")
Back to Journals » Risk Management and Healthcare Policy » Volume 15
Interventions on Reducing Exposure to Endocrine Disrupting Chemicals in Human Health Care Context: A Scoping Review
Authors Park J , Lee H, Lee S, Lee H
Received 15 January 2022
Accepted for publication 27 March 2022
Published 26 April 2022 Volume 2022:15 Pages 779—791
DOI https://doi.org/10.2147/RMHP.S358561
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Mecit Can Emre Simsekler
Jeongok Park,1,2 Hyejung Lee,1,2 Sejeong Lee,3 Hyojin Lee3
1College of Nursing, Mo-Im Kim Nursing Research Institute, Yonsei University, Seoul, Korea; 2Yonsei Evidence Based Nursing Centre of Korea: A JBI Affiliated Group, Seoul, Korea; 3College of Nursing and Brain Korea 21 FOUR Project, Yonsei University, Seoul, Korea
Correspondence: Hyojin Lee, College of Nursing and Brain Korea 21 FOUR Project, Yonsei University, Seoul, 03722, Korea, Tel +82-10-4756-0692, Email [email protected]
Purpose: Inevitability of exposure to endocrine disrupting chemicals (EDCs) in daily lives of modern society is increasing interests in developing and implementing interventions to prevent or reduce harmful health effects of EDCs in various academic areas. This is a scoping review of intervention studies aimed at reducing exposure to EDCs in the text of human health care.
Methods: Scoping review methodology was used to explore the extent, range, and nature of current literature. A comprehensive systematic search of PubMed, CINAHL, Cochrane, PcycINFO, EMBASE, and RISS was performed for studies published to date. The authors followed Arksey and O’Malley’s stages; 1) identification of research questions; 2) identification of relevant studies using a total of six electronic databases; 3) study selection; 4) charting the data; and 5) collation, summarization and reporting of the data.
Results: A total of 2114 articles were retrieved, from which 13 articles were included in the final review. Among the 13 studies, 12 conducted interventions regarding dietary modification or replacement of household or personal goods. The duration of interventions ranged from at least three days to a maximum of six months, including six studies with a period of less than ten days. The participants were all healthy populations, eight of which were for adults, three for children or adolescents, and two for families. Outcome of the interventions were measured through concentration of EDCs in urine or/and house air. The effects of the interventions were inconsistent, with 11 studies showing significant changes of EDC concentration while no significant change was found in two studies.
Conclusion: The results indicate a need for randomized controlled trials, participant-centered studies promoting active participation and practices of subjects, studies specifying subgroups of participants, and studies including families as units in interventions.
Keywords: endocrine disruptors, nursing, education, program evaluation, review
Introduction
Endocrine disrupting chemicals (EDCs), or environmental hormones, are defined as exogenous chemicals or mixtures of chemicals that affect health even at very low concentrations by interfering with normal hormonal action.1,2 Since various items used in everyday life contain EDCs, for instance, preservatives such as plasticizers and parabens used in the production of plastics such as phthalates and bisphenol A (BPA) being used in various cosmetics and food containers and terephthalates and polycarbonates being consumed through canned foods and drinks,3–5 unintentional exposure to various EDCs is inevitably increasing in modern society.
EDCs are known to affect various health problems at both physical and psychological levels. Looking at their mechanism of action, EDCs interfere with receptor binding, steroid production, and hormone metabolism.6 EDCs are associated with the incidence of cancers such as prostate cancer,7 diabetes and thyroid problems,8,9 and psychological problems such as anxiety, depression, and aggression.10,11 EDCs have a decisive effect, especially on women’s health problems. They act mainly on female reproductive organs composed of estrogen receptors, which can cause reproductive health problems such as premenstrual syndrome, breast cancer, endometrial cancer, and infertility.12 In particular, EDCs are more fatal for women of childbearing age because exposure to EDCs through placenta or breast milk affects the brain and behavior of fetuses or newborns.13 Previous studies have reported that exposure to parabens during pregnancy showed an association with fetus growth indicators, including exposure to methylparaben and propylparaben decreasing the head circumference of the fetus.14 The urinary concentration of EDCs also showed statistically significant positive correlation with each other among pregnant women, indicating that those who are vulnerable to exposure to one type of EDC are also at higher risk for exposure to another type of EDC.15
Despite the results of various studies on the risks of EDCs to human health, public awareness and knowledge of EDCs have been reported to be low. A qualitative study on public awareness of EDCs revealed that the majority of participants were unaware of EDCs, and even though they were more familiar with some specific EDCs such as pesticides and BPA, their knowledge of the chemicals was limited.16 Previous studies revealed that education on EDCs is not sufficiently provided to the public, including breastfeeding women,17 and that even perinatal health professionals lacked sufficient information about the risks of EDCs during pregnancy.18 Strategies for prevention of exposures to EDCs may include educating the public, clinical professionals, and individuals at higher risk, for example, those using pesticides or paints, as well as developing relevant regulations and providing proper infrastructure by policy makers and authorities.19 Prior to developing and implementing effective strategies to prevent exposure to EDCs, it is necessary to identify measures that have been previously studied and found efficient through existing literature.
