")
Back to Journals » Therapeutics and Clinical Risk Management » Volume 19
Intraoperative Variables Enhance the Predictive Performance of Myocardial Injury in Patients with High Cardiovascular Risk After Thoracic Surgery When Added to Baseline Prediction Model
Authors Lin S , Huang X , Zhang Y, Zhang X, Cheng E, Liu J
Received 27 February 2023
Accepted for publication 8 May 2023
Published 24 May 2023 Volume 2023:19 Pages 435—445
DOI https://doi.org/10.2147/TCRM.S408135
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Deyun Wang
Shuchi Lin,1,* Xiaofan Huang,1,* Ying Zhang,1 Xiaohan Zhang,1 Erhong Cheng,1 Jindong Liu1– 4
1Department of Anesthesiology, the Affiliated Hospital of Xuzhou Medical University, Xuzhou, Jiangsu, People’s Republic of China; 2Jiangsu Province Key Laboratory of Anesthesiology, Xuzhou Medical University, Xuzhou, Jiangsu, People’s Republic of China; 3Jiangsu Province Key Laboratory of Anesthesia and Analgesia Application Technology, Xuzhou Medical University, Xuzhou, Jiangsu, People’s Republic of China; 4NMPA Key Laboratory for Research and Evaluation of Narcotic and Psychotropic Drugs, Xuzhou Medical University, Xuzhou, Jiangsu, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Jindong Liu, Department of Anesthesiology, the Affiliated Hospital of Xuzhou Medical University, Huaihai Road West, Quanshan District, Xuzhou, Jiangsu, People’s Republic of China, Tel +86-13951355136, Email [email protected]
Purpose: Myocardial injury after non-cardiac surgery is closely related to major adverse cardiac and cerebrovascular event and is difficult to identify. This study aims to investigate how to predict the myocardial injury of thoracic surgery and whether intraoperative variables contribute to the prediction of myocardial injury.
Methods: The prospective study included adult patients with high cardiovascular risk who underwent elective thoracic surgery from May 2022 to October 2022. Multivariate logistic regression was used to establish a model with baseline variables and a model with baseline and intraoperative variables. We compare the predictive performance of two models for postoperative myocardial injury.
Results: In general, 31.5% (94 of 298) occurred myocardial injury. Age ≥ 65 years old, obesity, smoking, preoperative hsTnT, and one-lung ventilation time were independent predictors of myocardial injury. Compared with baseline model, the intraoperative variables improved model fit, modestly improved the reclassification (continuous net reclassification improvement 0.409, 95% CI, 0.169 to 0.648, P< 0.001, improved integrated discrimination 0.036, 95% CI, 0.011 to 0.062, P< 0.01) of myocardial injury cases, and achieved higher net benefit in decision curve analysis.
Conclusion: The risk stratification and anesthesia management of high-risk patients are essential. The addition of intraoperative variables to the baseline predictive model improved the performance of the overall model of myocardial injury and helped anesthesiologists screen out the patients at the greatest risk for myocardial injury and adjust anesthesia strategies.
Keywords: prediction model, myocardial injury, thoracic surgery, cardiovascular risk, hsTnT
Introduction
Myocardial injury after non-cardiac surgery (MINS) has been defined as postoperative troponin elevation caused by myocardial ischemia within 30 days after surgery, and it does not require ischemic characteristics.1 It is estimated that one out of every seven surgical patients over 45 years old with an increased risk of perioperative cardiovascular (CV) events suffered from MINS.2 In the largest cohort study of cardiovascular events in patients undergoing non-cardiac surgery (VISION), the incidence of MINS after thoracic surgery was 19.8%.3 Troponin increased during the perioperative period is an essential indicator of poor prognosis in patients, which will increase the risk of death within 30 days after surgery and is independently related to the increase in mortality.4–6 A cohort study of 3085 patients showed that the higher postoperative troponin level was independently related to the lower self-reported score of Health-Related Quality of Life (HRQoL) at one-year follow-up.7
Pathological and physiological causes of MINS are varied, and the imbalance of oxygen supply or demand is considered the main cause of MINS.8 The patients undergoing thoracic surgery are aging gradually. During one-lung ventilation (OLV) in thoracic surgery, the increase of pulmonary vascular resistance and pulmonary artery pressure may lead to acute cardiovascular changes, which may trigger excessive contraction of myocardium and lead to the increase of troponin.9 However, up to 82% of myocardial injuries are asymptomatic,5 and most occurred within 1–2 days after surgery. The majority of patients were still using self-controlled analgesia pumps or sedative drugs, which makes the symptoms of myocardial injury more difficult to identify. Sinus tachycardia, hypotension, nausea, and other manifestations of myocardial ischemia may be mistaken for complications such as atelectasis, hypovolemia, or drug side effects.10 The consensus statement issued by the European Society of Cardiology/American College of Cardiology/American Heart Association/World Heart Federation suggested that routine postoperative troponin measurement should be used as a valuable strategy to identify MINS.11,12 Therefore, it is crucial to stratify the risk of patients with high cardiovascular risk so as to identify the high-risk patients who may need further examination and more intensive monitoring and support. The Revised Cardiac Risk Index (RCRI), commonly used to predict cardiac complications, has been proven to be independently related to MINS and is helpful in guiding postoperative troponin monitoring. It has been widely used in the past 20 years, because it is simple and easy to implement.13,14 Polygenic Risk Scores (PRS) can also gradually improve the ability to predict MINS.15 Additionally, some studies have revealed a poor correlation between the National Surgical Quality Improvement Program (NSQIP) and MINS.16
Several risk factors have been proven to be related to MINS, such as preoperative anemia, the duration of surgery, three or more complications, atrial fibrillation, etc.2,4,17 However, compared with the model composed entirely of preoperative variables, it is unclear whether and how the increase of intraoperative variables will affect the baseline prediction model of MINS after thoracic surgery. Accurate prognosis information is crucial for patients and doctors to make the best health-related and life decisions.18 Therefore, in this study, we will establish a baseline prediction model of myocardial injury in thoracic patients with high cardiovascular risk after thoracic surgery and develop another model containing intraoperative variables to determine whether the intraoperative data improve our ability to identify MINS in patients with high cardiovascular risk.
