")
Back to Journals » International Journal of Women's Health » Volume 11
Intimate partner violence among HIV-positive women in Nairobi, Kenya
Authors Brooks RD, Jolly PE, Marsh L, Velazquez JM, Padilla L , Jaoko WG
Received 29 January 2019
Accepted for publication 9 July 2019
Published 19 August 2019 Volume 2019:11 Pages 451—461
DOI https://doi.org/10.2147/IJWH.S203327
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Elie Al-Chaer
RD Brooks,1 PE Jolly,1 L Marsh,1 JM Velazquez,1 L Padilla,1 WG Jaoko2
1Department of Epidemiology, University of Alabama at Birmingham School of Public Health, Birmingham, AL, USA; 2Department of Medical Microbiology, School of Medicine, University of Nairobi, Nairobi, Kenya
Correspondence: PE Jolly
Department of Epidemiology, University of Alabama at Birmingham, School of Public Health, 1665 University Boulevard, RPHB 217, Birmingham, Alabama 35294-0022, USA
Tel +1 205 934 1823
Fax +1 205 975 3329
Email [email protected]
Purpose: This study was conducted to identify the prevalence and sociodemographic factors associated with four forms of intimate partner violence (IPV) among HIV-positive women attending the Comprehensive Care Centre at the Kenyatta National Hospital in Nairobi, Kenya.
Methods: A cross-sectional study was conducted among 600 sexually active HIV-positive women aged 18–69 years from May to August of 2012. A structured questionnaire including questions pertaining to sociodemographic characteristics, health care decisions, and forms of IPV (controlling behavior, emotional abuse, physical violence, and sexual violence) was administered to each woman.
Results: All women reported experiencing emotional abuse; 20%, 17%, and 15% experienced controlling behavior, physical violence, and sexual violence, respectively. Women who reported low/below average socioeconomic status (SES) had a greater likelihood of experiencing controlling behavior than women with high/average SES (adjusted odds ratio [aOR] =1.62, 95% CI 1.05–2.51). Women who were unemployed had greater odds of experiencing physical violence than those who were employed (aOR =2.35, 95% CI 1.31–4.23). Non-Christian women had higher odds of experiencing controlling behavior, physical violence, and sexual violence than Christian women (aOR =4.41, 95% CI 1.81–10.76 and aOR =3.33, 95% CI 1.43–7.80).
Conclusion: Based on the prevalence of IPV and the sociodemographic factors identified to be associated with IPV among women in this study it may be beneficial to include IPV screening as part of routine clinic visits for HIV-positive and other women. Furthermore, women who report emotional abuse or controlling behavior from spouse should not be overlooked, as these two forms of IPV may precede or accompany physical and sexual IPV. Women who report experiencing IPV during clinic visits may be referred to organizations and resources available to battered women in Kenya. Increased funding for anti-IPV programs and changes in policy may also contribute to a reduction in IPV among HIV-positive and other women in Kenya.
Keywords: intimate partner violence, emotional abuse, sexual violence, physical violence, controlling behavior, violence against women
Introduction
Intimate partner violence (IPV) is the most common form of violence experienced by women globally.1 The World Health Organization (WHO) considers physical violence, sexual violence, emotional abuse, and controlling behavior by an intimate partner in all forms of IPV.2 According to Fustos (2011), 30% of the women aged ≥15 years, have been physically and/or sexually abused by an intimate partner during their lifetime.1 Moreover, prior findings have identified positive correlations between IPV and HIV infection.2,3 Women who suffer abuse from a partner are less likely to demand condom use, resulting in a greater risk of HIV infection.4 Furthermore, Human Rights Watch researchers in Zambia documented instances in which women were physically, sexually, and emotionally abused when they attempted to discuss HIV treatment with their husbands.5 Other studies reported that women who experienced violence in the past were more likely to fear violence upon disclosure of their HIV-positive status.6–8 Thus, some women may refrain from being tested for HIV fearing their partner’s reaction should they test positive. Women who managed to obtain treatment without their husbands’ knowledge or permission were more likely to neglect necessary care (ie, missing ART treatment or doctor’s appointments) as they did not want their husbands to find out about their treatment for fear of abuse.5
