")
Back to Journals » Drug Design, Development and Therapy » Volume 14
Intravenous Iron Isomaltoside 1000 Reduces Postoperative Anemia in Patients Undergoing Elective Urologic Surgery and Those with Urosepsis
Authors Goh HJ , Lee KS , Kim TH, Kim KN, Lim HJ, Kim KS, Yang WJ, Jo JK
Received 13 August 2020
Accepted for publication 7 December 2020
Published 23 December 2020 Volume 2020:14 Pages 5679—5687
DOI https://doi.org/10.2147/DDDT.S276904
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Anastasios Lymperopoulos
Hyeok Jun Goh,1 Ki Soo Lee,1 Tae Hyo Kim,1 Kyu Nam Kim,2 Hyun Jin Lim,2 Kyu Shik Kim,3 Won Jae Yang,4 Jung Ki Jo3
1Department of Urology, Dong-A University, College of Medicine, Busan, Korea; 2Department of Anesthesia and Pain Medicine, Hanyang University, College of Medicine, Seoul, Korea; 3Department of Urology, Hanyang University, College of Medicine, Seoul, Korea; 4Department of Urology, Soonchunghyang University Hospital, Seoul, Korea
Correspondence: Jung Ki Jo
Department of Urology, Hanyang University, College of Medicine, 222-1 Wangsimni-ro, Seongdong-gu, Seoul 04763, Korea
Tel +821025196241
Email [email protected]
Purpose: Postoperative anemia is associated with increased morbidity and mortality in patients undergoing surgery. Anemia is also a common feature during sepsis. Therefore, here, we aimed to investigate the safety and efficacy of intravenous iron isomaltoside 1000 (Monofer®) in patients undergoing elective urologic surgery and in those with urosepsis.
Materials and Methods: This multicenter study was conducted through the review of the medical records of patients with postoperative anemia undergoing elective urologic surgery or with urosepsis in a multicenter hospital. Patients received a single intravenous iron isomaltoside (IIM), and their hemoglobin (Hb) level was evaluated before and after administration of IIM. Safety data included adverse effects and hypersensitivity reactions. In addition, the patients were divided into three groups (200 mg, 400 mg, and 600 mg IIM) to compare Hb changes before and after the administration of IIM.
Results: The study analyzed 52 men and 30 women with a mean age of 67 years. There was a significant difference between pre-treatment Hb and post-treatment Hb according to the type of the surgery after administration (p=0.01) of IIM in patients with postoperative anemia, and the mean preoperative Hb before IIM administration was 8.5 g/dL and that after IIM administration was 9.9 g/dL (p=0.006) in patients with urosepsis. The mean preoperative Hb changed from 10 g/dL to 11 g/dL after administration (p< 0.001) of IIM in the whole cohort. There were no side effects due to the administration of intravenous IIM.
Conclusion: A single perioperative intravenous injection of IIM 1000 significantly increased the Hb level in patients with anemia who underwent urologic elective surgery. Moreover, this treatment can be considered to have potential clinical benefits for anemia caused by sepsis.
Keywords: anemia, iron, iron isomaltoside 1000, urosepsis
Introduction
Anemia is very common in patients with acute illness, including those in the intensive care unit. In 3534 ICU patients, Vincent et al observed mean hemoglobin (Hb) concentrations of 11.3 g/dL at admission, with 29% of these patients having a concentration of less than 10 g/dL.1 Many factors are known to influence the Hb level in critically ill patients; some of the important factors among these are sepsis, overt or occult blood loss, decreased production of endogenous erythropoietin, and functional iron deficiency.2
Preoperative anemia was independently associated with increased morbidity and mortality in patients who underwent surgery.3,4 Untreated preoperative anemia and acute perioperative blood loss may increase surgical risk. Beattie et al5 reported that preoperative anemia was associated with a nearly five-fold increase in the odds of post-operative mortality in noncardiac surgery.
Sepsis is the culmination of complex interactions between the infecting microorganism and the host immune, inflammatory, and coagulation responses.6 Anemia is common in sepsis, in part because it is mediated by TNF-α and interleukin-1β and decreases the expression of the erythropoietin gene and protein.7 Sepsis due to urological problems, including obstructive uropathy and acute prostatitis, is common and fatal. The mortality ranges from 28% to 50% in patients with severe sepsis. Transfusion is worthwhile if needed at the emergency stage of sepsis; Rivers et al observed a marked decrease in mortality due to sepsis when transfusion was provided early.8
However, recent evidence has emerged to indicate that red blood cell transfusion may adversely impact patients who underwent surgery, causing higher mortality, increased risk of infection, and longer hospital and intensive care unit stays.9,10
In addition, religious concerns, such as those posed by the Jehovah’s Witnesses, may require a substitute for blood transfusion after elective surgery or sepsis. The use of erythropoiesis-stimulating agents and intravenous iron repletion have played a central role in the optimal correction of this anemia.
Therefore, here, we investigated the efficacy and safety of iron isomaltoside 1000 (Monofer®) in urologic sepsis and elective urologic surgery.
Materials and Methods
This study was conducted at two institutions (Hanyang University Seoul Hospital, Soonchunhyang University Seoul Hospital) in Korea from January to December 2017 and conducted in accordance with good clinical practice and the Declaration of Helsinki.