Materials and Methods
Participants
This prospective research included 298 patients with high cardiovascular risk who underwent elective thoracic surgery to understand the occurrence and progress of MINS. This study was conducted at the Affiliated Hospital of Xuzhou Medical University from May 2022 to October 2022. This study complies with the Declaration of Helsinki, has been approved by the Clinical Trial Ethics Committee of the Affiliated Hospital of Xuzhou Medical University on 9 May 2022 (XYFY2022-KL126-01), and was registered at the Chinese Clinical Trial (ChiCTR2200059926).
Researchers screened eligible patients before the operation. Eligible patients were over 45 and must satisfy at least one of the following criteria: 1. Coronary artery disease; 2. Peripheral arterial disease; 3. Stroke OR 4. Any two of the following seven conditions (a-g): a). Over 70 years old; b). History of congestive heart failure; c). Cerebrovascular diseases; d). Hypertension; e). Diabetes and currently taking oral hypoglycemic drugs or insulin; f). Smoking; g). Preoperative creatinine >2.0 mg/dl. Patients who meet one of the following criteria will be excluded: 1. Sepsis; 2. Using inotropic drugs; 3. Severe heart failure; 4. History of asthma. Patients who met one of the following criteria were eliminated from the trial: 1. Voluntary withdrawal; 2. Operation cancelled; 3. Myocardial injury is caused by non-ischemic causes such as pulmonary embolism and myocarditis. 4. Biomarker is not measured once after the operation.
Data Collection
All patients had obtained written informed consent before the operation. Before the experiment started, we planned to collect demographic (age and sex) and anthropometric (body mass index, BMI) data, preoperative complications (including hypertension, diabetes, coronary heart disease, peripheral arterial disease, cerebrovascular disease, chronic renal failure, chronic heart failure, chronic obstructive pulmonary disease), smoking, laboratory examination (hemoglobin, troponin, arterial oxygen partial pressure), and preoperative medication. In addition, we collected the American Society of Anaesthesiologists physical status (ASA physical status) and Age-adjusted Charlson Comorbidity Index (ACCI). The patients’ RCRI scores were counted, and our patients’ RCRI scores were ≥2. Intraoperative data include duration of anesthesia, duration of surgery, one-lung ventilation time, duration of leaving operating room, cumulative duration of intraoperative hypotension (IOH), blood loss, infusion volume of crystalloid fluid, and colloid fluid, variables related to anesthesia management during operation (dosage of narcotic drugs and vasoactive drugs), type of surgery and operative posture. The duration of leaving operating room is defined as the time from the end of the surgery to leaving the anesthesia recovery room. We measured the non-invasive blood pressure and invasive arterial blood pressure and recorded the blood pressure of each patient every 20 seconds during the whole operation. The cumulative duration of IOH is defined as the duration that the intraoperative blood pressure is 20% lower than the basal blood pressure.
Study Outcomes
The primary outcome was postoperative myocardial injury, defined as postoperative hsTnT >20 to <65 ng/L, and the absolute change is at least 5 ng/L or hsTnT level of at least 65 ng/L.19 We measured hsTnT on postoperative days 1~3, and the highest postoperative measurement allowed the diagnosis of MINS, which was considered to be the occurrence of MINS. MINS is not considered to have occurred if the hsTnT increase was due to non-ischemic causes, including congestive heart failure, pulmonary embolism, aortic valve disease, and sepsis.
Sample Size
The sample size of this experiment was not recalculated. We included all patients who met the inclusion criteria in the analysis to maximize the statistical ability. Our primary outcome is the incidence of MINS. According to the principle of events per variable, we think that at least 10 outcome events should be included in each predictor variable. Therefore, the required sample size was a minimum of 50 patients presenting with MINS (5 predictors).
Statistical Analysis
Firstly, we divided patients into groups according to whether MINS occurred and described the characteristics of variables, respectively. Continuous variables were visually assessed for normal distribution using histograms and pp-plots, and the homogeneity of variance was tested by Levene test. The continuous variables with normal distribution were reported as mean (SD) and were compared by Student’s t-tests. The non-normal distribution data were reported as median (IQR, [range]) and were compared by Mann–Whitney U-tests. The categorical variables were reported as counts (percentages) and were compared by χ2 or Fisher’s exact tests.
We used the Least Absolute Shrinkage and Selection Operator (LASSO) method to select non-zero characteristic factors, risk factors associated with MINS were selected from the raw data, and the complexity of the model was controlled by a series of parameters.20 Risk factors were taken as independent variables and MINS as dependent variables, and multivariate logistic regression was used to build a baseline model with preoperative variables. Then, a second model with baseline and intraoperative variables was established using the same criteria above. We used the Variance Inflation Factor (VIF) to evaluate the collinearity of all risk factors, a VIF ≥10 indicated strong multicollinearity. The discrimination of the model was evaluated by the area under the receiver operating characteristic curve (AUC), and the calibration of the model was evaluated by Hosmer–Lemeshow test. The final model calibration is a calibration curve formed by visualizing the results of goodness-of-fit test, showing actual incidence and predicted incidence.
