")
Back to Journals » International Journal of Women's Health » Volume 15
Intimate Partner Violence; Are Saudi Physicians in Primary Health Care Setting Ready to Identify, Screening, and Respond?
Authors Alsalman Z , Shafey M, Al Ali L
Received 18 December 2022
Accepted for publication 16 March 2023
Published 18 April 2023 Volume 2023:15 Pages 623—633
DOI https://doi.org/10.2147/IJWH.S401926
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Marleen van Gelder
Zaenb Alsalman,1 Marwa Shafey,2 Laila Al Ali3
1Departments of Family and Community Medicine, College of Medicine, King Faisal University, Al Ahsa, Saudi Arabia; 2Department of Family and Community Medicine, College of Medicine, Imam Abdulrahman Bin Faisal University, Dammam, Saudi Arabia; 3Ministry of Health, Dammam, Saudi Arabia
Correspondence: Zaenb Alsalman, Departments of Family and Community Medicine, College of Medicine, King Faisal University, Po Box 3311, Al Ahsa, 36346, Saudi Arabia, Tel +966545611633, Email [email protected]; [email protected]
Introduction: Intimate partner violence (IPV) is a growing hot topic in Saudi Arabia and primary health care (PHC) physicians play a significant role in preventing it. Our objective was to assess the PHC Physicians’ readiness and barriers to identify, screen, and respond to IPV in Saudi Arabia.
Methods: A cross-sectional study recruited physicians working in PHC centers in Saudi Arabia. Data was collected using a modified online self-administered questionnaire based on the PREMIS “The Physician Readiness to Identify and Manage IPV.” The questionnaire consisted of respondent profile, perceived preparedness and knowledge, actual knowledge, practice issues, and opinion regarding barriers.
Results: Among 169 PHC physicians, 60.9% had never experienced any formal IPV training. Around one-fifth of participants have a good perceived and actual knowledge, whereas one-third have a good perceived preparedness. Nearly half of the participants (46.7%) do not screen for IPV and two-thirds of them (66.3%) have never identified an IPV case during the previous 6 months. The logistic regression model showed that family physicians were 2.27 times more likely to have a good knowledge than a general practitioner, and participants with IPV training were more likely to have a good level of perceived preparedness, perceived knowledge, and more likely to perform screening of IPV.
Conclusion: The low level of PHC physicians’ readiness to identify and respond to IPV is worrisome. Findings emphasize the urgent need for an IPV training program, a supportive work environment, and a clear referral system in order to help the practitioner to provide comprehensive services and ensure safety plans for abused women.
Keywords: intimate partner violence, primary health care, women, family physicians, Saudi Arabia
Introduction
Intimate partner violence (IPV) is defined as any physical, sexual, or psychological harm induced by the current or former partner, in addition to emotional insulting and monetary constrained behaviors.1,2 IPV is more prevalent among women than men.1 According to the World Health Organization, 30% of women worldwide have been subjected to either physical and/or sexual IPV in their lifetime.1 Studies in Saudi Arabia showed a varying prevalence of IPV ranging from 34% to 43%.3–9 However, as IPV is often under-reported, this figure is likely to be underestimated.10
IPV against women is a major public health concern with negative impacts on all aspects of their life.1,2 Abused women are at higher risk for reproductive health problems, sexually transmitted diseases, substance abuse disorders, and chronic diseases.11,12 IPV is also a major cause of a wide variety of mental health problems ranging from mild depression and anxiety to suicide attempts and death.12–14
IPV is a preventable issue. Globally different laws and policies have been developed to address this issue.15 Saudi Arabia is acting at various levels to address IPV; in 2005, the National Family Safety Program (NFSP) was established and an abuse hotline number and website were activated to report any case of violence.16,17
Health care providers play a vital role in violence prevention and management.18 IPV screening within health care services is an opportunity to provide victims with information, referral to support services, and discuss coping ways.19–21 The primary health care (PHC) setting is the ideal place to detect IPV cases, as it is the first level to contact the health care system.22 However, one of the biggest obstacles to the NFSP program’s implementation is the insufficiency of skilled medical professionals to handle IPV patients.23 The Physicians’ readiness to identify IPV has been studied in different countries, which revealed that health care providers had insufficient knowledge and preparedness to identify and properly respond to IPV.24,25
In Saudi Arabia, IPV is a growing hot topic; studies have been conducted aiming at estimating the prevalence of IPV, while the physicians’ readiness to recognize, screen, and respond to IPV is less tackled. Moreover, little data are available about what has been done to address this issue among PHCs despite the global recommendations to incorporate IPV training and education into the curriculum and professionals continuing medical education. Hence, this study aims at assessing the PHC Physicians’ readiness and barriers to identify, screen, and respond to IPV in Saudi Arabia.
Materials and Methods
Setting and Participants
This cross-sectional study was targeting Saudi primary health care physicians. The sample size was estimated by using the Cochran formula assuming the proportion of physicians’ preparedness is 30% as reported by a previous Saudi study with the desired level of precision of 5%, and a confidence interval is 95%.26 A convenience sampling technique was utilized to choose study participants from 322 online questionnaires that were delivered through email and WhatsApp under the supervision of the Saudi Commission of Health Specialties.
