")
Back to Journals » Neuropsychiatric Disease and Treatment » Volume 12
Investigation of facial emotion recognition, alexithymia, and levels of anxiety and depression in patients with somatic symptoms and related disorders
Authors Ozturk A , Kilic A, Deveci E , Kirpinar I
Received 23 February 2016
Accepted for publication 31 March 2016
Published 29 April 2016 Volume 2016:12 Pages 1047—1053
DOI https://doi.org/10.2147/NDT.S106989
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Roger Pinder
Ahmet Öztürk, Alperen Kiliç, Erdem Deveci, İsmet Kirpinar
Department of Psychiatry, Faculty of Medicine, Bezmialem Vakif University, Istanbul, Turkey
Background: The concept of facial emotion recognition is well established in various neuropsychiatric disorders. Although emotional disturbances are strongly associated with somatoform disorders, there are a restricted number of studies that have investigated facial emotion recognition in somatoform disorders. Furthermore, there have been no studies that have regarded this issue using the new diagnostic criteria for somatoform disorders as somatic symptoms and related disorders (SSD). In this study, we aimed to compare the factors of facial emotion recognition between patients with SSD and age- and sex-matched healthy controls (HC) and to retest and investigate the factors of facial emotion recognition using the new criteria for SSD.
Patients and methods: After applying the inclusion and exclusion criteria, 54 patients who were diagnosed with SSD according to the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-5) criteria and 46 age- and sex-matched HC were selected to participate in the present study. Facial emotion recognition, alexithymia, and the status of anxiety and depression were compared between the groups.
Results: Patients with SSD had significantly decreased scores of facial emotion for fear faces, disgust faces, and neutral faces compared with age- and sex-matched HC (t=-2.88, P=0.005; t=-2.86, P=0.005; and t=-2.56, P=0.009, respectively). After eliminating the effects of alexithymia and depressive and anxious states, the groups were found to be similar in terms of their responses to facial emotion and mean reaction time to facial emotions.
Discussion: Although there have been limited numbers of studies that have examined the recognition of facial emotion in patients with somatoform disorders, our study is the first to investigate facial recognition in patients with SSD diagnosed according to the DSM-5 criteria. Recognition of facial emotion was found to be disturbed in patients with SSD. However, our findings suggest that disturbances in facial recognition were significantly associated with alexithymia and the status of depression and anxiety, which is consistent with the previous studies. Further studies are needed to highlight the associations between facial emotion recognition and SSD.
Keywords: emotion, somatization, facial, recognition
Introduction
Somatic symptoms are one of the most common causes of doctor visits. These symptoms are so common that ~80% of the population reports somatic symptoms within a 7-day period.1 When these symptoms cannot be explained by traditional or advanced medical tools, they can cause comorbid psychiatric disorders and disrupt the patient’s quality of life.2 Thus, the psychiatric associations of these somatic symptoms are quite important.
The etiology of somatoform disorders remains unclear. However, the etiology includes a complicated and vicious cycle among physiological disturbances, increased attention devoted to the body, increased perception of illness-related symptoms, concerns of illness, expression of distress, avoidance, disability, and changes in social interactions. This complicated and vicious cycle also involves factors related to emotion and arousal in addition to the abovementioned factors.3,4 Additionally, unconscious conflicts present as somatic symptoms according to the psychodynamic explanation. Regarding the vicious cycle of emotional arousal in somatoform disorders, it is thought that the emotional disturbances can cause impairments in interpersonal and social interactions. Thus, the vulnerability resulting from these disturbed emotional interactions may cause stressful events.5,6
The concept of facial emotion recognition indicates that human beings generally react and communicate with emotional expressions, especially emotional facial expressions. Thus, it is well established that facial emotion recognition has an important place in emotion regulation, interpersonal communication skills, and in the development of psychopathologies. Thus, there has been a great interest in the field of neuropsychiatry, and there have been numerous studies that investigated the relationship between facial emotion recognition and psychiatric disorders.7 In literature, there have been two studies that compared facial emotional expressions between patients with somatoform disorder and healthy controls (HC). One of these studies reported significant differences between patients with somatoform disorder and healthy subjects; however, the authors reported that the differences in facial emotion recognition were a result of alexithymia.8 The other study reported a reduced performance in the recognition of neutral and sad emotional expressions, even if confounding factors such as alexithymia and levels of anxiety and depression were taken into account in the comparisons.9 Besides the abovementioned studies, there was one study conducted that compared facial emotion recognition between HC and patients with somatoform pain disorder, but no significant differences were reported between the groups.10
The diagnostic criteria for somatoform disorders11 were changed considerably in the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-5), and the disorder name was also changed to somatic symptoms and related disorders (SSD).12 In the present study, we aimed to investigate and retest the facial emotional expressions in this new diagnostic criteria and then compare them between patients with age- and sex-matched HC. We also hypothesized that there would be a discrepancy associated with the new diagnostic criteria in terms of facial emotion recognition.