The AUC and DeLong tests were used to compare the ability of the two models to distinguish MINS from non-MINS. The reclassification ability of the model was evaluated by the Net Reclassification Index (NRI) and Integrated Discrimination Improvement (IDI), which indicate the net proportion of patients with improved risk classification. We use continuous NRI for preliminary analysis, because it is considered a more objective method to compare various studies. For patients with MINS, this can be explained by the increase of true positive rate. For patients without MINS, this can be explained by the decrease of false positive rate, so as to find a better model to predict MINS.
The calibration between models was tested by the likelihood ratio test, Akaike Information Criterion (AIC), Bayesian Information Criterion (BIC), and Nagelkerke R2, Brier Score. Prediction model with smaller AIC and BIC values has better fitting and calibration. Not only the fitting of the model is improved but also the penalty term is introduced so that the model parameters are as few as possible, which helps to reduce the possibility of over-fitting. The Decision Curve Analysis (DCA) was also carried out to evaluate the effectiveness of the two models, that is, the probability level of patients choosing to receive treatment, and compared the net benefits of the models within a series of reasonable thresholds. In any given threshold, a greater net benefit is better. The clinical impact curve (CIC) was drawn to evaluate the benefit ratio of the model. We used 1000 bootstrap samples for internal verification to evaluate the robustness of our model.
Statistical analysis was performed using SPSS statistical software version 26.0 (IBM) and R version 4.2.1 (R Foundation for Statistical Foundation, Vienna, Austria). Among all analyses, P-values <0.05 were considered statistically significant.
Results
Preoperative and Intraoperative Characteristics of Patients
We recruited 308 patients with increased risk of CV and finally included 298 patients in the analysis, of whom 94 (31.5%) had MINS. The baseline characteristics of the two groups of patients are provided in Table 1. Patients with MINS are more likely to be elderly men and obese. Although there is no significant difference in the incidence of complications such as hypertension and diabetes between the two groups, the incidence of MINS is higher in patients with an ACCI score of 5. In addition, there are more people who smoke in patients with MINS, and the preoperative baseline value of hsTnT was also higher (Supplementary Figure 1).
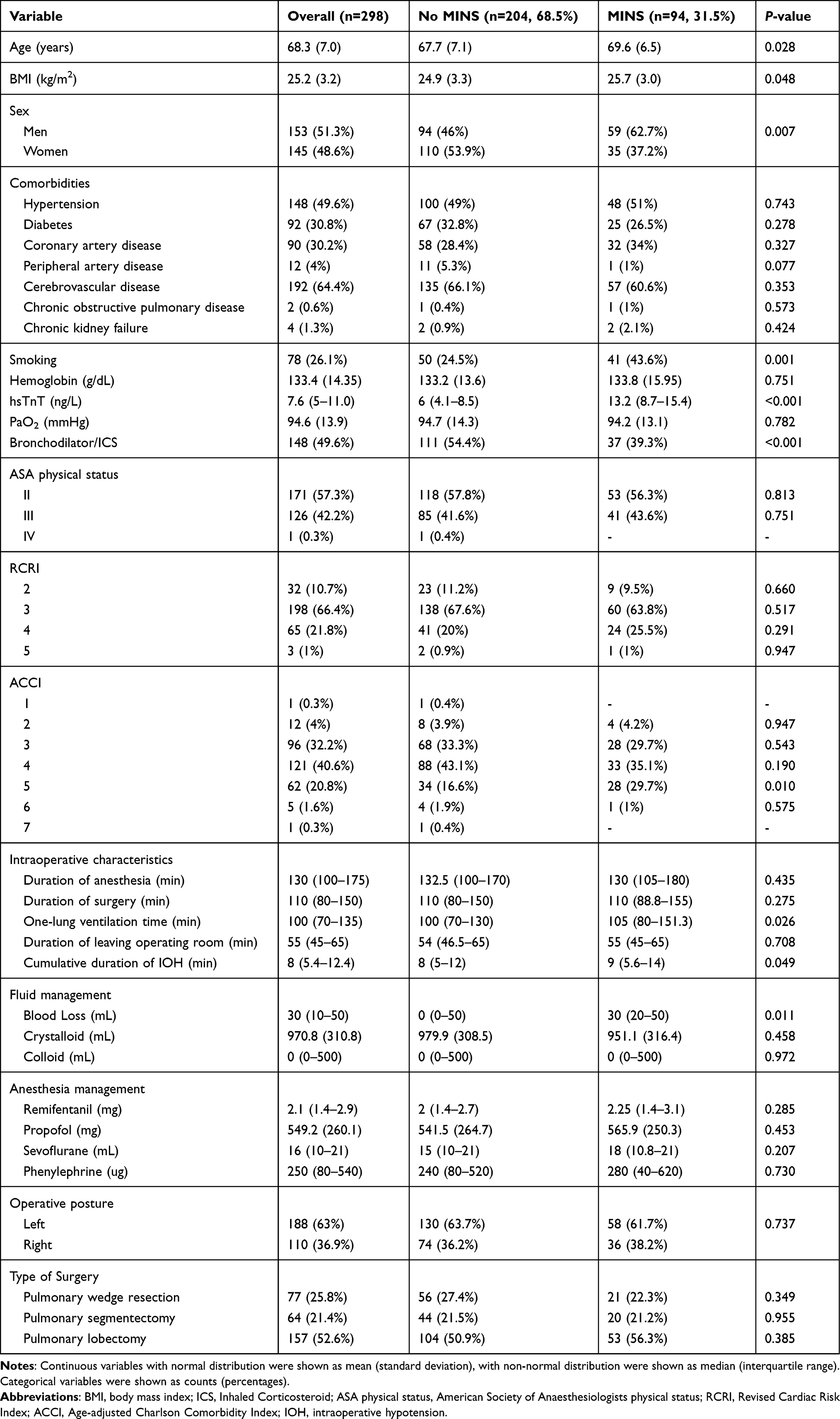 |
Table 1 Comparison of Baseline and Intraoperative Characteristics Between Patients |
There are also differences in intraoperative variables between the two groups. Although the duration of surgery and anesthesia in the two groups of patients were not much different, the patients with MINS experienced longer one-lung ventilation time, longer cumulative duration of IOH, and more blood loss.
