")
Back to Journals » Journal of Pain Research » Volume 12
Introduction of pulsed radiofrequency cautery in infraorbital nerve block method for postoperative pain management of trauma-induced zygomaticomaxillary complex fracture reduction
Authors Kim KS , Lee WS , Cho H , Shim SM , Kwak S, Ji SY, Jeon S , Kim YM
Received 5 December 2018
Accepted for publication 26 March 2019
Published 11 June 2019 Volume 2019:12 Pages 1871—1876
DOI https://doi.org/10.2147/JPR.S197139
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor E Alfonso Romero-Sandoval
Video abstract presented by Yong-Min Kim.
Views: 348
Kwan-Sub Kim,1 Wu-Seop Lee,2 Haejun Cho,3 Sung-Min Shim,4 Soohyun Kwak,5 So-Young Ji,2 SangYoon Jeon,1 Yong-Min Kim6
1Department of Anesthesiology and Pain Medicine, Dongkang Medical Center, Ulsan, South Korea; 2Department of Plastic Surgery, Dongkang Medical Center, Ulsan, South Korea; 3Department of Medical Education, Icahn School of Medicine at Mount Sinai, New York, NY, USA; 4Department of Anesthesiology and Pain Medicine, Gangneung Asan Medical Center, University of Ulsan College of Medicine, Gangneung, South Korea; 5Department of Rehabilitation Medicine, Semin Hospital, Ulsan, South Korea; 6Department of Chemical and Biomolecular Engineering, Hong Kong University of Science and Technology, Hong Kong, Hong Kong
Abstract: Although various cases of neuralgia and its treatments have been reported, not enough evidence is present to recommend a single type of treatment as the most effective. The patient we have dealt with experienced significant interferences in his daily life due to chronic allodynia, but the symptom could not be resolved via previously reported treatments. We report a case of which a patient who presented infraorbital neuralgia after trauma was successfully treated by a novel treatment strategy. The patient was treated by applying infraorbital nerve block and pulsed radiofrequency cautery side by side. Through this report, we evaluate proper prevention and treatment strategies for patients who develop infraorbital neuralgia through similar etiologies.
Keywords: pulsed radio frequency, infraorbital nerve block, orbital wall fracture, ultrasound-guided, stellate ganglion block
Introduction
Zygomatico-orbital fracture is one of the most common facial injuries and has been estimated to occur in 10.4 per 100,000 inhabitants (Esbjerg, Denmark by St Joseph's Hospital statistics). In most cases, fracture lines involve the infraorbital (IO) foramen.1 Zygomatic complex fracture is known to cause paresthesia in 81% of patients, with 42% of those patients experiencing continued sensory disturbances even after surgery. Many patients that undergo maxillary bone fracture experience neuropathy even after surgical intervention.2 Hypoesthesia is a particularly common complaint, because the trigeminal nerve that exits via the IO foramen is a sensory nerve. The rate of permanent nerve injury is much lower, however, with one paper reporting permanent injury in 12% of cases2 and another paper reporting 10% of cases.3 As is the case in other neuralgias, carbamazepine is used as the first-line treatment among the pharmacological and surgical options for treating traumatic IO neuralgia. Other pharmaceuticals such as lamotrigine and baclofen has also been used to treat neuralgias.1,4,5 While there had been various attempts to treat allodynia caused by trauma, there is still not enough systematic evidence to recommend a particular algorithm for effective treatment.6 While surgical decompression is sometimes recommended, initial open reduction of the fracture is sometimes adequate as well.7
The patient in this report has experienced significant interferences in his daily life due to chronic allodynia following injury of the right eye and reconstruction surgery. Various attempts were made according to previously reported cases to resolve the discomfort, but no significant effect could be found. Eventually, we were able to alleviate the continued symptoms through the IO nerve block and ultrasound-guided IO nerve pulsed radiofrequency cautery (RFC).8 We report our treatment strategy in conjunction with the pain management clinic to evaluate proper prevention and treatment strategies for patients who develop IO neuralgia through similar etiologies.
Case report
A male patient 58 years of age was accepted to the emergency room, presenting right tripod fracture, right inferior blow-out fracture, and pneumocephalus due to extrinsic trauma. The patient was admitted to the neurosurgery department for pneumocephalus management after primary closure of lacerations in the right periorbital area (Figure 1). In the 3D computed tomography (CT) image, we could see the zygomaticomaxillary complex that was crushed and scattered from outside impact. Initial physical exam also showed that the patient’s senses on the right cheek and right IO territory were deprived.
