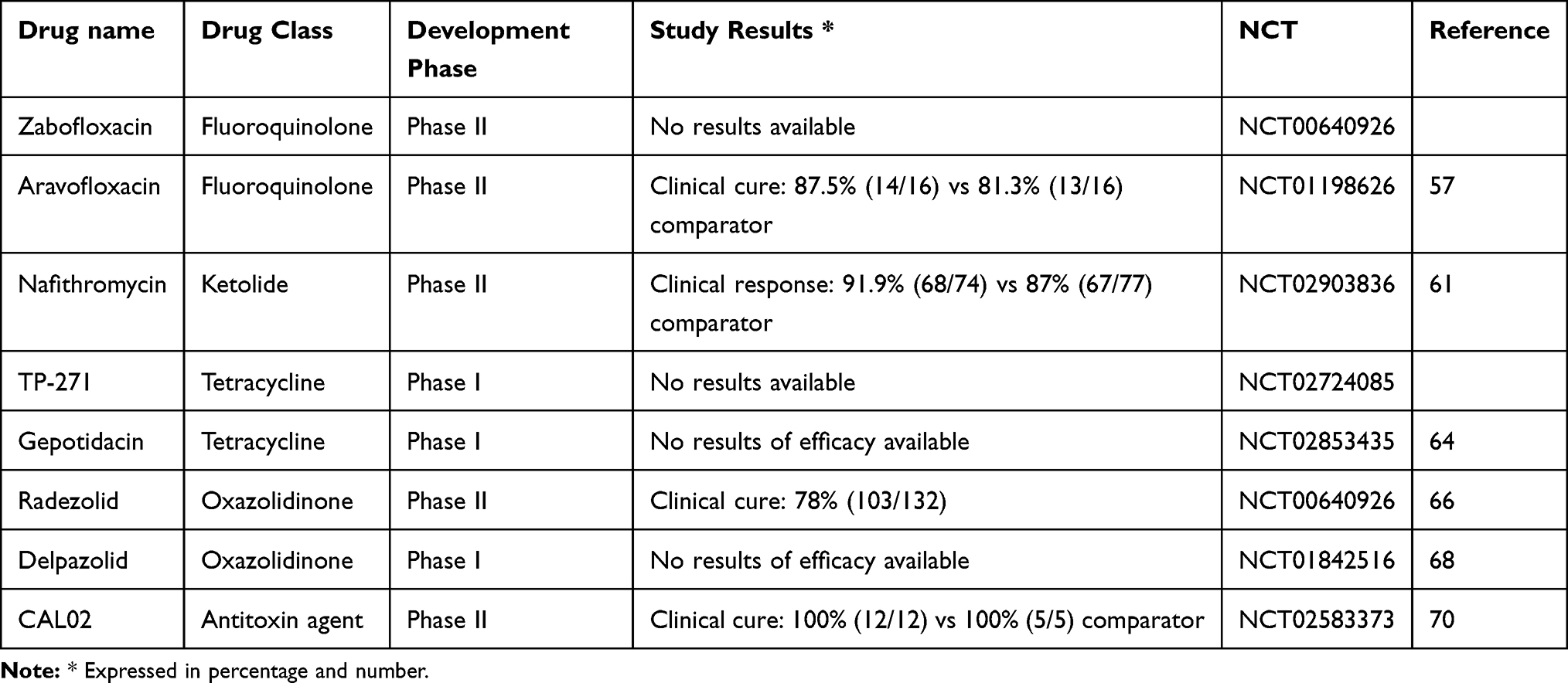 |
Table 2 Compounds in Phase I and II Clinical Trials |
Zabofloxacin
Zabofloxacin is a novel fluoroquinolone with identical mechanism of action than other quinolones and with a broad-spectrum against respiratory pathogens. It has proven bactericidal efficacy both in vitro and in vivo against Gram-positive and Gram-negative pathogens, including S. pneumoniae, S. aureus, H. influenzae, and M. catarrhalis. By contrast, zabofloxacin has no activity against major pathogens associated with hospital-acquired pneumonia, such as P. aeruginosa and Acinetobacter baumannii.52,53 Scarce clinical data exist regarding the efficacy of this drug in pneumonia. Only, a phase II clinical trial to evaluate the safety and efficacy of oral zabofloxacin compared with oral levofloxacin in CAP has been performed, and although it was finished in 2012, results have not been yet published.54
Aravofloxacin (JNJ-Q2)
Aravofloxacin (JNJ-Q2) is a novel fifth-generation fluoroquinolone that has excellent in vitro and in vivo activity against a variety of Gram-positive and Gram-negative organisms. In vitro studies that included 3757 isolates indicate that aravofloxacin has potent activity against pathogens responsible for CAP, such as S. aureus (MIC50, 0.12 μg/mL) and S. pneumoniae (MIC50/90, 0.008/0.015 μg/mL), being >16-fold more potent than moxifloxacin and levofloxacin. The activity of avarofloxacin was equivalent to that of moxifloxacin against Gram-negative microorganisms.55,56 Aravofloxacin has also been shown to have a higher barrier to resistance compared to other agents in the class and it remains highly active against drug-resistant organisms, including MRSA, ciprofloxacin-resistant S. aureus, and drug-resistant S. pneumonia.55,56 A Phase II, randomized, double-blind, multicenter study evaluating the efficacy of aravofloxacin (150 mg iv every 12 hours, followed by 250 mg orally every 12 hours) versus that of moxifloxacin (400 mg iv or orally every 24 hours) for the treatment of CAP has been published.57 The study was designed to enroll 120 subjects to ensure ability to detect non-inferiority of aravofloxacin to moxifloxacin; however, this was not feasible due to the strict inclusion criteria. Clinical cure was achieved in 87.5% (14/16) and 81.3% (13/16) of patients treated with aravofloxacin and moxifloxacin, respectively (OR = 1.66, 95% CI, 0.23 to 11.75). However, the small sample sizes preclude