Patients and methods
The present study was conducted in Faculty of Medicine, Bezmialem Vakif University, between June 2015 and January 2016. The patients who were diagnosed with SSD according to the DSM-5 criteria were included in the present study.12 The diagnosis was made by two senior psychiatrists according to the DSM-5 criteria for SSD. An interrater reliability analysis using the kappa statistic was performed to determine the consistency between the two senior psychiatrists. The interrater reliability for the raters was κ=0.88 (P<0.001). The inclusion criteria for the participants were as follows: diagnosed with SSD, age between 18 years and 65 years, and willing to participate in the study. The exclusion criteria were as follows: older than 65 years and younger than 18 years, diagnosed with other psychiatric disorders and undergoing follow-up for any psychiatric disorder, treated with any psychotropic agent, educated <5 years, diagnosed with mental retardation, taking any drug that affects attention or cognition, diagnosed with any medical illness, addicted to alcohol or other illicit drugs, or unwilling to participate in the present study. Initially, 72 patients with the diagnosis of SSD were examined; ten patients were excluded because of a comorbid psychiatric disorder, five patients were excluded because of a comorbid medical illness, and three patients were excluded because they chose not to participate in the study after receiving an explanation of the procedure. No patient was excluded because of sex or age criteria. The patients who were excluded from the study had sociodemographic properties similar to those of the included patients. After meeting the exclusion and inclusion criteria, 54 patients were included in the present study. According to the exclusion criteria, 46 age- and sex-matched HC participated in the study. All the patients had sufficient mental capacity to understand the aim of the study and provided written informed consent. The ethics committee of Bezmialem Vakif University approved the study.
Instruments
Sociodemographic and clinical form
This form included data regarding age, sex, marital status, education status, and the subdiagnosis of SSD.
Beck Depression Inventory
The Beck Depression Inventory (BDI) is a self-reported scale that assesses the presence and severity of depression. It has 21 items scored with a 4-point Likert scale ranging between 0 and 3. The BDI cutoffs were as follows: <10, absence or minimal depression; 10–18, mild to moderate depression; 19–29, moderate to severe depression; and 30–63, severe depression. The BDI was created by Beck13 and was validated into Turkish language by Hisli.14
Beck Anxiety Inventory
This scale is used to assess the level of anxiety in clinical practice. It is a self-reported scale that ranges between 0 and 63. The higher scores of the Beck Anxiety Inventory (BAI) refer to higher levels of anxiety. It was created by Beck et al.15 The Turkish form was reported to be reliable and validated by Ulusoy et al.16
Toronto Alexithymia Scale
The Toronto Alexithymia Scale (TAS) is a self-reported scale that is used for assessing alexithymia. It consists of 20 items, with scores from one to five, with the total score range between 20 and 100. The three subscores of the TAS are as follows: difficulties in identifying feelings (TAS1), difficulties in describing feelings (TAS2), and externally oriented thinking (TAS3). The reliability and validity of the TAS were previously shown.17,18
Emotion Recognition Test
This tool is a computer-based test that consists of four male and four female models that have expressions of happy, surprised, fearful, sad, angry, disgusted, and neutral images from the Ekman and Friesen’s series.19 These photo images of faces were digitized on a computer presentation via an SQL data application in a Visual Basic NET software program that was created for portable computers (2.4 GHz and 3 MB processor, 3 GB main memory, 15.6-inch LCD screen with 1,366×768 pixel resolution). Initially, there was a trial for each participant in which seven photo images that included each emotional expression were presented. In this trial, the order of the seven faces with different emotional expressions was shown for each participant. After the trial, 49 photos that were in a permuted order were used for the assessment, and each expression was represented in an equal number of images.
