")
Back to Journals » Substance Abuse and Rehabilitation » Volume 8
Intranasal naloxone and related strategies for opioid overdose intervention by nonmedical personnel: a review
Authors Lewis CR, Vo HT, Fishman M
Received 1 March 2017
Accepted for publication 29 June 2017
Published 11 October 2017 Volume 2017:8 Pages 79—95
DOI https://doi.org/10.2147/SAR.S101700
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Li-Tzy Wu
Christa R Lewis,1,2 Hoa T Vo,1 Marc Fishman1,3
1Maryland Treatment Centers, Baltimore, MD, USA; 2Department of Psychology, Towson University, Towson, MD, USA; 3Department of Psychiatry, Johns Hopkins School of Medicine, Baltimore, MD, USA
Abstract: Deaths due to prescription and illicit opioid overdose have been rising at an alarming rate, particularly in the USA. Although naloxone injection is a safe and effective treatment for opioid overdose, it is frequently unavailable in a timely manner due to legal and practical restrictions on its use by laypeople. As a result, an effort spanning decades has resulted in the development of strategies to make naloxone available for layperson or “take-home” use. This has included the development of naloxone formulations that are easier to administer for nonmedical users, such as intranasal and autoinjector intramuscular delivery systems, efforts to distribute naloxone to potentially high-impact categories of nonmedical users, as well as efforts to reduce regulatory barriers to more widespread distribution and use. Here we review the historical and current literature on the efficacy and safety of naloxone for use by nonmedical persons, provide an evidence-based discussion of the controversies regarding the safety and efficacy of different formulations of take-home naloxone, and assess the status of current efforts to increase its public distribution. Take-home naloxone is safe and effective for the treatment of opioid overdose when administered by laypeople in a community setting, shortening the time to reversal of opioid toxicity and reducing opioid-related deaths. Complementary strategies have together shown promise for increased dissemination of take-home naloxone, including 1) provision of education and training; 2) distribution to critical populations such as persons with opioid addiction, family members, and first responders; 3) reduction of prescribing barriers to access; and 4) reduction of legal recrimination fears as barriers to use. Although there has been considerable progress in decreasing the regulatory and legal barriers to effective implementation of community naloxone programs, significant barriers still exist, and much work remains to be done to integrate these programs into efforts to provide effective treatment of opioid use disorders.
Keywords: intranasal naloxone, Narcan Nasal Spray, take-home naloxone, naloxone autoinjector, naloxone, naloxone review, FDA implications
Introduction
The increasingly widespread abuse of prescription opioids and heroin has resulted in a well-documented health care crisis due to dramatically increased incidence of fatal or near-fatal opioid overdose-induced respiratory depression. In 2014, the USA alone had 1.9 million people with a substance use disorder involving prescription pain relievers and 586,000 had a substance use disorder involving heroin.1 Within this population, 18,893 overdose deaths were related to prescription pain relievers and 10,574 overdose deaths were related to heroin, corresponding to nearly 63% of all lethal drug overdoses in the USA in 2014.2 Although the introduction of abuse-deterrent technology in prescription opioids and changes in prescribing patterns appear to have stabilized the morbidity and mortality rates associated with prescription opioids, there has, nevertheless, been a striking increase in the rate of heroin-associated fatalities.2
Following the initial use of naloxone as an opioid antagonist that was invaluable for reversing opioid toxicity occurring in a hospital setting3,4 (e.g., following surgical anesthesia and/or analgesia), emergency departments began adopting it for treatment of opioid overdoses in patients who had been transported to the hospital. The success of such efforts obviously depended on the timely arrival of the patient after emergency medical services (EMS) had dispatched an ambulance to the scene of the overdose and returned with the patient. Due to numerous failures to resuscitate overdose patients under these circumstances, efforts were made to establish the effectiveness of field or prehospital administration of parenteral naloxone by first responders with medical training (typically, advanced life-support trained paramedics).5–7 Although an improvement over in-hospital treatment, the overall success of this intervention was recognized to be significantly limited, again, by the time delay following contact to initiation of treatment, in addition to the reluctance of overdose observers to contact EMS due to fear of arrest. These problems, together with difficulties of EMS personnel in obtaining vascular access due to damage from repeated intravenous (IV) drug use and the risk of potentially life-threatening infections due to needlestick injuries,8 were critical driving forces in the exploration of intranasal (IN) drug delivery9 as an alternative, needle-free approach to administration of naloxone.10,11 As discussed in this review, the effort to develop, test, and distribute IN naloxone delivery systems progressed sporadically over a number of years, but then increased and intensified considerably over the last decade. The present review discusses the history of this effort and the controversies that have emerged up to the most recent developments in the USA that include the belated endorsement of the effort by the National Institute of Drug Abuse (NIDA) and the recent provision of regulatory guidelines by the US Food and Drug Administration (FDA). This culminated in the first regulatory approval, in late 2015, of an IN naloxone kit for community use by medically untrained first responders. A parallel effort to provide another “take-home” formulation also emerged over the same time period, recently culminating in an FDA-approved intramuscular (IM) naloxone autoinjector for layperson use and is therefore also considered in this review. Finally, issues associated with the dissemination of both off-label and FDA-approved take-home naloxone (THN) in the USA (including state and Federal legislative efforts) are discussed along with the outstanding need to integrate this effort with the provision of effective treatments for opioid use disorders (OUDs), in order for this intervention to develop long-term public health impact.
Materials and methods
Our objective with this review is to provide a historical context for the development of IN naloxone and related strategies for the treatment of opioid overdoses, in addition to an assessment of the current status of this area. There is a particular focus on IN naloxone because of its practical combination of efficacy, administrator safety, and wide dissemination. There is also a particular focus on developments in the USA, in part due to the diversity of approaches being used that are broadly encompassed by the term “take-home naloxone”, which includes both improvised and FDA-approved IN naloxone kits as well as IM injectable naloxone for FDA-approved manual or autoinjector administration. This is a narrative review of selected relevant literature, emphasizing a health services perspective, rather than a comprehensive review of the full pharmacologic, clinical, legal, and economic bibliography.
Our literature search included the key terms “intranasal naloxone”, “Narcan Nasal Spray”, and “take-home naloxone”, a term that has been widely used to refer to both IN and IM naloxone. Computer-based searches were conducted using Google and Google Scholar, PubMed, fda.gov, and uspto.gov, which were supplemented by a manual search with a focus on reference lists in clinical reports and review papers. Reports and communications from both governmental and nongovernmental organizations and newspaper articles reporting developments in the adoption of IN naloxone were also searched. Articles not written in English were excluded.
We used our iterative search procedures branching out from our primary keyword searches, which generated lists of references from individual publications, coalescing to a core set of relevant references that turned up repeatedly in iterative cross-searching. Articles considered to be redundant with respect to other references were eliminated. Space limitations for this review preclude a more comprehensive listing of references, which can be found in the cited earlier reviews.12–32 The final sample for this review included the pioneering proof-of-concept preclinical study of IN naloxone; a group of case studies and case series, and retrospective observational studies along with prospective clinical trials of IN naloxone; pharmacokinetic studies comparing IN naloxone to parenteral formulations; issued US patents of two companies competing for FDA approval of different formulations of IN naloxone; transcripts and presentations from FDA-sponsored public meetings to discuss IN naloxone (including FDA advice on studies and data needed for regulatory approval); published FDA reviews of the one product that was approved; a substantial number of narrative reviews and commentaries addressing the balance of risks and benefits of both “off-label” and approved IN naloxone; and news articles and published communications from both governmental and nongovernmental organizations regarding naloxone policy issues. The text is supplemented with more comprehensive summary tables, several of which were adapted from other recent systematic reviews with a more limited focus, with the intention of providing balance as well as a discussion of broader issues that were not the subject of these earlier reviews.
Results
Utility and practical limitations of parenteral formulations of naloxone
Naloxone is a competitive opioid receptor antagonist with a high affinity for the mu-opioid receptor subtype, the primary site of action for the rewarding and addictive effects of opioids, as well as their lethality in depressing respiration.3,4 A decade following its synthesis at DuPont, naloxone HCl was approved by the FDA in 1971 as an injectable formulation under the brand name Narcan® and has since been widely used in emergency settings to reverse the effects of opioid toxicity, with minimal adverse effects apart from the induction of opioid withdrawal symptoms.3,4 This formulation of naloxone was approved only for IV, IM, and subcutaneous (SQ) administration to treat opioid overdose, with an initial dose of 0.4–2 mg followed by repeated doses up to 10 mg, and as with most other parenteral medications, usually only highly trained health care providers (e.g., paramedics) were permitted to administer it. However, because opioid-induced respiratory depression can progress rapidly to death, the practical effectiveness of injectable naloxone for reversal of in-the-field opioid overdoses has been limited by legal constraints on layperson access and delayed administration due to bystander reluctance to call EMS or delays in EMS arrival that result in significant morbidity or mortality in community settings. In such settings, without trained health care providers and adequate ventilatory support, there is a brief window before hypoxic injury becomes irreversible, and the unavailability of naloxone during this critical period can result in overdose fatalities.