to have sufficient power to detect non-inferiority for clinical test of cure. Adverse events were comparable between aravofloxacin and moxifloxacin, with the exception of nausea and vomiting.57 Considering its early stage of development, the definitive role of aravofloxacin against these infections and its safety profile will have to be determined in future phase III studies.
Nafithromycin
Nafithromycin (WCK 4873) is a novel antimicrobial agent of the ketolide class that interacts at multiple positions on the ribosome, thus allowing for activity against macrolide-resistant organisms.58 In a collection of 4739 clinical isolates, compiled worldwide, the antibiotic showed in vitro potency against S. pneumoniae (MIC50/90, 0.015/0.06 μg/mL), S. aureus (MIC50/90, 0.06/>2 μg/mL), and comparable in vitro activities against H. influenzae and M. catarrhalis isolates (MIC90 0.25 μg/mL).59 This drug has also an attractive pharmacokinetic profile, a good absorption, high levels in lung tissue, a good penetration in alveolar macrophages, and it seems to have an acceptable hepatic safety.60 A phase II, randomized, placebo-controlled study evaluated the safety, tolerability, pharmacokinetics, and efficacy of oral nafithromycin (800 mg 3 days and 5 days) versus oral moxifloxacin in the treatment of CAP in adults. The primary end-point (clinical response at day 4, tested in the ITT population) was achieved in 91.9% (68/74), 89% (65/73) and 87% (67/77) of patients in the nafithromycin 3 days, nafithromycin 9 days and moxifloxacin groups, respectively. Rates of serious adverse events were similar between groups (around 1–2%), nevertheless, nafithromycin had more non-serious adverse events, mainly gastrointestinal disorders (14.9% versus 12.5% versus 7.9%, respectively).61
TP-271
TP-271 is a promising new tetracycline with in vitro activity against the major pathogens associated with CAP.62 TP-271 is currently under assessment in phase I trial, single ascending-dose, in order to evaluate its safety, tolerability, and pharmacokinetics in patients with pneumonia.63
Gepotidacin
Gepotidacin is a broad-spectrum antibacterial agent with a novel mechanism of action. It inhibits the B subunit of DNA gyrase. Initial phase I studies with escalating oral dosing have demonstrated a safety profile similar to those of other marketed antibiotics.64 Its antibacterial activity and its properties make it have a potential role in the treatment of CAP.