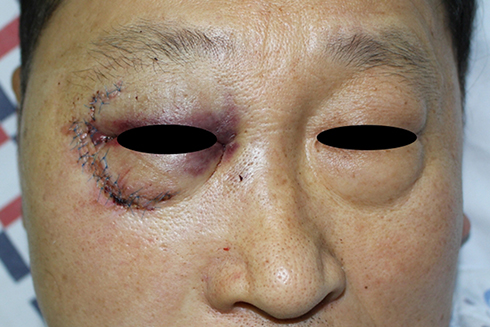 | Figure 1 Preoperative facial photograph. |
Seven days after the injury, pneumocephalus got better and the free air almost disappeared. The swelling of the region near eye and cheek area also went down, and malar reduction operation was conducted. He was then referred to the plastic surgery department. While the patient did not have any ophthalmologic abnormalities, the fracture was quite severe in that the overall bone structure between the arcus marginalis of the right zygomaticomaxillary complex bone and the inferior orbital wall was difficult to resolve (Figure 2).
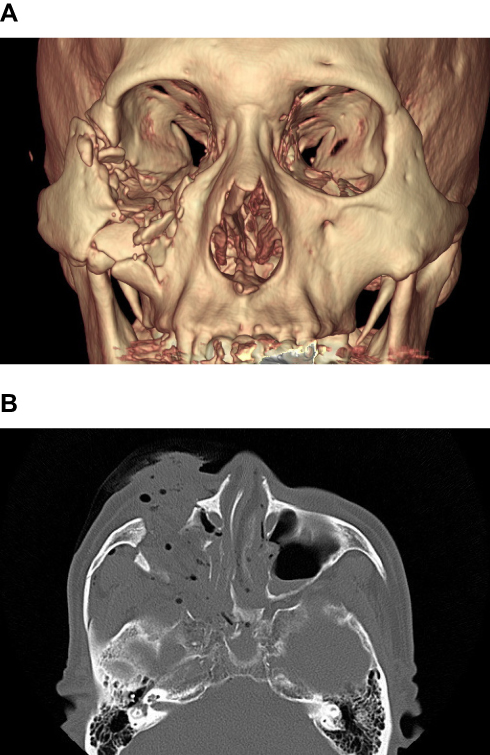 | Figure 2 Preoperative facial bone CT (computed tomogaphy). (A) 3D imaged photo. (B) Transverse section of CT. |
Preoperative measurements with the Hertel exophthalmometer (Good-Lite, Inc., Elgin, IL, USA) confirmed that the right orbit was depressed by 5 mm. The depressed area was reconstructed by reducing the zygomatic bone with a titanium plate and inlaying the IO wall with SynPOR® (DePuy Synthes, Inc., West Chester, PA, USA) (Figure 3). After the surgery, the depressed enophthalmos was approximately 3 mm, showing that the patient has improved in condition. During the outpatient follow-up, the right eye demonstrated decreased visual acuity upon medial side gaze due to enophthalmos. The patient also complained of lower eyelid sagging due to soft tissue loss, hypoesthesia in the right cheek, and intermittent neuralgia. Therefore, the patient was put under various cosmetic and therapeutic procedures in the following 2 years: a right lower blepharoplasty and fat graft at 6-month follow-up (Figure 4), correction of enophthalmos via artificial bone graft and fat graft on lower eyelid at 9-month follow-up (Figure 5), and scar revision and upper blepharoplasty to adjust the eyelid height at 16-month follow-up.