We performed our study after approving IRB from Hanyang University Hospital Institutional Review Board (IRB) (HY 2018–06-024-007). After approval was obtained with indication to have informed consent from IRB, written informed consent was obtained from all the patients. We reviewed the medical records of patients with postoperative anemia who were undergoing elective urologic surgery and patients with anemia due to sepsis. We defined anemic condition as patients with Hb ≤12.0 g/dL (7.45 mmol/L) for women and Hb ≤13.0 g/dL (8.1 mmol/L) for men, according to the WHO criteria. First, we excluded patients with iron overload or disturbances in utilization of iron (eg, hemochromatosis and hemosiderosis), s-ferritin >800 ng/mL, and diagnosed with inflammatory bowel disease such as Crohn’s disease and ulcerative colitis. Also we excluded patients with known hypersensitivity to any excipients in the investigational drug products, history of multiple allergies, decompensated liver cirrhosis and hepatitis, alanine aminotransferase >3 times the normal upper value, acute infection, and rheumatoid arthritis with symptoms or signs of active joint inflammation and pregnant or nursing women. In addition, patients with preoperative anemia and those who received blood transfusions due to urosepsis were excluded.
Iron isomaltoside (IIM) was administrated when postoperative anemia was observed on the first day after urologic elective surgery, while in the group of anemic patients with urosepsis, the administration was done on the day of admission. We measured the change in Hb in 7 days for both groups.
Patients receiving single doses of isomaltoside 1000 over 15 min were divided into three groups: 200 mg, 400 mg, and 600 mg. We decided the dose of IIM according to the degree of Hb change level.
Any concomitant medication or treatment deemed necessary to provide adequate supportive care was allowed throughout the trial, except for erythropoiesis stimulating agents and any iron supplementation other than the investigational drug, as they would have influenced the outcome of the study.