Radezolid
Radezolid (RX-1741) is a novel oxazolidinone antibiotic agent and is the first biaryloxazolidinone in clinical development. It is being developed for the treatment of serious MDRO infections, including infections caused by linezolid-resistant strains. Radezolid has shown excellent activity against a number of key CAP pathogens, including S. pneumoniae, S. aureus, H. influenzae, and atypical respiratory pathogens.65 It is 11 times more active in comparison to linezolid against a series of bacterial species capable of surviving intracellularly, such as Staphylococcus, Chlamydia, and Legionella species. A phase II clinical trial has been completed evaluating radezolid in mild-to-moderate CAP at three different doses: 300 mg once daily, 450 mg once daily, and 450 mg twice daily for 7–10 days. The study showed comparable efficacy across all three doses, with clinical cure rates ranging from 78 to 92%.66 However, its safety profile has not been established and its advantages over linezolid and tedizolid are not clear at present. Redezolid is ready for entering a phase III trial.
Delpazolid
Delpazolid (LCB01-0371) is a new oxazolidinone with good in vitro and in vivo activities against Gram-positive bacteria, similar to linezolid.67 The drug has also interesting properties such as high aqueous solubility and good absorption, distribution, metabolism, excretion, and toxicity and PK profiles.68 There are no phase II studies ongoing; however, its characteristics make it have a potential role in the treatment of CAP.
CAL02
CAL02 is a non-antibiotic drug, a novel antitoxin agent with a singular mechanism of action. CAL02 consists of a mixture of liposomes that capture bacterial toxins known to dysregulate inflammation, cause organ damage, and impede immune defense. Preclinical data show that when combined with antibiotics, CAL02 substantially improves survival outcomes in mice with severe pneumonia and bacteremia.69 A randomized, phase II, double-blind, multicentre, placebo-controlled trial was done in patients with severe pneumococcal CAP who required ICU admission. Nineteen patients were randomly assigned, resulting in 14 patients in the CAL02 groups (3 assigned to low-dose CAL02 and 11 assigned to high-dose CAL02) and 5 in the placebo group. Despite the limited number of patients, better patient outcomes were observed in the high-dose CAL02 group compared with placebo, with similar rates of side effects.70 The results of this study support further clinical development of CAL02 and provide a solid basis for a larger clinical study.
Conclusion
The treatment of CAP is a continuous challenge due to the constant changes in its etiological spectrum and the appearance of bacterial resistances. In recent years, new antimicrobials have been approved for use in CAP therapy, both at the hospital and community levels. Currently, several antimicrobials are being evaluated in phase III clinical trials and their results allow their possible incorporation into the treatment of CAP. Several drugs are being evaluated in preclinical phases with the aim of demonstrating efficacy against the majority of pathogens causing CAP. Quinolone are the leading antibiotic class, with more compounds under clinical testing. However, increasing concerns exist about its safety due to the reporting of some rare adverse events as tendinopathies or aortic dissection. On this basis, tetracyclines and ketolides could be interesting drugs to explore.
Funding
The authors are supported by Plan Nacional de I+D+I 2013–2016. They are also supported by the Instituto de Salud Carlos III, Subdirección General de Redes y Centros de Investigación Cooperativa, Ministerio de Economía, Industria y Competitividad, and the Spanish Network for Research in Infectious Diseases [REIPI RD16/0016/0003], which is co-financed by European Development Regional Fund ‘A way to achieve Europe’ and Operative program Intelligent Growth 2014–2020.