Establish Baseline and Intraoperative Prediction Models
We used LASSO regression to identify five potential risk factors: preoperative factors include age ≥65 years old, obesity, smoking, preoperative hsTnT, and intraoperative risk factors include one-lung ventilation time (Supplementary Table 1, Supplementary Figure 2). Univariate analysis showed that preoperative use of bronchodilators and ICS could reduce the incidence of postoperative myocardial injury. However, considering that other hospitals do not necessarily use bronchodilators and ICS before thoracic surgery, other studies have not confirmed that they are independently related to MINS. We decided not to include bronchodilators and ICS in LASSO regression. Multivariate logistic regression showed that these five risk factors were statistically significant with MINS. Therefore, we established a baseline model including preoperative risk factors and an intraoperative model including all risk factors (Table 2). The AUC of the baseline model was 0.931, and the AUC of the intraoperative model was 0.940 (Figure 1A). The calibration curve showed that the calibration of the model is good (Figure 1B). The final intraoperative model was represented by the nomogram in Figure 2.
 |
Table 2 Multivariate Logistic Regression Analysis of Baseline Model and Intraoperative Model |
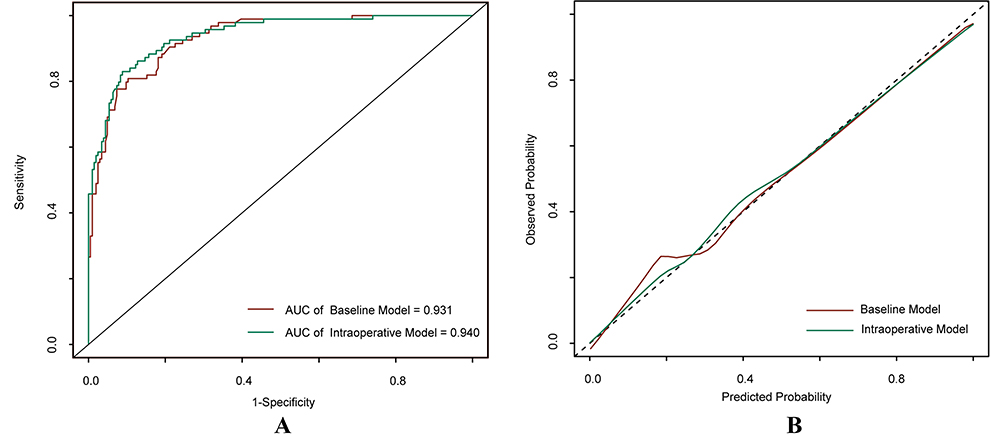 |
Figure 1 The receiver operating characteristic (ROC) curve and calibration curve. Notes: (A) Receiver-operating characteristic (ROC) curve of baseline model and intraoperative model. The AUC of baseline model was 0.931 (95% CI, 0.903–0.959). The AUC of intraoperative model was 0.940 (95% CI, 0.913–0.967), an increase of 0.009. (B) Calibration curve of baseline model and intraoperative model. |
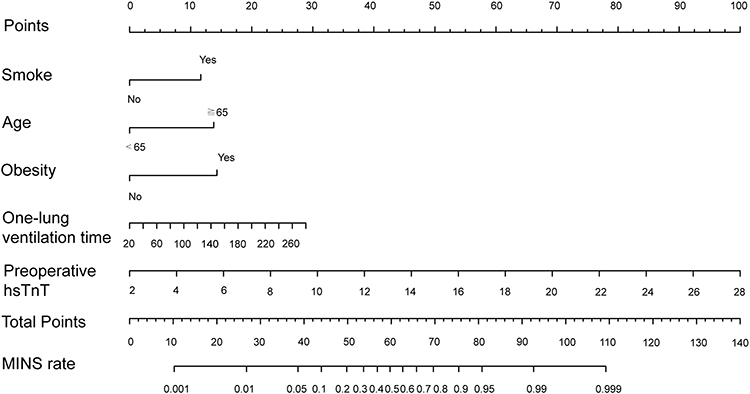 |
Figure 2 Nomogram for intraoperative predictive model of MINS. Notes: Nomogram for perioperative estimation of MINS risk. The first step of using nomogram is to find the position of each variable on the corresponding axis, draw a line on the point axis, add the points of all variables, and draw a line on the total point axis to determine the MINS rate at the lower line of nomogram. |
Improvement of Prediction Model by Intraoperative Variables
For the baseline model that included only preoperative risk factors, the AUC was 0.931 (95% CI, 0.903–0.959). With the addition of intraoperative factors in the baseline model, AUC increased to 0.940 (95% CI, 0.913–0.967), an increase of 0.009 (P for change = 0.141, Table 3). Although the DeLong test showed that the difference between the two models is not statistically significant, the likelihood ratio test showed that the intraoperative model fits better when the intraoperative factors are added (P < 0.001). The AIC and BIC values of the intraoperative model were 180.92 and 203.11, which were smaller than the baseline model and improved the fitting of the model. Nagelkerke R2 and Brier scores also showed that the fitting and calibration of the intraoperative model were better (Table 3). The reclassification of patients with MINS increased by 8.5% (95% CI, −0.153–0.376), and that of patients without MINS increased by 32.4% (95% CI, 0.162–0.550). The overall improvement of net reclassification was significant (continuous NRI = 0.409, 95% CI, 0.169–0.648, P<0.001), and IDI was 0.036 (95% CI, 0.011–0.062). Decision curve analysis can be seen from Figure 3A. With the increase of threshold probability, the net benefit of the model will decrease. According to the prediction results of the intraoperative model, the performance of the model is better under other threshold probabilities, except that the threshold probability is very small, and the performance of the model is always better than that of the baseline model (Figure 3A). The CIC analysis showed that the clinical effective rates of the two models are similar (Figure 3B). When the threshold probability is greater than 80%, the prediction model determines that the high-risk population of MINS is highly matched with the actual population with MINS.
