")
Back to Journals » Psychology Research and Behavior Management » Volume 15
Investigation of the Negative Emotions Exhibited in Patients with Coronary Heart Disease After PCI and Any Influencing Factors
Authors Yang XL, Xie WY, Cai YM, Tang HY, Tao MY, Shen ZM, Chen HJ
Received 23 June 2022
Accepted for publication 6 October 2022
Published 17 October 2022 Volume 2022:15 Pages 3027—3037
DOI https://doi.org/10.2147/PRBM.S379422
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Igor Elman
Xiao-Li Yang,1,* Wen-Yao Xie,2,* Yi-Min Cai,3 Hong-Ying Tang,1 Mei-Yi Tao,3 Zhou-Min Shen,3 Hong-Jiao Chen4
1Department of Liver Surgery, Hunan Provincial People’s Hospital (The First Affiliated Hospital of Hunan Normal University), Changsha, 410005, People’s Republic of China; 2Interventional Operating Room, Hunan Provincial People’s Hospital (The First Affiliated Hospital of Hunan Normal University), Changsha, 410005, People’s Republic of China; 3Department of Nursing, Hunan Provincial People’s Hospital (The First Affiliated Hospital of Hunan Normal University), Changsha, 410005, People’s Republic of China; 4Medical College of Hunan Normal University, Changsha, 410013, People’s Republic of China
*These authors contributed equally to this study
Correspondence: Yi-Min Cai, Nursing department, Hunan Provincial People’s Hospital (The First Affiliated Hospital of Hunan Normal University), No. 61, Jiefang West Road, Changsha, 410005, People’s Republic of China, Tel +86 13787129085, Fax +0731-83928047, Email [email protected]
Purpose: To understand existing negative emotions in patients with coronary heart disease after percutaneous coronary stent implantation (PCI) and analyse its influencing factors.
Methods: Patients with coronary heart disease after PCI in three tertiary hospitals in Changsha City from April to September 2018 were selected as the research subjects. The self-designed general information questionnaire assessed irritability, depression and anxiety (IDA) on a self-rating scale. It was used to examine patients’ existing negative emotions with coronary heart disease after PCI and analyse the influencing factors.
Results: 203 questionnaires were distributed, and 202 valid questionnaires were recovered, with an effective recovery rate of 99.5%. The IDA score of patients with coronary heart disease after PCI was 17.01± 7.60 points, the incidence of negative emotions was 63.8%, and the incidences of depression, anxiety and irritability were 39.6%, 8.4% and 15.8%, respectively. Negative emotion was taken as the dependent variable and a patient’s general data, such as lifestyle and disease, as the independent variables. A univariate analysis was conducted to obtain gender, age, educational level, marital status, work status, per capita monthly household income, sleep status, etc. Seven factors were identified as the influencing factors of negative emotions in patients with coronary heart disease after PCI, and the difference was statistically significant (P< 0.05).
Conclusion: Most patients with coronary heart disease after PCI tend to exhibit negative emotions such as anxiety and depression. Medical staff should attach great importance to evaluating any negative feelings in this group and take timely targeted intervention measures to prevent and mitigate the occurrence and development of these adverse emotions in patients with coronary heart disease after PCI.
Keywords: coronary heart disease, postoperative PCI, negative emotions, influencing factors
Introduction
Coronary Atherosclerotic Heart Disease (CHD) refers to heart disease caused by myocardial ischemia, hypoxia or necrosis due to atherosclerosis of the coronary arteries, which narrows or blocks the vascular lumen and causes myocardial ischemia, hypoxia or necrosis. Coronary heart disease is also known as ischemic heart disease.1 With the advent of an aging society in my country, the prevention and control of chronic non-communicable diseases have become a primary focus of medical care, particularly cardiovascular diseases such as coronary heart disease.2–4 CHD is a disease with a high mortality rate and adversely impacts general health. The treatment of CHD reached a recent milestone with a new era of interventional therapy.5 PCI can quickly and effectively achieve vascular recanalization and relieve symptoms and has become a necessary treatment and rescue method for CHD blood flow reconstruction.6,7 It is considered one of the most important medical technology advances in the 20th century. However, PCI surgery is not the end point of CHD treatment since surgery can only relieve the mechanical stenosis of coronary arteries, which will only temporarily solve the most urgent symptoms in CHD patients. Therefore, the surgery is only a starting point,8 albeit one that improves patients’ chances of survival.9 In addition, patients often need to take a large number of drugs for a long time after surgery, which can be a heavy financial burden to the patients’ families and society.10 As a result, negative emotions such as anxiety and depression are common in patients with coronary heart disease after PCI, which adversely affects the recovery rate of patients after surgery.11
Anxiety and depression are common in hospitalised patients, and these symptoms are closely related to various factors such as the patient’s physiology, psychology and state of the disease. These are recognised risk factors for coronary heart disease12 and directly affect the prognosis of patients with coronary heart disease.13–15 Negative feelings such as anxiety and depression can exacerbate the body’s sympathetic nerve activity, leading to increased catecholamine secretion, disordered lipid metabolism, and release of angiotensin II, resulting in increased heart rates and blood pressure and decreased myocardial blood supply and oxygen supply. Increased oxygen consumption eventually leads to or aggravates the occurrence and development of various heart diseases such as hypertension, coronary heart disease and arrhythmia.16 However, according to epidemiological research, less than 20% of individuals with depression get adequate care.17 These rates were considerably lower in patients with cardiovascular disease. In a study of hospitalised patients with heart disease, only 11% of depressed individuals got sufficient antidepressant medication.18 Long-term outcomes and their relationship with competing risks have seldom been explored, and the distribution of anxiety and depression symptoms in patients with coronary heart disease have not been thoroughly defined. To further develop secondary preventive methods to enhance the quality of life of CHD patients and improve their long-term prognosis, it is essential to study depression and anxiety and the variables associated with these symptoms.