The rapidly growing magnitude of the opioid overdose public health crisis in the USA and elsewhere has driven an increasingly widespread community-based effort to distribute THN kits to individuals considered to be likely to witness an overdose. While this effort has sometimes included provision of naloxone vials with syringes for parenteral (e.g., IM) administration, this approach has engendered concerns about the need for extensive training, as well as the risk of needlestick injury resulting in transmission of HIV and hepatitis. These difficulties, in addition to legal restrictions on the use of injectable naloxone by individuals having less than advanced paramedic training, led to efforts to develop a needle-free IN naloxone device that could be widely distributed and used “off-label” by medically untrained family members, friends, or bystanders to rescue opioid overdose victims (for previous reviews of IN naloxone and THN more broadly, see references12–32). This effort has intensified considerably over the last decade, and in the USA, it is unprecedented for having occurred in the absence of FDA regulatory guidance or pharmaceutical industry involvement until the last few years.
Gradual emergence of IN naloxone as an alternative method of delivery
In 1984, the IN administration of naloxone was studied pharmacokinetically in rats and compared with IV administration of the drug.33 The nasal bioavailability was found to be essentially 100%, equivalent to IV administration, peaking within 3 min. The first human clinical study of IN naloxone, in 1992, sought to use it as the basis of a test to identify opiate dependence in human subjects by precipitating withdrawal.34 In 1994, Loimer et al35 advanced the concept of use for clinical intervention by comparing the efficacy of IN naloxone to that of the established IV and IM routes of administration in 17 opiate-dependent patients. Administration of IN naloxone was reported to be as effective as the IV route in reversing opiate adverse effects. The authors suggested that IN naloxone administration provided the additional benefit of a wide margin of safety for medical staff as well as patients, particularly in emergency situations with regard to venipuncture-associated infection risks.
The notion of THN to reduce overdose risk was introduced shortly thereafter, in 1996, with Strang et al36 making the case for provision of prefilled naloxone syringes to opiate misusers at high risk of overdose, such as those leaving the emergency room against medical advice following naloxone-based resuscitation from an overdose. Surprisingly, this proposal did not make reference to IN naloxone, despite the earlier work of Loimer et al35 indicating its apparent utility in opiate-dependent patients in an emergency treatment setting. No further developments with IN naloxone appeared until 2002, when two landmark papers set the stage for a more intensive and organized effort to convincingly demonstrate the comparative efficacy of IN naloxone in treating opioid overdoses.
The first of these papers was a small case series report of six patients with acute heroin overdose successfully treated in a hospital emergency department with IN naloxone and ventilatory support.37 All six patients were reported to return to adequate spontaneous respiration within 2 min, with a median of 50s, following naloxone doses ranging from 0.8 to 2 mg. Although critical procedural details, such as drug concentration, volume, and method of IN administration, were not reported, these investigators advocated the value of IN naloxone and claimed proof of concept for life-saving administration by a wide variety of minimally trained community workers without the risk of needlestick injury.
Also, in 2002, Barton et al38 conducted the first prehospital study of the efficacy of IN naloxone, based on the rationale that 1) opioid addicts who inject drugs often have poor venous access, resulting in a loss of valuable time trying to gain IV access if multiple attempts are required; 2) IM and SQ routes of administration can be effective, but result in a much slower rate of absorption than IV administration, with a correspondingly longer time period for the patient to respond; and 3) EMS personnel are at risk for inadvertent needlestick injuries when attempting to place IV lines or give IM or SQ injections in the field with a patient population at increased risk of blood-borne diseases such as hepatitis C and HIV. IN naloxone was administered using a disposable mucosal atomizer device attached to a 1 mL syringe to spray 1 mL into each nostril, for a total IN dose of 2 mg naloxone. In this naturalistic study, 10/12 patients (83%) with suspected opioid overdose responded to IN naloxone with a significant improvement in the level of consciousness within 2–6 min.
Subsequently, Barton et al39 reported the results of an extension of the foregoing nonrandomized prospective trial in which patients suspected of opioid overdose received IN naloxone.38 Of the 52 patients who responded to naloxone by either IN or IV administration, 83% responded to 2 mg IN naloxone, although 7 (16%) of these responders were subsequently given IV naloxone due to declining response. Of the naloxone-sensitive patients, 17% failed to respond to IN naloxone, but then responded to IV naloxone. These results, while promising, also appeared to indicate a subpopulation of opioid overdose patients who might not benefit from IN naloxone. A majority of the IN naloxone nonresponders were noted by the paramedics to have nasal abnormalities (e.g., IN bleeding), while the IN naloxone responders were reported to not have these problems, again suggesting a potential limitation and possible treatment matching criterion for this route of administration.
Controlled randomized clinical trials of IN naloxone
Kelly et al40 reported the first prospective, randomized clinical trial to assess the comparative efficacy of IN and IM naloxone in patients (N=155) undergoing treatment of suspected opioid overdose in a prehospital setting. Without blinding, patients were randomly assigned to receive naloxone (2 mg in 5 mL) injected IM or the same solution delivered IN with a mucosal atomizer device. Patients receiving IM naloxone exhibited a significantly higher response rate (spontaneous respiration within 8 min) than IN patients (82% vs 63%), and also responded significantly faster than the IN group (means of 6 vs 8 min), with a trend for a lower proportion needing rescue IM naloxone (13% vs 26%). Together, these observations suggest lower bioavailability of IN compared to IM naloxone, which the authors suggested was due to the use of a volume of fluid (5 mL) that was too large for ready absorption by the surface of the nasal passages. In support of this explanation, the authors noted an earlier study38 that had used the same dose, but in a lower volume (2 mg in 2 mL solution; 1 mL per nostril), and reported a higher response rate (91%) to IN naloxone than that achieved in their study.
In a subsequent study,41 these investigators then compared the effectiveness of a more concentrated naloxone formulation (2 mg/mL) given IN (0.5 mL =1 mg into each nostril) vs IM in an open-label randomized trial of 172 patients suspected of heroin overdose.41 In contrast to the previous study, there were no significant differences between the IM and IN groups in rates of response within 10 min (77.5% vs 72.3%) or mean response times (8.0 vs 7.9 min). Thus, this study was considered to provide convincing evidence that IN naloxone is a safe and effective intervention for initial management of heroin overdose and support for the authors’ view that IN naloxone represents an opportunity for wider distribution of naloxone for administration by nonmedical community responders as well as a needle-free option for trained first responders.
More recently, a randomized trial was performed with 100 patients presenting to the ER with symptoms of opioid overdose, comparing the effects of 0.4 mg IN with 0.4 mg IV.42 Patients who had been administered IN naloxone demonstrated improvements in consciousness that were statistically significant compared to those patients who received standard IV treatment. However, this significance may not be reflecting a clinically meaningful difference. Similar improvements in respiratory rate and arterial oxygen saturation were observed with both treatments. A difference in time to respond to naloxone was in the direction expected, though, with a significantly longer mean response time in the IN group (2.56 min) compared to the IV group (1.48 min). Regardless, it was concluded that IV and IN naloxone are both effective treatments for reversing opioid-induced respiratory depression and impaired consciousness.
Supportive retrospective studies of IN naloxone
In a retrospective study43 of 154 patients with suspected narcotic overdose treated by EMS in the prehospital setting, similar rates of clinical response were observed in a group of patients treated with 2 mg IN naloxone (66%) compared to a historical comparison group given 1 mg IV or IM naloxone (56%). More patients in the IN group received two doses of naloxone (34% vs 18%), and although the mean time between naloxone administration and clinical response was longer for the IN group (12.9 vs 8.1 min), the mean time from patient contact to clinical response was not significantly different between the IN and IV groups (20.3 vs 20.7 min). The investigators concluded that IN naloxone appears to be a useful and potentially safer alternative because of the difficulty and potential hazards in obtaining IV access in many patients with narcotic overdose. These findings were confirmed in a similar EMS retrospective study44 of 344 patients, with 2 mg IN naloxone compared to 0.4–2 mg IV naloxone.
Taken together, the foregoing studies support the overall conclusion that IN naloxone is generally effective in reversing the lethal respiratory depressive effects of mu-opioids, as summarized in Table 1 (adapted from several earlier reviews16,19,25). While these studies have certain methodological limitations, collectively, their overall conclusion of effectiveness of IN naloxone appears valid. Although this conclusion has been contested by some investigators, the strength of the data was sufficient to motivate pharmaceutical companies to initiate the costly efforts to develop IN naloxone delivery systems that could meet rigorous FDA standards, as discussed in the following section.