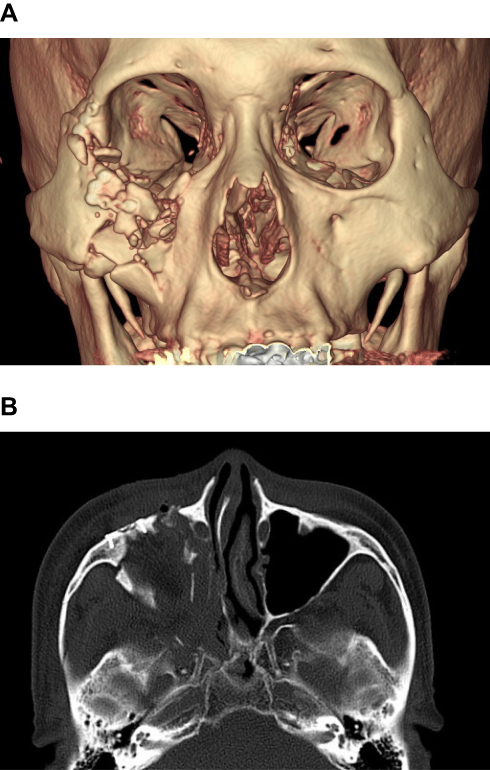 | Figure 3 Postoperative facial bone CT (computed tomography). (A) 3D imaged photo. (B) Transverse section of CT. |
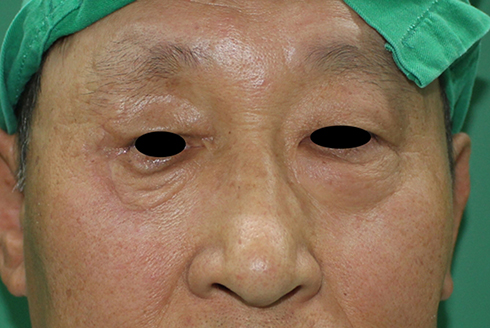 | Figure 4 Six-month follow-up photograph. |
 | Figure 5 Nine-month follow-up photograph. |
Usually, numbness due to zygomatic fracture is recovered within 6 months of follow-up. However, this patient had been suffering from decreased touch sensation up to 12 months of follow-up period. The hypoesthesia covered the cheek from the lower eyelid to gingiva of right upper second and third teeth with intermittent tingling sensation and allodynia. These symptoms put the patient under severe stress.
To deal with the symptoms, oral carbamazepine CR 200 mg twice a day and pregabalin 75 mg twice a day was prescribed side by side, but at 12-month follow-up neurological consult for hypoesthesia and neuralgia the visual analog scale (VAS) score was maintained at 50/100, showing no signs of improvement of the discomfort. Throughout the follow-up, other drugs such as mulex® (antispasmodic drug) and gliatamin® (Choline alfoscerate Code : N07AX02, Daewoong Bio Co., Ltd. Korea)(nootropics and neurotonics) were tested, but did not show any significant effect. Additional surgical process was considered unsuitable since it was too complex to remove all the bone fragments in the IO nerve, and in the process structural stability may be affected. The patient was already experiencing discomfort including diplopia due to 3 mm size enophthamos, and the removal of bone fractures to decompress the IO nerve could have worsened the situation. Simple pin removal was also considered, but the supportive force that was maintaining the structure was too unstable to proceed with the plate removal. After around 18 months of postoperative follow-up, facial CT images showed no signs of compression of nerves by the implant or bone fractures or any inflammation around the IO region, and operational decompression and pin removal were finally ruled out through discussion with the patient.
Meanwhile, the discomfort of the patient persisted and he found another clinic for more help. In the regional clinic, he went through a ganglion block procedure and experienced improvement in his symptoms. The alleviation, however, did not last long and the hypoesthesia continued. The patient especially suffered the most from sporadic neuralgia, and to resolve the issue we have planned and processed additional ganglion block and RFC in cooperation with the anesthesia department.
We first attempted a maxillary nerve block and stellate ganglion block, but the treatment showed no significant improvement in symptoms (Figure 6). The symptoms significantly alleviated after six IO nerve blocks with ropivacaine 0.2% + triamcinolone 20 mg (total volume 3 cc), before the patient was admitted to Department of Anesthesiology and Pain Medicine in Dong-Kang medical hospital and underwent ultrasound-guided IO nerve pulsed RFC (Figure 7). The patient experienced reduction of VAS from 50/100 to 30/100 through this procedure and was discharged for observation and follow-up. After 1 month the patient stated that the alleviated condition persisted.