In this study, a questionnaire survey was used to understand the occurrence of negative emotions in patients after PCI. Additionally, the influencing factors of negative emotions were analysed from varying patient general data, such as lifestyle and disease level, to provide a basis for evaluating the psychological health status and treatment effects in postoperative patients.
Materials and Methods
Research Subjects
A random sampling method was used to select patients with coronary heart disease after PCI who were hospitalised in three tertiary hospitals in Changsha from April to September 2018. The inclusion criteria were patients: (1) aged >18; (2) in line with the clinical diagnostic criteria of the International Society of Cardiology and the World Health Organization (WHO), meaning they were diagnosed with coronary heart disease via coronary angiography and received PCI treatment, and in a stable condition; (3) gave informed consent and voluntarily participated. Those excluded had: (1) acute infection, severe liver and kidney insufficiency, severe congestive heart failure, severe cerebrovascular sequelae, malignant tumour, and critically ill or end-stage disease; (2) existing coronary heart disease, PCI patients who had received formal psychotherapy before, or had been previously diagnosed with anxiety or depression; (3) Cognitive dysfunction, unable to cooperate with the completion of the assessment. All selected participants signed informed consent, and the Ethics Committee approved our hospital study.
Research Methods
Random sampling was used to investigate 202 patients with coronary heart disease after PCI utilising a self-designed general information questionnaire measuring irritability, depression and anxiety on a self-rating scale. The available data questionnaire includes demographic data, lifestyle and disease-related questions. IDA is a self-rating scale proposed by Saith R. P. in 1978 to distinguish the irritability symptoms of patients suffering from depression and anxiety.19 In 2002, it was introduced to China by Yuan Yonggui20 and other scholars. The questionnaire’s content has proved to be reliable, valid and consistent. Our results show that the scale’s test-retest correlation coefficient ranges from 0.488 to 0.761, and the homogeneity reliability Cronbach’s coefficient is from 0.419 to 0.769. The scale has 18 items corresponding to four choices on depression, anxiety, introverted irritability and extroverted irritability. Each object corresponds to a related symptom and is scored on a scale of 0 to 3, of which 1, 2, 5, 12, 13 and 17 are positive scores. The twelve items 3, 4, 6, 7, 8, 9, 10, 11, 14, 15, 16 and 18 are reverse scoring. Depression and introverted irritability scores are classified as normal if <4, borderline when ranging from 4–6 and abnormal if >6; anxiety scoring <6 is normal, borderline if 6–8 and abnormal when >8; extroverted irritation is classified as normal with a score of <5, borderline state when 5–7 and abnormal if >7.
Statistical Processing
SPSS version 20.0 statistical software (IBM Corp., CA, USA) was used for data analysis and a two-tailed P-value of less than 0.05 was considered statistically significant. The categorical data were described as counts (frequency) and the numerical data were expressed as mean ± standard deviations. After the Kolmogorov–Smirnov analysis, all numerical data were in line with normal distribution. The Student’s t-test or one-way variance analysis (ANOVA) was used to detect the differences between two or multiple independent groups. Univariate analysis was used to analyse the influencing factors of negative emotions in patients with coronary heart disease after PCI.
Results
The recovery rate was 99.5%, as 203 questionnaires were distributed in this study and 202 of those returned were valid. General information included three prominent parts: demographic data, lifestyle and disease-related data (Table 1–3). Most of the included population were male (69.8%) and 62.9% of the patients were over 60.