Objectives and Outcomes
The primary efficacy objective of the study was to evaluate the change in Hb level after IV IIM administration in patients with anemia undergoing elective urologic surgery and patients with anemia and urosepsis. Except for patients with severe anemia who required blood transfusion those who underwent urologic elective surgery, IIM was administrated. Then we assessed the safety (adverse events, vital signs, electrocardiogram (ECG), and biochemistry parameters).
Statistical Analyses
We analyzed demographics, change in hemoglobin (Hb) level, and Hb level according to the type of surgery using the Chi-squared test or Wilcoxon test, as appropriate. All statistical analyses were computed using SPSS (version 22.0 for Windows). All statistical tests were two-tailed, and the significance level was <0.05.
Results
Patients
In total, 82 patients were included in this study from January to December 2017 (Table 1). We classified the patients into two groups: patients with anemia that underwent urologic elective surgery (n=66) and anemic patients with urosepsis (n=16). Patients with urosepsis (70.1 years of age) were older than those undergoing urologic elective surgery (66.3 years of age). The patients were classified into three groups according to the dosage of iron isomaltoside 1000: 200 mg/mL (3.7%), 400 mg/mL (52.4%), and 600 mg/mL (43.9%). Patient demographics and baseline characteristics are summarized in Table 1. Overall, more men (63.4%) than women (36.6%) were included in this study.
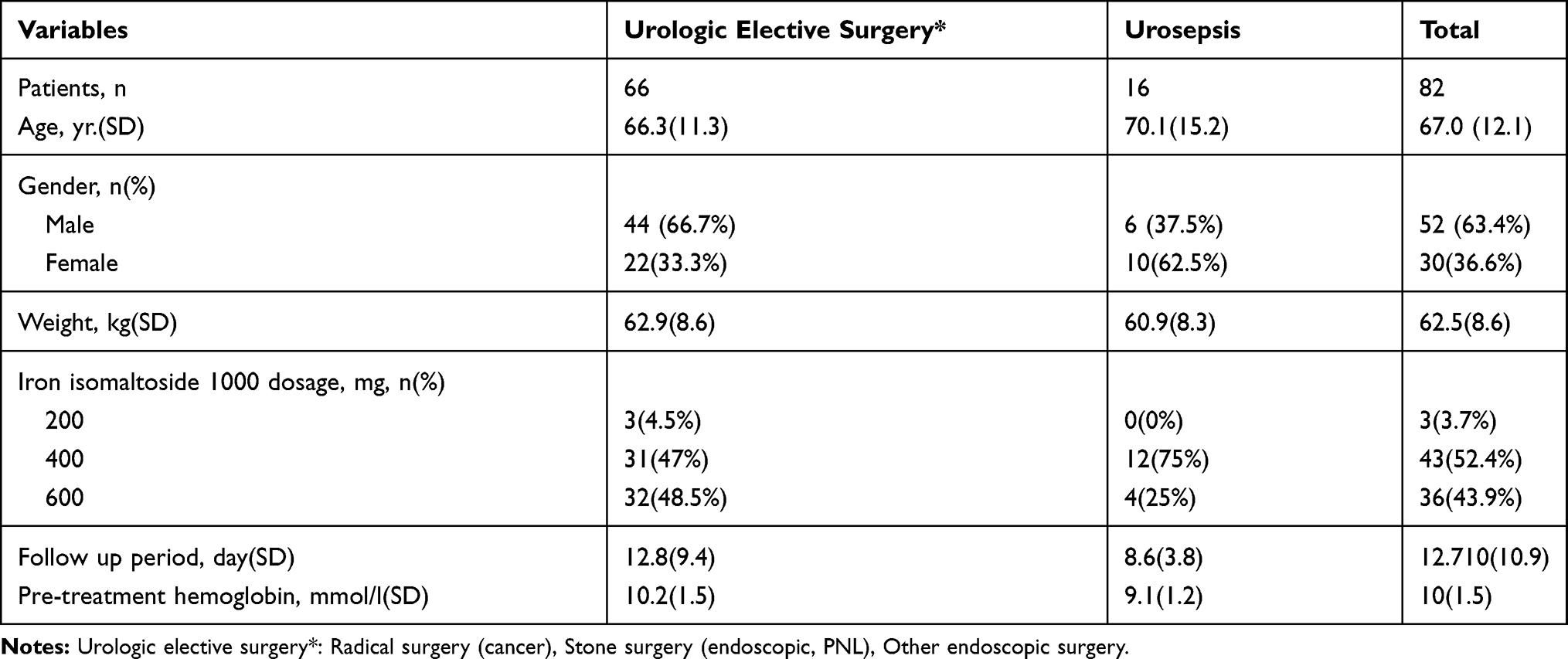 |
Table 1 Characteristics of Patients According to Group |
Efficacy of Iron Isomaltoside 1000 (IIM)
The primary efficacy analysis was the change in Hb concentration from baseline, following administration of IIM. We observed a significant difference between pre-treatment Hb and post-treatment Hb according to the type of surgery after IIM administration (p=0.01) in patients with postoperative anemia. The results of the Hb level change were measured by dividing patients