Among various methods of literature review, scoping review is an approach to reviewing the literature that to date has received little attention in the research methods literature.20 It was performed to confirm the gap between studies conducted to date and to investigate the scope of study.21 A scoping review is useful when a comprehensive review of a specific area has not been conducted, or when a systematic review cannot be conducted due to the complex or heterogeneous characteristics of target studies.22 Scoping reviews aim to provide an overview of evidence rather than produce a critically appraised or synthesized answer to a particular question.22,23 This study was conducted in accordance with the 5 stages of scoping review presented by Arksey and O’Malley (2005): 1) identifying the research question; 2) identifying relevant studies; 3) study selection; 4) charting the data; and 5) collating, summarizing, and reporting the results.
Considering the impact of EDCs on human health and the degree of risk of exposure to them, preventive intervention is needed to raise awareness and interest in EDCs and actually reduce exposure. Therefore, this study aims to present the direction of future studies by reviewing various intervention studies on reducing exposure to EDCs through the methods of scoping review.
Aim of the Study
The purpose of this study is to explore and summarize intervention studies published to date in order to present implications for the direction of future studies. The specific research questions of this study are as follows:
1. What are the general characteristics of the intervention studies on reducing exposure to EDCs?
2. What are the contents and characteristics of the interventions aimed at reducing exposure to EDCs?
3. What are the outcome variables in the intervention studies on reducing exposure to EDCs?
4. How effective are the interventions provided in the intervention studies in reducing exposure to EDCs?
Materials and Methods
Study Design
This study is a scoping review to present the direction of future studies by analyzing the characteristics and contents of intervention studies on reducing exposure to EDCs.
Search and Study Selection
Academic research databases such as PubMed, CINAHL, Cochrane, PcycINFO, EMBASE, and the Research Information Sharing Service (RISS) were used to search for studies. Data were collected with search criteria “research conducted on humans,” “research published in Korean or English,” and “research conducted in peer review,” without restrictions on the year of publication. First, in order to select search terms, MeSH terms were searched in PubMed for the main keywords of the research question, “endocrine disrupting chemicals” and “intervention.” As a result, the MeSH term for “endocrine disruptors” was searched as “endocrine disruptors,” and the MeSH terms for “intervention” were selected as “nursing,” “education,” “counsel,” “program development,” and “program evaluation.” Multiple terms for the meaning of intervention were selected since this study attempted to comprehensively explore academic domains of intervention for EDCs. Based on the selected MeSH terms, the search was conducted by combining them. In addition, manual search work was performed by checking the references of the selected studies.
The inclusion and exclusion criteria are presented in Table 1. The inclusion criteria were studies that provided intervention for humans regarding EDCs, studies published in English or Korean, and studies that were peer-reviewed. The exclusion criteria were studies on cost effectiveness or the environment, studies regarding techniques for discovering or detecting EDCs in bodies or materials, and studies in which related professionals were mainly involved as participants. The study selection process is shown in Figure 1. A total of 2144 articles were searched, of which the researcher reviewed 1290 titles and abstracts, excluding 854 duplicates. As a result, 14 studies were first selected. Two reviewers screened the full texts of these 14 studies, and as a result, one study was excluded since the outcome variable was environmental health literacy, which was irrelevant to the study aim. As a result, 13 studies were finally analyzed. At the beginning of the study design stage, the authors intended to include various interventions related to EDCs without limitations on the goals of interventions. The search results, however, only included studies with the purpose of reducing exposure to EDCs, from which the title and scope of this study were modified accordingly. Disagreements during the screening process were resolved through discussion between the authors, including the two reviewers.