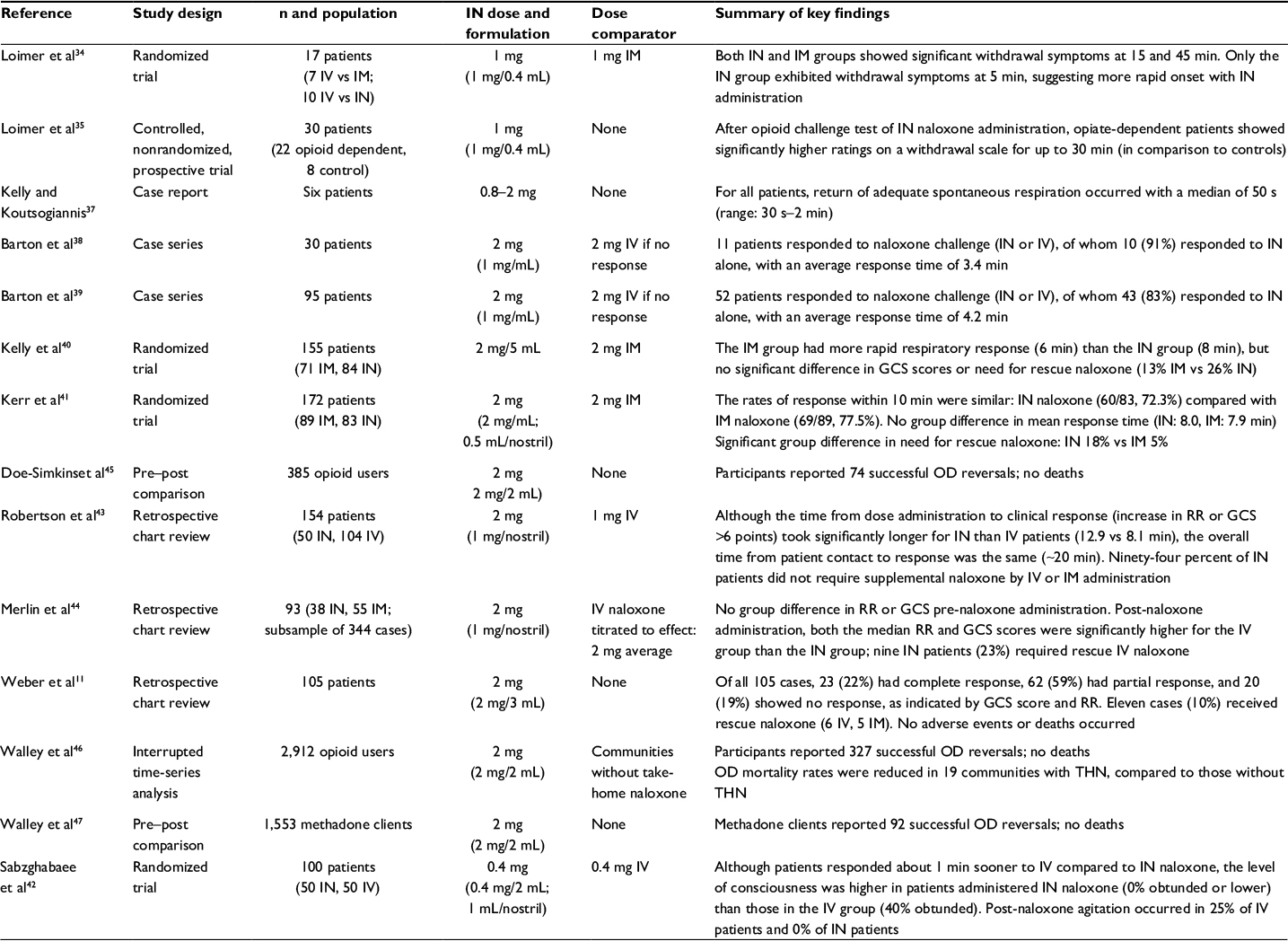 | Table 1 Comparative studies of IN and parenteral naloxone formulations in patients Notes: The table is updated and modified from tables of studies compiled in previous reviews;16,19,25 summaries of the listed studies differ from those previously provided in several cases, as deemed appropriate based on clinical as well as statistical significance. Abbreviations: GCS, Glasgow Coma Scale; IM, intramuscular; IN, intranasal; IV, intravenous; OD, overdose; RR, respiratory rate; THN, take-home naloxone. |
FDA approval of IN naloxone: process, outcome, and controversy
All of the foregoing clinical research on IN naloxone utilized off-label, essentially improvised IN delivery devices to deliver varying volumes and doses of naloxone, with little evidence that these parameters had been optimized. However, over the period of time when this research had been conducted, there was no evidence of support from the NIDA or regulatory guidance from the US (FDA) regarding the necessary characteristics of an approvable IN naloxone delivery system. However, with the increasing momentum of community-level efforts to increase the distribution and timely availability of THN, including IN naloxone, in response to the public health crisis of opioid overdose fatalities, there was increasing pressure to develop new IN naloxone products for formal FDA approval. At a 2012 joint meeting held by the FDA with NIDA and the Centers for Disease Control and Prevention (CDC),48 the FDA provided its initial guidance concerning the results of studies required to support the approval of an IN naloxone product.49 Fundamentally, the requirement was that an approvable IN naloxone product must exhibit essentially the same (or better) pharmacokinetic properties compared to the already approved parenteral naloxone product, with evidence of effective usability without prior training. Under FDA regulations, a product meeting these criteria can be approved without additional efficacy studies, based on the predictive validity of the required pharmacokinetic profile. Although the validity of the pharmacokinetic bioequivalency criterion is based on core principles of pharmacology and seldom challenged, it was not without controversy in this case, as discussed next.
Controversy over “off-label” vs approved IN naloxone
Prior to the FDA approval of the first IN naloxone product, there was considerable controversy in the field about criteria for approval between those who advocated caution, careful scrutiny, and waiting for full efficacy and safety data, vs those who advocated proceeding more quickly with limited but presumably adequate data in light of the urgent public health need.25–31 Strang, the original proponent of “take-home” injectable naloxone,36 defended the case for a cautious approach based on the assessed merits and problems associated with off-label provision of improvised IN naloxone, and provided recommendations for the testing of such products prior to widespread public distribution.25,31 Noting the evidence from some studies that single nasal administration of naloxone may have a lower success rate than IM or IV naloxone, Strang argued that the context of emergency care is fundamentally different from a family member or peer with a nasal spray naloxone kit. In brief, the paramedic teams are able to give a naloxone injection when the nasal spray fails, while no fallback treatment exists in the community setting for the family member or caregiver with only the nasal spray. Although the point was acknowledged, the counterargument was that the fallback would be of little use if the victim had died waiting for the arrival of the paramedic. Other arguments concerned the criterion of usability of the IN product by the care provider (especially nonmedically trained persons), with many investigators advocating that broader deployment was of paramount importance, to prevent patients from dying as a consequence of withholding a substantially effective treatment that had not yet been optimized.
A key part of the debate concerned pharmacological technical criteria for evaluation of efficacy of IN vs approved naloxone injection products. In particular, questions were raised about whether FDA pharmacokinetic criteria of bioequivalence (e.g., the dose-normalized maximal plasma concentration, the time to reach it, and the duration of time at or above this concentration) were alone sufficient to prove pharmacodynamic equivalence and efficacy of IN compared to injectable naloxone products. Questions were also raised about the logistical and ethical issues related to conducting efficacy trials in patients at risk of dying from opioid overdoses. But if human lab data would be used instead of clinical trials, should elicitation of withdrawal symptoms in opioid-dependent volunteers be considered a surrogate for reversing overdose-induced respiratory depression? What probably swayed the field, and the FDA, ultimately to move more quickly, was the sense of the public health urgency and the need to act practically in response. As summarized by Winstanley,26 “The regulatory barriers to take-home naloxone have been significant, and while we wrestle with questions of superiority of naloxone formulations and who is allowed to administer these drugs, people are dying and they will continue to die”.
Meanwhile, as these debates were taking place, the FDA reviewed applications for two IN naloxone products and then approved only one of them, Narcan Nasal Spray, substantially on the basis of pharmacokinetic equivalence to the approved starting dose of IM naloxone, without requiring additional efficacy studies. The study data provided by Adapt Pharma, Inc., for its Narcan Nasal Spray are reviewed and summarized in FDA documents50 and reported in detail in a peer-reviewed publication.51 In brief, based on both pharmacokinetic and human ease-of-use studies, a 4 mg dose delivered in a single device (0.1 mL) was selected as the final product, with a package of two devices approved by the FDA in accordance with the criteria described above. The study data provided to the FDA by AntiOp, Inc., for its IN naloxone product are not publicly available, since it was not approved; however, comparison of the bioavailability profiles of the two products in the corresponding US patents52,53 suggests that the AntiOp product did not meet the pharmacokinetic criteria for bioequivalency to the existing parenteral formulation of naloxone. This may be due in part to the selection of a lower dose of naloxone, 1.8 mg, by AntiOp, compared to 4 mg for the approved Adapt Pharma product. However, the FDA has most recently approved a 2 mg version of Narcan Nasal Spray with the restriction that prescription is limited to opioid-dependent patients who are considered to be at risk for severe opioid withdrawal symptoms in situations where there is a low risk for accidental or intentional opioid exposure by household contacts.54 Several competing products are in late stages of development or regulatory review at this time, so the landscape of approved THN products is expected to continue evolving over the next few years. It is safe to predict that pharmacokinetic evidence of equivalency or superiority to the smallest approved parenteral dose of naloxone will remain the cornerstone of approvability. The key to bioequivalence success was using a more concentrated solution in a smaller volume, which minimizes the loss of solution (and resulting nonabsorption of drug) due to the low retention capacity of the nasal cavity.