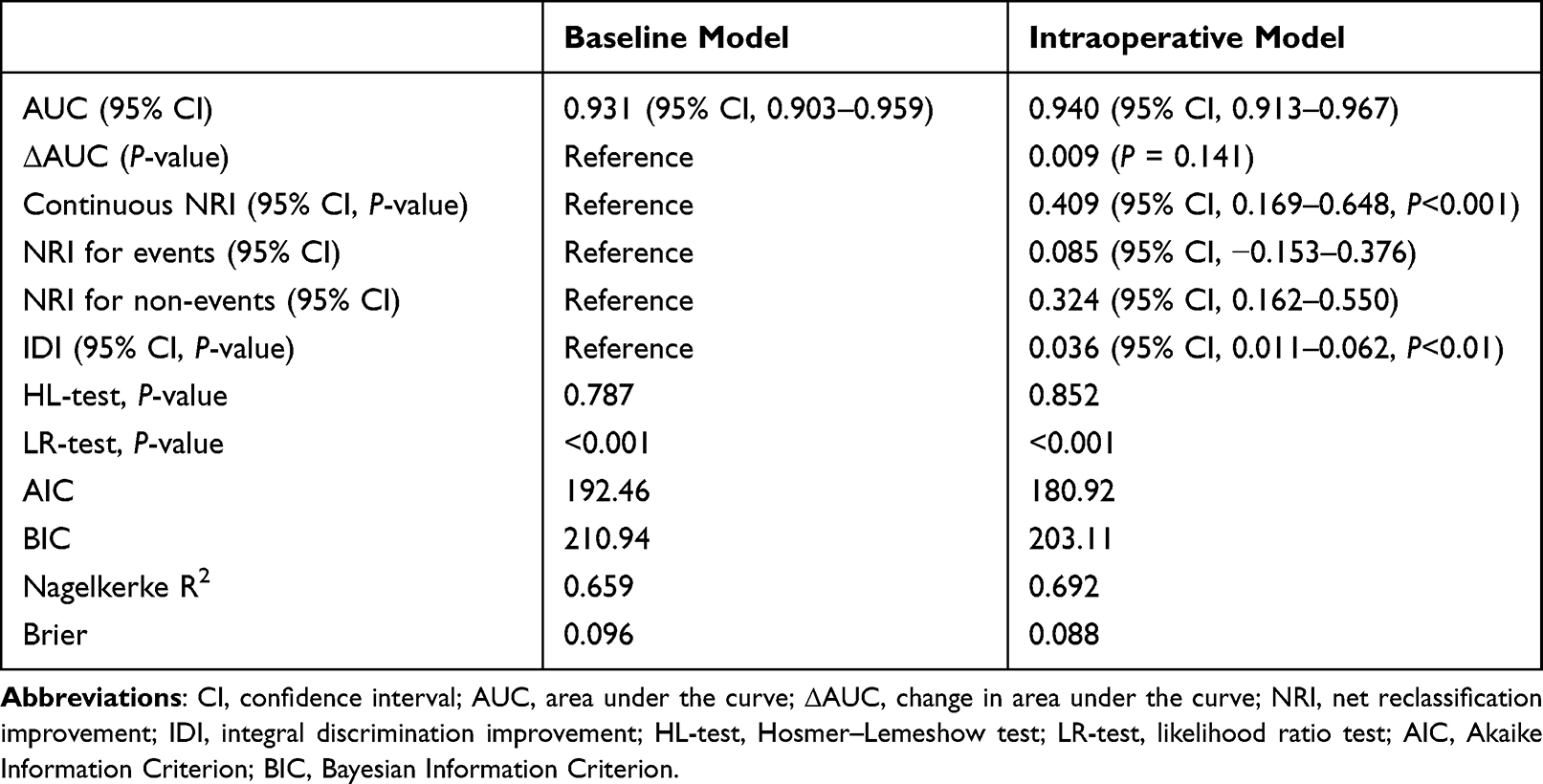 |
Table 3 Additional Performance Metrics of Intraoperative Model Compared with Baseline Model |
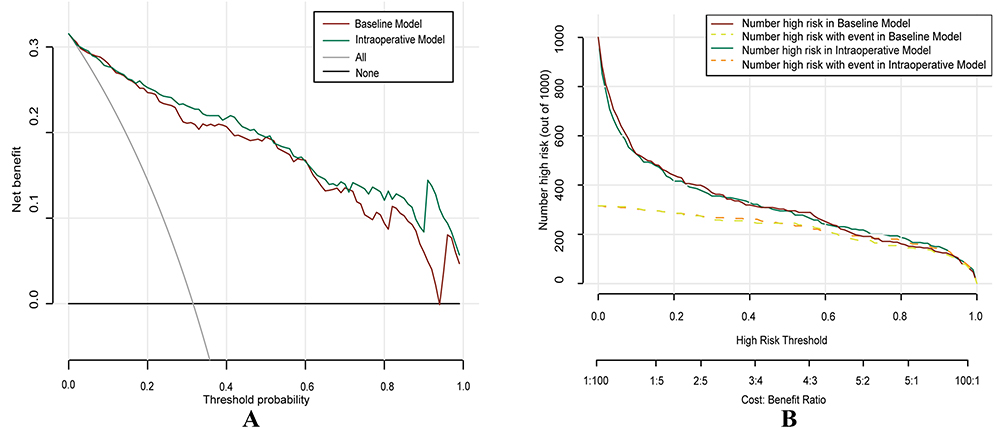 |
Figure 3 Decision curve and clinical impact curve. Notes: (A) Decision curve was used for assessing the net benefit of using models with or without MINS. (B) Clinical impact curve was used for assessing the clinical effective rates of the two models. |
Internal Verification
The bootstrapping internal verification showed the C-index of the baseline model was 0.926, and the C-index of the intraoperative model was 0.933. The performance of internal verification is similar.