 |
Table 1 Eligibility Criteria for the Studies |
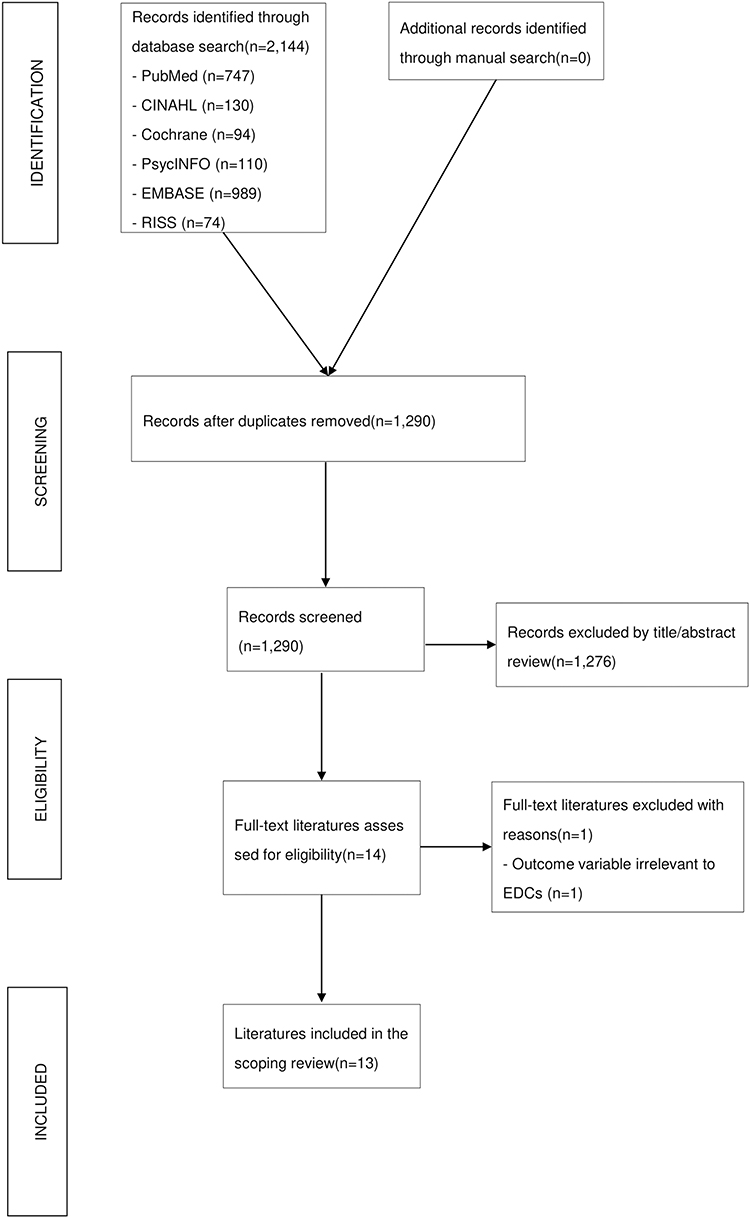 |
Figure 1 Flow diagram of the literature screening process. |
Extracting, Charting, and Analyzing the Data
Prior to data extraction, a data extraction form was developed by the reviewers to aid the process. The form included details concerning year of publication, country, academic domain, study design, author (s), participants, contents of intervention, intervention duration, timing of post-test, primary outcome variables, and findings of the study. They were then classified into three categories to be analyzed as follows: general characteristics of the studies; contents and characteristics of the interventions; and outcome variables and findings, which demonstrated the effectiveness of interventions. First, the general characteristics of the studies included year of publication, country, academic domain, and study design. Next, the contents and characteristics of the interventions included participants, contents of intervention, intervention duration, and timing of post-test. Lastly, the primary outcome variables and results of the study were summarized. Two researchers independently reviewed 13 selected studies and organized the contents according to the data extraction form. The extracted data were documented with Microsoft Excel 2016 and analyzed using descriptive statistics including frequency and percentage.