Naloxone IM autoinjector
As noted before, the original concept of THN espoused by Strang36 in the UK was predicated on the distribution of injectable naloxone, and subsequent efforts to establish THN were standardized based on the government-approved parenteral formulation distributed with syringes.57 This method was also employed in US distribution efforts, but legal complications and concerns about needlestick injury risks resulted in a preference for off-label IN naloxone. However, the effectiveness of parenteral naloxone established the current standard of care for treatment of opioid overdose; so, in parallel with the commercial efforts to develop approvable IN naloxone delivery systems, a NIDA-supported competing effort was undertaken to develop a naloxone autoinjector. A clear precedent had been established by the success of the Epipen epinephrine autoinjector for layperson emergency treatment of acute, life-threatening anaphylaxis. The Evzio naloxone autoinjector is a preassembled, lightweight, compact, battery-operated, disposable, prefilled device for use in the lateral thigh and is designed for immediate administration, with little to no training, by caregivers of opioid overdose victims outside of a medically supervised setting.58,59 The device provides voice instructions that assist in guiding the user through administration of 2 mg naloxone and seeking further medical care after injection, which involves a retractable needle system that conceals the needle before, during, and after administration, eliminating the risk of caregiver needlestick injury. With strong advocacy by NIDA, Evzio was rapidly approved by the FDA in 2014, prior to the approval of Narcan Nasal Spray the following year.
How the Evzio autoinjector compares to Narcan Nasal Spray
The approved autoinjector and nasal spray had to meet the same FDA regulatory requirements for pharmacokinetic bioequivalence or superiority to the reference product, an IM/SC syringe containing 0.4 mg naloxone, as well as usability and labeling comprehension studies that take into account use scenarios, critical task success, and representative user populations.60 Since both products had to meet the same pharmacokinetic criteria, as well as product safety and usability criteria, it is reasonable to consider the products fundamentally comparable. Evzio’s manufacturer, Kaléo, Inc., has sought to differentiate the autoinjector from off-label IN naloxone in sponsored usability studies, demonstrating its superior performance to the latter device,61 which had to be assembled and operated by untrained or trained volunteers under simulated emergency conditions, using only brief printed directions without diagrams. However, these study directions lack the details and instructional diagrams contained in directions generally recommended for take-home IN naloxone kits,62 compromising the validity of the comparison. Although the study did not compare the autoinjector to the FDA-approved, preassembled IN naloxone device (Narcan Nasal Spray), a recent review article also coauthored by Kaléo employees has, nevertheless, made sweeping claims for the superiority of the autoinjector and its route of administration relative to IN naloxone,63 without clearly differentiating the off-label and approved products. As noted above, since the autoinjector and the approved IN naloxone product both satisfied FDA standards for pharmacokinetic equivalency/superiority, safety, and layperson usability under challenging circumstances, these claims may not be justified, particularly in the absence of a direct comparative study of the two products. They are differentiated by price, however: Narcan Nasal Spray is currently priced at $125, with a discount to $75 for bulk purchasers (e.g., community clinics and first responder organizations), while Evzio has been priced at $3750, with a discount to $360 for patients without government or commercial insurance. Although the manufacturer has a limited program to offer Evzio at no cost to individuals who may be eligible for Medicaid, the cost is likely to remain a barrier to sustainability and scale, especially in economically disadvantaged populations and communities.
The ongoing debate: how much naloxone is enough?
As noted above, the FDA was criticized by some investigators for approving Narcan Nasal Spray based on its current pharmacokinetic standard for approval of naloxone products for use in the community, which requires demonstration of naloxone levels comparable to or greater than the levels achieved with the approved starting dose of 0.4 mg of naloxone, over a comparable time course, when administered by one of the approved, labeled routes of administration (IV, IM, or SQ injection) in adults. At an October 2016 FDA Advisory Committee meeting to discuss the issue of whether the currently approved naloxone dose is adequate or too low,60 a consensus was not reached, in part, because of unknown variability in dose, potency, and half-life of the particular opioid causing an overdose. Although the committee agreed that the risk of not having a high enough dose is much greater than having too much, and that the current standard (0.4 mg) set in 1971 reflected inpatient use rather than use in the community where time to resuscitate may be minimal, only a slight majority of the committee (15 to 13) favored increasing the minimum acceptable naloxone exposure to that comparable to or greater than a higher dose of naloxone injection (i.e., >0.4 mg). Another factor may be the increasing frequency of overdoses with very high potency opioids, such as fentanyl and carfentanyl, which may require higher naloxone doses for reversal. It is presently unclear how the FDA will deal with multiple dose forms of IN naloxone that have been proposed by manufacturers, a source of concern to some members of the committee based on the view that a community-distributed naloxone product should be simplified to a single dose form to avoid confusion.
Intended IN naloxone user populations: lay responders and first responders
There are two main intended user populations for IN naloxone products: lay responders (e.g., a parent, friend, or other family member of a known or suspected opioid overdose victim) who would be responsible for administering naloxone to the patient, and authorized first responders (e.g., firefighters, paramedics, emergency medical technicians, or police officers) who would be responsible for administering naloxone if no one had been able to do so at the time the first responders arrive at the scene. Although the studies of naloxone use by EMS first responders discussed above37–44 focus on the comparative pharmacologic effectiveness of IN naloxone, studies of lay responder use, as discussed below, have more of a health services research focus, emphasizing the distribution and take-home delivery of naloxone.
Lay responders: outcomes of THN programs
The first naloxone distribution program in the USA began in Chicago, in 2001, when the Chicago Recovery Alliance Mobile Van program started community distribution of IM injectable naloxone in very inexpensive ($2.53) generic 10-dose multiuse vials together with unfilled syringes.64 Over the subsequent decade, this program delivered naloxone to 10,211 people, with 1011 reported reversals of opioid overdoses.65 During this time period, efforts to promote the distribution of THN began to spread across the USA, reportedly driven almost entirely by harm reduction advocates, friends and families of overdose victims, and policymakers concerned about the rising rates of overdose in their communities.62
A Harm Reduction Coalition survey analyzed and reported by CDC showed that as of 2010, 188 local naloxone programs in 15 states and the District of Columbia had distributed naloxone to 53,032 individuals and received reports of 10,171 drug overdose reversals.66 A subsequent survey analyzed and reported by CDC indicated that by June 2014, 644 local programs in 30 states and Washington, DC, were responsible for the distribution of 152,283 naloxone kits and 26,453 opioid overdose reversals.67
A recent FDA document60 prepared for the October 2016 Meeting provided a comprehensive review of two recently published systematic reviews referenced as McDonald and Strang32 and Clark et al,19 aimed at assessing the effectiveness of THN programs. Both of these reviews summarized and aggregated germane studies related to community naloxone distribution programs (the USA and otherwise) reporting data on naloxone use and outcomes (overdose reversals, and so on). Although there was substantial variability in how many THN kits were distributed and the percentage subsequently used (0.5%–67%) based on the program being assessed, almost all studies reported very high rates of opioid overdose reversals after THN administration among the instances they were able to track. More specifically, Clark et al19 reviewed 14 studies examining evaluations of 18 community opioid overdose prevention programs that featured bystander naloxone training and distribution that cumulatively reported 1949 naloxone administrations. The mean pooled survival rate was 96% across programs, ranging from 83% to 100%. McDonald and Strang32 reviewed a slightly different, but overlapping set of 22 studies reporting 2336 naloxone administrations with a pooled survival rate of 96%. Incomplete capture of THN administration instances was a consistent methodological limitation in the studies. None of these studies were randomized. Only one study46 had a comparator to survival rate outside of the overdose prevention program, reporting that areas with higher levels of enrollment in the multisite program had lower rates of overdose death after controlling for other factors, using an interrupted time series analysis. McDonald and Strang32 made a persuasive argument that although the studies were only correlational rather than experimental, the overall aggregate evidence meets generally accepted epidemiologic criteria in support of the hypothesis of causation in the effectiveness of THN. The results of these studies, which included both IN and IM forms of THN, are summarized in Table 2 (adapted from previous reviews19,32,60).