Discussion
In this prospective study of myocardial injury in patients with high cardiovascular risk undergoing thoracic surgery, we found that age ≥65 years old, obesity, smoking, preoperative hsTnT, and one-lung ventilation time were independent predictors of MINS. Compared with the baseline model containing routine preoperative risk factors (such as demographics, complications, laboratory examination, etc.), the predictive model with intraoperative risk factors has the better predictive ability for MINS and moderately improves the ability to distinguish and reclassify patients with MINS. These variables are significantly related to the risk of MINS, indicating that intraoperative data can better help us predict the risk of MINS after surgery.
Our research did not emphasize the role of individual risk factors but focused on the overall prediction and examined the overall impact of risk factors in the context of MINS. Compared with the baseline model, the intraoperative model has better discrimination. Although the absolute change of AUC may seem small, AUC is an insensitive indicator to evaluate the impact of newly added risk factors. Because the AUC of the baseline model is already very large, it will be very difficult to improve it when the risk forecast is significantly improved. Even if there is no statistical difference between the two models, there is no doubt that the intraoperative model has a strong predictive ability. However, NRI and IDI showed that adding intraoperative data could improve the risk reclassification of patients with MINS. The decision curve analysis can also support the improvement of intraoperative model performance. Our findings supplement previous studies, which usually do not consider the influence of intraoperative factors on MINS. Intraoperative blood transfusion, intraoperative hypotension, and blood loss, which are the risk factors of perioperative adverse cardiovascular events.21,22 We also found the existence of changeable risk factors, such as smoking and one-lung ventilation time. Targeted support can improve the prognosis of patients. For example, advising patients to quit smoking in advance, shortening the time of one-lung ventilation as much as possible during the surgery, and intermittently giving both lungs ventilation can be considered the steps to prevent MINS. Preoperative anemia, duration of surgery, RCRI, and hsTnT are also proven to be risk factors for MACCE.23,24 Although there is no evidence-based guideline to support any preoperative strategy to improve MINS, enhancing hemodynamic monitoring, blood management, and optimization of cardiovascular drugs can improve the perioperative management of anesthesiologists.4
In our study, patients with high preoperative troponin are more likely to have myocardial injury after surgery, which may be because most of them have cardiovascular complications. In a multivariate model, the risk of myocardial injury is increased in patients with preoperative high hsTnT, and this risk will be enlarged if hsTnT is further increased, which is consistent with our results. Chew et al supported increasing hsTnT in RCRI to identify high-risk patients, so as to improve the value of preoperative risk stratification.4 A previous study showed that, in addition to the increase in preoperative hsTnT level, the risk of adverse cardiovascular events gradually increased when the level of perioperative hsTnT changed.17 However, when the changes of hsTnT during perioperative period are considered, preoperative measurement alone cannot provide information on acute perioperative events. Although the advantage of informing patients about risks before the operation is lost to some extent, the information obtained can be used to determine the postoperative troponin measurement. Therefore, we suggest that hsTnT should be monitored routinely after operation.
Our multivariate regression analysis showed that the probability of MINS increased in patients older than 65 years. Sixty-four percent of our patients are over 65 years old, and almost all of them have preoperative hypertension or coronary artery history. Most experts agreed that for all patients over 65 years old and those over 45 years old with at least one cardiovascular risk factor, postoperative troponin monitoring is required.25 A recent study showed that overweight is inversely related to postoperative mortality, while underweight and obesity are positively related to mortality. This phenomenon persists during long-term follow-up.26 Our multivariate regression analysis also found that obesity was independently related to MINS. Smoking was also found to be an independent risk factor for MINS in an observational study.9 Smoking can cause an increase of secretion in the trachea, and long-term smoking may cause pulmonary fibrosis and atrophy, which can easily cause alveolar infection and pulmonary vascular injury. The relationship between smoking and MINS is complex, and it may also be related to inflammatory reactions and airway remodeling, so it probably cannot be reduced to simple indicators. These relationships need to be further explored.
There are few studies to observe the correlation between one-lung ventilation time and MINS during thoracic surgery. During OLV in thoracotomy, blood is redistributed to the ventilated side and non-operative lung due to gravity and increased pulmonary vascular resistance. Hypoxic pulmonary vasoconstriction and the increase of pulmonary vascular resistance will lead to excessive contraction of myocardium, which will lead to the increase of troponin.27,28 In our study, there was no difference in the duration of surgery and anesthesia between the two groups, while the patients with longer one-lung ventilation time were more likely to have postoperative myocardial injury. Our study found for the first time that shortening the time of one-lung ventilation during operation may be beneficial to myocardial injury. In a preoperative clinical model to predict myocardial injury with a large sample size, age, vascular surgery, and ASA scores III and IV were identified as three independent preoperative predictors of MINS.2 Compared with our experiment, the most significant difference may be due to the study population and the type of operation. We included people with high cardiovascular risk, and thoracic surgery has a special physiological state, which explains why our model included new risk factors.