Disclosure
J. Burgos has received honoraria for speaking at educational events from Janssen Pharmaceuticals, Merck Sharp and Dohme (MSD) and ViiV Healthcare and has received research funding from MSD. V. Falco has received honoraria for speaking at educational events for Janssen Pharmaceuticals, MSD, ViiV Healthcare, has received research funding from Gilead Sciences, MSD and ViiV Healthcare, and reports grants and personal fees from Merck Sharp Dhome, ViiV, and Gilead and personal fees from Janssen Pharmaceuticals, outside the submitted work. B. Almirante has received honoraria for speaking at educational events from MSD, Pfizer Inc, Gilead Sciences and Angellini and has received research funding from Gilead Sciences, MSD and Pfizer Inc. The authors have no other relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript apart from those disclosed.
References
1. Prina E, Ranzani OT, Torres A. Community-acquired pneumonia. Lancet. 2015;386:1097–1108. doi:10.1016/S0140-6736(15)60733-4
2. Jain S, Self WH, Wunderink RG, et al. Community-acquired pneumonia requiring hospitalization among U.S. adults. N Engl J Med. 2015;373:415–427. doi:10.1056/NEJMoa1500245
3. Griffin MR, Zhu Y, Moore MR, et al. U.S. hospitalizations for pneumonia after a decade of pneumococcal vaccination. N Engl J Med. 2013;369:155–163. doi:10.1056/NEJMoa1209165
4. Ramirez JA, Wiemken TL, Peyrani P, et al. Adults Hospitalized with pneumonia in the United States: incidence, epidemiology, and mortality. Clin Infect Dis. 2017;65:1806–1812. doi:10.1093/cid/cix647
5. Bordon J, Slomka M, Gupta R, et al. Hospitalization due to community-acquired pneumonia in patients with chronic obstructive pulmonary disease: incidence, epidemiology and outcomes. Clin Microbiol Infect. 2020;26:220–226. doi:10.1016/j.cmi.2019.06.025
6. File TM. Community-acquired pneumonia. Lancet. 2003;362:1991–2001. doi:10.1016/S0140-6736(03)15021-0
7. Lim WS, Macfarlane JT, Boswell TCJ, et al. Study of community acquired pneumonia aetiology (SCAPA) in adults admitted to hospital: implications for management guidelines. Thorax. 2001;56:296–301. doi:10.1136/thorax.56.4.296
8. Johansson N, Kalin M, Tiveljung-Lindell A, et al. Etiology of community-acquired pneumonia: increased microbiological yield with new diagnostic methods. Clin Infect Dis. 2010;50:202–209. doi:10.1086/648678
9. Metlay JP, Waterer GW, Long AC, et al. Diagnosis and treatment of adults with community-acquired pneumonia. Am J Respir Crit Care Med. 2019;200:E45–E67. doi:10.1164/rccm.201908-1581ST
10. Burk M, El-Kersh K, Saad M, et al. Viral infection in community-acquired pneumonia: A systematic review and meta-analysis. Eur Respir Rev. 2016;25:178–188. doi:10.1183/16000617.0076-2015
11. Holter JC, Müller F, Bjørang O, et al. Etiology of community-acquired pneumonia and diagnostic yields of microbiological methods: A 3-year prospective study in Norway. BMC Infect Dis. 2015;15:64. doi:10.1186/s12879-015-0803-5
12. Gadsby NJ, Russell CD, Mchugh MP, et al. Comprehensive molecular testing for respiratory pathogens in community-acquired pneumonia. Clin Infect Dis. 2016;62:817–823. doi:10.1093/cid/civ1214
13. Prina E, Ranzani OT, Polverino E, et al. Risk factors associated with potentially antibiotic-resistant pathogens in community-acquired pneumonia. Ann Am Thorac Soc. 2015;12:153–160. doi:10.1513/AnnalsATS.201407-305OC
14. Wunderink RG, Waterer G. Advances in the causes and management of community acquired pneumonia in adults. BMJ. 2017;358:1–13. doi:10.1136/bmj.j2471