While the participant viewed the photo, he or she selected one of the seven boxes that included one of the written emotions. Participants were asked to choose the selection according to the emotion when they saw the image on the screen. The instructions were given to all the participants, and they were asked whether they were ready for the test. After they noted that they were ready for the assessment, the test was conducted in a quiet room without tools that could disturb them.
Statistical analysis
All data were assessed using the Statistical Package for the Social Sciences, PC Version 17.0 (SPSS Inc., Chicago, IL, USA). A confidence interval of 95% and a two-tailed P-value <0.05 were determined to be statistically significant for all the analyses. The numerical data were analyzed using the Shapiro–Wilk test to determine whether the data were parametric. The numeric data were compared between the groups using Student’s t-test, and if appropriate, the Mann–Whitney U-test and Kruskal–Wallis test were used. After the first comparison, a general linear model was constructed. In this model, the scores of facial emotion recognition were noted as the dependent variable, group was included as a fixed factor, and the first BAI, BDI, and TAS scores were included as covariants. The Bonferroni test was used to compare the scores of facial emotion recognition in this model. In this model, Bonferroni correction was used to overcome the cumulative alpha error, and the P-value was noted as P<0.007. All the numerical data were expressed as mean ± SD. The differences in categorical variables were assessed using the χ2 test and expressed as numbers and percentages.
Results
The SSD group consisted of 28 patients with SSD, 19 patients with conversion disorder, three patients with illness anxiety disorder, one patient with other SSD, and three patients with unspecified SSD. The mean ages were 38.37±10.45 years in the patient group and 37.17±10.68 years in the control group. The groups were similar in terms of age (t=0.56, P=0.57). There were 41 females and 13 males in the patient group and 36 females and ten males in the control group. The sex distribution was similar between groups (χ2=0.76, P=0.48). The marital status and educational status were similar between groups (P>0.05). The median BDI scores in the patient and control groups were 19 (min =3; max =41) and 5 (min =0; max =40), respectively. The median BAI values in the patient and control groups were 23 (min =3; max =54) and 4.5 (min =0; max =28), respectively. The BDI and BAI scores were significantly higher in the patient group compared with the control group (Z=−6.30, P<0.001; Z=−7.16, P<0.001, respectively). The median TAS1, TAS2, and TAS3 scores were, respectively, 20.5 (min =7; max =33), 14 (min =5; max =25), and 21 (min =11; max =21) in the patient group, whereas these values were 10 (min =7; max =23), 11.5 (min =6; max =20), and 20 (min =10; max =28) in the control group. The TAS1 and TAS2 scores were significantly higher in the patient group (Z=−6.83, P<0.001; Z=−3.36, P=0.001, respectively). The TAS3 score was similar between groups (Z=−1.74, P=0.08; Table 1).