The RCRI is a commonly used clinical risk assessment tool for cardiac complications. The VISION study found that RCRI is not enough to guide MINS monitoring.16 In an analysis of the predictors of adverse events within 30 days after non-cardiac surgery, low-risk RCRI (1 variable) underestimated the incidence of MINS and death in this population. The National Surgical Quality Improvement Program (NSQIP) was proved to have a poor correlation with MINS.14,29 We collected ACCI and RCRI scores before the operation. The results showed that ACCI scores were strongly correlated with MINS in univariate analysis. The more patients with ACCI score of 5, the greater the risk of MINS. Although there is no correlation in the multivariate model, we can still refer to it. ACCI also needs to be combined with other prediction tools and biomarkers to predict MINS accurately.
Our predictive model, as a simple tool, can not only be used to identify patients with middle and high risk of MINS but also be used as a simple guide for anesthesiologists to manage MINS. Our model does not simply classify patients into high-risk or low-risk but continuously and comprehensively manages the risks of MINS. Our prediction model is easy to use and suitable for patients with cardiovascular risk factors, but our findings may not be suitable for relatively healthy people. Another advantage of our model is that it includes intraoperative parameters so that anesthesiologists have the opportunity to prevent MINS during surgery. Our study also has some limitations. As a single-center experiment, our results may not be applicable to other races. Our experiment also needs external verification, but the relationships established in our study are generally acceptable. The relationship between our predicted variables and MINS may be complicated and nonlinear. Future analysis may benefit from alternative methods that can explain these relationships, such as spline function. Our analysis focused on specific intraoperative variables, but there may be other related factors to be considered, such as cardiac output, arrhythmia, hypertension, temperature, etc.
Conclusions
In summary, our study found that the addition of intraoperative variables to the baseline predictive model improved the performance of the overall model of myocardial injury and helped anesthesiologists screen out the patients at the greatest risk for MINS and adjust anesthesia strategies. The risk stratification and anesthesia management of high-risk patients are essential. Further studies are required to validate our findings.
Abbreviations
MINS, myocardial injury after non-cardiac surgery; CV, cardiovascular; HRQoL, Health-Related Quality of Life; OLV, one-lung ventilation; RCRI, Revised Cardiac Risk Index; PRS, Polygenic Risk Scores; NSQIP, National Surgical Quality Improvement Program; BMI, body mass index; ASA, American Society of Anaesthesiologists; ACCI, Age-adjusted Charlson Comorbidity Index; IOH, intraoperative hypotension; LASSO, Least Absolute Shrinkage and Selection Operator; VIF, Variance Inflation Factor; AUC, area under the receiver operating characteristic curve; ROC, receiver operating characteristic; NRI, Net Reclassification Index; IDI, Integrated Discrimination Improvement; AIC, Akaike Information Criterion; BIC, Bayesian Information Criterion; DCA, Decision Curve Analysis; CIC, clinical impact curve; ICS, inhaled corticosteroid; MACCE, Major Adverse Cardiac and Cerebrovascular event.
Data Sharing Statement
The datasets used and/or analysed during the current study are available from the corresponding author on reasonable request.
Acknowledgments
The authors would like to sincerely thank Dr XF Huang for statistical analysis support and Prof. JD Liu for valuable advice on study design.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Disclosure
The authors state that they have no known competitive financial interests or personal relationships, which may affect the work reported in this article.
References
1. Botto F, Alonso CP, Chan MT, et al. Myocardial injury after noncardiac surgery: a large, international, prospective cohort study establishing diagnostic criteria, characteristics, predictors, and 30-day outcomes. Anesthesiology. 2014;120:564–578.
2. Serrano AB, Gomez-Rojo M, Ureta E, et al. Preoperative clinical model to predict myocardial injury after non-cardiac surgery: a retrospective analysis from the MANAGE cohort in a Spanish hospital. BMJ Open. 2021;11:e045052. doi:10.1136/bmjopen-2020-045052
3. Shelley B, Glass A, Keast T, et al. Perioperative cardiovascular pathophysiology in patients undergoing lung resection surgery: a narrative review. Br J Anaesth. 2022;2:43.
4. Chew MS, Puelacher C, Patel A, et al. Identification of myocardial injury using perioperative troponin surveillance in major noncardiac surgery and net benefit over the Revised Cardiac Risk Index. Br J Anaesth. 2022;128:26–36. doi:10.1016/j.bja.2021.10.006
5. Humble CAS, De HS, Chew MS. Expert consensus on peri-operative myocardial injury screening in noncardiac surgery. Eur J Anaesthesiol. 2021;38:569–570. doi:10.1097/EJA.0000000000001497
6. Hallqvist L, Mårtensson J, Granath F, Sahlén A, Bell M. Intraoperative hypotension is associated with myocardial damage in noncardiac surgery: an observational study. Eur J Anaesthesiol. 2016;33:450–456. doi:10.1097/EJA.0000000000000429
7. Mol KHJM, van Lier F, Liem VGB, Stolker RJ, Hoeksm SE. Immediate postoperative high-sensitivity troponin T concentrations and long-term patient-reported health-related quality of life: a prospective cohort study. Eur J Anaesthesiol. 2020;37:680–687. doi:10.1097/EJA.0000000000001234
8. Neumann JT, Weimann J, Sörensen NA, et al. A Biomarker Model to Distinguish Types of Myocardial Infarction and Injury. J Am Coll Cardiol. 2021;78:781–790. doi:10.1016/j.jacc.2021.06.027
9. González-Tallada A, Borrell-Vega J, Coronado C, et al. Myocardial Injury After Noncardiac Surgery: incidence, Predictive Factors, and Outcome in High-Risk Patients Undergoing Thoracic Surgery: an Observational Study. J Cardiothorac Vasc Anesth. 2020;34:426–432. doi:10.1053/j.jvca.2019.08.014
10. Devereaux PJ, Goldman L, Yusuf S, Gilbert K, Leslie K, Guyatt GH. Surveillance and prevention of major perioperative ischemic cardiac events in patients undergoing noncardiac surgery: a review. Can Med Assoc J. 2005;173:779–788. doi:10.1503/cmaj.050316
11. Fleisher LA, Fleischmann KE, Auerbach AD, et al. 2014 ACC/AHA Guideline on Perioperative Cardiovascular Evaluation and Management of Patients Undergoing Noncardiac Surgery: a Report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. Circulation. 2014;1:130.