15. Lim WS, Baudouin S, George R, et al. British Thoracic Society guidelines for the management of community acquired pneumonia in adults: update 2009. Thorax. 2009;64(Suppl 3):iii1–55. doi:10.1136/thx.2009.121434
16. Sligl WI, Asadi L, Eurich DT, et al. Macrolides and mortality in critically ill patients with community-acquired pneumonia: a systematic review and meta-analysis. Crit Care Med. 2014;42:420–432. doi:10.1097/CCM.0b013e3182a66b9b
17. Restrepo MI, Mortensen EM, Waterer GW, et al. Impact of macrolide therapy on mortality for patients with severe sepsis due to pneumonia. Eur Respir J. 2009;33:153–159. doi:10.1183/09031936.00054108
18. Lee JS, Giesler DL, Gellad WF, Fine MJ. Antibiotic therapy for adults hospitalized with community-acquired pneumonia a systematic review. JAMA - J Am Med Assoc. 2016;315:593–602. doi:10.1001/jama.2016.0115
19. Postma DF, Van Werkhoven CH, Van Elden LJR, et al. Antibiotic treatment strategies for community-acquired pneumonia in adults. N Engl J Med. 2015;372:1312–1323. doi:10.1056/NEJMoa1406330
20. American Thoracic Society. Infectious Diseases Society of America. Guidelines for the management of adults with hospital-acquired, ventilator-associated, and healthcare-associated pneumonia. Am J Respir Crit Care Med. 2005;171:388–416. doi:10.1164/rccm.200405-644ST
21. Grenier C, Pépin J, Nault V, et al. Impact of guideline-consistent therapy on outcome of patients with healthcare-associated and community-acquired pneumonia. J Antimicrob Chemother. 2011;66:1617–1624. doi:10.1093/jac/dkr176
22. Mufson MA, Chan G, Stanek RJ. Penicillin resistance not a factor in outcome from invasive Streptococcus pneumoniae community-acquired pneumonia in adults when appropriate empiric therapy is started. Am J Med Sci. 2007;333:161–167. doi:10.1097/MAJ.0b013e3180312cd5
23. Tleyjeh IM, Tlaygeh HM, Hejal R, et al. The impact of penicillin resistance on short-term mortality in hospitalized adults with pneumococcal pneumonia: a systematic review and meta-Analysis. Clin Infect Dis. 2006;42:788–797. doi:10.1086/500140
24. Weinstein MP, Klugman KP, Jones RN. Rationale for revised penicillin susceptibility breakpoints versus Streptococcus pneumoniae: coping with antimicrobial susceptibility in an era of resistance. Clin Infect Dis. 2009;48:1596–1600. doi:10.1086/598975
25. Cherazard R, Epstein M, Doan TL, et al. Antimicrobial resistant Streptococcus pneumoniae. Am J Ther. 2017;24:e361–e369. doi:10.1097/MJT.0000000000000551
26. Schroeder MR, Stephens DS. Macrolide resistance in Streptococcus pneumoniae. Front Cell Infect Microbiol. 2016;6:1–9. doi:10.3389/fcimb.2016.00098
27. Haran JP, Volturo GA. Macrolide resistance in cases of community-acquired bacterial pneumonia in the Emergency Department. J Emerg Med. 2018;55:347–353. doi:10.1016/j.jemermed.2018.04.031
28. Mandell LA, Wunderink RG, Anzueto A, et al. Infectious Diseases Society of America/American Thoracic Society consensus guidelines on the management of community-acquired pneumonia in adults. Clin Infect Dis. 2007;44:S27–S72. doi:10.1086/511159
29. Self WH, Wunderink RG, Williams DJ, et al. Staphylococcus aureus community-acquired pneumonia: prevalence, clinical characteristics, and outcomes. Clin Infect Dis. 2016;63:300–309. doi:10.1093/cid/ciw300
30. FDA Drug Safety Communication. FDA updates warnings for oral and injectable fluoroquinolone antibiotics due to disabling side effects. FDA. Available from: https://www.fda.gov/drugs/drug-safety-and-availability/fda-drug-safety-communication-fda-updates-warnings-oral-and-injectable-fluoroquinolone-antibiotics.