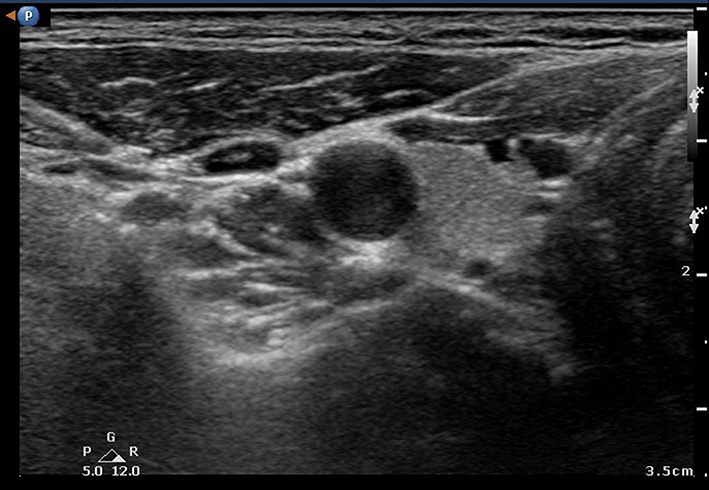 | Figure 6 Photograph during the infraorbital nerve block procedure. |
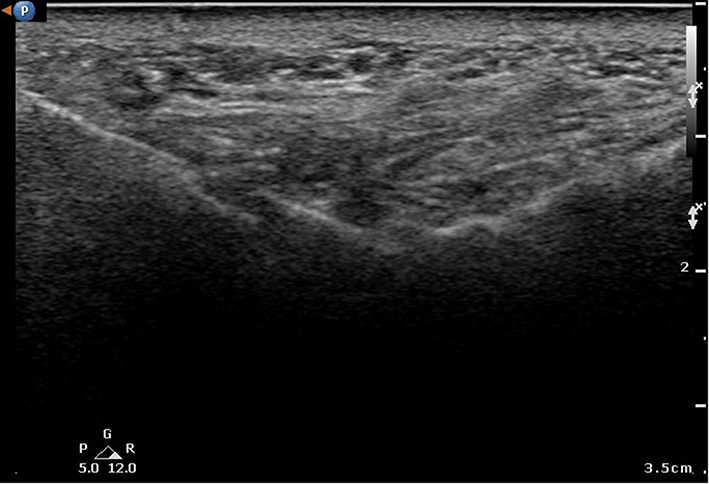 | Figure 7 Photograph during the infraorbital nerve radiofrequency cautery. |
Discussion
We are the first to report the utility of the pulsed radiofrequency cautery (RFC) in trauma-induced neuralgia. Most hypoesthesia secondary to zygomatic fracture typically improves over 6 months,1 this patient continued to complain of severe discomfort from hypoesthesia as well as intermittent tingling sensation and allodynia in the cheek from the lower eyelid to the gingiva of right upper second and third teeth throughout the 12-month follow-up period.
In this case, the IO foramen was severely fractured after the crushing trauma and the disruption of anatomy caused by the trauma introduced various constraints. For example, the severity of the injury caused difficulties in performing IO nerve block. While we evaluated surgical decompression of the IO nerve due to the neuropathic development of hypoesthesia and neuralgia following open reduction, reconstructing the original anatomy was difficult due to the severe crushing and fracturing of the nearby area that left no stable structure to fix the plate. For this reason, the patient was left with enophthalmos and IO territory numbness after the surgery, of which later developed into neuropathy. We thus proceeded with the reduction by subcillary incision and lateral eyebrow incision (without canthotomy), and fixed the plate on arcus marginalis and later rim of the orbit. SynPOR® sheet was also positioned on the holed orbital floor. Furthermore, there are some reports that a transconjunctival and transoral approach is enough to reduce the zygomaticomaxillary fracture, and this approach is superor to subcillary incision in the aspect of postoperative scarring.9,10 It could be a better option for this patient. However, the crushing injury of this patient was too severe, we choose subcillary incision to expose the bone fragment sufficiently. After the initial surgery, repeated attempts were made to restore the decompressed area and fix the enophthalmos. It seems that this procedure resulted in severe complication. Therefore, even though the patient experienced functional and structural improvements after multiple surgeries, we consulted the pain management service to manage the pain caused by the trauma and reconstruction procedures. There are several points to consider in determining whether to proceed with further surgery or consult the pain management nonoperatively: the severity of the pain, whether IO foramen needs to be widened, or only the pin is to be removed, and if the surgical process would worsen the existing symptoms (eg, enophthalmos). It is thus crucial for the plastic surgeon to take these points into consideration and cooperate with the anesthesia department at the outpatient ward postoperatively for rapid improvement of the patient's symptom.