The Kenya 2014 Demographic and Health Survey reported that 49% of Kenyan women who have ever been married reported that they experienced violence at least once from an intimate partner.9 Moreover, several studies have evaluated IPV among women in Kenya; of these, two of three found that HIV risk was significantly associated with psychological, physical, and/or sexual IPV.3,10–13 One study found that associations between HIV infection and IPV were dependent on the presence of controlling behavior.14 More specifically, the association between HIV and IPV among women who were exposed to physical, sexual, or emotional IPV and no controlling behavior was weaker than among those who experienced controlling behavior.14 While this study included data from 12 sub-Saharan African countries, including Kenya, the Kenyan study did not contain controlling behavior, and therefore was not included in this analysis.14 Controlling behaviors were included in one study conducted among HIV-positive female sex workers in Mombasa, Kenya.13 They found that women who experienced controlling behaviors by an index partner (a regular emotional partner, defined as a boyfriend or husband, who they did not consider to be a client or a casual partner) were significantly more likely to report recent physical, sexual, or emotional IPV,13 thereby validating the importance of including controlling behaviors in IPV studies among women in Kenya. Studies evaluating IPV among women in developing countries often focus on physical, psychological/emotional abuse, and sexual violence. While these three types of IPV are most commonly evaluated, other studies have focused on one or two types.3,10–22 While few studies have evaluated controlling behavior as a form of IPV among women in sub-Saharan Africa. Several have identified associations between partners’ controlling behavior and other forms of IPV, including physical, sexual, and emotional.21–25 These findings highlight the importance of including controlling behavior as a form of IPV, as it may precede or accompany other forms of IPV. Moreover, no studies to date have evaluated all four forms of IPV among HIV-positive Kenyan women who were not female sex workers. Our study examined the prevalence and sociodemographic factors associated with physical, sexual, and emotional IPV and controlling behaviors among HIV-positive women attending the Comprehensive Care Centre (CCC), at the Kenyatta National Hospital (KNH) in Nairobi, Kenya. These CCCs are clinic sites where people living with HIV go to for holistic care and management. They offer clinical care, counselling services on nutritional, psychological, and spiritual issues, palliative care, referral care, and stress management.26
Methods
Study design and data collection
A quantitative cross-sectional study using consecutive sampling was conducted among 600 HIV-positive women who attended the CCC at KNH from May to August of 2012. Based on an estimated prevalence of 45% for IPV among women in Kenya,9 we needed 381 women to assess overall IPV in our study with a 95% confidence level and 5% margin of error. We went over this number and recruited 600 women in order to increase our power and to account for incomplete surveys. KNH is a large teaching and referral hospital in Kenya with a 1800 bed capacity. It serves as the primary hospital for the four million residents of the capital city of Nairobi and surrounding areas. Women attending the CCC were considered eligible for the study if they were HIV-positive, 18–69 years of age, and were sexually active in the past 6 months with their intimate sexual partner. Women who did not meet these criteria or who engaged in commercial sex work were excluded from participation in the study. Commercial sex was selected as an exclusion criterion since it suggests more transient sexual activity. Commercial sex may also involve multiple partners and increase the risk of sexual abuse and other forms of IPV, as 78.7% female sex workers in one Kenyan study reported any IPV in the last 30 days.27 We wanted to investigate abuse by intimate partners in more lasting relationships and involved in dealing with matters of daily life. Being sexually active in the past 6 months was also selected as an inclusion criterion since the focus of the research is on IPV and sexual activity suggests intimacy. Lack of sexual activity for a period longer than 6 months may suggest less intimate interaction and less chance of abuse.