31. Mogle BT, Steele JM, Thomas SJ, et al. Clinical review of delafloxacin: a novel anionic fluoroquinolone. J Antimicrob Chemother. 2018;73:1439–1451. doi:10.1093/jac/dkx543
32. Horcajada JP, Salata RA, Álvarez-Sala R, et al. A phase 3 study to compare delafloxacin with moxifloxacin for the treatment of adults with community-acquired bacterial pneumonia (Define-CABP). Open Forum Infect Dis. 2020;7:1–13. doi:10.1093/ofid/ofz514
33. Melinta Therapeutics announces U.S. FDA approval of supplemental new drug application for BAXDELA® (delafloxacin) for the treatment of community-acquired bacterial pneumonia (CABP). Melinta Therapeutics, Inc. Available from: http://ir.melinta.com/news-releases/news-release-details/melinta-therapeutics-announces-us-fda-approval-supplemental-new.
34. Baker DE. Omadacycline. Hosp Pharm. 2019;54:80–87. doi:10.1177/0018578718823730
35. Stets R, Popescu M, Gonong JR, et al. Omadacycline for community-acquired bacterial pneumonia. N Engl J Med. 2019;380:517–527. doi:10.1056/NEJMoa1800201
36. Chambers HF. Omadacycline - The newest tetracycline. N Engl J Med. 2019;380:588–589. doi:10.1056/NEJMe1900188
37. Falcó V, Burgos J, Almirante B. An overview of lefamulin for the treatment of community acquired bacterial pneumonia. Expert Opin Pharmacother. 2020;21:629–636. doi:10.1080/14656566.2020.1714592
38. File TM, Goldberg L, Das A, et al. Efficacy and safety of intravenous-to-oral lefamulin, a pleuromutilin antibiotic, for the treatment of community-acquired bacterial pneumonia: the Phase III lefamulin evaluation against pneumonia (LEAP 1) trial. Clin Infect Dis. 2019;69:1856–1867. doi:10.1093/cid/ciz090
39. Alexander E, Goldberg L, Das AF, et al. Oral lefamulin vs moxifloxacin for early clinical response among adults with community-acquired bacterial pneumonia: the LEAP 2 randomized clinical trial. JAMA - J Am Med Assoc. 2019;322:1661–1671. doi:10.1001/jama.2019.15468
40. Sakoulas GM. U.S. FDA approves lefamulin for community-acquired bacterial pneumonia. NEJM J Watch. 2019. doi:10.1056/NEJM-JW.NA49805
41. Donald BJ, Surani S, Deol HS, et al. Spotlight on solithromycin in the treatment of community-acquired bacterial pneumonia: design, development, and potential place in therapy. Drug Des Devel Ther. 2017;1:3559–3566. doi:10.2147/DDDT.S119545
42. Barrera CM, Mykietiuk A, Metev H, et al. Efficacy and safety of oral solithromycin versus oral moxifloxacin for treatment of community-acquired bacterial pneumonia: a global, double-blind, multicentre, randomised, active-controlled, non-inferiority trial (SOLITAIRE-ORAL). Lancet Infect Dis. 2016;16:421–430. doi:10.1016/S1473-3099(16)00017-7
43. File TM, Rewerska B, Vucinić-Mihailović V, et al. SOLITAIRE-IV: a randomized, double-blind, multicenter study comparing the efficacy and safety of intravenous-to-oral solithromycin to intravenous-to-oral moxifloxacin for treatment of community-acquired bacterial pneumonia. Clin Infect Dis. 2016;63:1007–1016. doi:10.1093/cid/ciw490
44. FDA Briefing Document. Solithromycin oral capsule and injection meeting of the Antimicrobial Drugs Advisory Committee (AMDAC). November. 2016;4.