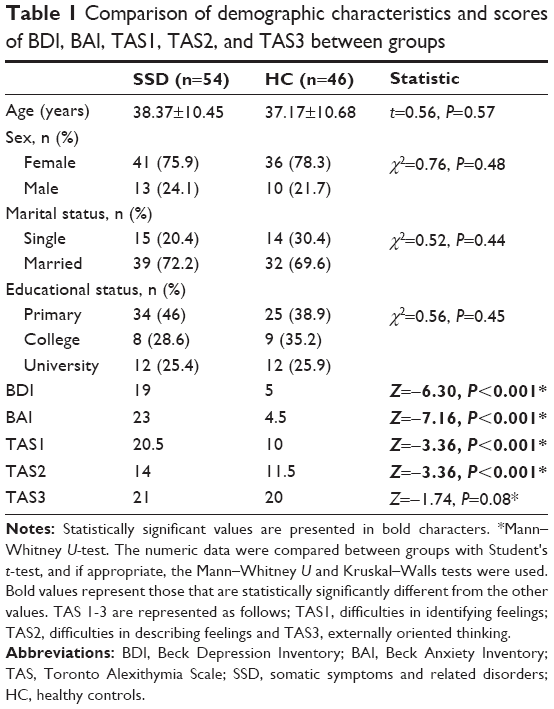 | Table 1 Comparison of demographic characteristics and scores of BDI, BAI, TAS1, TAS2, and TAS3 between groups |
The mean scores for responses to each facial emotion in the patient group were as follows: happy faces =6.83±0.54, sad faces =5.16±1.30, fear faces =3.18±0.69, disgust faces =4.84±1.51, angry faces =5.87±1.15, surprised faces =5.29±1.32, and neutral faces =5.70±1.88. In the control group, the median values were as follows: happy faces =6.85±0.51, sad faces =5.45±1.37, fear faces =4.13±1.55, disgust faces =5.63±1.06, angry faces =6.02±0.97, surprised faces =5.95±1.09, and neutral faces =6.47±0.86. The mean scores for responses to facial emotions for fear faces (t=-2.88, P=0.005), disgust faces (t=−2.86, P=0.005), and neutral faces (t=−2.56, P=0.009) were significantly lower in the patient group. The comparisons of mean reaction times to facial emotions in the patient group were as follows: happy faces =3.14±1.30 ms, sad faces =6.36±1.30 ms, fear faces =6.80±2.61 ms, disgust faces =7.08±2.01 ms, angry faces =6.35±2.75 ms, surprised faces =5.49±3.12 ms, and neutral faces =4.88±2.15 ms. In control group, the time to recognize facial emotions were as follows: happy faces =2.91±1.64 ms, sad faces =6.05±1.33 ms, fear faces =7.43±2.74 ms, disgust faces =5.83±3.45 ms, angry faces =7.23±2.75 ms, surprised faces =5.60±3.98 ms, and neutral faces =4.61±2.78 ms. The mean reaction time to facial emotions was similar between groups (t=0.78, P=0.43; t=0.49, P=0.62; t=−0.84, P=0.41; t=1.67, P=0.09; t=−0.92, P=0.35; t=−0.16, P=0.87; t=0.54, P=0.58, respectively; Tables 2 and 3).
 | Table 2 Comparison of responses to each facial emotion between groups |
 | Table 3 Comparison of mean reaction time to facial emotions between groups |
In the general linear model, the scores for the facial emotion recognition test were noted as the dependent variable, group was included as the fixed factor, and BAI, BDI, and TAI scores were included as covariants. Initially, the BAI and BDI scores were noted as covariants, and no significant differences were found between the groups in terms of scores of responses to each facial emotion and the mean score for reaction time to facial emotion (F=1.17; P=0.31). Then, scores for the TAS were added as covariants individually, and similarly, there were no significant differences between the groups (F=0.79; P=0.72). After adding the covariants, as expected, there were no significant differences in the mean scores of responses to each facial emotion or the mean scores for reaction times to facial emotions (F=0.87; P=0.59).
The subclasses of SDD, including somatic symptom disorder, conversion disorder, illness anxiety disorder, and unspecified somatic symptom and related disorder, were compared in terms of the mean scores for responses to each facial emotion and the mean reaction time to facial emotions. Because there was only one patient with other specified somatic symptom and related disorder, this subclass was not included in the comparison. There was no significant difference between the subdiagnostic groups (P-values for happy face =0.64, surprised face =0.21, fearful face =0.79, sad face =0.06, angry face =0.32, disgusted face =0.44, and neutral face =0.77; P-values for mean reaction time to happy face =0.07, surprised face =0.06, fearful face =0.14, sad face =0.41, angry face =0.06, disgusted face =0.58, and neutral face =0.08).
Discussion
The main findings of the present study were significantly decreased scores for responses to facial emotion of fear faces, disgust faces, and neutral faces in individuals with SSD compared with age- and sex-matched HC. After eliminating the effects of alexithymia and depressive and anxious states, the groups were similar in terms of responses to facial emotion and mean reaction time to facial emotions.