After written informed consent was obtained in private clinic rooms from eligible women, a trained research assistant conducted an interview with each woman using a structured questionnaire that was administered to each participant in a consistent manner, in either English or Swahili, depending on the participant’s preference. English and Swahili are official languages in Kenya. The questionnaire was developed in English, translated into Swahili and back-translated into English to ensure consistency, and was pre-tested by native language interpreters. The refusal rate was very low at <2%. The instrument consisted of questions on sociodemographic characteristics, health care decisions, and IPV (emotional abuse, controlling behavior, physical violence, and sexual violence) with current partner within the previous 6 months. The interviews were conducted in private rooms with closed doors at the CCC to ensure privacy and confidentiality. Data from paper surveys were entered into a Microsoft Access database and verified by two research assistants trained in data entry. The WHO definitions were used to categorize each of the four IPV types. Each abuse-related question was put into one of the four IPV type categories (ie, Controlling behavior, Emotional abuse, Physical violence, Sexual abuse). Survey responses were dichotomized (0-No/1-Yes). The list of IPV questions and responses used in this study as well as how questions were categorized can be found in Table 1. Information on the following socioeconomic, head of household (HoH), and health care decisions variables were obtained by asking participants the following questions: “How would you classify your socioeconomic status (SES)?”, “Who is the head of your household?”, “Who in your household usually has the final say on your own health care?”. Each variable was categorized appropriately: SES (ie, “High”, “Average”, “Low”, “Below the poverty line”), HoH (ie, “I am”, “Sexual partner/spouse”, “Father”, “Mother”, “Other, specify”), health care decisions (ie, “I am”, “Sexual partner/spouse”, “Father”, “Mother”, “Other, specify”).
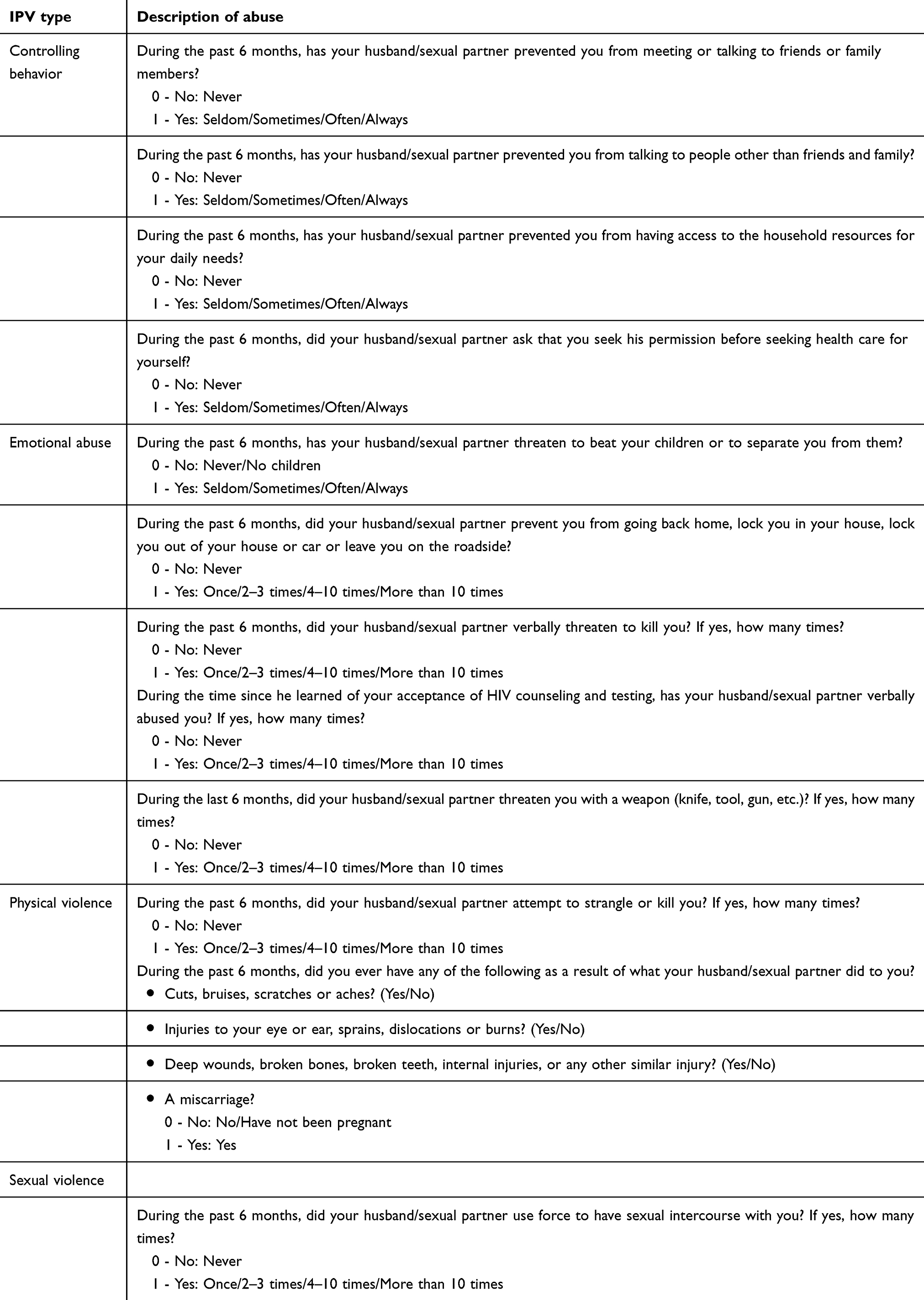 |
Table 1 Abuse questions, responses, and their respective intimate partner violence (IPV) type |
Statistical analysis
The data were imported into SAS (Statistical Analysis System, Cary, NC) version 9.4 and analyzed. Binary variables (No - 0, Yes - 1) were created for the four different IPV types: “emotional abuse”, “controlling behavior”, “physical violence”, and “sexual violence”. Combinations of the different types of IPV experienced by the women were also examined, such as both physical violence and sexual violence or both controlling behavior and physical violence. Descriptive statistics (frequencies and percentages) were computed for all variables, overall and by each IPV type (Table 2). Comparisons were conducted to identify the differences between each sociodemographic variable and across the three of the four IPV types (ie, controlling behavior, physical violence, and sexual violence), using chi-squared tests. Since women’s level of education and employment status are likely to be correlated, a chi-squared test was used to determine if differences in employment status were observed by the level of education.
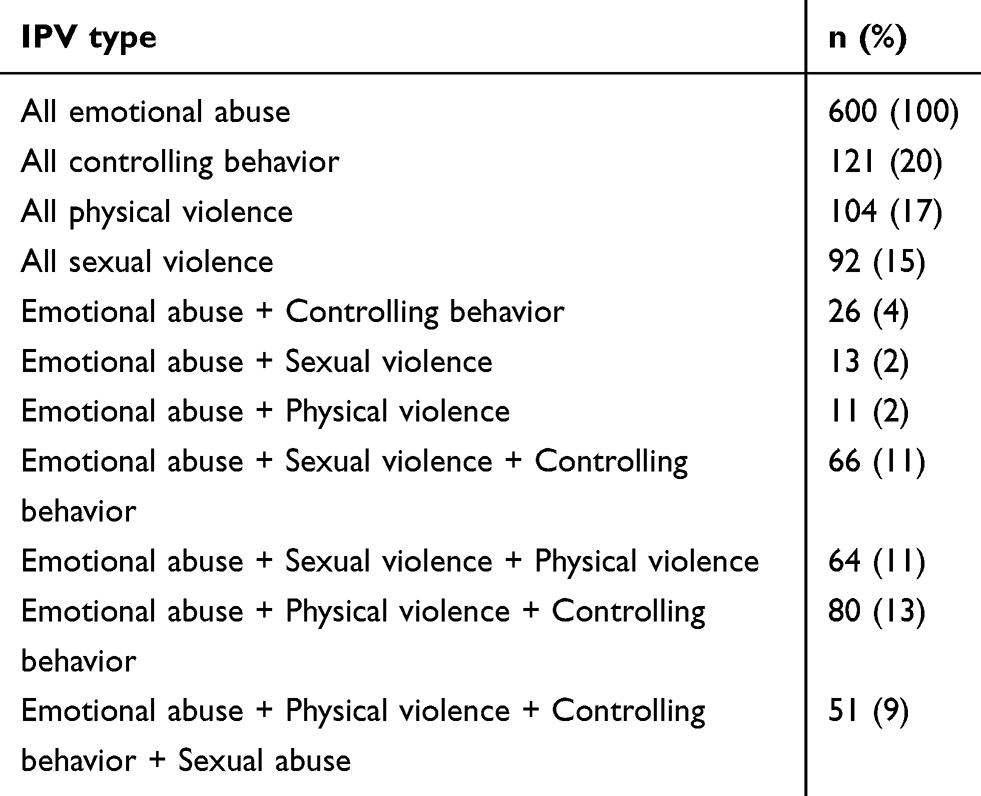 |
Table 2 Intimate partner violence (IPV) types experienced by participants (N=600) |
Multivariable logistic regression analyses were used to explore the adjusted association for two forms of IPV (ie, physical abuse and controlling behavior) as outcomes and covariates that had a p<0.1 using chi-squared tests, as used in other studies.12,28 Since all women experienced emotional abuse, we could only provide frequencies and percentages, as this outcome was not dichotomous. Since only one covariate of sexual abuse had a p<0.1 in the chi-squared test, a multivariable analysis was not conducted for this outcome. In most cases in multivariable logistic models, the most prevalent variable level served as the referent group, however, for the “Level of education” variable the highest ordinal level served as the referent group. Odds ratios were used as a measure of association and 95% confidence intervals were computed. All tests were two-sided and p-values of ≤0.05 were considered significant.