Instrument
A modified version of a validated questionnaire “The Physician Readiness to Manage IPV Survey” (PREMIS) was used. The original questionnaire consists of five sections: respondent profile, perceived preparedness and knowledge, actual knowledge, and practice issues.27 The survey was modified in order to reflect Saudi culture and primarily addresses women’s abuse. For instance, questions on lesbian women, single mothers, Black or Hispanic women, immigrant women, and homosexual men were all deleted since they are not applicable to Saudi culture. Additional references to legal advocates, victim witness advocates, batterers’ treatment programs, batterers’ women support groups, and lesbian, homosexual, bisexual, and transgender support organizations were eliminated due to the lack of support services in Saudi Arabia. In the practice section, items related to using the camera, taking photographs, and utilizing a body map to document victims’ injuries were removed since these practices are not permitted in Saudi Arabia. Moreover, all statements regarding how physicians perceive patients with a history of IPV behaviors at the appropriate stage of change were deleted for the sake of survey length. All statements outside the scope of our study’s goal were withdrawn such as questions regarding abuse of children, elders, or male victims. Researchers also included statements about participants’ opinion regarding barriers to IPV screening. Finally, the utilized tool consisted of perceived preparedness (4 statements), perceived knowledge (10 statements); each of the five-point Likert’s scale, actual knowledge (17 statements) scored correct or incorrect, practice questions; screening of IPV (yes/no), and those for responding to identified IPV comprised 6 action statements of yes/no answers. Additionally, six opinion statements about barriers to screening of three points Likert’s scale were included. The modified questionnaire was tested for its internal consistency reliability, with a Cronbach’s alpha >0.7 (perceived preparedness 0.88, perceived knowledge 0.94, and Opinion 0.72).
Data Analysis
Collected data was coded, entered, and analyzed using the Statistical Package for the Social Sciences (SPSS).28 Researchers followed the PREMIS tool Kit, which provides a scoring system for preparedness and knowledge.26 The raw scores for perceived preparedness (4–20), perceived knowledge (10–50), the actual knowledge (0–17), and the response to identified IPV (0–6). Mean scores and mean percentage scores were calculated and a cutoff point was set for the categorization of perceived preparedness, perceived knowledge, and actual knowledge where good levels were ≥75%, fair 75 to ≥50%, and poor level of <50. Regarding opinion toward barriers six negative statements were scored from 1 to 3; (totally agree, neutral, disagree), raw scores (6–18), mean and mean percent scores were calculated, and further the mean percent scores were categorized into negative, neutral, and positive opinions of service provision (<50%, 50–<75%, and ≥75%). A test of normality was conducted and the relation between physicians’ scores of preparedness, and knowledge of demographic or job characteristics was assessed using parametric and non-parametric data. Logistic regression analysis of sociodemographic and job characteristics with a good level of perceived preparedness, perceived knowledge, actual knowledge, and the practice of screening was performed. A p-value of <0.05 was set as significant.