SSD were replaced with somatoform disorders while revising the Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition, Text Revision to DSM-5.11,12 As previously mentioned, there has been a considerable revision in this classification. Somatoform disorders have been criticized for a long time in terms of their diagnostic validities and reliabilities. Although the new diagnostic criteria of the SSD have also been criticized, they have been reported to enhance the diagnostic validity and clinical utility in patients who were suffering from somatic symptoms.20
Regarding emotional face recognition, there have been a limited number of studies in the literature that investigated this issue in patients with somatoform disorders. Buhlmann et al21 reported that patients with body dysmorphic disorder demonstrated deficits in facial emotion recognition. Pedrosa et al reported higher levels of alexithymia and deficits in facial emotion recognition in patients with somatoform disorders compared with HC. They found that there were no significant differences in facial recognition even when alexithymia was controlled for statistically. They suggested that deficits in facial recognition could be a consequence of alexithymia in patients with somatoform disorders.8 Pollatos et al found that patients with somatoform disorders had significantly reduced sad and neutral facial recognition performances in their study, which investigated autonomic imbalance and its relationships with facial recognition in patients with somatoform disorders. They also reported significant interactions between facial emotion recognition and alexithymia, anxiety, and depression.9 Schönenberg et al investigated facial affect perception and mental abilities in female pain disorder patients, which revealed impaired mental abilities and increased alexithymia in patients with pain disorder compared with HC. They reported that facial recognition was affected in patients with pain disorder.10 The etiology of SSD has been of great interest since the earliest times of psychiatry but still remains unclear. Each subclass of somatoform disorder, such as somatization disorder, conversion disorder, hypochondriasis, pain disorder, and body dysmorphic disorder, has a different etiological background. Although each subclass of the somatoform disorders has particular differences in terms of the etiology, it can be said that they have some shared psychodynamic, neurobiological, and cognitive backgrounds.22 As mentioned in the Introduction section, there have been numerous factors that create vicious cycles between physiological disturbances and emotional arousal in the etiology of SSD.3,4 According to the psychodynamic approach, patients with SSD have strong negative emotions that arise from interpersonal conflicts. They repress their negative emotions and present somatic symptoms that are related to their affective conditions.23,24 The neurobiological evidence and biomarkers can be assumed to be infantile in somatoform disorders compared with psychotic disorders, anxiety disorders, and mood disorders.22,25 Neuroanatomically and neurophysiologically, patients with somatoform disorders have been reported to have disturbed neuronal activity in numerous brain regions, such as the left amygdala, left insula, bilateral parahippocampal gyrus, left postcentral gyrus, and left posterior insula compared with HC.26 Regarding the neuroanatomical associations of facial emotion recognition, fearful faces and disgust faces have been reported to be associated with several neuroanatomical structures that have overlapping neuroanatomical and neurophysiological associations with somatoform disorders (eg, left amygdala, left insula, left postcentral gyrus, and left posterior insula).27 In our study, we found significant differences in the scores of facial emotion of fear faces, disgust faces, and neutral faces between patients with SSD and HC. Considering the psychodynamic and neuroanatomical explanations of somatoform disorders and neuroanatomic associations of facial emotion recognition, we consider that the results of our study support the literature.
Alexithymia is described as the inability to be aware of one’s own emotions and the inability to regulate one’s own emotions.28 Somatoform disorders were reported to be significantly related to alexithymia.29–34 Furthermore, alexithymia is related to deficits in facial recognitions among clinical disorders and partially the levels of depression and anxiety.7 As expected, patients with SSD had significantly higher TAS1, TAS2, BAI, and BDI scores. We first examined the scores for the facial emotion recognition test by statistically eliminating the effects of anxiety and depression, but we found no significant differences between the groups in terms of scores of facial emotion recognition. Then, we examined the scores for the facial emotion recognition test by eliminating the effects of alexithymia, and we found no significant differences between the groups. Finally, we compared the scores for the facial emotion recognition test by eliminating the effects of alexithymia, anxiety, and depression statistically, and as expected, we again found no significant differences between the groups. Pedrosa et al8 also reported no significant differences between patients with somatoform disorders and HC after eliminating the effect of alexithymia, and they argued that the impaired facial recognition in patients with somatoform disorders was associated with alexithymia. Regarding our results, they are in line with the results of Pedrosa et al’s study, and we also consider that the disturbed facial emotion recognition was the consequence of a higher level of alexithymia, depression, and anxiety.