Ethical approval for the study was obtained from the Institutional Review Board of the University of Alabama at Birmingham and the Kenyatta National Hospital/University of Nairobi Ethics and Research Committee. Written informed consent was obtained from each participant prior to enrollment into the study, and the study was conducted in accordance with the Declaration of Helsinki.
Results
The most common IPV type reported was emotional abuse, which was reported by all women. This was followed by controlling behavior (20%), physical violence (17%), and sexual violence (15%; Table 2). Overlaps in IPV types were observed. Of the overlapping IPV types, controlling behavior by spouse/partner was reported by most women who experienced physical (77%, 80/104) or sexual (72%, 66/92) IPV (Table 2). Moreover, physical IPV was reported by 70% (64/92) of women who experienced sexual IPV (Table 2).
Most of the women were 36–45 years old (41%), lived in an urban setting (91%), were married (70%), had a relationship duration of 10 or more years (41%), had a household of <5 people (69%), had 1–2 kids (64%), had a secondary education (38%), had a spouse with college/vocational education (45%), were employed (46%), Christian (96%), were not HoH (64%) and made their own healthcare decisions (79%) (Table 3). Table 3 also displays the frequencies and percentages by IPV type as well as p-values from chi-squared tests. Differences were observed in women’s employment status and SES between women controlling behavior and between women who did and did not report physical violence, using chi-squared tests. While differences in religion were observed between women who did and did not report physical violence and between women who did and did not report sexual abuse, using chi-squared