 |
Table 1 Distribution of General Demographic Characteristics of Patients with Coronary Heart Disease After PCI (n=202, %) |
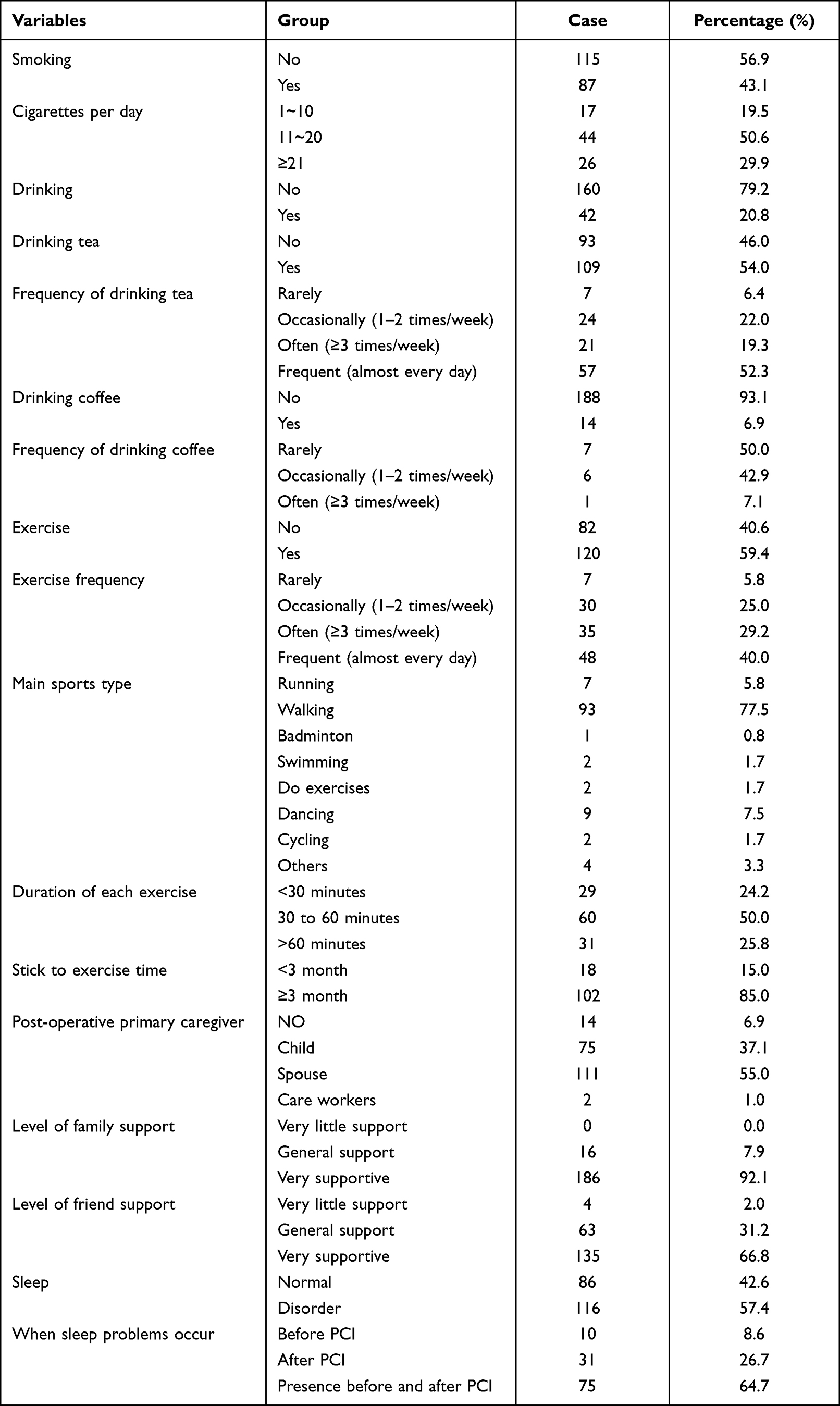 |
Table 2 Lifestyle Data of Patients with Coronary Heart Disease After PCI (n=202, %) |
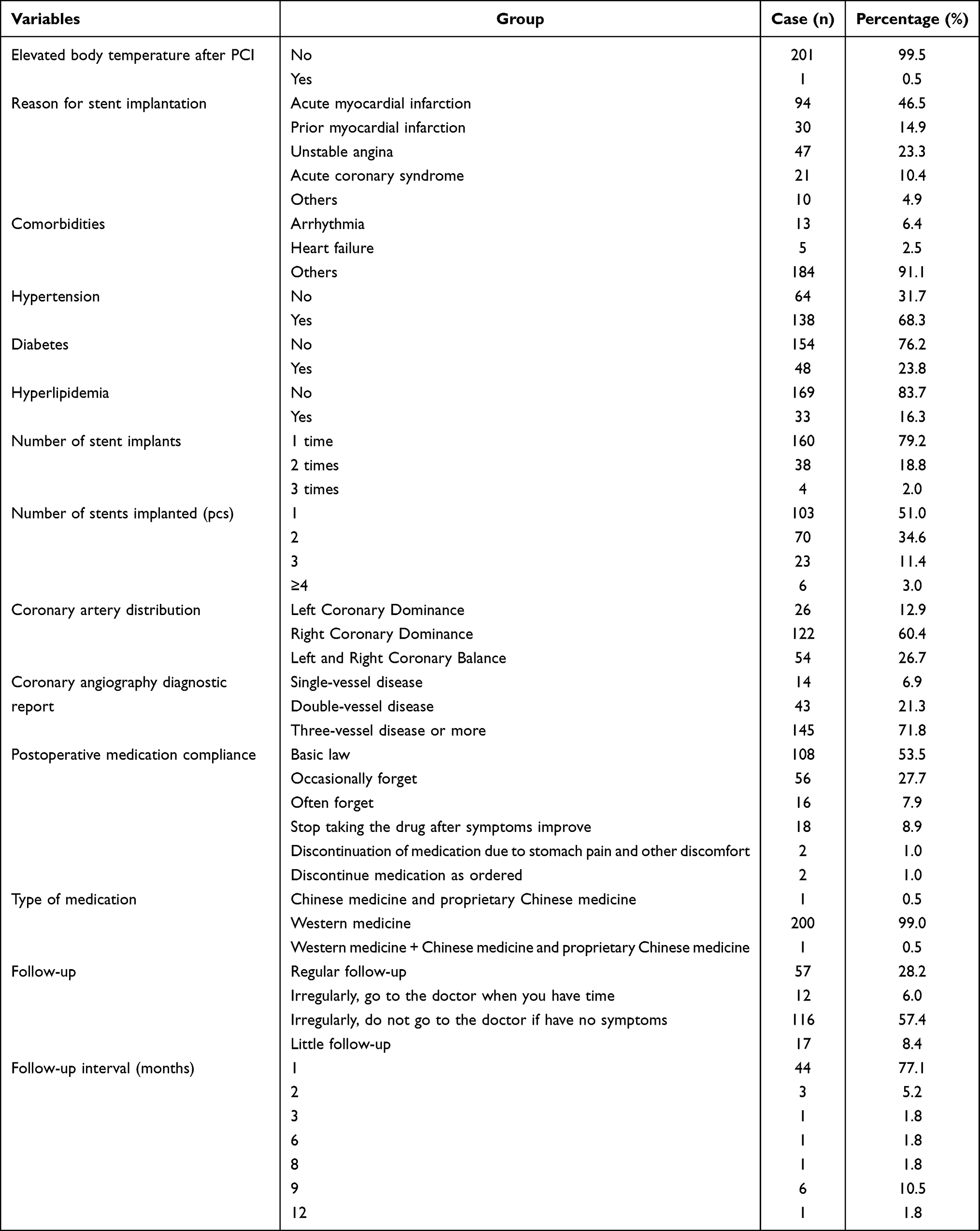 |
Table 3 Disease Data of Patients with Coronary Heart Disease After PCI (n=202, %) |
Overall Negative Emotion Scores
As shown in Table 4, the negative emotion, anxiety, depression, introverted irritability and extroverted irritability scores were 17.01±7.60, 6.08±2.92, 4.57±2.73, 2.51±2.20 and 3.86±2.28, respectively. The incidences of anxiety, depression and abnormal irritability in patients with coronary heart disease after PCI were 8.4%, 39.6% and 15.8%, respectively. The univariate analysis found that among patients’ general data on lifestyle and disease, seven factors were associated with a negative emotion score after PCI in patients with coronary heart disease (P<0.05 for all).
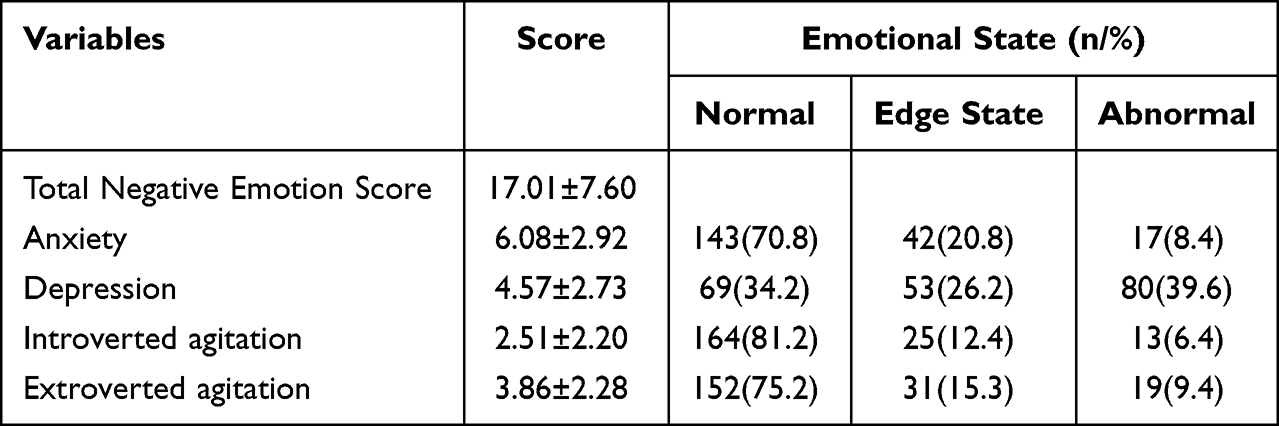 |
Table 4 Negative Emotional Status of Patients with Coronary Heart Disease After PCI (n=202, %) |
Gender Effect on Negative Emotion Scores
As shown in Table 5, male patients had significantly lower anxiety (4.13±2.64 vs 5.57±2.70, P=0.001) and IDA total score (16.19±7.73 vs 18.92±6.70, P=0.015) than female patients. However, the two sexes had no significant differences in depression and introverted and extroverted agitation.
 |
Table 5 Comparison of Negative Emotion Scores in Patients with Coronary Heart Disease After PCI in Different Genders ( |

Age Effect on Negative Emotion Scores
As shown in Table 6, those ≥60 had significantly higher depression scores than the <60 group (6.45±3.10 vs 5.45±2.52, P=0.019). There were no significant differences in other dimensions, such as anxiety, introverted and extroverted agitation, or IDA total score between these groups.
 |
Table 6 Comparison of Negative Emotion Scores in Patients with Coronary Heart Disease After PCI at Different Ages ( |

Effect of Education Level on Negative Emotion Scores
As shown in Table 7, compared with other groups, illiterate patients with coronary heart disease after PCI had the highest scores in depression (8.42±2.84), anxiety (6.42±3.12), introverted irritability (3.83±2.12) and overall IDA score (22.50±7.51), all with statistically significant differences (P<0.05).