Results
Characteristics of Participants
The total number of physicians was 169 (response rate of 52.4%). Nearly two-thirds (64.5%) were below 40 years, 54.4% were men, 80.5% were married, and 39.1% saw an average of <40 patients per week. Moreover, the highest percentage of physicians (60.9%) had never experienced any formal IPV training and 59.8% had experienced disclosure for IPV. The remaining participants’ sociodemographic and job characteristics are shown in Table 1.
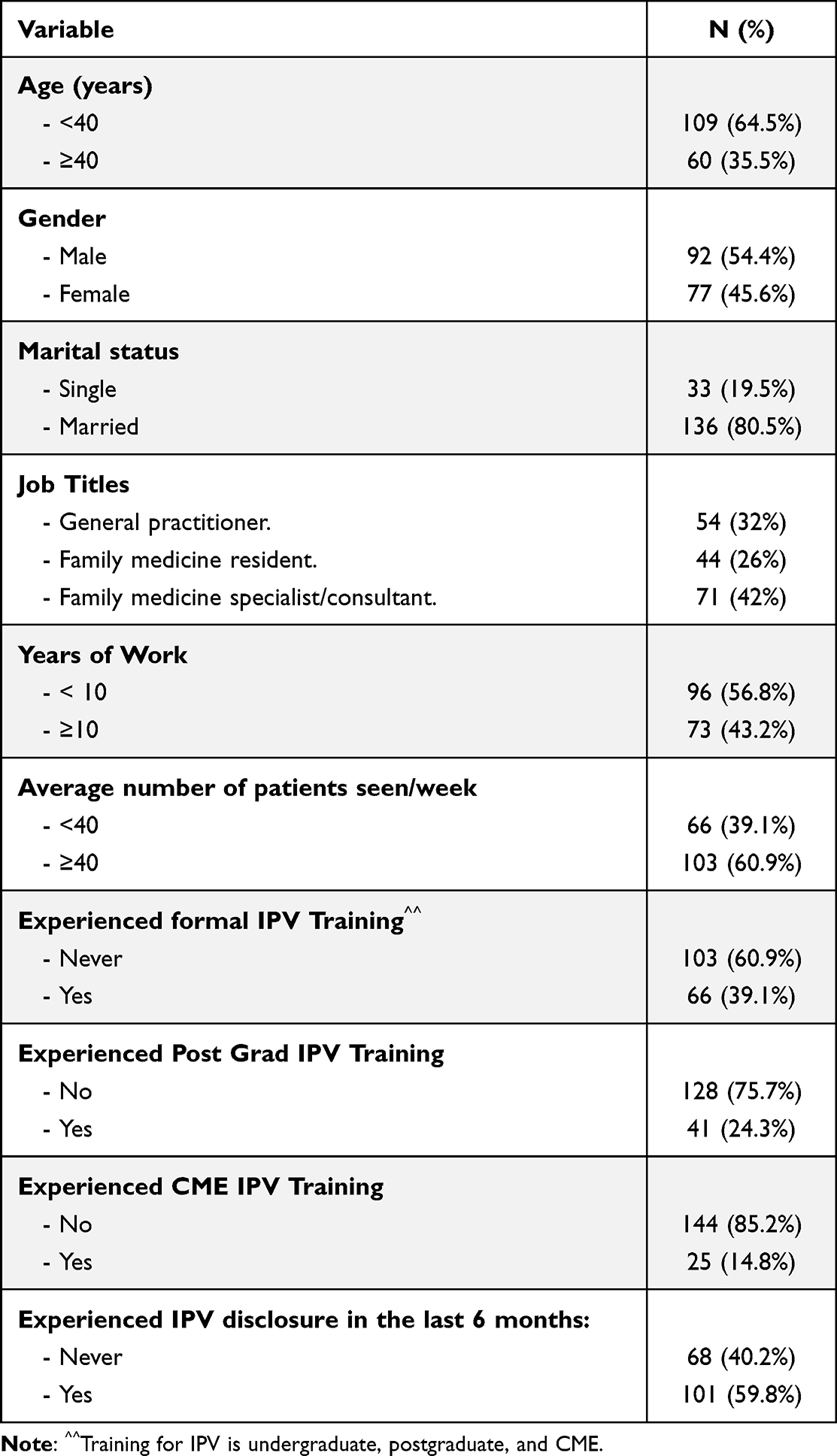 |
Table 1 Participants’ Sociodemographic and Job Characteristics (N=169) |
Participants’ Perceived Preparedness, Perceived Knowledge, and Actual Knowledge of IPV
Only around one-fifth of participants have a good perceived and actual knowledge (18.3% and 21.9% respectively), whereas one-third (33.2%) have a good perceived preparedness toward IPV (Figure 1).
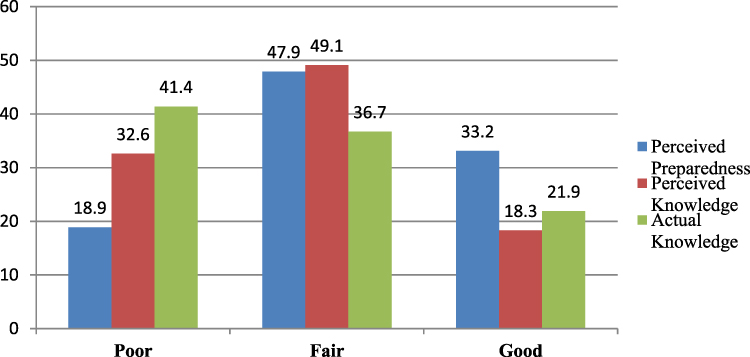 |
Figure 1 Physicians’ Levels of Perceived Preparedness, Perceived Knowledge, and Actual Knowledge. |
The perceived preparedness to IPV mean raw score is 12.56±3.94 with a mean percent score of 62.84± 19.71. Additionally, the perceived knowledge mean raw score is 28.65±9.89 with a mean percent score of 57.29±19.37 (Table S1). Regarding the actual knowledge, only 17.8% of physicians correctly answered the question regarding being a female risk factor for IPV, whereas 42.6% correctly answered about the batterers using violence as a means of controlling their partners, and nearly half correctly responded about how to ask appropriately about IPV. The most reported warning sign of partner abuse was frequent injuries (78.7%). The mean raw score for actual knowledge is 9.18±3.61 with a mean percent score of 54.05± 21.27 (Table S2).
In Table 2, differences in perceived preparedness, knowledge, and actual knowledge mean percent scores in relation to sociodemographic and job characteristics are seen with age; participants older than 40 years had significantly higher perceived preparedness and perceived knowledge. Family medicine specialists/consultants had significantly higher perceived knowledge scores than family medicine residents or general practitioners meanwhile general practitioners had significantly lower actual knowledge scores than family medicine residents or family medicine specialists/consultants. Physicians who had formal IPV training were significantly higher in their preparedness and perceived knowledge, and those who had post-grad IPV training significantly scored higher actual knowledge scores. Participants with previous IPV disclosure significantly had higher perceived preparedness and actual knowledge scores.