Our study has some limitations. First, although all of SSD conditions share similar etiologies, we grouped and assessed the patients under the main diagnostic title; however, the clinical features were different between each subdiagnosis. For identifying this issue, we also compared factors of facial emotion recognition between subclasses of SSD, and we did not find any significant differences. Second, our sample size may be considered small for making a general conclusion even if our sample size is larger than the previous studies. Another limitation is the high percentage of female patients; however, the groups were age and sex matched. Although the control group was defined as having no psychiatric disorders, there may be undetected psychiatric conditions in HC. Furthermore, we assessed the patients in detail; however, comorbid psychiatric disorders are common in SSD, and there may also be undetected comorbid conditions in the patient group. The facial emotion recognition tests were performed in a quiet room; however, state anxiety and attention can affect the results of this test, which can be considered as another limitation.
There have been a limited number of studies that have investigated facial emotion recognition in patients with somatoform disorders. Considering the major changes in the diagnostic criteria of somatoform disorders, our study is the first to investigate facial emotion recognition in SSD. We suggest that the differences in the scores of facial emotion recognition between groups are associated with alexithymia and the levels of depression and anxiety. Further studies are needed to highlight the associations between facial emotion recognition and SSD.
Disclosure
The authors report no conflicts of interest in this work.
References
Hiller W, Rief W, Brähler E. Somatization in the population: from mild bodily misperceptions to disabling symptoms. Soc Psychiatry Psychiatr Epidemiol. 2006;41(9):704–712. | ||
Konnopka A, Schaefert R, Heinrich S, et al. Economics of medically unexplained symptoms: a systematic review of the literature. Psychother Psychosom. 2012;81(5):265–275. | ||
Rief W, Martin A. How to use the new DSM-5 somatic symptom disorder diagnosis in research and practice: a critical evaluation and a proposal for modifications. Annu Rev Clin Psychol. 2014;10:339–367. | ||
Kirmayer LJ, Taillefer S. Somatoform disorders. In: Turner SM, Hersen M, editors. Adult Psychopathology and Diagnosis. New York: Wiley; 1997:333–383. | ||
Allen LA, Woolfolk RL. Somatization and conversion disorder. In: Rief W, editor. A CBT Reference Guide. Vol. 2. New York: Wiley; 2013:181. | ||
Bailer J, Witthöft M, Rist F. Psychological predictors of short- and medium-term outcome in individuals with idiopathic environmental intolerance (IEI) and individuals with somatoform disorders. J Toxicol Environ Health A. 2008;71(11–12):766–775. | ||
Grynberg D, Chang B, Corneille O, et al. Alexithymia and the processing of emotional facial expressions (EFEs): systematic review, unanswered questions and further perspectives. PLoS One. 2012;7(8):e42429. | ||
Pedrosa Gil F, Ridout N, Kessler H, et al. Facial emotion recognition and alexithymia in adults with somatoform disorders. Depress Anxiety. 2009;26(1):26–33. | ||
Pollatos O, Herbert BM, Wankner S, et al. Autonomic imbalance is associated with reduced facial recognition in somatoform disorders. J Psychosom Res. 2011;71(4):232–239. | ||
Schönenberg M, Mares L, Smolka R, Jusyte A, Zipfel S, Hautzinger M. Facial affect perception and mentalizing abilities in female patients with persistent somatoform pain disorder. Eur J Pain. 2014;18(7):949–956. | ||
American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, DSM-IV. Washington, DC: American Psychiatric Press; 2000. | ||