into those who underwent stone surgery (including percutaneous nephrolithotomy) and those who underwent radical surgery and other endoscopic surgery. Seven days after surgery, Hb level had increased to an average of 11.4 g/dL from 9.5 g/dL in the patients who underwent stone surgery, and also increased to an 11.0 g/dL from 10.1 g/dL in the patients who underwent other surgery. We also found a significant difference between stone surgery (including percutaneous nephrolithotomy) and other types of urologic surgery (p=0.009) (Table 2). The mean preoperative Hb before IIM administration was 8.5 g/dL, and it was 9.9 g/dL after IIM administration (p=0.006) in patients with urosepsis (Table 3). Mean preoperative Hb changed from 10 g/dL to 11 g/dL after administration (p<0.001) in the whole cohort.
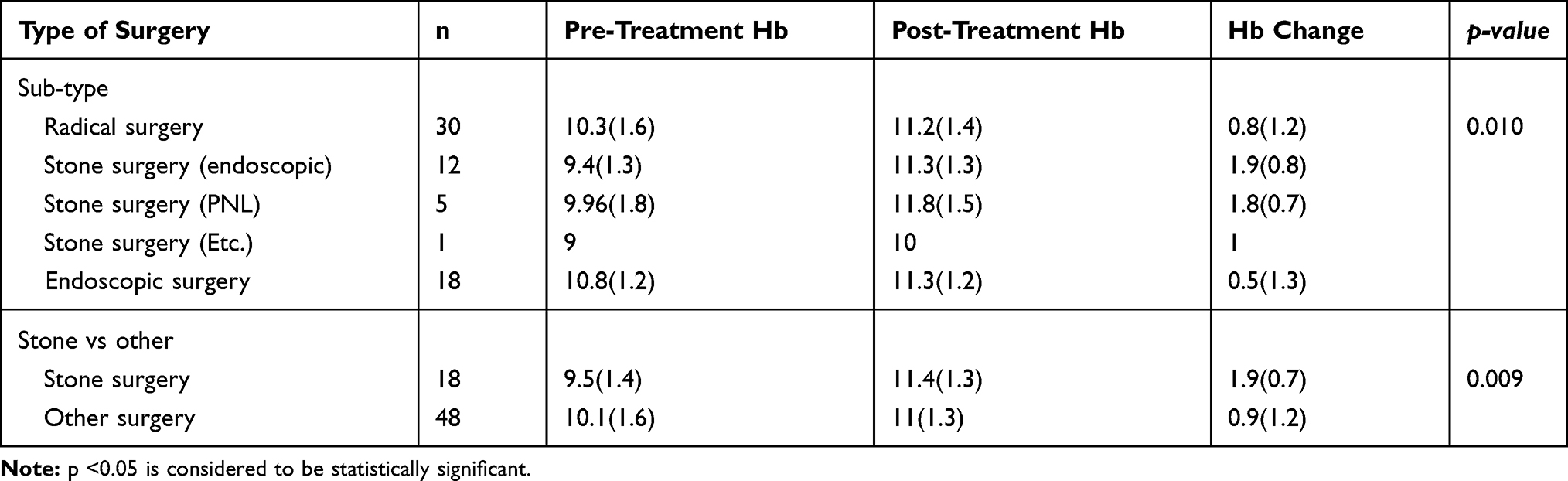 |
Table 2 Outcomes of Elective Surgery Type |
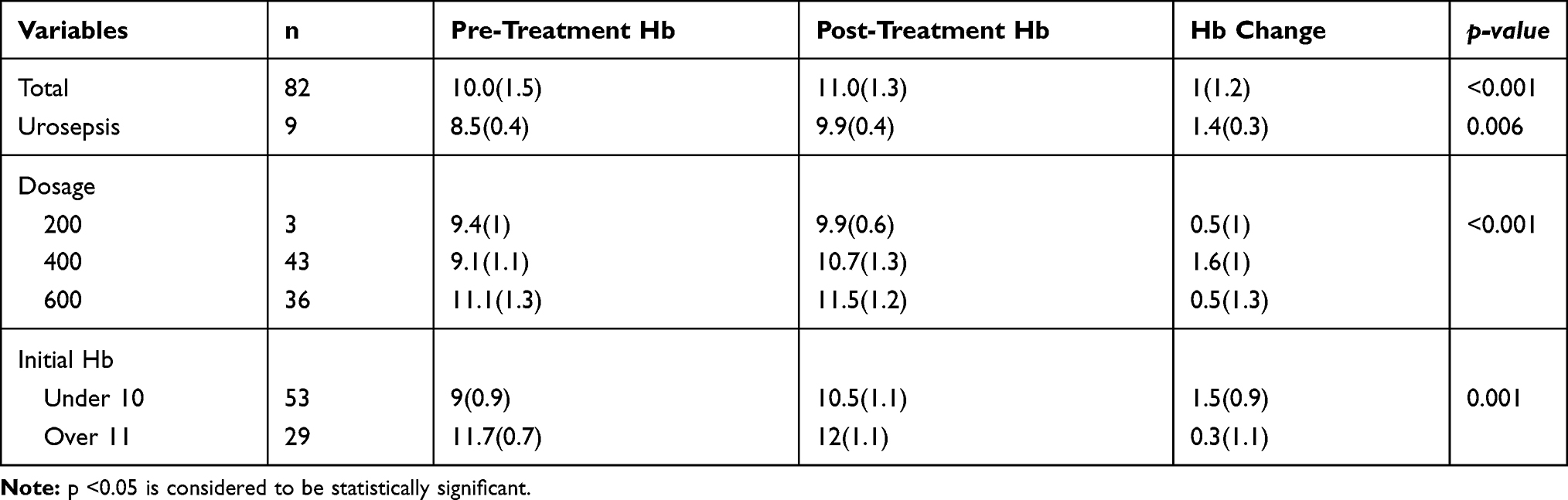 |
Table 3 Comparison of Hb Change Before and After Treatment with Iron Isomaltoside 1000 |
The Hb level change differed according to the type of surgery in this cohort (Figure 1), and the pre-treatment Hb level and post-treatment Hb level were different for each surgery type (Figure 2). The pre-treatment Hb level and post-treatment Hb level in patients with urosepsis were also different (Figure 3).
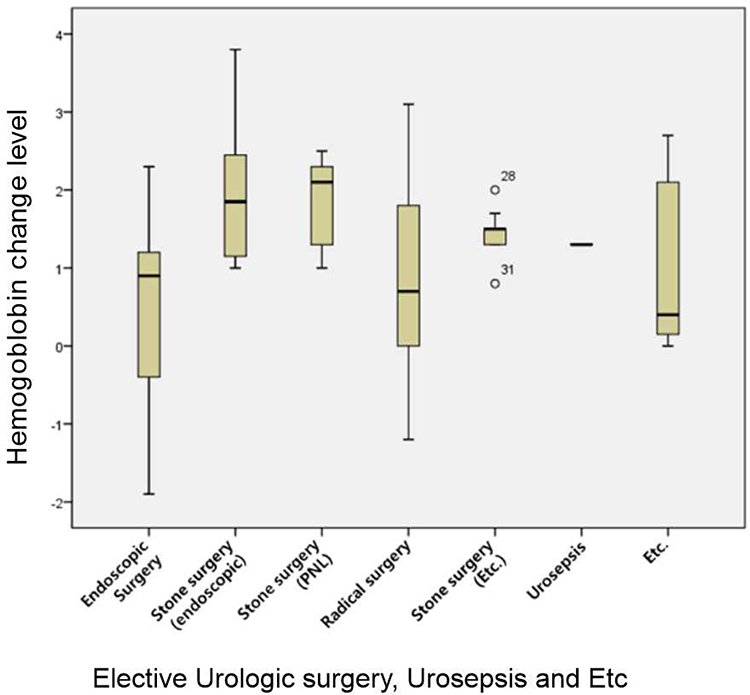 |
Figure 1 The change of hemoglobin level according to the type of surgery. |
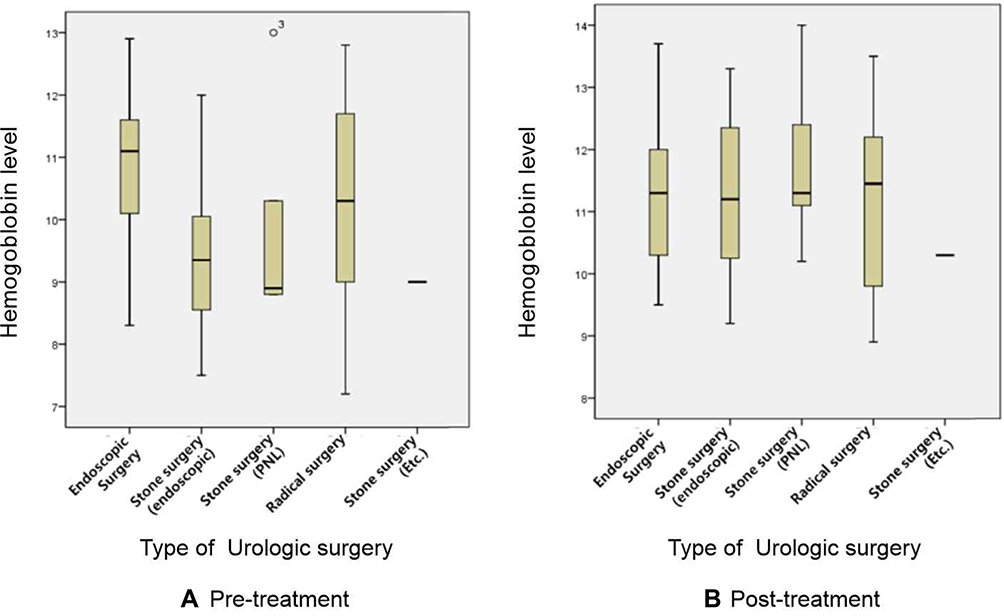 |
Figure 2 The differences of hemoglobin level for each surgery type. (A) Pre-treatment (B) Post-treatment. |
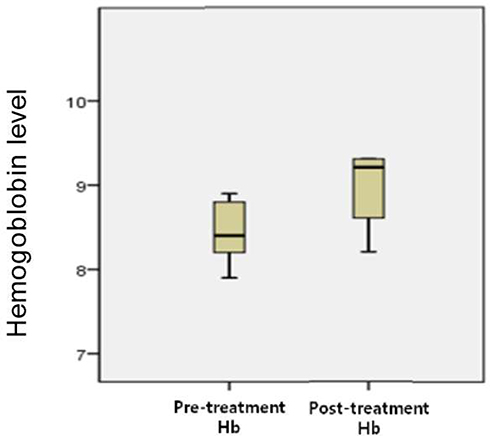 |
Figure 3 The pre-treatment Hb level and post-treatment Hb level in patients with urosepsis. |
Safety
Among the 82 patients available for safety analysis in the present study, no adverse drug reactions were reported to be related to the IIM. The hematological and biochemistry parameters and vital signs were checked at each trial visit, and no cases of hypophosphatemia (defined as a phosphate level <2 mg/dL) were observed.