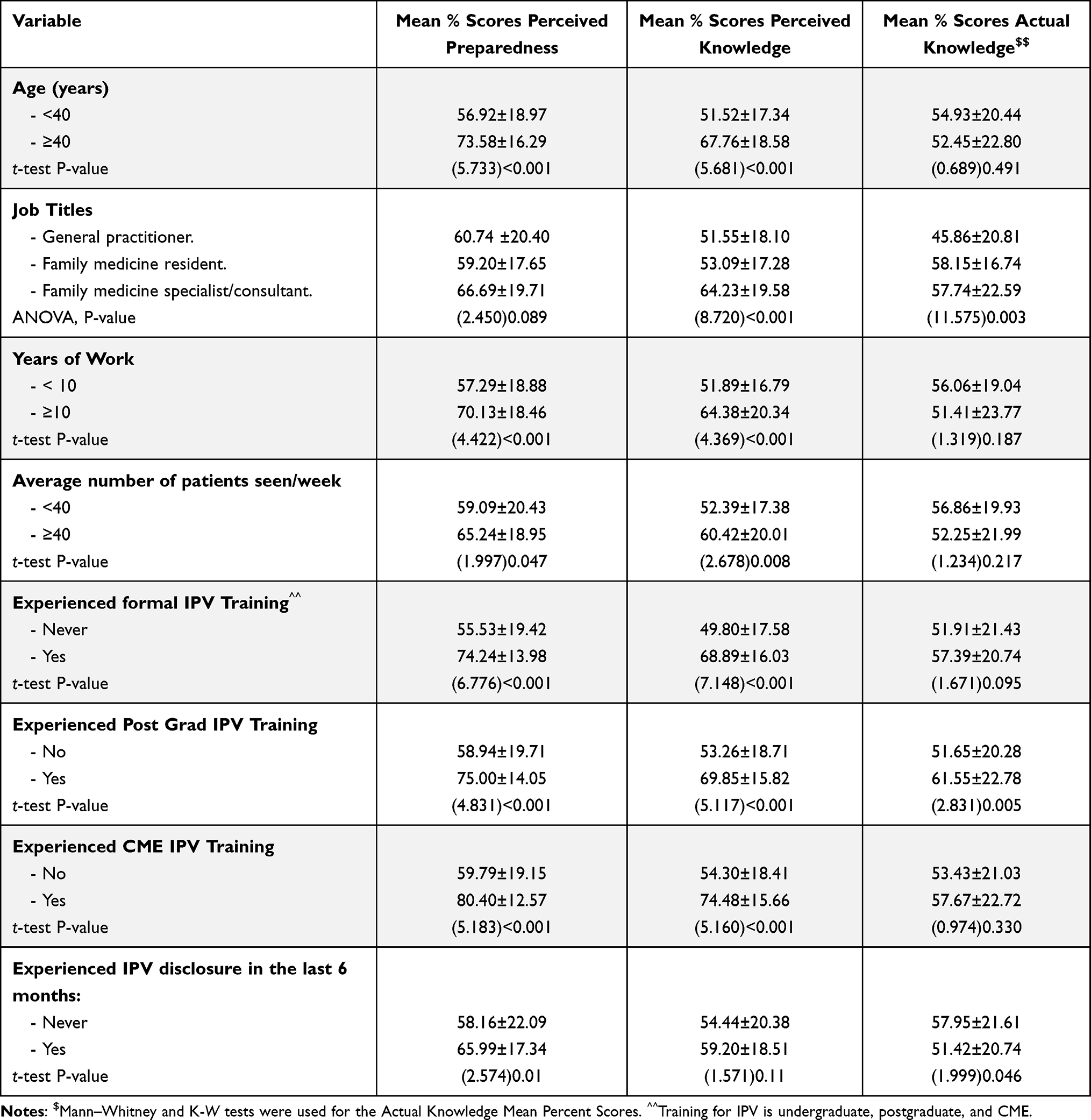 |
Table 2 Differences in Perceived Preparedness, Knowledge, Opinion, and Actual Knowledge Mean Percent Scores in Relation to Sociodemographic and Job Characteristics |
Physicians’ Practice of Screening and Responding to IPV
Nearly half of the physicians (46.7%) do not screen for IPV. Two-thirds of participants (66.3%) have never identified an IPV case during the previous 6 months (Table S3). Moreover, various responses were reported by participants toward IPV cases when identified (Figure 2).
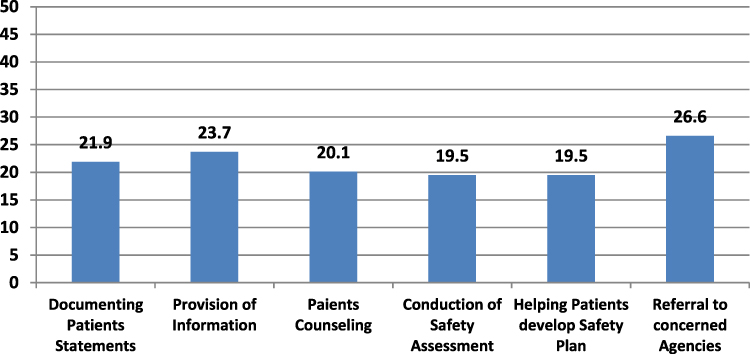 |
Figure 2 Physicians’ Responses to Identified IPV. |
Physicians who exhibited good practice score were only 11.2%. Whereas around one-fifth of the physicians (20.1%) were familiar with IPV screening and management guidelines, as well as 29.2% were aware of the protocol for dealing with IPV, 17.8% stated having adequate IPV referral resources and only 7.1% affirmed that educational resource materials are available at their work site. The mean practice score is 1.31±1.92, and the mean percent practice score is 21.89±32.69 (Table S3).
Chi2 test was performed to show differences between the practice of screening and different sociodemographic and job characteristics, where age, years of experience, experiencing CME IPV training courses and IPV disclosure were not of significant differences. On the contrary, family specialists/consultants, experiencing formal, post-grad training courses, good levels of perceived preparedness, knowledge, and levels of actual knowledge were all of significantly high percentages of practicing screening towards IPV; p-value <0.001 (Table 3).