American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders: DSM-5. Washington, DC: American Psychiatric Publishing; 2013. | ||
Beck AT. An inventory for measuring depression. Arch Gen Psychiatry. 1961;4:561–571. | ||
Hisli N. A study on the validity of Beck Depression Inventory. Turkish Journal of Psychology. 1988;6:118–122. | ||
Beck AT, Epstein N, Brown G, Steer RA. An inventory for measuring clinical anxiety: psychometric properties. J Consult Clin Psychol. 1988;56(6):893–897. | ||
Ulusoy M, Şahin NH, Erkmen H. Turkish version of the Beck anxiety inventory: psychometric properties. J Cogn Psychother. 1998;12(2):163–172. | ||
Bagby RM, Taylor GJ, Parker JD. The 20-item Toronto-Alexithymia-Scale-2. Convergent, discriminant, and concurrent validity. J Psychosom Res. 1994;38(1):33–40. | ||
Sayar K, Güleç H, Ak I. Validity and reliability of the twenty-item Toronto Alexithymia Scale (Turkish version). 37th National Psychiatry Congress Book. Istanbul, Turkey: Psychiatric Association of Turkey. 2001:130. | ||
Ekman P. Facial expressions. In: Power T, Dalgelish M, editors. Handbook of Cognition and Emotion. USA: Wiley Publishers University of California; 1999:301–320. | ||
Voigt K, Wollburg E, Weinmann N, et al. Predictive validity and clinical utility of DSM-5 somatic symptom disorder: prospective 1-year follow-up study. J Psychosom Res. 2013;75(4):358–361. | ||
Buhlmann U, Etcoff NL, Wilhelm S. Emotion recognition bias for contempt and anger in body dysmorphic disorder. J Psychiatr Res. 2006;40(2):105–111. | ||
Atmaca M. Neuro-imaging in somatoform disorders: a review. Turk Psikiyatri Derg. 2012;23(4):276–281. | ||
Waller E, Scheidt CE. Somatoform disorders as disorders of affect regulation: a development perspective. Int Rev Psychiatry. 2006;18(1):13–24. | ||
Marsh AA, Blair RJ. Deficits in facial affect recognition among antisocial populations: a meta-analysis. Neurosci Biobehav Rev. 2008;32(3):454–465. | ||
Browning M, Fletcher P, Sharpe M. Can neuroimaging help us to understand and classify somatoform disorders? a systematic and critical review. Psychosom Med. 2011;73(2):173–184. | ||
De Greck M, Scheidt L, Bölter AF, et al. Altered brain activity during emotional empathy in somatoform disorder. Hum Brain Mapp. 2012;33(11):2666–2685. | ||
Fusar-Poli P, Placentino A, Carletti F, et al. Functional atlas of emotional faces processing: a voxel-based meta-analysis of 105 functional magnetic resonance imaging studies. J Psychiatry Neurosci. 2009;34(6):418–432. | ||
Bach M, Bach D. Alexithymia in somatoform disorder and somatic disease: a comparative study. Psychother Psychosom. 1996;65(3):150–152. | ||
Bankier B, Aigner M, Bach M. Alexithymia in DSM-IV disorder: comparative evaluation of somatoform disorder, panic disorder, obsessive-compulsive disorder, and depression. Psychosomatics. 2001;42(3):235–240. | ||
Duddu V, Isaac MK, Chaturvedi SK. Alexithymia in somatoform and depressive disorders. J Psychosom Res. 2003;54(5):435–438. | ||
Grabe HJ, Frommer J, Ankerhold A, et al. Alexithymia and outcome in psychotherapy. Psychother Psychosom. 2008;77(3):189–194. | ||
Burba B, Oswald R, Grigaliunien V, Neverauskiene S, Jankuviene O, Chue P. A controlled study of alexithymia in adolescent patients with persistent somatoform pain disorder. Can J Psychiatry. 2006;51(7):468–471. | ||
Mattila AK, Kronholm E, Jula A, et al. Alexithymia and somatization in general population. Psychosom Med. 2008;70(6):716–722. | ||
Berthoz S, Pouga L, Wessa M. Alexithymia from the social neuroscience perspective. In: Decety J, Cacciopo J, editors. The Oxford Handbook of Social Neuroscience. New York: Oxford University Press; 2011:906–934. |
 © 2016 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2016 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.