Discussion
This study is, to the best of our knowledge, the first cohort study to investigate the effects of intravenous iron administration in place of allogenic blood transfusion in patients with postoperative anemia in the field of urologic surgery. The etiology of anemia is diverse and includes blood loss, decreased RBC production owing to functional iron deficiency, and altered erythropoiesis in critically ill patients. In addition, perioperative anemia, which occurs in 33% to 50% of surgical patients, is one of the major predictive factors for allogenic blood transfusion (ABT) in surgeries with moderate to high perioperative blood loss and it induces postoperative anemia and aggravates existing anemia.11
ABT carries increased risks for transmission of infectious diseases, postoperative nosocomial infection and has been clearly demonstrated to be associated with adverse outcomes related to postoperative acute kidney injury, neurological complications and postoperative atrial fibrillation after cardiac surgery.12 Despite efforts to reduce ABT, transfusion requirements still remain high. In this regard, a discussion on patient blood management (PBM) programs aim at identifying patients at risk for transfusions has been conducted in Europe.13 PBM programs are based on multimodal approach including early preoperative recognition and treatment of anemic patients, surgical efforts to minimize blood loss. From this point of view, preoperative optimization of anemia seems to be a key aspect of PBM.
Iron deficiency is common, either owing to the depletion of whole-body iron stores or because of the restricted availability of iron for erythrogenesis (functional iron deficiency). Thus, iron therapy is commonly used to restore the iron reserve to prevent anemia after bleeding. Iron plays an essential role in erythropoiesis and hemoglobin synthesis.14 Therefore, here, we tried to investigate the effect of the preoperative administration of intravenous iron isomaltoside 1000 (Monofer®) in patients undergoing elective urologic surgery. In our study, a significant elevation in Hb was observed without blood transfusion in endoscopic stone surgery and percutaneous nephrolithotomy (PNL), which can cause postoperative anemia or bleeding.
The new IV iron supplement, iron isomaltoside 1000 (IIM), is composed of iron and chemically modified isomalto-oligosaccharides that have a mean molecular weight of 1000 Da and consist predominantly of 3–5 glucose units. In contrast to dextran polysaccharides present in iron dextran, isomaltoside is a linear and unbranched molecule with a theoretically reduced anaphylactogenic potential.15 Physiochemically, the strong binding of iron within the IIM formulation enables a controlled and slow release of bioavailable iron to the iron-binding proteins, with only a low risk of free iron toxicity.16 This allows the rapid administration of high single doses of IIM. Several studies employing IIM have shown it to be well tolerated and to improve iron-related parameters in patients with various conditions, including patients with CKD receiving dialysis,17 patients with chronic heart failure, patients with inflammatory bowel disease,18,19 and patients undergoing cardiac surgery,20 major orthopedic surgery,11 or major abdominal surgery.21 To date, clinical trials of IIM have demonstrated a good efficacy and a good safety profile, and systemic reviews and meta-analysis of randomized clinical trials comparing intravenous iron to other comparators have indicated that all currently available intravenous iron preparations are safe.22,23
Perioperative anemia is common among patients scheduled to undergo elective surgery and it is also a predictor of blood transfusion. The prevalence of perioperative anemia is reported to range from 5% to 75% of electively scheduled patients.24,25 In our study, the average Hb level of 66 patients who were scheduled for elective surgery was 10.2 g/dL, which is quite low according to the definition provided by the World Health Organization. Van Straten et al4 reported that a lower preoperative Hb level is an independent predictor of late mortality in patients undergoing coronary artery bypass grafting, whereas anemia is a risk factor for early and late mortality. Iron-deficiency anemia is the most common form of anemia and may be associated with other hematologic deficiencies, particularly among the elderly population; it compromises patients’ ability to recover Hb after surgery.26 Based on previous studies and our experiences, we expect intravenous iron administration to be able to reduce the incidence of postoperative infections associated with blood transfusion, reduce the length of hospital stay, and facilitate better recovery and outcome.