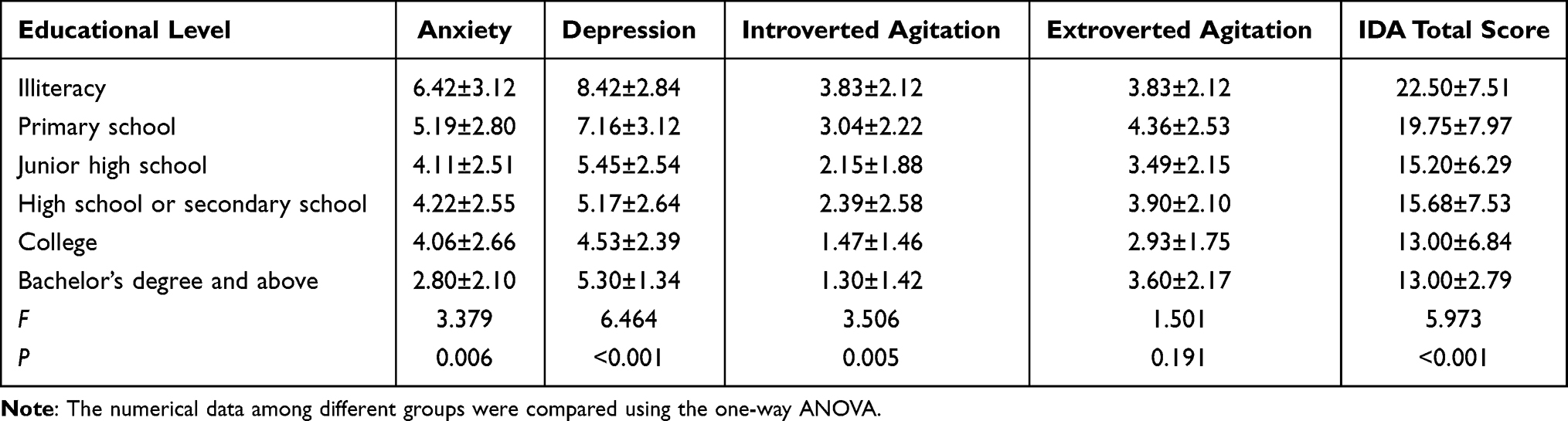 |
Table 7 Comparison of Negative Emotion Scores in Patients with Different Educational Levels of Coronary Heart Disease After PCI ( |

Marital Status Effect on Negative Emotion Scores
As shown in Table 8, the depression (5.89±2.74 vs 7.25±3.73, P=0.022), introverted irritability dimension (2.36±2.19 vs 3.46±2.01, P=0.013), and overall IDA score (16.56±7.51 vs 19.86±7.69, P=0.033) of married patients were lower than those listed as “other”.
 |
Table 8 Comparison of Negative Emotion Scores in Patients with Coronary Heart Disease After PCI with Different Marital Status ( |

Effect of Employment Status on Negative Emotion Scores
As shown in Table 9, the unemployed patients had higher anxiety (4.85±2.78 vs 3.95±2.53, P=0.025) and overall IDA scores (17.78±7.83 vs 15.32±6.82, P=0.032) than those that were employed.
 |
Table 9 Comparison of Negative Emotion Scores in Patients with Coronary Heart Disease After PCI in Different Working States ( |

Effect of Income Level on Negative Emotion Scores
As shown in Table 10, the group with ≤1000 tuples had the highest negative scores, including depression (7.03±2.98), introverted irritability (3.56±2.22), and the overall IDA score (20.53±6.70) with statistically significant differences (P<0.05 for all).
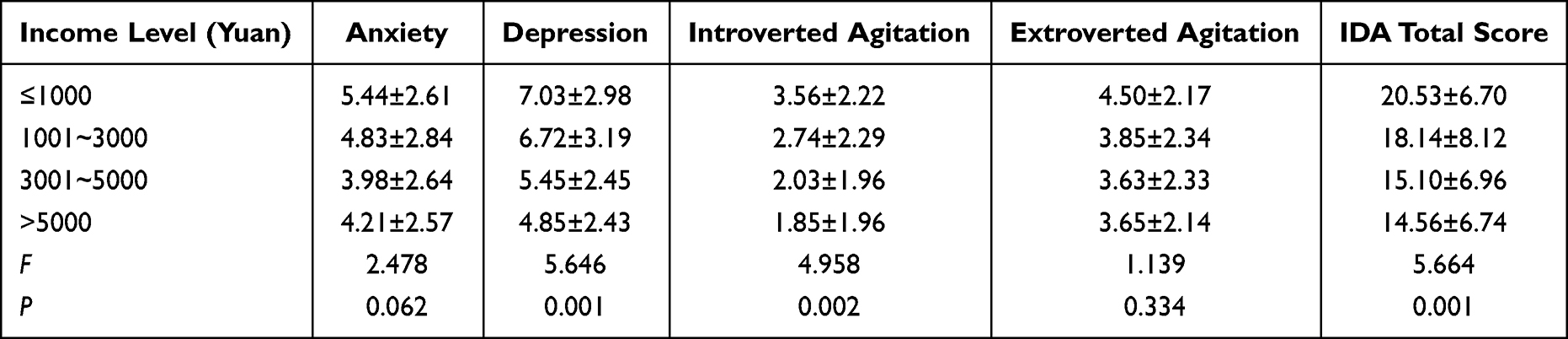 |
Table 10 Comparison of Negative Emotion Scores of Patients with Coronary Heart Disease After PCI with per Capita Monthly Income of Different Families ( |

Effect of Sleep States on Negative Emotion Scores
As shown in Table 11, those patients with a sleep disorder had significantly higher scores of depression (7.22±2.88 vs 4.55±2.20, P<0.001), anxiety (5.42±2.70 vs 3.42±2.34, P<0.001), introverted irritability (2.86±2.20 vs 2.03±2.11, P=0.007), and overall IDA score (19.40±7.49 vs 13.79±6.51, P<0.001) than those with normal sleep.
 |
Table 11 Comparison of Negative Emotion Scores in Patients with Coronary Heart Disease After PCI in Different Sleep States ( |

Discussion
In this cross-sectional study, we explored the occurrence and influencing factors of negative emotions in patients with coronary artery disease after PCI. The main findings can be summarised as follows: 1) patients with coronary heart disease after PCI often exhibited negative emotions such as anxiety and depression; 2) gender, age, educational level, marital status, work status, per capita monthly household income and sleep status can be associated with these negative emotions. Therefore, more efforts should be paid to evaluating negative emotions in high-risk groups and early prevention strategies in patients with coronary heart disease after PCI.