tests. There was a significant association between employment status and women’s level of education level (p<0.0001) among study participants, with unemployment being highest among women with a primary education (44%). Meanwhile, only 25% and 13% of the women with secondary and college/vocational education, respectively, were unemployed. Table 4 displays the crude and adjusted odds ratios (aOR) by IPV type. Several sociodemographic variables were significantly associated with the IPV types. Women who reported low and below average SES had higher odds of experiencing controlling behavior than women reporting average-high SES (aOR =1.62, 95% CI 1.05–2.51). Those who were unemployed had greater odds of experiencing physical violence than those who were employed (aOR =2.35, 95% CI 1.31–4.23). Women who were non-Christian had increased odds of experiencing physical and sexual violence than Christian women (aOR =4.41, 95% CI 1.81–10.76 and aOR =3.33, 95% CI 1.43–7.80).
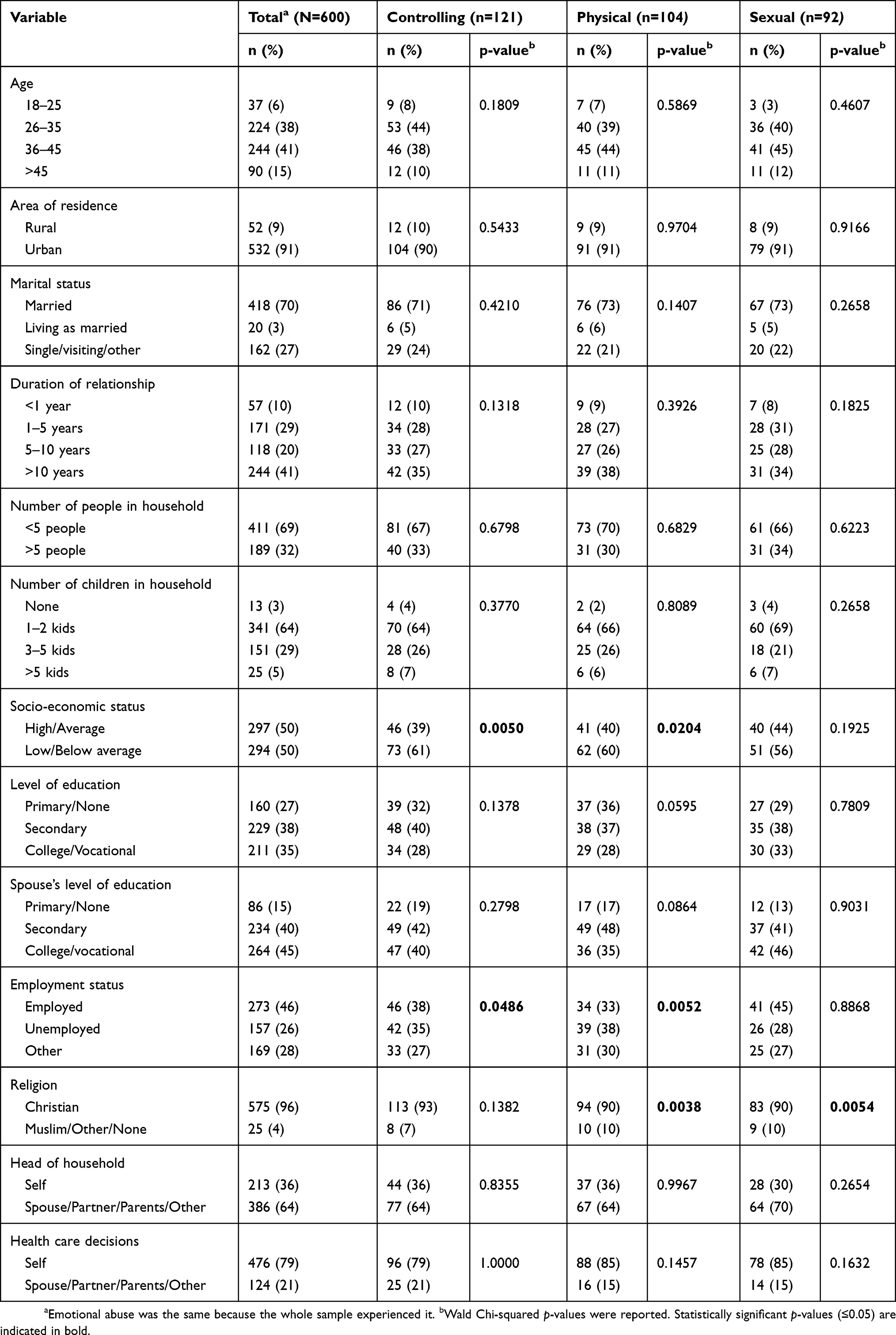 |
Table 3 Sociodemographic characteristics of study participants by intimate partner violence (IPV) type (N=600) |
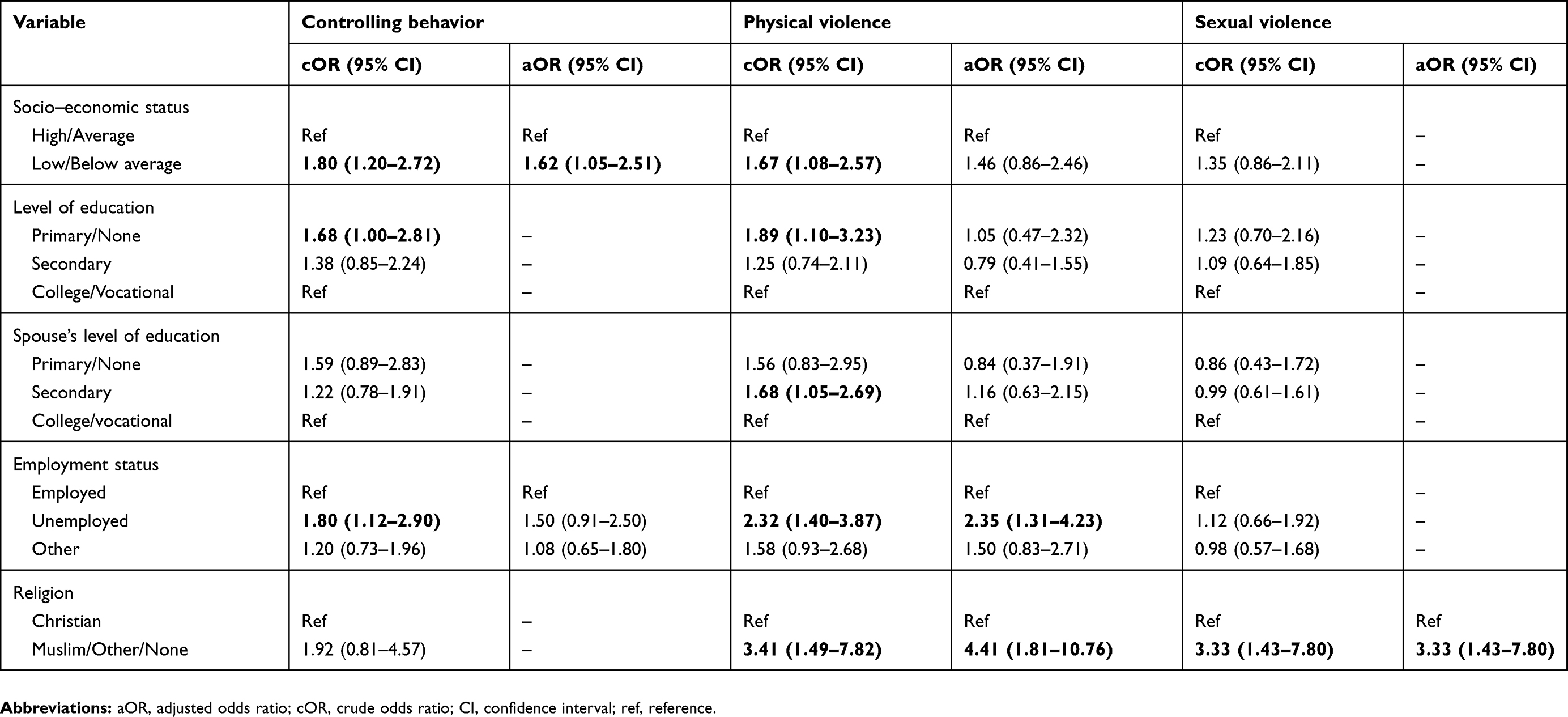 |
Table 4 Logistic regression: crude odds ratios (cORs) and adjusted odds ratios (aORs) and 95% confidence intervals by intimate partner violence (IPV) type |
Discussion
This study evaluated the prevalence and sociodemographic factors associated with IPV among HIV-positive women attending the CCC at KNH in Nairobi, Kenya. All women in this study reported experiencing emotional abuse; 20%, 17%, and 15% experienced controlling behavior, physical violence, and sexual violence, respectively. Characteristics associated with IPV included, low/below average SES, unemployment, and religion other than Christian.