Another notable result of our study was that intravenous iron administration caused a statistically significant elevation of the Hb level (from 8.5 g/dL to 9.9 g/dL) in patients with urosepsis. Consensus guidelines for the management of sepsis have been published.27 Early in the course of sepsis, the cornerstone of emergency management of sepsis is early, goal-directed therapy plus administration of lung protective ventilation broad-spectrum antibiotics.8,28 Similar to the management of patients with sepsis, the guideline for patients with urosepsis recommends antibiotic treatment as soon as possible after diagnosis, but only after blood and urine cultures have been obtained (recommendation grade B, evidence level Ic).29 According to the concept of early goal-directed therapy, hemodynamic stabilization promotes the delivery of an adequate oxygen supply to the tissues. Therefore, as soon as the diagnosis of urosepsis is suspected, the intravenous administration of isotonic crystalloid solution should be started, and blood products should be administered to target a hemoglobin level of 7–9 g/dL. Anemia is common in sepsis, and erythropoietin requires between days to weeks to induce red blood cell production; thus, it may not be effective.7 To date, the criteria for which blood products should be used to correct anemia with supportive treatment in urosepsis are unclear and lack supporting evidence. In our study, 16 patients with urosepsis showed a significant increase in Hb level (from 8.5 g/dL to 9.9 g/dL) after the administration of IIM. Our study also showed that the degree of elevation of the Hb level was significantly greater in the group with initial Hb ≤10 g/dL compared to that in the group with initial Hb ≥11 g/dL when comparing the effects of intravenous IIM. Based on these findings, IIM may be an alternative to allogenic blood transfusion, with a reduced incidence of adverse effects due to blood transfusion, which may increase mortality.
To date, there are no clinical guidelines to support the use of prophylactic intravenous iron before major elective surgery. Therefore, we searched the literature in MEDLINE (January 1, 1990, through December 31, 2017) that examined intravenous iron therapy in patients scheduled to undergo elective surgery, except for patients with iron-deficiency anemia, inflammatory bowel disease, and chronic kidney disease. We selected and summarized five studies that were well-designed. One paper described treatment with IIM and four papers detailed treatment with iron sucrose (Table 4). Owing to the differences in the type, timing, and dosage of the intravenous iron supplement used prior to surgery, the results of the Hb level and transfusion requirements were statistically different. When comparing our study with the PROTECT trial, which evaluated the effect of perioperative IV IIM in patients without anemia undergoing elective or subacute coronary artery bypass graft or valve replacement, we found that the Hb level had significantly increased, and fewer patients were anemic in the IV IIM-treated group in both studies.20
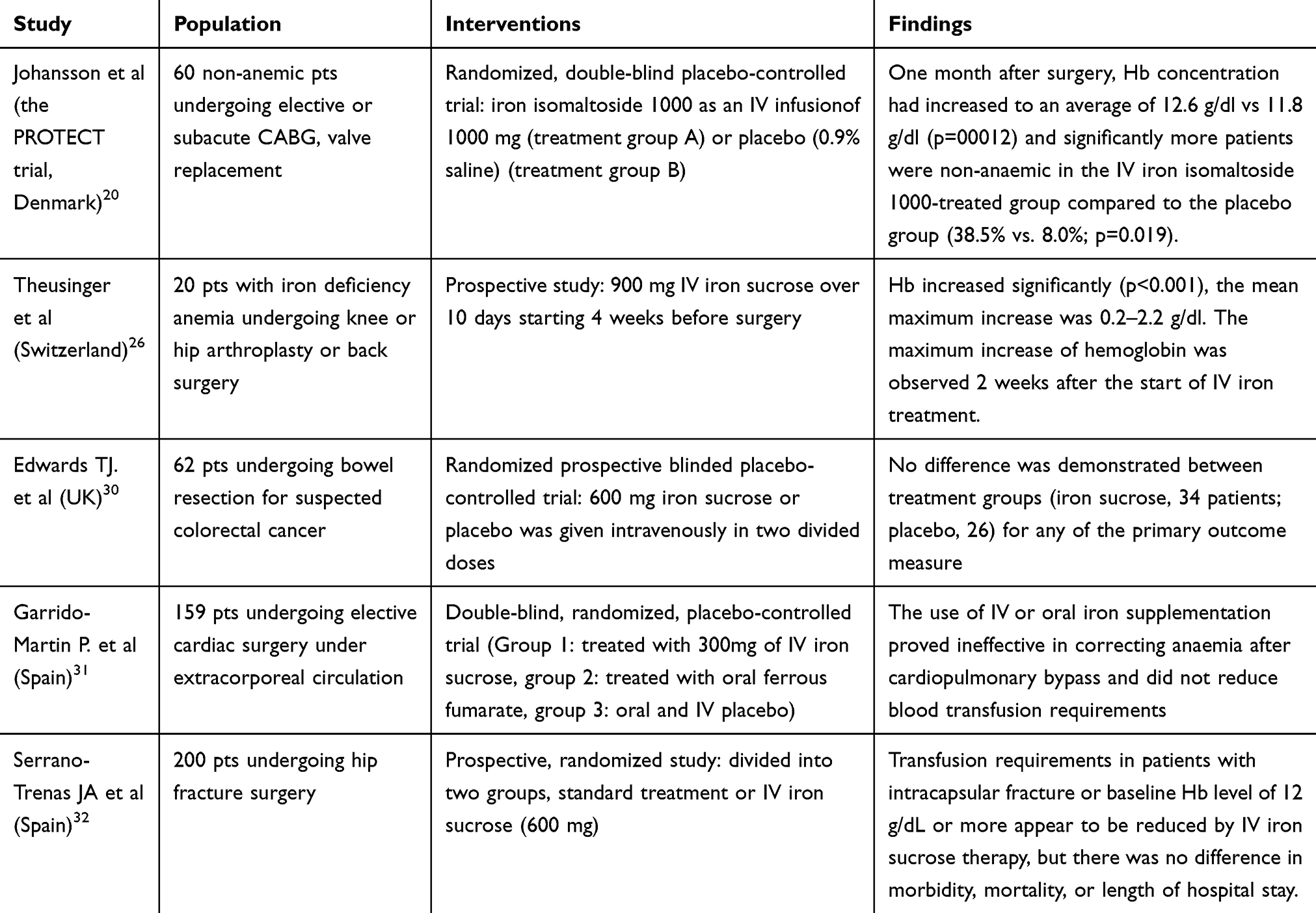 |
Table 4 Summary of Studies About Intravenous Iron Preparations for Patients Undergoing Elective Surgery |
This trial was an exploratory and retrospective study with the limitation of a small sample size of the patients undergoing elective urologic surgery. And the limitation of this study is that there was no data on iron-related parameters (transferrin saturation, ferritin, reticulocytes) as a retrospective study to find out the effects of IIM as an alternative to blood transfusion in patients who underwent urologic surgery with postoperative anemia. In this cohort, there was no control group receiving either placebo or comparing result about transfusion requirement. We only compared and reported the treatment before and after at anemic status. Designed as a retrospective study, there is a limitation that each group could be heterogenous. The novelties of this study are the feasibility of Intravenous IIM in patients with anemia after elective urologic surgery and the efficacy of Intravenous IIM in patients with anemia due to urosepsis.