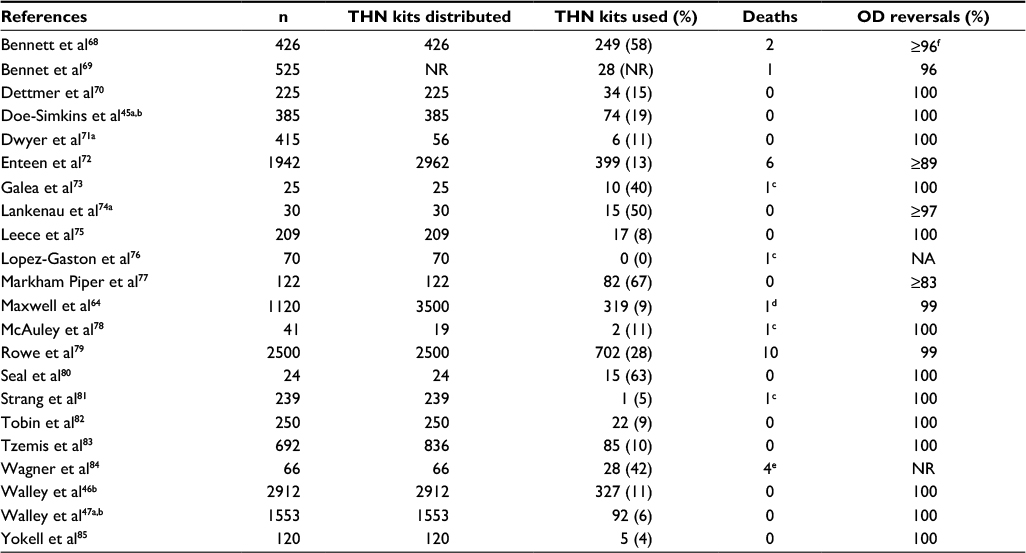 | Table 2 Naloxone kits distributed and used, overdose deaths, and overdose reversals Notes: The table is modified from substantially overlapping tables of studies provided in previous reviews.19,32,60 aNot included in summary measures to avoid (partial) duplication of samples; b2 mg naloxone administered IN (2 mg/2 mL); other studies used different (non-nasal) routes of THN; cnaloxone not administered; dnonopioids present; eunclear if naloxone administered; fwhere applicable, unknown outcomes were counted toward unsuccessful THN administration (as indicated by the ≥ symbol). Abbreviations: IN, intranasal; NA, not applicable; NR, not reported; OD, overdose; THN, take-home naloxone. |
Objections to bystander use of naloxone
Objections to community naloxone distribution and training have been reviewed and addressed elsewhere.86 For example, it has been suggested that providing people who use drugs with the knowledge and medication to respond to opioid overdoses might increase their opioid use or delay entry into addiction treatment by reducing interactions with emergency health care providers and decreasing the risk of adverse consequences of using drugs.87,88 However well intentioned, these concerns are irrelevant if the alternative is nonreversal of overdoses leading to death. Although one relatively small survey of people who inject drugs found that about one-third of respondents anticipated feeling comfortable using more heroin after receiving a naloxone rescue kit,80 no studies of existing Overdose Education and Naloxone Distribution (OEND) programs have demonstrated increased drug use by participants.86 In a series of studies examining drug use outcomes of OEND programs, statistically significant decreases in heroin injection were reported at 6-month follow-up,84 and 53% of trained substance users had decreased drug use at 3 months,73 although a smaller study of trained substance users reported no difference in drug use at follow-up.80 There is considerable variety in the format, content, and thoroughness of the various OEND programs, and evidence of their differential effectiveness suggests that further program improvements are possible, and also points to the need to integrate such programs with effective treatment interventions, as further discussed below. Although there is no evidence to support the view that OEND programs promote illicit drug use,86 some US policymakers still hold to this view; for example, Maine Governor Paul LePage vetoed a bill in April 2016 that would allow pharmacists to dispense naloxone without a prescription, stating that naloxone “does not truly save lives; it merely extends them until the next overdose”.89 The veto was quickly overridden by the state legislature, consistent with the nationwide trend to liberalizing naloxone access laws to combat the current opioid overdose epidemic.90
A further objection to trained bystander use of naloxone has been the belief that once naloxone rescue kits were distributed into the community to people trained in overdose treatment with naloxone, these kits would be further disseminated through social networks to people who were not trained directly by the distribution programs. The objection, then, was that the ability of these untrained potential bystanders to successfully respond to overdoses with naloxone rescue kits is not known. Although the ability of untrained bystanders to successfully use off-label IN naloxone may be brought into question since connection of the atomizer to the naloxone syringe is required, it is difficult to then conclude that overdose victims would be better off if all bystander naloxone were simply unavailable. This objection is less relevant to FDA-approved, fully assembled IN naloxone devices49–51 and IM autoinjectors,58,59 since approval required, in part, experimental demonstration of usability by untrained laypersons.
Another point of controversy has been the question of whether overdose reversal in the field by laypeople will lead to increased refusal of further care, and if so, whether there will be an increase in post-resuscitation delayed respiratory depression and death as a result of the prolonged half-life of certain opioids relative to naloxone. It is a well-described phenomenon that some proportion of persons who receive “prehospital” naloxone are not transported to the hospital emergency department, either because they explicitly refuse the recommendations of first responders or, in the case of layperson administration, bystanders or resuscitated persons are not motivated to call EMS, go to the hospital, or otherwise seek further care.72 In the review by Clark et al,19 the rates of EMS notification by laypersons following naloxone administration in the nine overdose prevention program evaluation articles that reported that particular outcome ranged from 29% to 100%, with six studies reporting a rate less than 50%.
Despite the hypothetical risk that field administration of naloxone without follow-up care may be only transiently effective, with the possibility of reinstatement of the overdose condition, including mortality risk, multiple studies indicate this is generally not the case.72 In a series of 205 cases of refusal of further care following EMS naloxone administration, there was only 1 death (0.5%) within 24 h.91 Even persons who do arrive at the hospital emergency department following field resuscitation may refuse further care by leaving prematurely, raising the same question of hypothetical risk. However, in two series of such patients who left against medical advice, there were no deaths within 12 h of field naloxone administration.92,93 Table 3 summarizes objections to the distribution and use of IN and nonmedical naloxone, with corresponding responses to these objections providing a rationale for such use, and source citations for further detail.
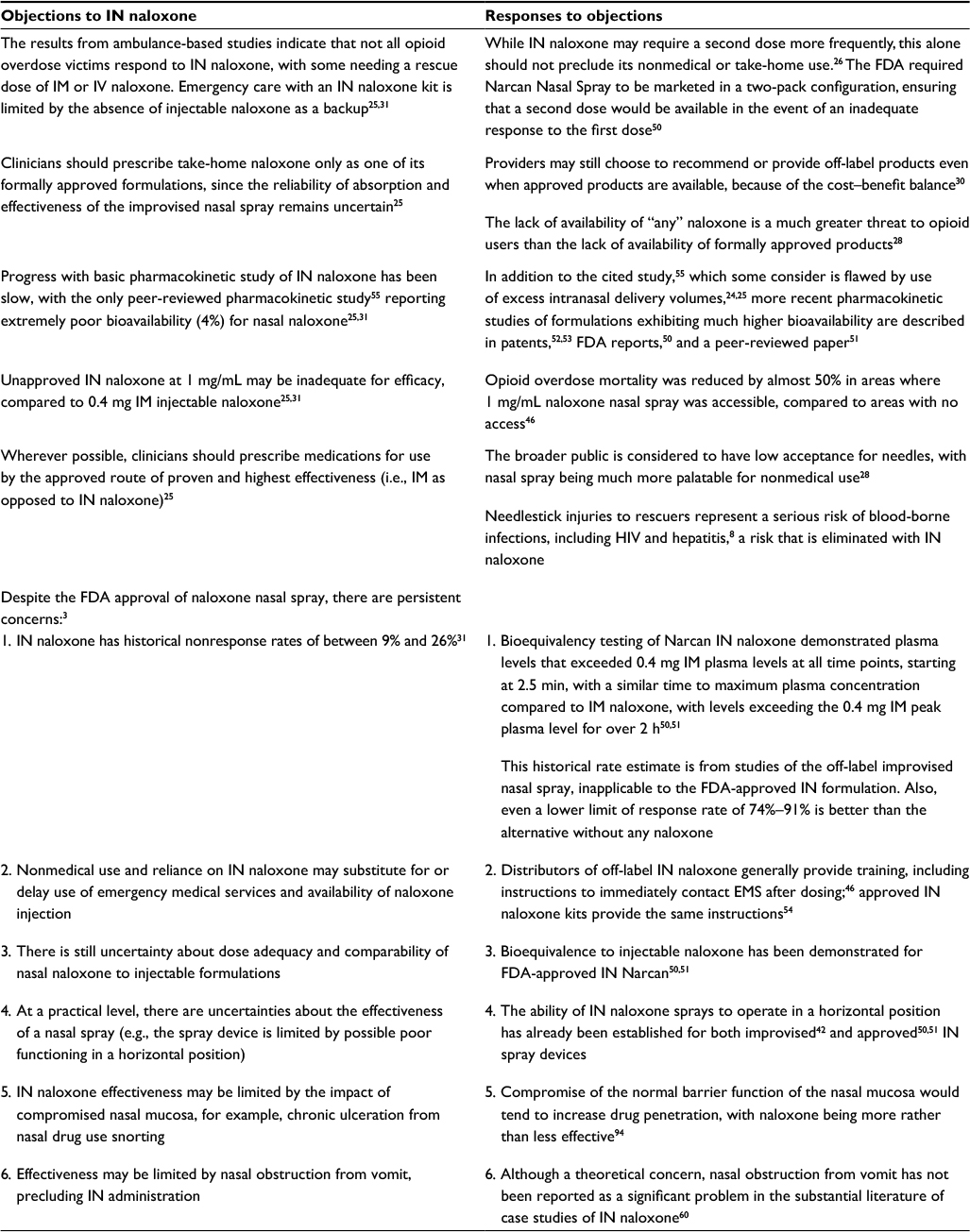 | Table 3 Summary of the debate over IN and nonmedical naloxone Abbreviations: FDA, US Food and Drug Administration; IM, intramuscular; IN, intranasal; IV, intravenous. |
The changing legal landscape for IN or THN
Historically, in the USA, there have been substantial legal barriers to increasing community access or use of naloxone.90,95–98 For example, some physicians have been reluctant to prescribe naloxone because of liability concerns, and even where naloxone is available, bystanders to a drug overdose may be afraid to administer it because of liability concerns, or fail to summon medical assistance for fear of being prosecuted for possession of illegal drugs, or fear arrest for other reasons (e.g., existing warrants or nondrug crimes).