While the prevalence of emotional IPV was higher in this study than in others, it is not surprising that it is the most prevalent of all four forms of IPV. Other studies among women in sub-Saharan Africa have also identified emotional/psychological IPV as the most prevalent form of IPV, with emotional/psychological IPV prevalence ranging from 21% among women in Rwanda to 85% among women in Nigeria.2,16–18 One reason for the higher prevalence of emotional IPV may be differences in survey questions between studies. The higher prevalence may also be attributed to HIV-positive status, as one study among HIV-positive Rwandan women found that psychological IPV and the overall IPV among married women were significantly correlated with HIV risk.29 Considering that emotional abuse is commonly preceded or accompanied by other forms of IPV, it is important to make note of the elevated prevalence among this group of women and also be sure to screen and monitor them for other forms of IPV.30–32
While the current study did not evaluate differences in odds of physical and sexual IPV among women who did and did not report controlling behavior like Durevall & Lindskog, frequencies and percentages of overlapping IPV types were reported.14 Of the overlapping IPV types, controlling behavior by spouse/partner was observed among most women who reported physical (77%, 80/104) or sexual (72%, 66/92) IPV. Taking this finding into consideration, HIV-positive women who experience controlling behavior should be screened for other IPV types. Moreover, this association may be worth further exploration.
Socioeconomic status
Participants who reported low/below average SES had a greater likelihood of experiencing controlling behavior than women with high/average SES. This finding is supported in the literature.33,34 It is likely that women with lower SES live in underprivileged neighborhoods with partners who feel they have limited control over their economic situations. As a result, these partners may exhibit more controlling behavior than those with higher SES. Benson et al (2003) reported that neighborhood economic disadvantage and subjective financial strain influence the likelihood of IPV against women.35 In addition, the WHO reported that in addition to stress, men living in poverty may also be susceptible to other factors associated with low SES, including overcrowding, hopelessness, frustration, and a sense of inadequacy.36 Taking these findings into consideration, it is likely that lower SES may be accompanied by other environmental factors that make these women more susceptible to experiencing controlling behavior from their partner than women with higher SES, as these conditions make men more likely to perpetrate controlling behavior. Since HIV-positive women who experience controlling behavior by a spouse/partner are more likely to report other forms of IPV than those who do not experience controlling behavior, special attention should be given to women with low SES, as they may be at an even greater risk of experiencing other IPV types.13
Employment status
Women who were unemployed had greater odds of experiencing physical violence than those who were employed. Similarly, a study by Kwagala et al (2013) found that Ugandan women who were professionally employed had a lower likelihood of physical IPV than those who were not.24 Furthermore, according to the WHO unemployed women may be more likely to stay with their partner despite violence, as they are financially dependent on them.2 While there was no significant association between women’s level of education and IPV in the current study, there was a significant association between unemployment and education level (p<0.0001) among study participants, with unemployment being highest among women with a primary education (44%). Meanwhile, only 25% and 13% of the women with secondary and college/vocational education, respectively, were unemployed. Given these findings, employment (and possibly higher education) may empower women and increase their likelihood of leaving a physically violent relationship. Educating and engaging men in violence prevention efforts through programs like Men as Partners and MenEngage may also be essential, as financial empowerment of women may result in greater IPV if men are not accepting of women being empowered, as some studies have found greater IPV risk among employed women than unemployed women.37,38
Religion
This study found that non-Christian women had higher odds of experiencing physical and sexual violence than Christian women. In contrast, Ahinkorah et al (2018) found that religious affiliation influenced women’s experience of IPV in sub-Saharan Africa, with non-Muslim women being more likely to experience IPV than Muslim women.37 Cunradi et al (2002) found a positive association between religion and IPV among women in the US.39 Meanwhile, others noted how religion could be used to keep women in abusive relationships, particularly when confronted with religious teaching discouraging them from seeking help or when the need to forgive abuser and pray/hope for change were highlighted.40–43 Given these findings and the lack of studies considering religion as it relates to IPV among women in sub-Saharan Africa, differences by religion were evaluated in this study. The differences in religion were particularly large with an underrepresentation of non-Christians and an overrepresentation of Christians in our sample. For this reason, these results should be interpreted with caution. Furthermore, it may be beneficial for future studies to evaluate this association in general, as well as among women in sub-Saharan Africa, since religion can have a positive or negative impact on IPV victims.
Limitations of the study
One limitation of our study is that due to its cross-sectional design, we are not able to establish temporality, or determine when the IPV started. Additionally, lack of temporality may result in recall bias. In an attempt to reduce this bias, we asked women about IPV within the past 6 months. Another limitation may be underestimation of IPV among women in the study due to fear or shame associated with disclosing this type of sensitive information. Verbal verification of inclusion/exclusion criteria was conducted before the survey was administered; however, it is possible that some women may have hidden commercial sex history and therefore social desirability may have been present. Moreover, our findings may not apply to women who are not receiving treatment, as only women who received treatment attended the clinic and were included in the study. Questions related to substance use and/or abuse by spouse were not collected in the survey. Since the association between IPV and substance use/abuse by spouse has been established in the literature, this is a limitation of our study.12,16 The way SES was measured in the survey was also limited, in that specific income information was not captured. Women provided what SES they believed they were in, and in doing so, the measure of SES was not quantifiable. Another limitation of our study is that when we separated and examined the data according to the different types of abuse, the numbers for each type of abuse are small and may affect the true strength of associations and conclusions reported and might have prevented significant findings for variables other than those found significant in the study.