12. Duceppe E, Parlow J, MacDonald P, et al. Canadian Cardiovascular Society Guidelines on Perioperative Cardiac Risk Assessment and Management for Patients Who Undergo Noncardiac Surgery. Can J Cardiol. 2017;33:17–32. doi:10.1016/j.cjca.2016.09.008
13. Ruetzler K, Smilowitz NR, Berger JS, et al. Diagnosis and Management of Patients With Myocardial Injury After Noncardiac Surgery: a Scientific Statement From the American Heart Association. Circulation. 2021;144:144. doi:10.1161/CIRCULATIONAHA.120.052788
14. Roshanov PS, Sessler DI, Chow CK, et al. Predicting Myocardial Injury and Other Cardiac Complications After Elective Noncardiac Surgery with the Revised Cardiac Risk Index: the VISION Study. Can J Cardiol. 2021;37:1215–1224. doi:10.1016/j.cjca.2021.03.015
15. Douville NJ, Surakka I, Leis A, et al. Use of a Polygenic Risk Score Improves Prediction of Myocardial Injury After Non-Cardiac Surgery. Circ Genomic Precis Med. 2020;13:e002817. doi:10.1161/CIRCGEN.119.002817
16. Vasireddi SK, Pivato E, Soltero E, et al. Postoperative Myocardial Injury in Patients Classified as Low Risk Preoperatively Is Associated With a Particularly Increased Risk of Long--Term Mortality After Noncardiac Surgery. J Am Heart Assoc. 2021;10:e019379. doi:10.1161/JAHA.120.019379
17. Puelacher C, Lurati Buse G, Seeberger D, et al. Perioperative Myocardial Injury After Noncardiac Surgery: incidence, Mortality, and Characterization. Circulation. 2018;137:1221–1232. doi:10.1161/CIRCULATIONAHA.117.030114
18. Alba AC, Agoritsas T, Walsh M, et al. Discrimination and Calibration of Clinical Prediction Models: users’ Guides to the Medical Literature. JAMA. 2017;318:1377. doi:10.1001/jama.2017.12126
19. Pedersen SS, Holse C, Mathar CE, et al. Intraoperative Inspiratory Oxygen Fraction and Myocardial Injury After Noncardiac Surgery: results From an International Observational Study in Relation to Recent Controlled Trials. Anesth Analg. 2022;135:1021–1030. doi:10.1213/ANE.0000000000006042
20. Norrish G, Ding T, Field E, et al. Development of a Novel Risk Prediction Model for Sudden Cardiac Death in Childhood Hypertrophic Cardiomyopathy (HCM Risk-Kids). JAMA Cardiol. 2019;4:918. doi:10.1001/jamacardio.2019.2861
21. De HS, Staender S, Fritsch G, et al. Pre-operative evaluation of adults undergoing elective noncardiac surgery: updated guideline from the European Society of Anaesthesiology. Eur J Anaesthesiol. 2018;35:407–465. doi:10.1097/EJA.0000000000000817
22. Abbott TEF, Pearse RM, Archbold RA, et al. A Prospective International Multicentre Cohort Study of Intraoperative Heart Rate and Systolic Blood Pressure and Myocardial Injury After Noncardiac Surgery: results of the VISION Study. Anesth Analg. 2018;126:1936–1945. doi:10.1213/ANE.0000000000002560
23. Weber M, Luchner A, Seeberger M, et al. Incremental value of high-sensitive troponin T in addition to the revised cardiac index for peri-operative risk stratification in non-cardiac surgery. Eur Heart J. 2013;34:853–862. doi:10.1093/eurheartj/ehs445
24. Humble CAS, Huang S, Jammer I, Björk J, Chew MS. Prognostic performance of preoperative cardiac troponin and perioperative changes in cardiac troponin for the prediction of major adverse cardiac events and mortality in noncardiac surgery: a systematic review and meta-analysis. PLoS One. 2019;14:e0215094. doi:10.1371/journal.pone.0215094
25. Khanna AK, Gan TJ. Myocardial Injury After Noncardiac Surgery—Slightly Heavier May Be Better. Anesth Analg. 2021;132:957–959. doi:10.1213/ANE.0000000000005348
26. Tjeertes EK, Hoeks SE, Beks SB, et al. Obesity – a risk factor for postoperative complications in general surgery? BMC Anesthesiol. 2015;15:112. doi:10.1186/s12871-015-0096-7
27. Kowalewski J, Brocki M, Dryjański T, Kaproń K, Barcikowski S. Right ventricular morphology and function after pulmonary resection. Eur J Cardiothorac Surg. 1999;15:444–448. doi:10.1016/S1010-7940(99)00032-9
28. Van Mieghem W, Demedts M. Cardiopulmonary function after lobectomy or pneumonectomy for pulmonary neoplasm. Respir Med. 1989;83:199–206. doi:10.1016/S0954-6111(89)80032-0
29. Costa MCDBG, Furtado MV, Borges FK, et al. Perioperative Troponin Screening Identifies Patients at Higher Risk for Major Cardiovascular Events in Noncardiac Surgery. Curr Probl Cardiol. 2021;46:100429. doi:10.1016/j.cpcardiol.2019.05.002
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.