Since most of these barriers are rooted in unintended consequences of laws passed for other purposes, they may be addressed through relatively simple changes to those laws.90,97,98 At the urging of organizations including the US Conference of Mayors, the American Medical Association, and the American Public Health Association, the majority of states have removed some legal barriers to the seeking of emergency medical care and the timely administration of naloxone. In the USA, legislation designed to improve layperson access to naloxone has been passed in all but three states (KS, MT, WY), as of June 2016.98 States enacting this legislation have made it easier for people who might be in a position to assist in an overdose to access naloxone, encourage those individuals to summon emergency responders, or both. In addition, these states have amended their laws to make it easier for medical professionals to prescribe and dispense naloxone, and for lay administrators to use it without fear of legal repercussions.
The need to integrate improved access to naloxone with treatment for OUDs
Although there is increasingly widespread agreement in the USA and internationally, at the community, health care provider, and policymaker levels on the desirability of OEND programs (particularly with the recent FDA approval of both autoinjector and IN devices for untrained laypersons to safely and effectively administer naloxone to reverse acute opioid overdoses), the nationwide implementation of these programs remains a work in progress, awaiting more aggressive funding in an era when such funding may be increasingly constrained. Beyond the effective implementation of these programs to provide reliable and timely reversal of opioid overdoses, there is also widespread agreement that this effort must be integrated with programs to identify and provide effective long-term treatment for individuals with OUDs. At present, medication-assisted treatment (MAT) modalities remain underutilized, despite the evidence of improved health and social outcomes.99 MAT involves the use of a medication, such as methadone or buprenorphine or extended-release naltrexone, to reduce craving and reinforcement of further illicit opioid use, to increase the effectiveness of counseling, behavioral therapies, or other modifying techniques for the treatment of OUDs.100 However, patient access to MAT may not be available due to cost, unavailability of local providers, or other difficulties.99
As noted elsewhere, communities and states can work to improve known deficits in local treatment services, with particular attention to those that offer MAT. At a national level, with the recent passage by Congress of the Comprehensive Addiction and Recovery Act (CARA), the US Department of Health and Human Services can continue to make opioid overdose prevention a priority, as well as expand the use of MAT and lay the groundwork for linking receipt of life-saving naloxone in the community to participation in an MAT program as a step toward achieving an integrated, more effective approach to OUDs, a goal with significant intrinsic challenges.101 Although the effective implementation of such policies at the national level might be expected to meet significant political resistance despite the passage of CARA, due in part to changes in US national funding priorities, it is possible that the still-increasing magnitude of the current opioid overdose crisis will generate sufficient pressure to enable significant progress to be made in coming years.
Conclusion and future research
IN administration of naloxone allows medically untrained people to safely and effectively administer the medication with a substantial likelihood of success in reversing opioid-induced respiratory depression, if the overdose symptoms are observed. There is no need to learn how to administer an injection with aseptic technique, and the absence of a syringe needle eliminates the risk of needlestick injuries that could result in the transmission of infectious blood-borne pathogens. Thus, while THN programs have provided both syringes for IM injection or kits for converting syringes to nasal aerosol devices, and both treatment modalities appear to be similarly effective, there appear to be advantages to using the IN route of administration. Both treatment modalities have been simplified, improved, and standardized by recent FDA approvals of a naloxone autoinjector (Evzio) and IN spray (Narcan Nasal Spray), although relatively high pricing may be a significant disincentive for wider adoption. The lower cost spray may have an advantage in this regard, particularly if government purchases through funding for nationwide initiatives such as CARA turn out to be price-sensitive. Although the last few years have seen striking increases in the distribution capabilities of community naloxone distribution organizations, liberalization of naloxone prescription and use laws, in addition to protective Good Samaritan laws, there is considerable variation from state to state, and the opioid overdose epidemic remains largely unabated in the USA, as well as in other nations.
For many of the concerns raised about IN naloxone, THN, or field use naloxone in general, a compelling response is: “what is the comparator?” On the one hand, if more effective, more definitive interventions are the alternative, then certainly their advantages should be pursued to the extent that is practically possible. On the other hand, if the alternative in the meantime is poor access to any intervention, then the comparator should be “untreated overdose”, and in that case, even a potentially inferior but life-saving intervention that for now improves access with immediate scalability should be pursued. Of course, these approaches are not incompatible and can be staged to avoid “making the perfect become the enemy of the good”. Improved formulations, better distribution and delivery, and especially increased linkages to further addiction treatment should be studied and pursued, without impeding the urgent implementation of the tools we have in hand now.
Future research should explore:
- Comparisons of naloxone delivery methods in the field
- Facilitators of and barriers to use in the field by non-medical personnel
- More rigorous methodologies for assessing the effectiveness of distribution programs including comparators
- Empiric evaluation of the speculation that some users might be more imprudent in their use behaviors because of their overconfidence in the availability of naloxone
- Impact of naloxone distribution and training initiatives on entry to, or retention in treatment programs, and other outcomes that are pertinent to the overall medical and social objectives of these programs
- Cost-effectiveness assessments
At present, more widespread distribution of approved IN naloxone can generate additional volume-based cost reductions. In addition, it is clear that opioid overdose mitigation is only one piece of the puzzle, though a critical one, and that meaningful progress will require an integration of this effort with the broader, more difficult goal of transitioning individuals with OUD into effective, widely available treatment programs including medications, which at present remain underfunded and underutilized, despite the evidence of improved health and social outcomes.
Author contributions
Ms Christa Lewis was responsible for conducting the initial literature review, the preparation of the first draft, and the preparation and editing of subsequent drafts. Dr Hoa Vo assisted in outlining and editing the various drafts. Dr Marc Fishman assisted in outlining, editing, and composing the manuscript. All authors contributed toward data analysis, drafting and revising the paper and agree to be accountable for all aspects of the work.
Disclosure
While working on this review paper, the authors were on salary support at Mountain Manor Treatment Center. The authors report no other conflicts of interest in this work.
References
Substance Abuse and Mental Health Services Administration, Center for Behavioral Health Statistics and Quality. Behavioral health trends in the United States: Results from the 2014 National Survey on Drug Use and Health. Rockville, MD: Substance Abuse and Mental Health Services Administration; 2015. Available from: http://www.samhsa.gov/data/sites/default/files/NSDUH-FRR1-2014/NSDUH-FRR1-2014.pdf. Accessed June 24, 2016. | ||
Center for Disease Control and Prevention, National Center for Health Statistics, National Vital Statistics System, Mortality File. Number and age-adjusted rates of drug-poisoning deaths involving opioid analgesics and heroin: United States, 2000–2014. Atlanta, GA: Center for Disease Control and Prevention; 2015. Available from: http://www.cdc.gov/nchs/data/health_policy/AADR_drug_poisoning_involving_OA_Heroin_US_2000- 2014.pdf. Accessed June 24, 2016. | ||
Dahan A, Aarts L, Smith TW. Incidence, reversal, and prevention of opioid induced respiratory depression. Anesthesiology. 2010;112(1):226–238. | ||
Boyer EW. Management of opioid analgesic overdose. N Engl J Med. 2012;367(2):146–155. | ||
Yealy DM, Paris PM, Kaplan RM, Heller MB, Marini SE. The safety of prehospital naloxone administration by paramedics. Ann Emerg Med. 1990;19(8):902–905. | ||