Results
General Characteristics of the Studies
A total of 13 articles were used for the final analysis, and the analysis results are presented in Table 2. There were one (7.69%) article published in 2011,24 one in each year from 2014 to 2020 which sums up to seven (53.85%),25–31 and five (38.46%) in 2021.32–36 Considering the country where more than half of the authors were from as the country in which the study was conducted, five (38.46%) articles were conducted in the United States,24,26–28,33 four (30.77%) from Europe (UK,29 Poland,31 the Netherlands,32 Italy,36 three (23.08%) from Korea,25,34 and one (7.69%) from China.30 When the academic domain of the study was identified through the journal title and the author’s major or affiliated institution, public health,27,30,33 medicine,26,32,36 nursing,31,34,35 published three (23.08%) articles for each, and environmental science had two (15.38%) articles.24,29 The rest were pharmacy25 and kinesiology,28 one (7.69%) for each. For study designs, seven (53.85%) articles24,26,27,29,31,33,35 used one-group pretest-posttest design, three (23.08%) used randomized controlled trial design,25,28,34 and there were one (7.69%) for each of randomized crossover design,30 randomized factorial design,32 non-equivalent control group pretest-posttest design.36
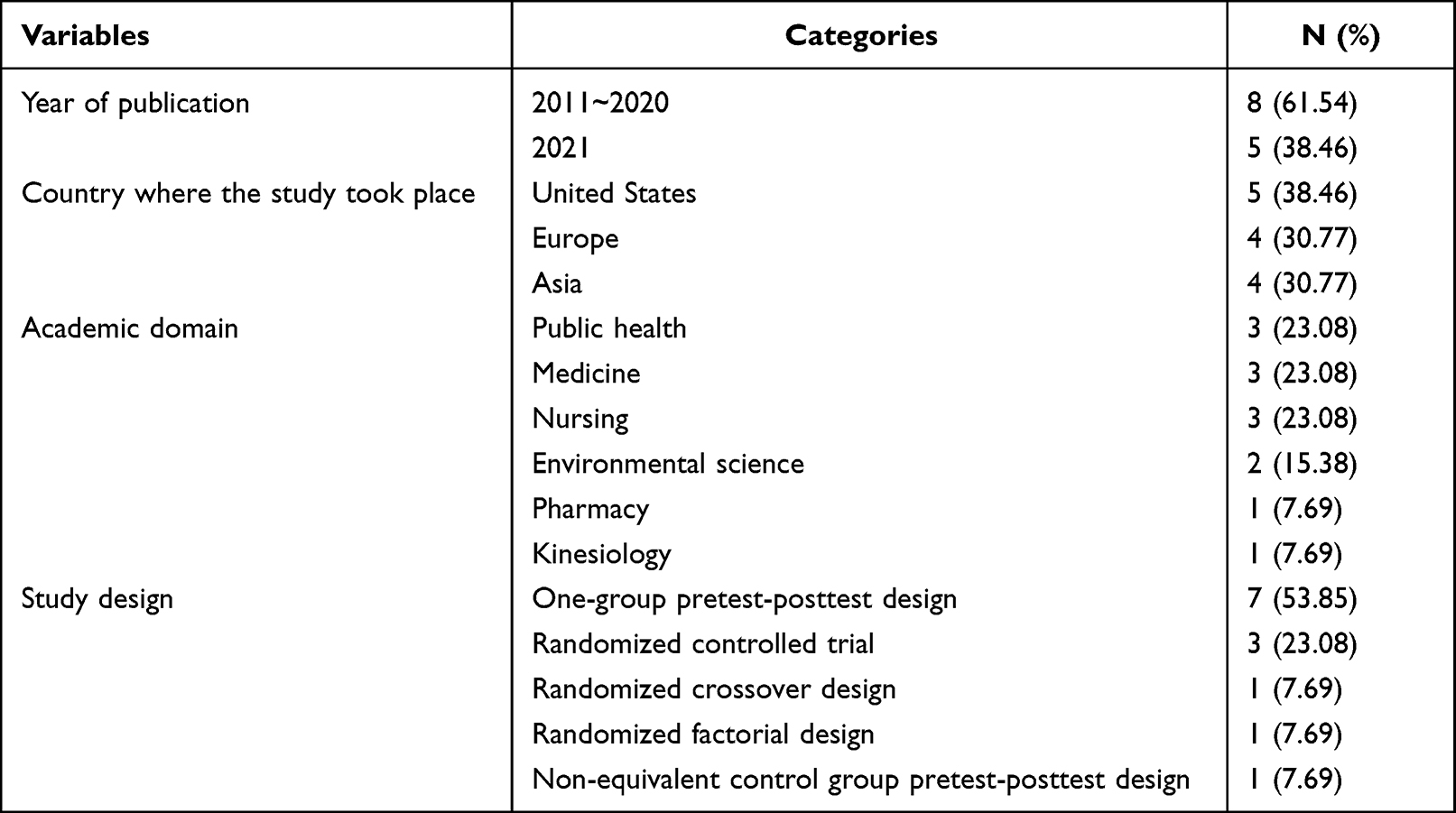 |
Table 2 General Characteristics of the Studies (n=13) |
Contents and Characteristics of the Interventions
Table 3 shows the contents and characteristics of the interventions provided in the studies. There were six (46.15%) studies in which dietary modification interventions were conducted,24,26,29,30,32,35 five (38.46%) with replacement of household or personal products,27,28,31,33,36 and one (7.69%) for each of supplementary food (red ginseng) intake25 and intervention that contained both dietary modification and household or personal product replacement.34 Among the intervention studies on diet modification, five (38.46%) provided food products that contained low levels of EDCs or restricted fast/processed food intake,24,26,29,30,35 and one (7.69%) provided a calorie control intervention.32 In all of the interventions on the use of household or personal products, interventions were conducted to replace existing goods by providing alternative goods with low levels of EDCs.27,28,31,33,36 In the intervention of the study of Kim et al34 educational content including diary modification, replacement of plastic products, and physical activity were delivered through educational videos, games, etc. The duration of interventions ranged from at least three days to a maximum of six months. There were six (46.15%) studies with a period of less than ten days,24,26,27,29,30,33 four (30.77%) studies from ten days to less than ten months,25,28,34,35 and three (23.08%) studies from one month to less than one year.31,32,36