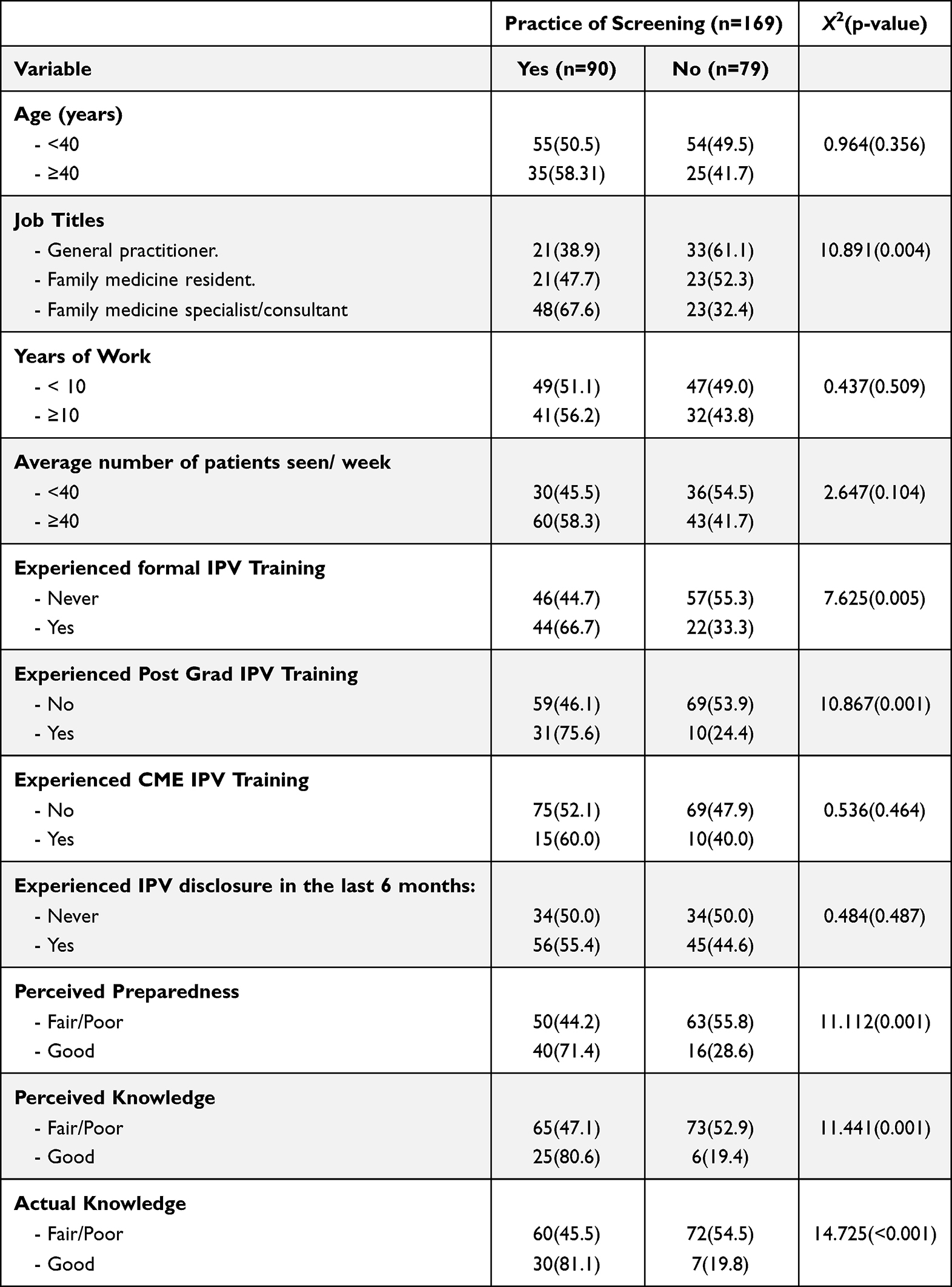 |
Table 3 Differences in the Practice of Screening Among Participants (n=169) According to Different Characteristics |
Perceived Opinion Regarding Barriers to Screening and Responding to IPV
Around half of the participants agreed (58.6%) that they do not have sufficient training to assist individuals in addressing IPV and 38.6% agreed they do not have the necessary skills to discuss the abuse with a female IPV victim, and 35.6% agreed that screening is likely to offend those who are screened. However, only around a third of physicians agreed that their workplace encouraged them as well as provided them with adequate private space and time to respond to IPV cases (33.7%, 30.7%, and 27.2% respectively).
The mean perceived opinion score was 11.29±2.44, the mean percent score is 62.75±13.59. Physicians who displayed negative opinion perception towards barriers to screening and responding to IPV constituted (n=28, 14.8%), neutral perceived opinion 68.0%, while those having positive perceived opinion were only (n=29, 17.2%) (Table S4).
Multivariable Analysis
The logistic regression model in Table 4 shows that participants over 40 were 10 times more likely to have a good level of perceived knowledge, while family physicians were 2.27 times more likely to have good knowledge and 1.77 times more likely to screen for IPV than general practitioners. Furthermore, participants who had received IPV training were more likely to screen for IPV and to have a good level of perceived preparedness as well as perceived knowledge.