Conclusion
This was the first study to determine the prevalence of IPV and identify sociodemographic factors associated with four types of IPV among HIV-positive Kenyan women who were not sex workers. An additional strength of the study is its large sample size that offers greater representation of HIV-positive women in Nairobi and surrounding areas who were receiving treatment at the major hospital in Kenya. All women experienced emotional IPV, while 20%, 17%, and 15% experienced controlling behavior, physical violence, and sexual violence, respectively. Sociodemographic factors associated with IPV included: (1) low/below average SES, (2) unemployment , and (3) non-Christian religion. In light of these findings, it may be beneficial to include IPV screening as part of routine clinic visits for HIV-positive women in Nairobi. Furthermore, women who report emotional abuse or controlling behavior from spouse should not be overlooked, as these two forms of IPV may precede or accompany physical and sexual IPV. Women who do screen positive for IPV during clinic visits may be referred to existing non-governmental organizations and resources available to battered women in Kenya including: Coalition on Violence Against Women (COVAW-Kenya), Federation of Women Lawyers for Kenya (FIDA-Kenya), Centre for Rights Education and Awareness (CREAW), and the Gender-Based Violence Prevention Network (GBV Prevention Network).44–47 Moreover, additional research should be conducted to further evaluate factors associated with IPV among HIV-positive women in Kenya. Increased funding for anti-IPV programs as well as and changes in policy may also contribute to a reduction in IPV among HIV-positive and other women in Kenya.
Acknowledgments
We thank the nurses at the CCC who facilitated the study and the women who participated in the study. This study was supported by the Minority Health International Research Training (MHIRT) grant no. T37-MD001448 from the National Institute on Minority Health and Health Disparities, National Institutes of Health (NIH), Bethesda, Maryland, USA.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Fustos K Gender-based violence increases risk of HIV/AIDS for women in sub-Saharan Africa. Population Reference Bureau; April 2011. Available from: https://www.prb.org/gender-based-violence-hiv/.
2. World Health Organization. Understanding and Addressing Violence Against Women; 2012. Available from: http://apps.who.int/iris/bitstream/10665/77432/1/WHO_RHR_12.36_eng.pdf.
3. Shi CF, Kouyoumdjian FG, Dushoff J. Intimate partner violence is associated with HIV infection in women in Kenya: a cross-sectional analysis. BMC Public Health. 2013;13:512. doi:10.1186/1471-2458-13-512
4. Population Council. Sexual and gender based violence in Africa: literature review; February 2008. Available from: http://citeseerx.ist.psu.edu/viewdoc/download;jsessionid=8D6627207F50CFA7A1550980F060073B?doi=10.1.1.296.6218&rep=rep1&type=pdf.
5. Human Rights Watch. Hidden in the mealie meal: gender-based abuses and women’s HIV treatment in Zambia; 2007. Available from: https://www.hrw.org/reports/2007/zambia1207/.
6. Rothenberg KH, Paskey SJ, Reuland MM, Zimmerman SI, North RL. Domestic violence and partner notification: implications for treatment and counseling of women with HIV. J Am Med Womens Assoc. 1995;50:87–93.
7. Gielen AC, McDonnell K, Burke J, O’Campo P. Women’s lives after an HIV-positive diagnosis: disclosure and violence. Matern Child Health J. 2000;4(2):111–120.
8. Gielen AC, O’Campo P, Faden R, Eke A. Women’s disclosure of HIV status: experiences of mistreatment and violence in an urban setting. Women Health. 1997;25(3):19–31. doi:10.1300/J013v25n03_02
9. National Bureau of Statistics-Kenya, ICF International. Kenya 2014 demographic and health survey key findings; 2015. Available from: https://www.dhsprogram.com/pubs/pdf/SR227/SR227.pdf.
10. Adudans MK, Montandon M, Kwena Z, Bukusi EA, Cohen CR. Prevalence of forced sex and associated factors among women and men in Kisumu, Kenya. Afr J Reprod Health. 2011;15(4):87–97.
11. Fonck K, Leye E, Kidula N, Ndinya-Achola J, Temmerman M. Increased risk of HIV in women experiencing physical partner violence in Nairobi, Kenya. AIDS Behav. 2005;9(3):335–339. doi:10.1007/s10461-005-9007-0
12. Makayoto LA, Omolo J, Kamweya AM, Harder VS, Mutai J. Prevalence and associated factors of intimate partner violence among pregnant women attending Kisumu District Hospital, Kenya. Matern Child Health J. 2013;17(3):441–447. doi:10.1007/s10995-012-1015-x
13. Wilson K, Deya R, Masese L, et al. Prevalence and correlates of intimate partner violence in HIV-positive women engaged in transactional sex in Mombasa, Kenya. Int J STD AIDS. 2016;27(13):1194–1203. doi:10.1177/0956462415611514
14. Durevall D, Lindskog A. Intimate partner violence and HIV in ten sub-Saharan African countries: what do the demographic and health surveys tell us? Lancet Glob Health. 2015;3(1):e34–e43. doi:10.1016/S2214-109X(14)70343-2
15. Osinde MO, Kaye DK, Kakaire O. Intimate partner violence among women with HIV infection in rural Uganda: critical implications for policy and practice. BMC Women's Health. 2011;11(1):1. doi:10.1186/1472-6874-11-50
16. Onigbogi MO, Odeyemi KA, Onigbogi OO. Prevalence and factors associated with intimate partner violence among married women in an urban community in Lagos State, Nigeria. Afr J Reprod Health. 2015;19(1):91–100.
17. Issahaku PA. Health implications of partner violence against women in Ghana. Violence Vict. 2015;30(2):250–264.
18. Umubyeyi A, Mogren I, Ntaganira J, Krantz G. Intimate partner violence and its contribution to mental disorders in men and women in the post genocide Rwanda: findings from a population based study. BMC Psychiatry. 2014;14:315. doi:10.1186/s12888-014-0315-7
19. Idoko P, Ogbe E, Jallow O, Ocheke A. Burden of intimate partner violence in The Gambia - a cross sectional study of pregnant women. Reprod Health. 2015;12:34. doi:10.1186/s12978-015-0023-x
20. Koenig MA, Lutalo T, Zhao F, et al. Domestic violence in rural Uganda: evidence from a community-based study. Bull World Health Organ. 2003;81(1):53–60.