Hence, we are planning additional clinical studies employing a large, randomized, controlled, prospective trial to allow further evaluation of the differences in effect according to iron status (serum iron, ferritin, and transferrin saturation index) for the treatment of anemia in clinical settings.
Conclusion
This study has demonstrated that IIM can be used safely and effectively to prevent anemia after elective urologic surgery and reduce the need for blood transfusion. The reviewed data in patients who underwent urologic elective surgery (n=66) and patients with anemia and urosepsis (n=16) showed adequate efficacy and a good safety profile of IIM. The results also showed that the hemopoietic response was evident in urosepsis. The safety profile of IIM is favorable. Therefore, we expect that the administration of IIM is attractive not only for patients with anemia that are undergoing urologic surgery, but also for patients with anemia due to sepsis.
Abbreviations
IIM, iron isomaltoside; Hb, hemoglobin; ICU, intensive care unit; ABT, allogenic blood transfusion; PBM, patient blood management; PNL, percutaneous nephrolithotomy; CKD, chronic kidney disease.
Acknowledgment
This article was funded by Pharmbio Inc. This study was performed statistical analysis by Inha Yoon, Ji Ye Han.
Disclosure
The authors report no conflicts of interest for this work.
References
1. Vincent JL, Baron JF, Reinhart K, et al. Anemia and blood transfusion in critically ill patients. JAMA. 2002;288(12):1499–1507.
2. Viljoen M, Coetzee IH, Roux LJ, et al. Anemia in surgical intensive care patients. Haematologica. 1994;79(1):19–24.
3. Karkouti K, Wijeysundera DN, Beattie WS. the Reducing Bleeding in Cardiac surgery (RBC) investigators. Risk associated with preoperative anemia in cardiac surgery: a multicentre cohort study. Circulation. 2008;117(4):478–484. doi:10.1161/CIRCULATIONAHA.107.718353
4. Van Straten AHM, Hamad MA, van Zundert AJ, et al. Preoperative Hemoglobin level as a predictor of survival after coronary artery bypass grafting. Circulation. 2009;120(2):118–125. doi:10.1161/CIRCULATIONAHA.109.854216
5. Beattie WS, Karkouti K, Wijeysundera DN, et al. Risk associated with preoperative anemia in noncardiac surgery: a single-center cohort study. Anesthesiology. 2009;110:574–581.
6. Hotchkiss RS, Karl IE. The pathophysiology and treatment of sepsis. N Engl J Med. 2003;348(2):138–150. doi:10.1056/NEJMra021333
7. Jelkmann W. Proinflammatory cytokines lowering erythropoietin production. J Interferon Cytokine Res. 1998;18(8):555–559. doi:10.1089/jir.1998.18.555
8. Rivers E, Nguyen B, Havstad S, et al. Early goal-directed therapy in the treatment of severe sepsis and septic shock. N Engl J Med. 2001;345(19):1368–1377. doi:10.1056/NEJMoa010307
9. Dunne JR, Malone D, Tracy JK, et al. Perioperative anemia: an independent risk factor for infection, mortality, and resource utilization in surgery. J Surg Res. 2002;102(2):237–244. doi:10.1006/jsre.2001.6330
10. Bernard AC, Davenport DL, Chang PK, et al. Intraoperative transfusion of 1 U to 2 U packed red blood cells is associated with increased 30-day mortality, surgical-site infection, pneumonia, and sepsis in general surgery patients. J Am Coll Surg. 2009;208(5):931–937. doi:10.1016/j.jamcollsurg.2008.11.019
11. Munoz M, Gomez-Ramirez S, Cuenca J, et al. Very-short-term perioperative intravenous iron administration and postoperative outcome in major orthopedic surgery: a pooled analysis of observational data from 2547 patients. Transfusion. 2014;54(2):289–299.