Current Situation of Negative Emotions in Patients with Coronary Heart Disease After PCI
This study showed that the incidence of negative emotions in patients with coronary heart disease after PCI was 63.8%, and depression, anxiety and irritability were 8.4%, 39.6% and 15.8%, respectively. Studies have reported that the incidence of anxiety in patients after PCI ranges from 25% to 37%,21 while depression can reach 67%.22 In our survey, 1461 people were selected as the research subjects, and follow-up times were controlled for 7 to 9 years. It was found that the mortality rate of patients with coronary heart disease and depression was significantly higher than that of patients with simple coronary heart disease, at an increased rate of 80%. At the same time, the more pronounced the depressive symptoms were in patients, the greater their risk of adverse cardiovascular events of coronary heart disease.23 The low incidence of depression in this study may be attributed to the small sample size of this study. CHD is a chronic disease; if long-term chronic stress is not relieved or reduced over time, it will inevitably lead to anxiety and tension. Studies have shown24 that the serum inflammatory marker IL-6 in patients with depression after PCI was uncommonly high, and the magnitude of the increase was positively correlated with the severity of depression. Therefore, anxiety, depression and coronary heart disease PCI are causal and mutually reinforcing, which is not conducive to the recovery of patients’ health.
Influencing Factors of Negative Emotions in Patients with Coronary Heart Disease After PCI
This study showed that the negative emotions of patients with coronary heart disease after PCI significantly differed in the following seven aspects (P<0.05).
Gender
The anxiety dimension score of female patients was (5.57±2.70) points, and the total IDA score was (18.92±6.70) points, which were higher than those of male patients, indicating that female patients with coronary heart disease after PCI were more likely to have anxiety symptoms than male patients. A study by some scholars found that the proportion of anxiety, depression and anxiety with depression in female patients with coronary heart disease after PCI was higher than that in males, and the difference was statistically significant (P<0.05).25 In a population at one month after myocardial infarction, compared with men, women were at higher risk for anxiety or depression and the severity of depression increased with age in men. In contrast, the severity of anxiety decreased.26 These are consistent with the findings of this study. This phenomenon may result from the fact that women are more vulnerable physically and psychologically and have more sensitive, volatile emotions than men.27,28 Gonadal hormones may be the prominent factor in this difference. Women are more likely to experience mood disorders during hormonal flow, and testosterone may have a protective effect against anxiety and depression.29 Therefore, personalised treatment should target the pathogenesis of negative emotions in patients undergoing revascularization.
Age
People over 60 had a higher depression score (6.45±3.10) points, while those under 60 scored lower (5.45±2.52). The results showed that with increasing age, patients with coronary heart disease after PCI were more likely to have depression. The reason may be that health declines with age and the inevitable increase in chronic diseases. These diseases are prone to recur due to the long course of the disease and require long-term drug maintenance. In addition, a decreased sense of self-worth is common with psychological changes such as scepticism, withdrawal, anxiety and depression.30,31
Educational Level
The results of this study showed that illiterate CHD patients had the highest scores in depression, anxiety, introverted irritability dimensions, and overall IDA score after PCI, which shows that patients with lower educational levels are more likely to have depression and anxiety. The reason may be that different levels of education manifest in differing viewpoints and cognition levels from the same disease. Patients with coronary heart disease after PCI with higher education levels often understand and learn more about their condition, treatment, and prognosis through mobile phones, computers and various apps, while having a confident psychological grasp of the disease. However, patients with low education levels often have inadequate disease-related knowledge and retain an elevated sense of uncertainty about the condition. This means they are more likely to have harmful psychological effects, such as stress and depression.32,33
Marital Status
The results of this study showed that CHD patients with other marital identifications (including single, divorced and widowed) were more likely to have negative emotions after PCI than married patients with a spouse. The reasons may be that, on the one hand, when a patient with a spouse is facing the pressure of the disease, they can seek help or comfort from their partners or get help. From a psychological point of view, they have strong emotional support. Conversely, unmarried, divorced or widowed patients may suffer mental health discrimination from others or psychological traumas. When they experience additional pressure from a disease recurrence, their psychological endurance is often close to a breaking point, which may be difficult to endure and thus prone to extremely negative emotions.34,35
Working Status
Unemployed patients with coronary heart disease after PCI are more likely to have anxiety than working patients. The reasons may be that working can ease the financial pressures on the family while acting as a distraction to a patient from their pain. Additionally, at work, patients can communicate with colleagues and share their thoughts, which can be a release for negative emotions. Therefore, work may play a particular role in promoting the improvement of negative emotions in patients with coronary heart disease after PCI.36
Sleep Status
Patients with poor sleep quality after coronary heart disease PCI are more prone to depression and anxiety than patients with normal sleep. The reason may be that lack of sleep or sleep disorders in patients can lead to the lack of regular rest for the brain, and changes in hormone levels, making patients’ emotions harder to regulate and resulting in anxiety and depression.37,38
Limitations
This study has certain limitations. First, the sample size included in this study was relatively small, and we plan to increase the sample size in future studies. Secondly, there has been no follow-up on the prognosis of patients with negative emotions, and no definite conclusions can be drawn about the impact. In addition, we only provided an overview of the current situation and potential influencing factors of negative emotions in patients undergoing PCI due to a cross-sectional design. Further longitudinal studies are thus warranted to reveal any possible associations between negative emotions and other socio-economic factors in multicentre, large cohorts.