45. Lai CC, Liu WL, Ko WC, et al. Multicenter study in Taiwan of the in vitro activities of nemonoxacin, tigecycline, doripenem, and other antimicrobial agents against clinical isolates of various Nocardia species. Antimicrob Agents Chemother. 2011;55:2084–2091. doi:10.1128/AAC.01808-10
46. Chotikanatis K, Kohlhoff SA, Hammerschlag MR. In vitro activity of nemonoxacin, a novel nonfluorinated quinolone antibiotic, against Chlamydia trachomatis and Chlamydia pneumoniae. Antimicrob Agents Chemother. 2014;58:1800–1801. doi:10.1128/AAC.02263-13
47. Chang SP, Lee HZ, Lai CC, Tang HJ. The efficacy and safety of nemonoxacin compared with levofloxacin in the treatment of community-acquired pneumonia: a systemic review and meta-analysis of randomized controlled trials. Infect Drug Resist. 2019;12:433–438. doi:10.2147/IDR.S193233
48. Liu Y, Zhang Y, Wu J, et al. A randomized, double-blind, multicenter Phase II study comparing the efficacy and safety of oral nemonoxacin with oral levofloxacin in the treatment of community-acquired pneumonia. J Microbiol Immunol Infect. 2017;50:811–820. doi:10.1016/j.jmii.2015.09.005
49. Amalakuhan B, Echevarria KL, Restrepo MI. Managing community acquired pneumonia in the elderly - the next generation of pharmacotherapy on the horizon. Expert Opin Pharmacother. 2017;18:1039–1048. doi:10.1080/14656566.2017.1340937.MANAGING
50. Yuan J, Mo B, Ma Z, et al. Safety and efficacy of oral nemonoxacin versus levofloxacin in treatment of community-acquired pneumonia: a phase 3, multicenter, randomized, double-blind, double-dummy, active-controlled, non-inferiority trial. J Microbiol Immunol Infect. 2019;52:35–44. doi:10.1016/j.jmii.2017.07.011
51. Van Rensburg DJJ, Perng RP, Mitha IH, et al. Efficacy and safety of nemonoxacin versus levofloxacin for community-acquired pneumonia. Antimicrob Agents Chemother. 2010;54:4098–4106. doi:10.1128/AAC.00295-10
52. Kwon AR, Min YH, Ryu JM, et al. In vitro and in vivo activities of DW-224a, a novel fluoroquinolone antibiotic agent. J Antimicrob Chemother. 2006;58:684–688. doi:10.1093/jac/dkl304
53. Kocsis B, Domokos J, Szabo D. Chemical structure and pharmacokinetics of novel quinolone agents represented by avarofloxacin, delafloxacin, finafloxacin, zabofloxacin and nemonoxacin. Ann Clin Microbiol Antimicrob. 2016;15:1–8. doi:10.1186/s12941-016-0150-4
54. Safety and efficacy study of oral zabofloxacin in community-acquired pneumonia. ClinicalTrials.gov. Available from: https://clinicaltrials.gov/ct2/show/NCT01081964?cond=zabofloxacin&draw=2&rank=2.