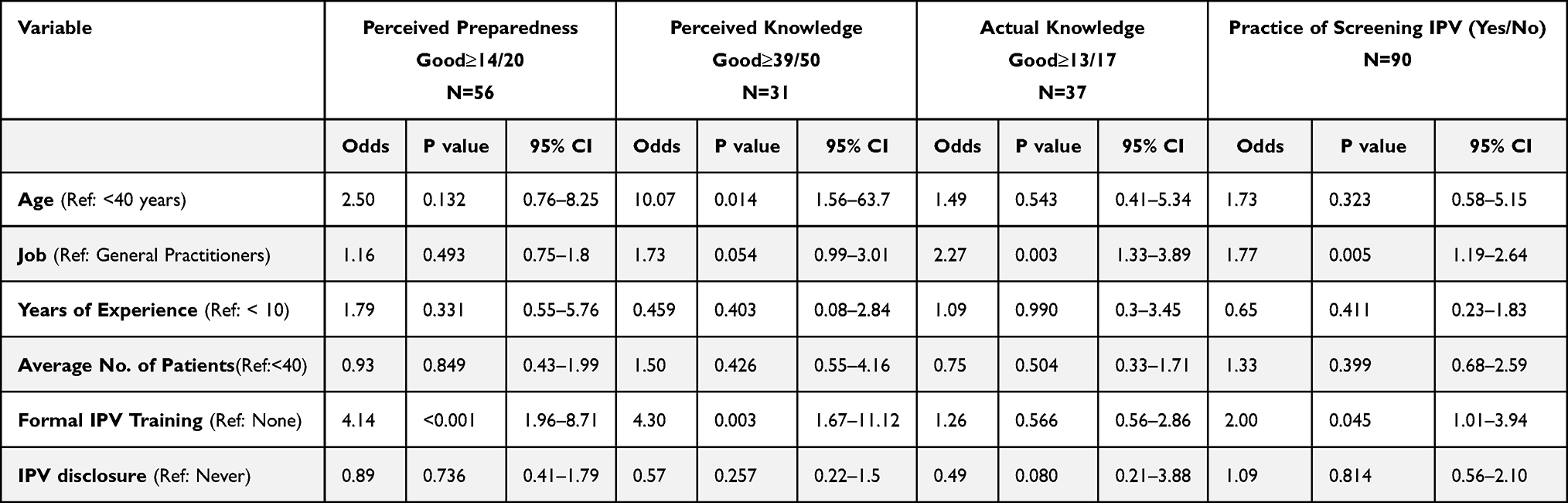 |
Table 4 Logistic Regression Analysis of Sociodemographic and Job Characteristics with Good Level of Perceived Preparedness, Perceived Knowledge, Actual Knowledge and the Practice of Screening |
Discussion
IPV is a crucial and preventable health concern that PHC physicians frequently encounter.9 The aim of this study was to assess physicians’ readiness and barriers to identify, screen, and respond to IPV.
The current study revealed that approximately one-third of the participants perceived themselves as well-prepared to ask appropriate questions about IPV, respond to abuse disclosure, and identify as well as assist victims. Moreover, only 18.3% of them perceived themselves to have good knowledge regarding IPV. Similar findings were reported in Saudi Arabia and elsewhere.23,24,26,29 Different factors may explain the inadequate level of perceived preparedness; nonetheless, in our study, formal IPV training was a significant predictor of good perceived preparedness, which matches a British study outcome.24 However, less than half of our sample had received training in this field. This finding emphasizes the critical need for an IPV training program at the undergraduate and postgraduate levels, which would provide physicians with a high self-confidence level in recognizing and managing abused women.
Numerous factors contribute to inducing IPV including female gender, low education, parental violence, childhood maltreatment, and gender inequity.1 Being female is the risk factor that significantly leads to IPV.27 However, in our study, just a handful of physicians properly recognized being female as the most significant factor while almost half of them stated that alcohol consumption is the main risk. Similar results were reported from national and global studies.23,24,26 Additionally, most of the participants believed that financial dependency and children’s needs were the most constraints not leaving abusive relationships. IPV is a complex societal issue rather than a clinical illness, resulting from cultural norms and differences, such as male dominance and religious factors.30 Furthermore, Saudi women are financially dependent on their partners, and they are forced to live with their relatives if they were divorced.30 Physicians in our study had insufficient IPV knowledge, which may be explained by employment characteristics such as job title, number of patients seen, as well as IPV disclosure, and training. Unsurprisingly, family physicians were more likely to have a good knowledge level than general practitioners. This discrepancy is expected due to the training residency programs, curriculum, and continuous professional development of a family physician.
IPV must be addressed at various levels within the medical field; the first step of intervention is to identify females who may be exposed to violence.31 According to the US Preventive Services Task Force, physicians should screen all women of reproductive age for IPV.32 Different screening tools are available, and despite this around half of our physicians never screen women for IPV, which is in line with Ramsay et al's study on English physicians.24,33 On the other hand, this observed percentage is greater than that reported in prior Saudi research in 2020 but lower than a Spanish study in 2016.26,34 This disappointing screening level probably explains why most participants never identified an IPV incident in the previous 6 months, which is consistent with Alghamdi et al; however, Ramsey et al found a greater rate of IPV detection.24,26 The low proportion of experiencing IPV disclosure by the victim could be explained by the fact that women generally do not reveal information regarding experienced domestic violence in the absence of screening questions from the physician as they are often too ashamed or afraid to do so.24
Consequently, given the high prevalence of IPV among Saudi women and the suboptimal screening level, many cases of violence are likely to go unnoticed by PHC professionals.9 In our study, the observed inadequate screening was associated with low physician preparedness, knowledge, and IPV training. It could also be explained by screening barriers that might restrict physicians from performing their duties and detecting cases early, where a high percentage of our participants agreed that they do not have sufficient training and necessary skills to assess and discuss abuse with female victims. Similar findings have been reported in Saudi Arabia, Egypt, and Canada, which revealed that gaps in providers’ knowledge and the lack of IPV training are the key factors limiting physicians’ practice of screening.22,35,36
Additionally, participants in the present study perceived a variety of workplace challenges that might play a significant role in detecting and dealing with abused women, such as a lack of enough time and private space in their workplace to discuss and assist the victim. This highlights the responsibility of the health institution in providing the appropriate infrastructure and resources for assisting physicians, including local protocols, adequate time, and a private area to deal with abused women.29
Screening alone is insufficient to address IPV patients’ health and safety needs; a comprehensive assessment and management program should accompany it.9 Our participants reported a very low-action response toward IPV victims; documentation, providing information, conducting safety assessment or plan, and referral to the concerned agencies. Physicians’ confidence in IPV referring pathways and resources is a key component of the perceived support system, which is linked to a higher rate of IPV screening.22,37 Disparately our participants were unaware of IPV referral resources and the concerned referral agencies. Low referral levels were also reported in Saudi and US studies.23,26,29 Physicians should be aware of their legal and ethical responsibilities as well as the appropriate responses when violence is reported, in order to address the concerns and break the cycle of violence. According to our study, only a few physicians were familiar with IPV guidelines and the local protocol, which is congruent with research by Zaher et al.23
Without physicians’ training and evaluation, the availability of IPV guidelines and protocols at health institutions will not be adequate to enhance physicians’ practice of identifying IPV.9 The medical record for an abused case highlights areas where they might improve care and meet the best standards.37 Physicians should get training on how to use protocols and standard documentation to enhance their practice.