Conclusion
In conclusion, the results of this study showed that the negative emotions of patients with coronary heart disease after PCI were at moderate to severe levels. Seven factors, including gender, age, education level, marital status, work status, family monthly income and sleep status were the primary influencing factors of negative emotions in patients with coronary heart disease after PCI. Healthcare workers should take a series of interventions, including death education, cognitive behavioural education, collaborative nursing, health education, stress counselling and support, to help caregivers aid patients more effectively.
Ethics Approval and Consent to Participate
This study was conducted in accordance with the Declaration of Helsinki and approved by the Medical Ethics Committee of Hunan People’s Hospital, (Protocol number: No.70). We obtained signed informed consent from the participants in this study.
Funding
1.Natural Science Foundation of Hunan Province: Research on Sleep Quality, Influencing Factors and Comprehensive Intervention Nursing of Inpatients (Project No. 2018JJ2227);
2.2022 Hunan Provincial Health Commission Project: Research on the Main Caregiver Burden, Influencing Factors and Comprehensive Intervention Nursing of Inpatients with Liver Cancer (Project No. 202214023133).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Giannini J, Padilla J, Eaton RP, Gonzales K, Schade DS. Prevention of coronary heart disease: a translational clinical challenge. World J Cardiovasc Dis. 2022;12(1):13. doi:10.4236/wjcd.2022.121002
2. Costa VL, Ruidavets JB, Bongard V, et al. Prediction of coronary heart disease incidence in a general male population by circulating non-coding small RNA sRNY1-5p in a nested case-control study. Sci Rep. 2021;11(1):1837. doi:10.1038/s41598-021-81221-8
3. Qiu X, Wang J, Shi Z, et al. Predictive value of miRNA-126 on in-stent restenosis in patients with coronary heart disease: a protocol for meta-analysis and bioinformatics analysis. Medicine. 2021;100(22):e25887. doi:10.1097/MD.0000000000025887
4. Martikainen P, Korhonen K, Jelenkovic A, et al. Joint association between education and polygenic risk score for incident coronary heart disease events: a longitudinal population-based study of 26 203 men and women. J Epidemiol Community Health. 2021;1:214358. doi:10.1136/jech-2020-214358
5. Giovanni V, Hugh TP, Ferrario MM, et al. Combined effect of educational status and cardiovascular risk factors on the incidence of coronary heart disease and stroke in European cohorts: implications for prevention. Eur J Prev Cardiol. 2020;4(4):152.
6. Percutaneous coronary intervention in octogenarians. 10-year experience from a primary percutaneous coronary intervention centre with off-site cardiothoracic support. J Geriatric Cardiol. 2022;19(3):189–197. doi:10.11909/j.issn.1671-5411.2022.03.010
7. Walters D, Mahmud E. Thrombolytic Therapy for ST-Elevation Myocardial Infarction Presenting to non-Percutaneous Coronary Intervention Centers During the COVID-19 Crisis. Curr Cardiol Rep. 2021;23(10):152. doi:10.1007/s11886-021-01576-2
8. Looser PM, Kim LK, Feldman DN. In-stent restenosis: pathophysiology and treatment. Curr Treat Options Cardio Med. 2016;18(2):10. doi:10.1007/s11936-015-0433-7
9. Li Y, Liang X, Zhang W, et al. The clinical and angiographic outcomes of postdilation after percutaneous coronary intervention in patients with acute coronary syndrome: a systematic review and meta-analysis. J Interv Cardiol. 2021;2021:6699812. doi:10.1155/2021/6699812
10. Huang X, Li Q, Hao Y, et al. Study on the effect of continuous nursing after coronary heart disease intervention in elderly patients. China Circulation Journal. 2017;32(Supplement 1):231–232.
11. De Smedt D, Clays E, Annemans L, et al. Self-reported health status in coronary heart disease patients: a comparison with the general population. Eur J Cardiovasc Nurs. 2015;14(2):117–125. doi:10.1177/1474515113519930
12. Van der Kooy K, van Hout H, Marwijk H, et al. Depression and the risk for cardiovascular diseases: systematic review and meta analysis. Int J Geriatr Psychiatry. 2007;22(7):613–626. doi:10.1002/gps.1723
13. Kuhlmann SL, Arolt V, Haverkamp W, et al. Prevalence, 12-Month Prognosis, and Clinical Management Need of Depression in Coronary Heart Disease Patients: a Prospective Cohort Study. Psychother Psychosom. 2019;88(5):300–311. doi:10.1159/000501502
14. Watkins LL, Koch GG, Sherwood A, et al. Association of anxiety and depression with all-cause mortality in individuals with coronary heart disease. J Am Heart Assoc. 2013;2(2):e000068. doi:10.1161/JAHA.112.000068
15. Moser DK, McKinley S, Riegel B, et al. Relationship of persistent symptoms of anxiety to morbidity and mortality outcomes in patients with coronary heart disease. Psychosom Med. 2011;73(9):803–809. doi:10.1097/PSY.0b013e3182364992
16. Hao R, Li Y, Xu Y, et al. Study on the development and application effect of an intelligent negative emotion improvement program for patients with coronary heart disease. Chine J Nursing. 2021;56(9):1285–1292.