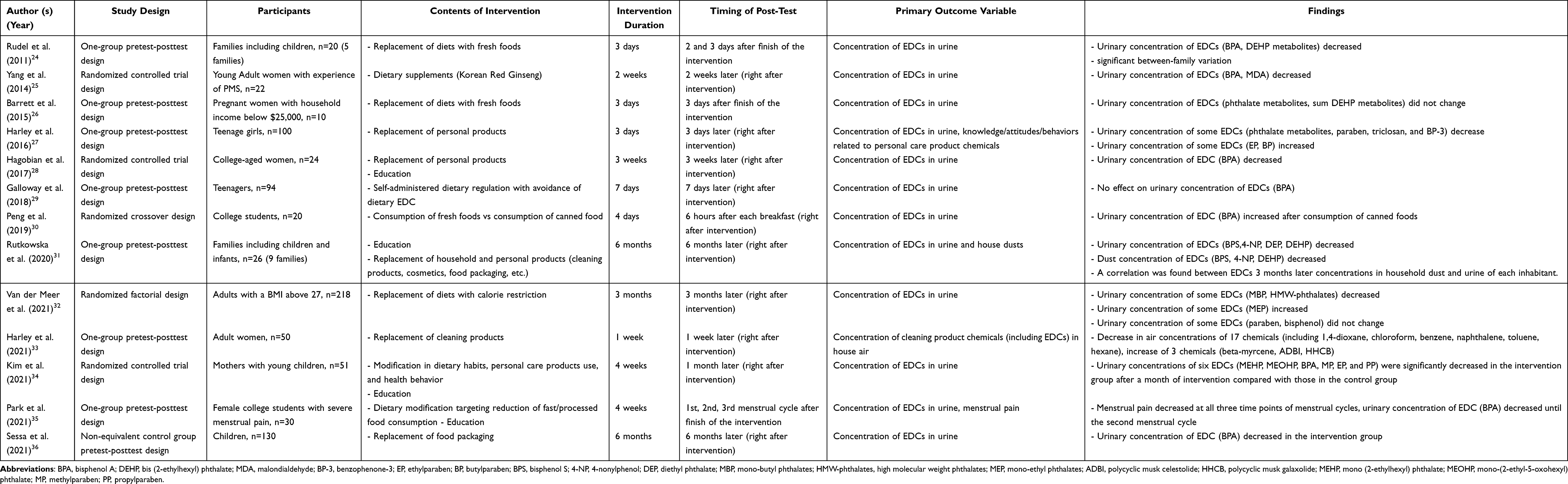 |
Table 3 Contents, Characteristics, Outcome Variables, and Findings of the Studies (n=13) |
Post-tests were conducted right after the interventions in ten (76.92%) studies.25,27–34,36 There were three (23.08%) studies in which post-tests were conducted after a certain period of time since the end of the interventions. Rudel et al 24 and Barrett et al26 conducted post-tests a few days after the finish of the interventions, and three post-tests were conducted on the first, second, and third menstrual period after the finish of the intervention in the study of Park et al.35 The number of participants ranged from ten to 218. All of the studies were for the general public in the community, but there were studies that particularly targeted people with premenstrual syndrome experience,25 severe menstrual pain,35 pregnancy,26 and obesity.32 Eight (61.54%) studies25,26,28,30,32–35 were for adults, while three (23.08%) were for children or adolescents.27,29,36 The remaining two (15.38%) studies recruited families as a unit, and the age groups of the participants were diverse, from newborns to the elderly.24,31 Seven (53.85%) studies limited the participants to women.25–28,33–35
Outcome Variables and Effectiveness of the Interventions
Primary outcome variables and findings are presented in Table 3. As a primary outcome variable for measuring the effectiveness of the interventions, the concentration of EDCs in the body or air was measured in all of the studies. 11 (84.62%) studies measured urine concentration of EDCs,24–30,32,34–36 with one study measuring level of menstrual pain and urine concentration of EDCs. One (7.69%) study measured the air concentration of EDCs in the house.33 Lastly, one (7.69%) study measured the concentration of EDCs both in urine and in dust in the house.31
The effectiveness of the interventions on the management of EDCs was evaluated through each of the study results. As a result of the interventions, 11 (84.62%) studies showed significant changes in the concentration of EDCs in the body or in the house than before the intervention,24,25,27,28,30–36 and no significant change was found in two (15.38%) studies.26,29 Among the studies with significant changes in body concentration, ten (76.92%) studies measured the urine concentration of EDCs,24,25,27,28,30–32,34–36 among which one study measured both the urine and dust concentration of EDCs.31 The other one with a significant change measured the air concentration of EDCs.33