This study has some limitations. First, researchers were optimistic to have a higher response rate, however because of the restrictions induced by COVID 19 such as social distance and paperless work, data was collected via an online platform and a convenience sampling technique was utilized. The modified PREMIS tool was lengthy, and the long time needed to fill it may have influenced the participants’ responses. Nevertheless, the data were self-reported, which might have introduced self-reporting biases.
Conclusion
IPV is a well-known public health concern in Saudi Arabia, and physicians have a critical role to play. Despite that, our study revealed a suboptimal level of physicians’ readiness to identify and respond to IPV, in addition to the existence of screening barriers. Physicians were also unknowledgeable about IPV; they neither practiced an adequate level of screening nor appropriately responded to it. These findings emphasize the urgent need for an IPV training program, a supportive work environment, and a clear referral system in order to help the PHC practitioner to provide comprehensive services and ensure safety plans for abused women.
Data Sharing Statement
The data sets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Ethics
Ethical approval was obtained from the Imam Abdulrahman Bin Faisal University Institutional Board (IRB 2021-01-293/Sep.8-2021). Additionally, informed consent was taken from all participants.
Acknowledgments
We would like to thank the Saudi Commission of Health Specialties and all participants for their collaboration.
Funding
This work was supported by the Deanship of Scientific Research, Vice Presidency for Graduate Studies and Scientific Research, King Faisal University, Saudi Arabia [Grant NO. 2167].
Disclosure
No conflict of interest to disclose.
References
1. World Health Organization. Violence against women prevalence estimates; 2018. Available from: https://www.who.int/publications/i/item/9789240022256.
2. Breiding MJ, Basile KC, Smith SG, et al. Intimate partner violence surveillance: uniform definitions and recommended data elements; 2015. Available from: https://www.cdc.gov/violenceprevention/pdf/intimatepartnerviolence.pdf.
3. Tashkandi A, Rasheed FP. Wife abuse: a hidden problem. A study among Saudi women attending PHC centers. East Mediterr Health J. 2009;15:1242–1253.
4. Fageeh W. Factors associated with domestic violence: a cross-sectional survey among women in Jeddah, Saudi Arabia. Br Med J Open. 2014;4(2):e004242.
5. Barnawi FH. Prevalence and risk factors of domestic violence against women attending a primary care center in Riyadh, Saudi Arabia. J Interpers Violence. 2017;32(8):1171–1186. doi:10.1177/0886260515587669
6. Alquaiz AM, Almuneef M, Kazi A, Almeneessier A. Social determinants of domestic violence among Saudi married women in Riyadh, Kingdom of Saudi Arabia. J Interpers Violence. 2021;36(3–4):1561–1585. doi:10.1177/0886260517746128
7. Wali R, Khalil A, Alattas R, Foudah R, Meftah I, Sarhan S. Prevalence and risk factors of domestic violence in women attending the National Guard Primary Health Care Centers in the Western Region, Saudi Arabia, 2018. BMC Public Health. 2020;20(1):239. doi:10.1186/s12889-020-8156-4
8. Afifi ZE, Al-Muhaideb NS, Hadish NF, Ismail FI, Al-Qeamy FM. Domestic violence and its impact on married women’s health in Eastern Saudi Arabia. Saudi Med J. 2011;32(6):612–620.
9. AlJuhani S, AlAteeq M. Intimate partner violence in Saudi Arabia: a topic of growing interest. J Fam Med Prim Care. 2020;9(2):481–484. doi:10.4103/jfmpc.jfmpc_1139_19
10. Abolfotouh MA, Almuneef M. Prevalence, pattern and factors of intimate partner violence against Saudi women. J Public Health. 2020;42(3):206–214. doi:10.1093/pubmed/fdz092
11. World Health Organization. Violence against women. World Health Organization; 2021. Available from: https://www.who.int/news-room/fact-sheets/detail/violence-against-women.
12. Eldoseri HM, Tufts KA, Zhang Q, Fish JN. Adverse health effects of spousal violence among women attending Saudi Arabian primary health-care clinics. East Mediterr Health J. 2014;20(11):717–725. doi:10.26719/2014.20.11.717
13. Bacchus LJ, Ranganathan M, Watts C, Devries K. Recent intimate partner violence against women and health: a systematic review and meta-analysis of cohort studies. BMJ Open. 2018;8(7):e019995. doi:10.1136/bmjopen-2017-019995
14. Ellsberg M, Emmelin M. Intimate partner violence and mental health. Glob Health Action. 2014;7:1–3. doi:10.3402/gha.v7.25658
15. Division of Violence Prevention National Center for Injury Prevention and Control. Preventing Intimate Partner Violence Across the Lifespan: A Technical Package of Programs, Policies, and Practices. Atlanta, Georgia: Centers for Disease Control and Prevention; 2017.