17. Kessler RC, Berglund P, Demler O, et al. The epidemiology of major depressive disorder: results from the National Comorbidity Survey Replication (NCS-R). JAMA. 2003;289(23):3095–3105. doi:10.1001/jama.289.23.3095
18. Huffman JC, Smith FA, Blais MA, Beiser ME, Januzzi JL, Fricchione GL. Recognition and treatment of depression and anxiety in patients with acute myocardial infarction. Am J Cardiol. 2006;98(3):319–324. doi:10.1016/j.amjcard.2006.02.033
19. Snaith R, Taylor C. Irritability: definition, Assessment and Associated Factors. Br J Psychiatry. 1985;147(2):127–136. doi:10.1192/bjp.147.2.127
20. Yuan Y, Shen X, Wu A, et al. The reliability and validity of irritability, depression and anxiety scale. Sichuan Mental Health. 2002;15(1):11–13.
21. Trotter R, Gallagher R, Donoghue J. Anxiety in patients undergoing percutaneous coronary interventions. Heart Lung. 2011;40(3):185–192. doi:10.1016/j.hrtlng.2010.05.054
22. Furuya RK, Costa Ede C, Coelho M, et al. Ansiedade e depressão entre homens e mulheres submetidos à intervenção coronária percutânea [Anxiety and depression among men and women who underwent percutaneous coronary intervention]. Rev Esc Enferm USP. 2013;47(6):1333–1337. doi:10.1590/S0080-623420130000600012 Portuguese.
23. Wang Z, Wang W, Zhou J, et al. Depressive State of Patients With Coronary Artery Disease and Its Influence on Prognosis. Chine General Practice. 2015;18(26):3148–3152.
24. Liang Y. Discussion on psychological nursing of patients with coronary heart disease interventional therapy. Chine Remedies Clin. 2016;16(9):1379–1381.
25. Li J. Multivariate Correlation Analysis of Insomnia, Anxiety, Depression and TCM Constitution in Patients After PCI. Lanzhou University; 2018.
26. Serpytis P, Navickas P, Lukaviciute L, et al. Gender-based differences in anxiety and depression following acute myocardial infarction. Arq Bras Cardiol. 2018;111(5):676–683. doi:10.5935/abc.20180161
27. Seney ML, Sibille E. Sex differences in mood disorders: perspectives from humans and rodent models. Biol Sex Differ. 2014;5(1):17. doi:10.1186/s13293-014-0017-3
28. Altemus M, Sarvaiya N, Neill Epperson C. Sex differences in anxiety and depression clinical perspectives. Front Neuroendocrinol. 2014;35(3):320–330. doi:10.1016/j.yfrne.2014.05.004
29. McHenry J, Carrier N, Hull E, Kabbaj M. Sex differences in anxiety and depression: role of testosterone. Front Neuroendocrinol. 2014;35(1):42–57. doi:10.1016/j.yfrne.2013.09.001
30. Luttik ML, Jaarsma T, Sanderman R, et al. The advisory brought to practice: routine screening on depression (and anxiety) in coronary heart disease; consequences and implications. Eur J Cardiovasc Nurs. 2011;10(4):228–233. doi:10.1016/j.ejcnurse.2010.08.005
31. Tully PJ, Newland RF, Baker RA. Cardiovascular risk profile before coronary artery bypass graft surgery in relation to depression and anxiety disorders: an age and sex propensity matched study. Aust Crit Care. 2015;28(1):24–30. doi:10.1016/j.aucc.2014.04.006
32. Lv J. Relevant Research of Depression and Anxiety of Young and Middle-Aged Coronary Heart Disease Patients After Stent Implantation. Army Medical University; 2015.
33. Cekirdekci EI, Bugan B. Level of Anxiety and Depression in Cardiac Syndrome X. Med Princ Pract. 2019;28(1):82–86. doi:10.1159/000495109
34. Albus C. Psychological and social factors in coronary heart disease. Ann Med. 2010;42(7):487–494. doi:10.3109/07853890.2010.515605
35. Shen N. Study on the Relationship Between Cognition of Chronic Diseases, Negative Emotions and Coping Styles Among the Urban Elderly [D]. East China Normal University; 2011.
36. Lorant V, Deliège D, Eaton W, et al. Socioeconomic inequalities in depression: a meta-analysis. Am J Epidemiol. 2003;157(2):98–112. doi:10.1093/aje/kwf182
37. Weiss A, Sutin AR, Duberstein PR, et al. The personality domains and styles of the five-factor model are related to incident depression in Medicare recipients aged 65 to 100. Am J Geriatr Psychiatry. 2009;17(7):591–601. doi:10.1097/jgp.0b013e31819d859d
38. Baglioni C, Nanovska S, Regen W, et al. Sleep and mental disorders: a meta-analysis of polysomnographic research. Psychol Bull. 2016;142(9):969–990. doi:10.1037/bul0000053
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.