21. Wandera SO, Kwagala B, Ndugga P, Kabagenyi A. Partners’ controlling behaviors and intimate partner sexual violence among married women in Uganda. BMC Public Health. 2015;15:214. doi:10.1186/s12889-015-1564-1
22. Conroy AA. Gender, power, and intimate partner violence: a study on couples from rural Malawi. J Interpers Violence. 2013;29(5):866–888. doi:10.1177/0886260513505907
23. McClintock H, Trego M, Wang E. Controlling behavior and lifetime physical, sexual, and emotional violence in sub-Saharan Africa. J Interpers Violence. 2019;088626051983587. doi:10.1177/0886260519835878
24. Kwagala B, Wandera SO, Ndugga P, Kabagenyi A. Empowerment, partner’s behaviours and intimate partner physical violence among married women in Uganda. BMC Public Health. 2013;13(1):1112. doi:10.1186/1471-2458-13-1112
25. Antai D. Controlling behavior, power relations within intimate relationships and intimate partner physical and sexual violence against women in Nigeria. BMC Public Health. 2011;11(1). doi:10.1186/1471-2458-11-511
26. The concept of comprehensive care centre (CCC). Kenyaplex.com; 2019. Available from: https://www.kenyaplex.com/resources/7858-the-concept-of-comprehensive-care-centre-ccc.aspx.
27. Pack A, L’Engle K, Mwarogo P, Kingola N. Intimate partner violence against female sex workers in Mombasa, Kenya. Cult Health Sex. 2013;16(3):217–230. doi:10.1080/13691058.2013.857046
28. Prabhu M, Mchome B, Ostermann J, Itemba D, Njau B, Thielman N. Prevalence and correlates of intimate partner violence among women attending HIV voluntary counseling and testing in northern Tanzania, 2005-2008. Int J Gynaecol Obstet. 2011;113(1):63–67. doi:10.1016/j.ijgo.2010.10.019
29. Dude A. Spousal intimate partner violence is associated with HIV and other STIs among married rwandan women. AIDS Behav. 2009;15(1):142–152. doi:10.1007/s10461-009-9526-1
30. Karakurt G, Silver K. Emotional abuse in intimate relationships: the role of gender and age. Violence Vict. 2013;28(5):804–821.
31. Bott S, Guedes A, Goodwin M, Mendoza J Violence against women in Latin America and the Caribbean: a comparative analysis of population-based data from 12 countries; 2019. Available from: https://stacks.cdc.gov/view/cdc/22295.
32. Garcia-Moreno C, Jansen H, Ellsberg M, Heise L, Watts C. WHO multi-country study on women’s health and domestic violence against women: initial results on prevalence, health outcomes and women’s responses. Geneva, Switzerland: World Health Organization; 2019. Available from: https://apps.who.int/iris/handle/10665/43309.
33. Jewkes R. Intimate partner violence: causes and prevention. Lancet. 2002;359(9315):1423–1429. doi:10.1016/S0140-6736(02)08357-5
34. Khalifeh H, Hargreaves J, Howard LM, Birdthistle I. Intimate partner violence and socioeconomic deprivation in England: findings from a national cross-sectional survey. Am J Public Health. 2013;103(3):462–472. doi:10.2105/AJPH.2012.300723
35. Benson ML, Fox GL, DeMaris A, Van Wyk J. Neighborhood disadvantage, individual economic distress and violence against women in intimate relationships. J Quant Criminol. 2003;19(3):207–235. doi:10.1023/A:1024930208331
36. World Health Organization. Preventing intimate partner and sexual violence against women: taking action and generating evidence; 2010. Available from: http://apps.who.int/iris/handle/10665/44350.
37. Ahinkorah BO, Dickson KS, Seidu AA. Women decision-making capacity and intimate partner violence among women in sub-Saharan Africa. Arch Public Health. 2018;76:5. doi:10.1186/s13690-018-0253-9
38. Cools S, Kotsadam A. Resources and intimate partner violence in sub-Saharan Africa. World Dev. 2017;95:211–230. doi:10.1016/j.worlddev.2017.02.027
39. Cunradi C, Caetano R, Schafer J. Religious affiliation, denominational homogamy, and intimate partner violence among U.S. Couples. J Sci Study Relig. 2002;41(1):139–151. doi:10.1111/1468-5906.00106
40. Hassouneh-Phillips D. "Marriage is half of faith and the rest is fear Allah": Marriage and spousal abuse among American Muslims. Violence Against Women. 2001;7(8):927–946. doi:10.1177/10778010122182839
41. Rotunda R, Williamson G, Penfold M. Clergy response to domestic violence: a preliminary survey of clergy members, victims, and batterers. Pastoral Psychol. 2003;52(4):353–365. doi:10.1023/B:PASP.0000016939.21284.a3
42. Stotland N. Tug-of-war: domestic Abuse and the misuse of religion. Am J Psychiatry. 2000;157(5):696–702. doi:10.1176/appi.ajp.157.5.696
43. Bent-Goodley TB, Fowler DN. Spiritual and religious abuse: expanding what is known about domestic violence. Affilia. 2006;21(3):282–295. doi:10.1177/0886109906288901
44. Centre for rights education and awareness. Available from: https://creawkenya.org/ke/.
45. Coalition on violence against women. Available from: https://covaw.or.ke/.
46. Federation of women lawyers for Kenya. Available from: https://www.fidakenya.org/.
47. Gender-Based Violence Prevention Network (GBV Prevention Network). Available from: http://preventgbvafrica.org/.
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.