Among the studies showing significant changes, ten (76.92%) studies showed a significant decrease in the concentration of some or all target EDCs in urine, house air, or dust after intervention,24,25,27,28,31–36 and one (7.69%) study showed a significant increase in BPA concentration in urine found in the group who consumed canned food.30 These results confirmed the harmfulness of canned food and the effectiveness of organic or fresh food in the reduction of EDCs in the body or house. In the study with red ginseng intervention, the intervention group, who were provided with 2.7 g of red ginseng daily after meals, showed a decreased urine concentration of BPA and malondialdehyde (MDA) compared to the control (placebo) group.25 It can be implied that red ginseng not only reduces the body concentration of EDCs but also relieves BPA-related oxidative stress. In addition, in the study regarding menstrual pain, dietary modification targeting reduction of fast/processed food consumption was confirmed to be effective in relieving menstrual pain as well as urinary BPA level.35 Meanwhile, three (23.08%) studies have found that the concentration of some chemicals increases after intervention: ethyl and butyl paraben,27 mono-ethyl phthalates,32 beta-myrcene, celestolide, and galaxolide.33
Association of the Concentration of EDCs with Other Variables
Associations between the concentration of EDCs in body or house dust and other variables were also confirmed. First, it was confirmed that the concentration of EDCs was similar among family members. There was a significant between-family variation in BPA level during dietary intervention.24 In another study, electronics use, plastic supplies use, and interior construction of house were associated with high EDC concentration in dust in the house, and all family members of heavy consumption of plastic products in kitchen commonly had high level of EDCs in urine.31 Second, there was a significant positive correlation with the concentration of EDCs in urine and dust.31
Discussion
This study was conducted to analyze the characteristics and contents of intervention studies for the management of EDCs published so far and to evaluate the effectiveness of the interventions. 13 studies were selected, and it was found that the number of studies has increased in recent years and that the studies have been conducted in various areas and academic fields. However, considering that there were no limits on the types of interventions, outcome variables, and publication year during the literature search, the number of studies is clearly insufficient. In terms of the design of the study, more than half of the studies used a design of a single group. Due to their nature, strict experimental designs are difficult to conduct in intervention studies on the management of EDCs which target reducing an individual’s everyday exposure to EDCs. However, it is required to expand designing and conducting randomized controlled trials in the future to confirm the effectiveness of interventions.