Although the trigeminal nerve block performed at the outside clinic was not very effective in the long-term, the IO nerve block with ropivacaine 0.2% followed by steroid and ultrasound-guided IO nerve pulsed RFC significantly improved the patient's satisfaction. By utilizing a sensory stimulator with 0.2–0.3 V stimulation at 50 Hz in addition to ultrasound guidance, we were able to accurately target the nerve by correlating the stimulated area to the painful area in real-time.
Even though the mechanism of pulsed RFC remains unclear, we have succeeded in alleviating the patient’s discomfort. This demonstrates the possibility of RFC use in treating IO neuralgia when conventional methods such as carbamazepine medication or surgical decompression are unsuitable. It was shown that the diagnostic nerve block is effective in relieving patient discomfort and pulsed RFC was applied to see continued effect in the long-term. The method has much resolved the symptoms, and currently the patient is under oral carbamazepine, pregabaline mediation and is being followedup.11,12 His neuralgia is being well controlled with drugs at the moment. However, considering that the pulsed RFC applied to medial branch nerve block normally shows effect for 3 to 6 months, we plan on re-performing the pulsed RFC once the patient discomfort arises again.13 Overall, the important part is that no complications following the procedure were observed, and we thus suggest that this may be an effective treatment approach for various patients who are poor candidates for surgical nerve decompression as in this case.
In this report, we have relied on VAS to diagnose neuralgia due to the lack of an objective measurement criteria. While the Magnetic Resonance Imaging (MRI) test maybe used to test for neuralgias objectively, it is not widely used because of its low specificity and high cost.5 Therefore, for further development of the reported treatment strategy, active development and adoption of new methods to objectively evaluate neuralgia are considered necessary to properly evaluate the efficacy of pulsed RF in treating neuralgia.9
Patient consent
The patient provided written informed consent for the publication and the use of their images. Institutional approval was not required for this case report.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Benoliel R, Birenboim R, Regev E, Eliav E. Neurosensory changes in the infraorbital nerve following zygomatic fractures. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2005;99:657–665.
2. Jungell P, Lindqvist C. Paraesthesia of the infraorbital nerve following fracture of the zygomatic complex. Int J Oral Maxillofac Surg. 1987;16:363–367.
3. Altonen M, Kohonen A, Dickhoff K. Treatment of zygomatic fractures: internal wiring-antral-packing-reposition without fixation: a comparative follow-up study. J Maxillofac Surg. 1976;4:107–115.
4. Al-Quliti KW. Update on neuropathic pain treatment for trigeminal neuralgia. The pharmacological and surgical options. Neurosciences (Riyadh). 2015;20:107–114. doi:10.17712/nsj.2015.2.20140501
5. Bescos A, Pascual V, Escosa-Bage M, Malaga X. [Treatment of trigeminal neuralgia: an update and future prospects of percutaneous techniques]. Rev Neurol. 2015;61:114–124.
6. Tajima S. Malar bone fractures: experimental fractures on the dried skull and clinical sensory disturbances. J Maxillofac Surg. 1977;5:150–156.
7. Cheshire WP. Trigeminal neuralgia: diagnosis and treatment. Curr Neurol Neurosci Rep. 2005;5:79–85.
8. Emril DR, Ho KY. Treatment of trigeminal neuralgia: role of radiofrequency ablation. J Pain Res. 2010;3:249–254. doi:10.2147/JPR.S14455
9. Cortese A, Caggiano M, Carlino F, Pantaleo G. Zygomatic fractures: technical modifications for better aesthetic and functional results in older patients. Int J Surg. 2016;33:S9–S15. doi:10.1016/j.ijsu.2016.05.057
10. Cortese A, D’Alessio G, Bongo S, Gargiulo M, Claudio PP. Management of zygomatic fractures in young patients: technical modifications for aesthetic and functional results. J Craniofac Surg. 2016;27(8):2073–2077.
11. Magrinelli F, Zanette G, Tamburin S. Neuropathic pain: diagnosis and treatment. Pract Neurol. 2013;13(5).
12. Gilron I, Baron R, Jensen T. Neuropathic pain: principles of diagnosis and treatment. Mayo Clin Proc. 2015;90:532–545. doi:10.1016/j.mayocp.2015.01.018
13. Lee JH, Ha SH, Kim HT, Park SC, Kwon YE. Pulsed radiofrequency lesioning of the medial branch in a patient with cervical pain caused by a metastatic tumor: a case report. Korean J Anesthesiol. 2005;49(4):590–593. doi:10.4097/kjae.2005.49.4.590
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.