55. Morrow BJ, He W, Amsler KM, et al. In vitro antibacterial activities of JNJ-Q2, a new broad-spectrum fluoroquinolone. Antimicrob Agents Chemother. 2010;54:1955–1964. doi:10.1128/AAC.01374-09
56. Biedenbach DJ, Farrell DJ, Flamm RK, et al. Activity of JNJ-Q2, a new fluoroquinolone, tested against contemporary pathogens isolated from patients with community-acquired bacterial pneumonia. Int J Antimicrob Agents. 2012;39:321–325. doi:10.1016/j.ijantimicag.2011.11.016
57. Covington PS, Davenport JM, Andrae DA, et al. A Phase 2 study of the novel fluoroquinolone JNJ-Q2 in community-acquired bacterial pneumonia. J Antimicrob Chemother. 2013;68:2691–2693. doi:10.1093/jac/dkt217
58. Krokidis MG, Márquez V, Wilson DN, et al. Insights into the mode of action of novel fluoroketolides, potent inhibitors of bacterial protein synthesis. Antimicrob Agents Chemother. 2014;58:472–480. doi:10.1128/AAC.01994-13
59. Flamm RK, Rhomberg PR, Sader HS. In vitro activity of the novel lactone ketolide nafithromycin (WCK 4873) against contemporary clinical bacteria from a global surveillance program. Antimicrob Agents Chemother. 2017;61:1–8. doi:10.1128/AAC.01230-17
60. Rodvold KA, Gotfried MH, Chugh R, et al. Comparison of plasma and intrapulmonary concentrations of nafithromycin (WCK 4873) in healthy adult subjects. Antimicrob Agents Chemother. 2017;61:1–9. doi:10.1128/AAC.01096-17
61. Phase II study of oral nafithromycin in CABP - Study results - ClinicalTrials.gov. Available from: https://clinicaltrials.gov/ct2/show/results/NCT02903836.
62. Grossman TH, Fyfe C, O’Brien W, et al. Fluorocycline TP-271 is potent against complicated community-acquired bacterial pneumonia pathogens. mSphere. 2017;2(1):e00004–17. doi:10.1128/mSphere.00004-17
63. A Phase 1 study to assess the safety, tolerability and PK of IV TP-271. ClinicalTrials.gov. Available from: https://clinicaltrials.gov/ct2/show/NCT02724085.
64. Tiffany CA, Hossain M, McDonald M, et al. Safety and pharmacokinetics of single escalating oral doses of GSK2140944, a novel bacterial topoisomerase inhibitor. Abstr 53rd Intersci Conf Antimicrob Agents Chemother. 2013;abstr F–1218.
65. Lemaire S, Kosowska-Shick K, Appelbaum PC, et al. Cellular pharmacodynamics of the novel biaryloxazolidinone radezolid: studies with infected phagocytic and nonphagocytic cells, using Staphylococcus aureus, Staphylococcus epidermidis, Listeria monocytogenes, and Legionella pneumophila. Antimicrob Agents Chemother. 2010;54:2549–2559. doi:10.1128/AAC.01724-09
66. Safety and efficacy study of oxazolidinone to treat pneumonia. ClinicalTrials.gov. Available from: https://clinicaltrials.gov/ct2/show/study/NCT00640926?cond=radezolid&draw=2&rank=1.
67. Pucci MJ, Bush K. Investigational antimicrobial agents of 2013. Clin Microbiol Rev. 2013;26:792–821. doi:10.1128/CMR.00033-13
68. Multiple ascending dose study for LCB01–0371. ClinicalTrials.gov. Available from: https://clinicaltrials.gov/ct2/show/NCT01842516.
69. Henry BD, Neill DR, Becker KA, et al. Engineered liposomes sequester bacterial exotoxins and protect from severe invasive infections in mice. Nat Biotechnol. 2015;33:81–88. doi:10.1038/nbt.3037
70. Laterre PF, Colin G, Dequin PF, et al. CAL02, a novel antitoxin liposomal agent, in severe pneumococcal pneumonia: a first-in-human, double-blind, placebo-controlled, randomised trial. Lancet Infect Dis. 2019;19:620–630. doi:10.1016/S1473-3099(18)30805-3
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.