The contents of intervention can be largely divided into three categories: diet, use of household goods, and intake of supplementary foods. Among the 13 studies, 12 conducted interventions regarding dietary modification or replacement of household or personal goods, which implies that the types of interventions are skewed. Only four studies provided their participants with education,28,31,34,35 and only four studies let their participants choose alternative goods or foods themselves.29,31,34,35 This shows that the scope of studies and the role of the participants have been limited and passive in the intervention studies of EDCs. In addition, out of a total of 13 studies, six studies provided the interventions for less than ten days,24,26,27,29,30,33 indicating that about half of the interventions lasted for a short time. The timing of post-tests, which were mostly right on the finish of the interventions, also shows that the intervention studies on EDCs conducted to date lack assessment of long-term effects. Behavioral changes, such as changes in dietary habits and using alternative household or personal products, require strategies for maintenance. Even though there were significant changes in outcome variables in the short term, it does not guarantee long-term effects. Since EDCs affect health over a long period of time, interventions that participants can continue to perform on their own and assessment of long-term effects are required. It is expected that lifestyle modification intervention studies, which can be conducted in daily life and are provided along with sufficient education, will be effective to raise awareness of EDCs and thus lead to a reduction in EDC consumption. In particular, practical educational interventions must be implemented so that consumers can learn how to select and use foods or goods containing fewer EDCs.
As for the outcome variable of the studies, the majority of studies were to confirm the concentration of EDCs in the body. Although knowledge and attitude toward EDCs were measured in some studies, it could not be considered that the effect of interventions on them was properly measured. For example, in the study of Harley et al27 EDCs-related knowledge, attitudes, and behaviors were measured after the intervention for replacement of personal goods was provided, but not before the intervention, which makes it impossible to confirm whether the intervention had an effect. To evaluate the effectiveness of interventions comprehensively and in depth, it is needed to conduct studies that assess knowledge and attitudes toward EDCs and variables regarding practices of EDC consumption, and that track long-term changes through longitudinal study methods.
In terms of the participants of the studies, the vulnerability of certain populations to EDCs seems to have been considered. One study provided intervention to pregnant women,26 three studies to children or teenagers,27,29,36 and one study to mothers with young children.35 In the future, it is necessary to expand research by specifying and subdividing vulnerable groups for EDCs and providing customized interventions. For example, considering the influence of EDCs on fertility, couples preparing for pregnancy or infertile couples can be recruited for future studies. Parents with infants and toddlers, who are thought to be highly exposed to EDCs through toys, may also be potential participants in EDC intervention studies.