16. The National Family Safety Program. Bureau of experts at the Council of Ministers: law of protection from abuse; 2013. Available form: https://www.nfsp.org.sa/ar/Pages/default.aspx.
17. Ministry of Social Affairs (MOSA). Kingdom of Saudi Arabia. Social protection; 2012. Available from: http://mosa.gov.sa/portal/modules/smartsection/item.php?itemid=13.
18. Signorelli MC, Hillel S, de Oliveira DC, Ayala Quintanilla BP, Hegarty K, Taft A. Voices from low-income and middle-income countries: a systematic review protocol of primary healthcare interventions within public health systems addressing intimate partner violence against women. BMJ Open. 2018;8(3):e019266. doi:10.1136/bmjopen-2017-019266
19. Phelan MB. Screening for intimate partner violence in medical settings. Trauma Violence Abuse. 2007;8(2):199–213. doi:10.1177/1524838007301221
20. O’Campo P, Kirst M, Tsamis C, Chambers C, Ahmad F. Implementing successful intimate partner violence screening programs in health care settings: evidence generated from a realist‐informed systematic review. Soc Sci Med. 2011;72(6):855–866. doi:10.1016/j.socscimed.2010.12.019
21. Miller E, McCaw B, Humphreys BL, Mitchell C. Integrating intimate partner violence assessment and intervention into healthcare in the United States: a systems approach. J Women's Health. 2015;24(1):92–99. doi:10.1089/jwh.2014.4870
22. Ibrahim E, Hamed N, Ahmed L. Views of primary health care providers of the challenges to screening for intimate partner violence, Egypt. East Mediterr Health J. 2021;27(3):233–241. doi:10.26719/emhj.20.125
23. Zaher E, Mason R. Saudi family medicine residents’ readiness to manage intimate partner violence: a needs assessment study. Middle East J Fam Med. 2014;12(1):14–19. doi:10.5742/MEFM.2014.92441
24. Ramsay J, Rutterford C, Gregory A, et al. Domestic violence: knowledge, attitudes, and clinical practice of selected UK primary healthcare clinicians. Br J General Pract. 2012;62:602. doi:10.3399/bjgp12X654623
25. Ambikile JS, Leshabari S, Ohnishi M. Knowledge, attitude, and preparedness toward IPV care provision among nurses and midwives in Tanzania. Hum Resour Health. 2020;18(1):56. doi:10.1186/s12960-020-00499-3
26. Alghamdi LM, Alzahrani F. Knowledge, detection, and reporting of domestic violence among family medicine residents of Eastern Province, Saudi Arabia. Int J Sci Study. 2020;8(1):72–78.
27. Short LM, Alpert E, Harris JM, Surprenant ZJ. A tool for measuring physician readiness to manage intimate partner violence. Am J Prev Med. 2006;30:173–180. doi:10.1016/j.amepre.2005.10.009
28. IBM Corp. IBM SPSS Statistics for Windows, Version 24.0. Armonk, NY: IBM Corp; 2017.
29. Renner LM, Wang Q, Logeais ME, Clark CJ. Health care provider’s readiness to identify and respond to intimate partner violence. J Interpers Violence. 2021;36(19–20):9507–9534. doi:10.1177/0886260519867705
30. Garcia-Moreno C, Jansen HA, Ellsberg M, Heise L, Watts CH. Prevalence of intimate partner violence: findings from the WHO multi-country study on women’s health and domestic violence. Lancet. 2006;368(9543):1260–1269. doi:10.1016/S0140-6736(06)69523-8
31. O’Doherty L, Hegarty K, Ramsay J, Davidson LL, Feder G, Taft A. Screening women for intimate partner violence in healthcare settings. Cochrane Database Syst Rev. 2015;12(7):348.
32. Nelson HD, Bougatsos C, Blazina I. Screening women for intimate partner violence: a systematic review to update the U.S. Preventive Services Task Force recommendation. Ann Intern Med. 2012;156(11):796–808. doi:10.7326/0003-4819-156-11-201206050-00447
33. Rabin R, Jennings J, Campbell J, Bair-Merritt M. Intimate partner violence screening tools: a systematic review. Am J Prev Med. 2009;36(5):439–445.
34. Rodriguez-Blanes GM, Vives-Cases C, Miralles-Bueno JJ, San Sebastian M, Goicolea I. Detection of intimate partner violence in primary care and related factors. Gac Sanit. 2017;31(7):410–415. doi:10.1016/j.gaceta.2016.11.008
35. Alsaedi JA, Elbarrany WG, AlMajnon WA, AlNamankany AA. Barriers that impede primary health care physicians from screening women for domestic violence at Makkah ALmukarramah City. Egypt J Hosp Med. 2017;69(8):3058–3065.
36. Gutmanis I, Beynon C, Tutty L, Wathen CN, MacMillan HL. Factors influencing identification of and response to intimate partner violence: a survey of physicians and nurses. BMC Public Health. 2007;7(12):1–11.
37. Ahmad I, Ali PA, Rehman S, Talpur A, Dhingra K. Intimate partner violence screening in emergency department: a rapid review of the literature. J Clin Nurs. 2017;26(21–22):3271–3285. doi:10.1111/jocn.13706
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.