12. Koch CG, Li L, Van Wagoner DR, et al. Red cell transfusion is associated with an increased risk for postoperative atrial fibrillation. Ann Thorac Surg. 2006;82(5):1747–1756. doi:10.1016/j.athoracsur.2006.05.045
13. Theusinger OM, Felix C, Spahn DR. Strategies to reduce the use of blood products: a European perspective. Curr Opin Anaesthesiol. 2012;25(1):59–65. doi:10.1097/ACO.0b013e32834dec98
14. Silverberg DS, Iaina A, Peer G, et al. Intravenous iron supplementation for the treatment of the anemia of moderate to severe chronic renal failure patients not receiving dialysis. Am J Kidney Dis. 1996;27(2):234–238. doi:10.1016/S0272-6386(96)90546-6
15. Altman LC, Petersen PE. Successful prevention of an anaphylactoid reaction to iron dextran. Ann Intern Med. 1988;109:346–347. doi:10.7326/0003-4819-109-4-346
16. Jahn MR, Andreasen HB, F€utterer S, et al. A comparative study of the physicochemical properties of iron isomaltoside 1000 (Monofer), a new intravenous iron preparation and its clinical implications. Eur J Pharm Biopharm. 2011;78:480–491. doi:10.1016/j.ejpb.2011.03.016
17. Bhandari S, Kalra PA, Kothari J, et al. A randomized, open-label trial of iron isomaltoside 1000 (MonoferVR) compared with iron sucrose (VenoferVR) as maintenance therapy in haemodialysis patients. Nephrol Dial Transplant. 2015;30:1577–1589. doi:10.1093/ndt/gfv096
18. Reinisch W, Altorjay I, Zsigmond F, et al. A 1-year trial of repeated high-dose intravenous iron isomaltoside 1000 to maintain stable hemoglobin levels in inflammatory bowel disease. Scand J Gastroenterol. 2015;50(10):1226–1233. doi:10.3109/00365521.2015.1031168
19. Dahlerup J, Lindgren S. High dose intravenous iron isomaltoside 1000 in patients with inflammatory bowel disease – the PROMISE trial.
20. Johansson PI, Rasmussen AS, Thomsen LL. Intravenous iron isomaltoside 1000 (MonoferVR) reduces postoperative anaemia in preoperatively non-anaemic patients undergoing elective or subacute coronary artery bypass graft, valve replacement or a combination thereof: a randomized double-blind placebo-controlled clinical trial (the PROTECT trial). Vox Sang. 2015;109:257–266.
21. Froessler B, Palm P, Weber I, et al. The important role for intravenous iron in perioperative patient blood management in major abdominal surgery: a randomized controlled trial. Ann Surg. 2016;264(1):41–46. doi:10.1097/SLA.0000000000001646
22. Avni T, Bieber A, Grossman A, et al. The safety of intravenous iron preparations: systematic review and meta-analysis. Mayo Clin Proc. 2015;90(1):12–23. doi:10.1016/j.mayocp.2014.10.007
23. Rognoni C, Venturini S, Meregaglia M, et al. Efficacy and safety of ferric carboxymaltose and other formulations in iron-deficient patients: a systematic review and network meta-analysis of randomised controlled trials. Clin Drug Investig. 2016;36(3):177–194. doi:10.1007/s40261-015-0361-z
24. Goodnough LT, Shander A, Spivak JL, et al. Detection, evaluation, and management of anemia in the elective surgical patient. Anesth Analg. 2005;101:1858–1861. doi:10.1213/01.ANE.0000184124.29397.EB
25. Shander A, Knight K, Thurer R, et al. Prevalence and outcomes of anemia in surgery: a systematic review of the literature. Am J Med. 2004;116(Suppl 7A):58S–69S. doi:10.1016/j.amjmed.2003.12.013
26. Theusinger OM, Leyvraz P-F, Schanz U, et al. Treatment of iron deficiency anemia in orthopedic surgery with intravenous iron: efficacy and limits: a prospective study. Anesthesiology. 2007;107(6):923–927. doi:10.1097/01.anes.0000291441.10704.82
27. Dellinger RP, Carlet JM, Masur H, et al. Surviving Sepsis Campaign guidelines for management of severe sepsis and septic shock. Crit Care Med. 2004;32(3):858–873. doi:10.1097/01.CCM.0000117317.18092.E4
28. Ibrahim EH, Sherman G, Ward S, et al. The influence of inadequate antimicrobial treatment of bloodstream infections on patient outcomes in the ICU setting. Chest. 2000;118(1):146–155. doi:10.1378/chest.118.1.146
29. Dreger NM, Degener S, Ahmad-Nejad P, et al. Urosepsis–etiology, diagnosis, and treatment. Dtsch Arztebl Int. 2015;112:837–847.
30. Edwards TJ, Noble EJ, Durran A, et al. Randomized clinical trial of preoperative intravenous iron sucrose to reduce blood transfusion in anaemic patients after colorectal cancer surgery. Br J Surg. 2009;96(10):1122–1128. doi:10.1002/bjs.6688
31. Garrido-Martín P, Nassar-Mansur MI, de la Llana-ducrós R, et al. The effect of intravenous and oral iron administration on perioperative anaemia and transfusion requirements in patients undergoing elective cardiac surgery: a randomized clinical trial. Interact Cardiovasc Thorac Surg. 2012;15(6):1013–1018. doi:10.1093/icvts/ivs344
32. Serrano-Trenas JA, Ugalde PF, Cabello LM, et al. Role of perioperative intravenous iron therapy in elderly hip fracture patients: a single-center randomized controlled trial. Transfusion. 2011;51(1):97–104. doi:10.1111/j.1537-2995.2010.02769.x
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.