Sporer KA, Firestone J, Isaacs SM. Out-of-hospital treatment of opioid overdoses in an urban setting. Acad Emerg Med. 1996;3(7):660–667. | ||
Belz D, Lieb J, Rea T, Eisenberg MS. Naloxone use in a tiered-response emergency medical services system. Prehosp Emerg Care. 2006;10(4):468–471. | ||
Ratcliffe JM, Lyden JT, Sousa S, Orelien JG, Boal WL, Jagger J. Blood exposure among paramedics: incidence rates from the national study to prevent blood exposure in paramedics. Ann Epidemiol. 2006;16(9):720–725. | ||
Wolfe TR, Bernstone T. Intranasal drug delivery: an alternative to intravenous administration in selected emergency cases. J Emerg Nurs. 2004;30(2):141–147. | ||
Kerr D, Dietze P, Kelly AM. Intranasal naloxone for the treatment of suspected heroin overdose. Addiction. 2008;103(3):379–386. | ||
Weber JM, Tataris KL, Hoffman JD, Aks SE, Mycyk MB. Can nebulized naloxone be used safely and effectively by emergency medical services for suspected opioid overdose? Prehosp Emerg Care. 2012;16(2):289–292. | ||
Robinson A, Wermerling DP. Intranasal naloxone administration for treatment of opioid overdose. Am J Health Syst Pharm. 2014;71(24):2129–2135. | ||
Leavitt SB. Intranasal naloxone for at-home opioid rescue. Pract Pain Manag. 2010;10:42-46. | ||
Lim JK, Bratberg JP, Davis CS, Green TC, Walley AY. Prescribe to prevent: Overdose prevention and naloxone rescue kits for prescribers and pharmacists. J Addic Med. 2016;10(5):300. | ||
Buck ML. Use of intramuscular/subcutaneous and intranasal naloxone products for pediatric opioid overdose. Pediatr Pharmacother. 2016;22(3):1–4. | ||
Ashton H, Hassan Z. Best evidence topic report. Intranasal naloxone in suspected opioid overdose. Emerg Med J. 2006;23(3):221–223. | ||
Wermeling DP. Opioid harm reduction strategies: focus on expanded access to intranasal naloxone. Pharmacother 2010;30(7):627–631. | ||
Wermeling DP. A response to the opioid overdose epidemic: naloxone nasal spray. Drug Deliv Transl Res. 2013;3(1):63–74. | ||
Clark AK, Wilder CM, Winstanley EL. A systematic review of community opioid overdose prevention and naloxone distribution programs. J Addict Med. 2014;8(3):153–163. | ||
World Health Organization. Community management of opioid overdose; 2014. Available from: http://apps.who.int/iris/bitstream/10665/137462/1/9789241548816_eng.pdf?ua=1&ua. Accessed August 18, 2016. | ||
Giglio RE, Li G, Dimaggio CJ. Effectiveness of bystander naloxone administration and overdose education programs: a meta-analysis. Inj Epidemiol. 2015;2(1):1–9. | ||
McAuley A, Aucott L, Matheson C. Exploring the life-saving potential of naloxone: a systematic review and descriptive meta-analysis of take home naloxone (THN) programmes for opioid users. Int J Drug Pol. 2015;26(12):1183–1188. | ||
Mueller SR, Walley AY, Calcaterra SL, Glanz JM, Binswanger IA. A review of opioid overdose prevention and naloxone prescribing: implications for translating community programming into clinical practice. Subst Abuse. 2015;36(2):240–253. | ||
Wermeling DP. Review of naloxone safety for opioid overdose: practical considerations for new technology and expanded public access. Ther Advan Drug Saf. 2015;6(1):20–31. | ||
Strang J, McDonald R, Tas B, Day E. Clinical provision of improvised nasal naloxone without experimental testing and without regulatory approval: imaginative shortcut or dangerous bypass of essential safety procedures? Addiction. 2016;111(4):574–582. | ||
Winstanley EL. Tangled-up and blue: releasing the regulatory chokehold on take-home naloxone. Addiction. 2016;111(4):583–584. | ||
Dietze P, Cantwell K. Intranasal naloxone soon to become part of evolving clinical practice around opioid overdose prevention. Addiction. 2016;111(4):584–586. | ||
Lobmaier PP, Clausen T. Radical red tape reduction by government supported nasal naloxone: the Norwegian pilot project is innovative, safe and an important contribution to further development and dissemination of take-home naloxone. Addiction. 2016;111(4):586–587. | ||
Dale O. Ethical issues and stakeholders matter. Addiction. 2016;111(4):587–589. | ||
Balster RL, Walsh SL. Ensure global access to naloxone for opioid overdose management. Addiction. 2016;111(4):589–590. | ||
Strang J, Mcdonald R. New approved nasal naloxone welcome, but unlicensed improvised naloxone spray kits remain a concern: proper scientific study must accompany innovation. Addiction. 2016;111(4):590–592. | ||
McDonald R, Strang J. Are take-home naloxone programmes effective? Systematic review utilizing application of the Bradford Hill criteria. Addiction. 2016;111(7):1177–1187. | ||
Hussain A, Kimura R, Chong-Heng H, Kashihara T. Nasal absorption of naloxone and buprenorphine in rats. Intl J Pharmaceut. 1984;21(2):233–237. | ||
Loimer N, Hofmann P, Chaudhry HR. Nasal administration of naloxone for detection of opiate dependence. J Psychiat Res. 1992;26(1):39–43. | ||
Loimer N, Hofmann P, Chaudhry HR. Nasal administration of naloxone is as effective as the intravenous route in opiate addicts. Int J Addic. 1994;29(6):819–827. | ||
Strang J, Darke S, Hall W, Farrell M, Ali R. Heroin overdose: the case for take-home naloxone. Brit Med J. 1996;312(7044):1435. | ||
Kelly A, Koutsogiannis Z. Intranasal naloxone for life threatening opioid toxicity. Emerg Med J. 2002;19(4):375. | ||
Barton ED, Ramos J, Colwell C, Benson J. Baily J, Dunn W. Intranasal administration of naloxone by paramedics. Prehosp Emerg Care. 2002;6(1):54–58. | ||
Barton ED, Colwell CB, Wolfe T, et al. Efficacy of intranasal naloxone as a needleless alternative for treatment of opioid overdose in the prehospital setting. J Emerg Med. 2005;29(3):265–271. | ||
Kelly AM, Kerr D, Dietze P, Patrick I, Walker T, Koutsogiannis Z. Randomised trial of intranasal versus intramuscular naloxone in prehospital treatment for suspected opioid overdose. Med J Austral. 2005;182(1):24–27. | ||
Kerr D, Kelly AM, Dietze P, Jolley D, Barger B. Randomized controlled trial comparing the effectiveness and safety of intranasal and intramuscular naloxone for the treatment of suspected heroin overdose. Addiction. 2009;104(12):2067–2074. | ||
Sabzghabaee AM, Eizadi-Mood N, Yaraghi A, Zandifar S. Naloxone therapy in opioid overdose patients: intranasal or intravenous? A randomized clinical trial. Arch Med Sci. 2014;10(2):309–314. | ||
Robertson TM, Hendey GW, Stroh G, Shalit, M. Intranasal naloxone is a viable alternative to intravenous naloxone for prehospital narcotic overdose. Prehosp Emerg Care. 2009;13(4):512–515. | ||
Merlin MA, Saybolt M, Kapitanyan R, et al. Intranasal naloxone delivery is an alternative to intravenous naloxone for opioid overdoses. Am J Emerg Med. 2010;28(3):296–303. | ||
Doe-Simkins M, Walley AY, Epstein A, Moyer P. Saved by the nose: bystander-administered intranasal naloxone hydrochloride for opioid overdose. Am J Public Health. 2009;99(5):788–791. | ||
Walley AY, Xuan Z, Hackman HH, et al. Opioid overdose rates and implementation of overdose education and nasal naloxone distribution in Massachusetts: interrupted time series analysis. Brit Med J. 2013;346:f174. | ||
Walley AY, Doe-Simkins M, Quinn E, Pierce C, Xuan Z, Ozonoff A. Opioid overdose prevention with intranasal naloxone among people who take methadone. J Subst Abuse Treat. 2013;44(2):241–247. | ||
US Food and Drug Administration. Role of Naloxone in Opioid Overdose Fatality Prevention. Available from: http://www.fda.gov/downloads/drugs/newsevents/ucm304621.pdf. Accessed August 18, 2016. | ||
Hertz S. Naloxone for Outpatient Use: Data Required to Support an NDA. Available from: http://www.fda.gov/downloads/drugs/newsevents/ucm300874.pdf. Accessed August 18, 2016. | ||
US Food and Drug Administration. Narcan Nasal Spray Summary Review for Regulatory Action. Available from: http://www.fda.gov/downloads/Drugs/DevelopmentApprovalProcess/DevelopmentResources/UCM480092.pdf. Accessed June 7, 2016. | ||
Krieter P, Chiang N, Gyaw S, et al. Pharmacokinetic properties and human use characteristics of an FDA-approved intranasal naloxone product for the treatment of opioid overdose. J Clin Pharmacol. 2016;56(10):1243–1253. | ||
Crystal R, Weiss MB, inventors; Lightlake Therapeutics Inc., assignee. Nasal drug products and methods of their use. United States Patent US 9211253. 2015. | ||
Wyse J, DeHart, MP, inventors; AntiOp, Inc., assignee. Intranasal naloxone compositions and methods of making and using same. United States Patent US 9192570 B2. 2015. | ||
Adapt Pharma, Inc. NARCAN® (naloxone HCl) Nasal Spray 2 mg Approved by U.S. Food and Drug Administration (FDA). Available from:http://adaptpharma.com/adapt_press_release/january-25-2017-narcan-nasal-spray-2 mg-approved-by-us-food-and-drug-administration/. Accessed June 7, 2016. | ||
Dowling J, Isbister GK, Kirkpatrick CM, Naidoo D, Graudins A. Population pharmacokinetics of intravenous, intramuscular, and intranasal naloxone in human volunteers. Ther Drug Monit. 2008;30(4):490–496. | ||
Mundin G, McDonald R, Smith K, Harris S, Strang J. Pharmacokinetics of concentrated naloxone nasal spray over first 30 minutes post-dosing: analysis of suitability for opioid overdose reversal. Addiction. 2017. Epub ahead of print. | ||
Bird SM, McAuley A, Perry S, Hunter C. Effectiveness of Scotland’s National Naloxone Programme for reducing opioid-related deaths: a before (2006–10) versus after (2011–13) comparison. Addiction. 2015;111(5):883–891. | ||
Kaléo, Inc. Briefing Dossier. Joint Meeting of the Anesthetic and Analgesic Drug Products and the Drug Safety and Risk Management Advisory Committees October 5, 2016. Available from:http://www.fda.gov/downloads/AdvisoryCommittees/CommitteesMeetingMaterials/Drugs/AnestheticAndAnalgesicDrugProductsAdvisoryCommittee/UCM522691.pdf. Accessed November 24, 2016. | ||
Merlin MA, Ariyaprakai N, Arshad FH. Assessment of the safety and ease of use of the naloxone auto-injector for the reversal of opioid overdose. Open Acc Emerg Med. 2015;7:21. | ||
US Food and Drug Administration. FDA Briefing Document. Joint Meeting of Anesthetic and Analgesic Drug Products Advisory Committee and Drug Safety and Risk Management Advisory Committee October 5, 2016. Available from: http://www.fda.gov/downloads/AdvisoryCommittees/CommitteesMeetingMaterials/Drugs/AnestheticAndAnalgesicDrugProductsAdvisoryCommittee/UCM522687.pdf. Accessed November 24, 2016. | ||
Edwards ET, Edwards ES, Davis E, Mulcare M, Wiklund M, Kelley G. Comparative usability study of a novel auto-injector and an intranasal system for naloxone delivery. Pain Ther. 2015;4(1):89–105. | ||
Wheeler E, Burk K, McQuie H, Stancliff S. Harm Reduction Coalition Guide To Developing and Managing Overdose Prevention and Take-Home Naloxone Projects; 2012. Available from: http://harmreduction.org/wp-content/uploads/2012/11/od-manual-final-links.pdf. Accessed February 1, 2017. | ||
Elzey MJ, Fudin J, Edwards ES. Take-home naloxone treatment for opioid emergencies: a comparison of routes of administration and associated delivery systems. Exp Opin Drug Deliv. 2016;17:1–4. | ||
Maxwell S, Bigg D, Stanczykiewicz K, Carlberg-Racich S. Prescribing naloxone to actively injecting heroin users: a program to reduce heroin overdose deaths. J Addict Dis 2006;25(3):89–96. | ||
Harm Reduction Coalition [Internet]. Available from:http://harmreduction.org/. Accessed February 1, 2017. | ||
Wheeler E, Davidson PJ, Jones TS, Irwin KS. Community-based opioid overdose prevention programs providing naloxone – United States, 2010. MMWR Morbid Mortal Wkly Rep. 2012;61(6):101–105. | ||
Wheeler E, Jones TS, Gilbert MK, Davidson PJ. Opioid overdose prevention programs providing naloxone to laypersons – United States, 2014. MMWR Morbid Mortal Wkly Rep. 2015 Jun 19;64(23):631–635. | ||
Bennett AS, Bell A., Tomedi L, Hulsey EG, Kral AH. Characteristics of an overdose prevention, response, and naloxone distribution program in Pittsburgh and Allegheny County. J Urban Health. 2011;88(6):1020–1030. | ||
Bennett T, Holloway K. The impact of take-home naloxone distribution and training on opiate overdose knowledge and response: an evaluation of the THN project in Wales. Drugs Educ Prev Policy. 2012;19(4):320–328. | ||
Dettmer K, Saunders B, Strang J. Take home naloxone and the prevention of deaths from opiate overdose: two pilot schemes. BMJ. 2001;322(7291):895–896. | ||
Dwyer K, Walley AY, Langlois BK, et al. Opioid education and nasal naloxone rescue kits in the emergency department. West J Emerg Med. 2015;16(3):381–384. | ||
Enteen L, Bauer J, McLean R, et al. Overdose prevention and naloxone prescription for opioid users in San Francisco. J Urban Health. 2010;87(6):931–941. | ||
Galea S, Worthington N, Piper TM, Nandi VV, Curtis M, Rosenthal DM. Provision of naloxone to injection drug users as an overdose prevention strategy: early evidence from a pilot study in New York city. Addict Behav. 2006;31(5):907–912. | ||
Lankenau SE, Wagner KD, Silva K, et al. Injection drug users trained by overdose prevention programs: responses to witnessed overdoses. J Community Health. 2013;38(1):133–141. | ||
Leece PN, Hopkins S, Marshall C, Orkin A, Gassanov MA, Shahin RM. Development and implementation of an opioid overdose prevention and response program in Toronto, Ontario. Can J Pub Heal. 2013;104(3):e200-e204. | ||
Lopez-Gaston R, Best D, Manning V, Day E. Can we prevent drug related deaths by training opioid users to recognize and manage overdoses. Harm Reduct J. 2009;6(1):26. | ||
Markham Piper TM, Stancliff S, Rudenstine S, et al. Evaluation of a naloxone distribution and administration program in New York City. Subst Use Misuse. 2008;43(7):858–870. | ||
McAuley A, Lindsay G, Woods M, Louttit D. Responsible management and use of a personal take-home naloxone supply: a pilot project. Drugs Educ Prev Policy. 2010;17(4):388–399. | ||
Rowe C, Santos G-M, Vittinghoff E,Wheeler E, Davidson P, Coffin PO. Predictors of participant engagement and naloxone utilization in a community-based naloxone distribution program. Addiction. 2015;110(8):1301–1310. | ||
Seal KH, Thawley MR, Gee ML, et al. Naloxone distribution and cardiopulmonary resuscitation training for injection drug users to prevent heroin overdose death: a pilot intervention study. J Urban Health. 2005;82(2):303–311. | ||
Strang J, Manning V, Mayet S, et al. Overdose training and take-home naloxone for opiate users: prospective cohort study of impact on knowledge and attitudes and subsequent management of overdoses. Addiction. 2008;103(10):1648–1657. | ||
Tobin KE, Sherman SG, Beilenson P, Welsh C, Latkin CA. Evaluation of the staying alive programme: training injection drug users to properly administer naloxone and save lives. Int J Drug Policy. 2009;20(2):131–136. | ||
Tzemis D, Al-Qutub D, Amlani A, Kesselring S, Buxton JA. A quantitative and qualitative evaluation of the British Columbia take home naloxone program. Can Med Assoc J Open. 2014;2(3):E153–E161. | ||
Wagner KD, Valente TW, Casanova M, et al. Evaluation of an overdose prevention and response training programme for injection drug users in the Skid Row area of Los Angeles, CA. Int J Drug Policy. 2010;21(3):186–193. | ||
Yokell MA, Green TC, Bowman S, McKenzie M, Rich JD. Opioid overdose prevention and naloxone distribution in Rhode Island. Med Health R I. 2011;94(8):240–242. | ||
Bazazi AR, Zaller ND, Fu JJ, Rich JD. Preventing opiate overdose deaths: examining objections to take-home naloxone. J Health Care Poor Underserv. 2010;21(4):1108–1113. | ||
Mountain D. Take home naloxone for opiate addicts. Big conclusions are drawn from little evidence. Brit Med J. 2001;323(7318):934. | ||
Seal KH, Downing M, Kral AH, et al. Attitudes about prescribing take-home naloxone to injection drug users for the management of heroin overdose: a survey of street-recruited injectors in the San Francisco Bay Area. J Urban Health. 2003;80(2):291–301. | ||
BDN Maine. Group aims to save lives by offering free Narcan in Bangor, Ellsworth. May 20, 2016. Available from: http://bangordailynews.com/2016/05/20/health/group-aims-to-save-lives-by-offering-free-narcan-in-bangor-ellsworth/. Accessed November 15, 2016. | ||
Davis CS., Carr D. Legal changes to increase access to naloxone for opioid overdose reversal in the United States. Drug Alcohol Depend. 2015;157:112–120. | ||
Levine M, Sanko S, Eckstein M. Assessing the risk of prehospital administration of naloxone with subsequent refusal of care. Prehosp Emerg Care. 2016;20(5):566–569. | ||
Vilke GM, Sloane C, Smith AM. Assessments for deaths in out-of-hospital heroin overdose patients treated with naloxone who refuse transport. Acad Emerg Med. 2003;10(8):893–896. | ||
Vilke GM, Buchanan J, Dunford JV, et al. Are heroin overdose deaths related to patient release after prehospital treatment with naloxone? Prehosp Emerg Care. 1999;3(3):183–186. | ||
Salama NN, Eddington ND, Fasano A. Tight junction modulation and its relationship to drug delivery. Adv Drug Deliv Rev. 2006;58(1):15–28. | ||
Burris S, Beletsky L, Castagna C, Casey C, Colin C, McLaughlin JM. Stopping an invisible epidemic: legal issues in the provision of naloxone to prevent opioid overdose. Drexel Law Rev. 2009:1(2):273–339. | ||
Beletsky L, Ruthazer R, Macalino GE, Rich JD, Tan L, Burris S. Physicians’ knowledge of and willingness to prescribe naloxone to reverse accidental opiate overdose: challenges and opportunities. J Urb Health. 2007;84(1):126–136. | ||
Davis C, Webb D, Burris S. Changing law from barrier to facilitator of opioid overdose prevention. J Law Med Ethics. 2013;41(s1):33–336. | ||
Davis C. Legal interventions to reduce overdose mortality: naloxone access and overdose Good Samaritan laws. The Network for Public Health Law, Robert Wood Johnson Foundation, June, 2016. Available from: https://www.networkforphl.org/_asset/qz5pvn/network-naloxone-10-4.pdf. Accessed January 2, 2017. | ||
Kresina TF, Lubran RL. Improving public health through access to and utilization of medication assisted treatment. Int J Environ Res Public Health. 2011;8(10):4102–4117. | ||
Volkow ND1, Frieden TR, Hyde PS, Cha SS. Medication-assisted therapies – tackling the opioid-overdose epidemic. N Engl J Med. 2014 May 29;370(22):2063–2066. | ||
Office of the Assistant Secretary for Planning and Evaluation. Opioid Abuse in the U.S. and HHS Actions to Address Opioid-Drug Related Overdoses and Deaths. March 26, 2015. ASPE Issue Brief, Department of Health and Human Services. Available from: https://aspe.hhs.gov/sites/default/files/pdf/107956/ib_OpioidInitiative.pdf. Accessed November 16, 2016. |
 © 2017 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2017 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.