As a result of the studies, the effect of interventions was inconsistent. Among the studies that included dietary modification, five studies showed the interventions were effective in changing the concentration of EDCs in the body.24,30,32,34,35 However, two studies found their interventions ineffective.26,29 In four of the studies with effective interventions, when the participants consumed or were educated to consume foods with a low level of EDCs, the urine concentration of EDCs was significantly reduced.24,32,34,35 And the concentration was higher in the group with consumption of canned foods in the study of Peng et al 30 Rudel et al 24 and Park et al 35 educated people to consume or provided them with fresh food, which was found effective in lowering EDC levels in the body. The results from the study of Peng et al 30 are in line with those of Van der Meer et al32 Kim et al 34 and Park et al 35 in that the reduction in consumption of calories, fat, or processed foods is efficient in lowering EDC levels in the body. In studies where the intervention results were effective, the types of EDCs measured as indicators could be largely classified into BPA,24,30,34,35 phthalates,24,32,34 and paraben,34 although the indicators varied depending on the studies. In studies of Barrett et al 26 and Galloway et al 29 however, consumption of fresh food and avoiding foods with high levels of EDCs were found to have no effect on changing the EDC level in the body.26,29 In studies that restricted the use of household or personal products or provided alternatives, contradictory research results were found on the effectiveness of interventions. In detail, participants were encouraged to use or were provided with personal hygiene products such as shampoo and body wash that included less chemicals,27,28 cleaning products such as toilet bowl cleaner and dish soap with less chemicals,33 and kitchen ware or food packaging that were plastic-free.28,34,36 Five studies among them reported that the concentration of some or all target EDCs in the body or air decreased,27,28,33,34,36 while some other EDCs were found to have increased in two of them.27,33
The reason why the intervention through alternative diets and household or personal products was ineffective is assumed to be the low level of adherence. According to the study by Park et al 35 56.7% of the participants were categorized as low-adherence groups. Three reasons are thought to have caused the low adherence of the participants. First, exposure to EDCs through various sources is inevitable due to the prevalence of EDCs in industrial products used in everyday life. Among the 13 studies analyzed, there was no study that restricted both food and household or personal products. The target studies only limited exposure to EDCs in a certain part of life, leaving the possibility that EDCs were absorbed through other routes excluded. For example, it was reported that certain types of foods including cookies, dairy products, jelly, sauces, and jams, and personal care products including body wash, mouthwash, makeup base, shaving cream, sunscreen, lotion, and eye makeup products could be sources of exposure to different types and levels of parabens.37,38 Meanwhile, Barrett et al 26 stated that there are so many foods containing EDCs that it is almost impossible to predict and control them all, and that there is a need to reduce exposure to EDCs during the stage of food processing and packaging. In the study by Harley et al33 it is also pointed out that there is no standard definition or designation to help consumers choose household products without chemicals of concern, and that access to alternative products continues to be a problem, particularly in low-income communities. In summary, it is necessary to cultivate the ability of the public as consumers to independently manage EDCs in their daily lives, and at the same time, it is necessary to strengthen regulations on EDCs in the process of supply.
Second, the inappropriate labeling of products containing EDCs needs to be considered. Urine concentration of ethylparaben and butylparaben increased after the intervention of using alternative products for personal hygiene goods in the study of Van der Meer et al32 It is possible that ethylparaben and butylparaben were included in the production process as substitutes for methylparaben and propylparaben, whose concentrations in the body decreased after the intervention; however, whether they were included was not explicit. That is, the specificity and reliability of information on EDCs or other harmful substances in commercial products are not sufficiently provided to customers. Harley et al 27 also mentioned that it should be considered that labeling indicating whether an EDC is present in food may be insufficient or inappropriate. In addition, Galloway et al 29 suggested the improvement of labeling as a way to increase the effect of dietary changes to reduce the absorption of EDCs into the body. In the United States, the Consumer Product Safety Improvement Act (CPSIA) requires that traceable information be indicated on products and packaging for children’s products, and the California state corporation Prop. 65 regulates to indicate whether food containers contain BPA. On the other hand, in Korea, there is currently no independent law on EDCs, and EDCs are regulated as chemicals through several laws on chemicals in general. Therefore, safety or labeling standards that serve as regulatory standards are often insufficient and sometimes conflict with each other.39 It is true that it is difficult to indicate all of the EDC contents since the types and release routes of them are very diverse, but it is still necessary to strengthen and standardize the labeling system indicating the presence of EDCs in food or daily-use products.
Third, in the case of dietary intervention, the resistance of participants to changing their dietary habits can be considered. EDCs are frequently included in processed foods and delivery foods that people in modern society enjoy.40 In the studies that tested eating organic and fresh foods low in EDCs, Galloway et al 29 reported that the study participants were not motivated, expressed dissatisfaction with eating the provided food, and tended not to adhere to the suggestions made by the study. Barrett et al 26 also stated that it would be more realistic and effective to suggest small changes to gradually improve eating habits rather than dietary changes in the form of completely remodeling eating habits in a short period of time. It is necessary to study what factors motivate or induce resistance to change in people’s dietary behaviors, and to conduct intervention studies that include effective strategies for change rather than simply providing alternative foods containing a low level of EDCs.
Finally, it is noteworthy that the concentration of EDCs in the body showed similar trends in members of the family as a unit.24,31 Since food intake and household goods use, which are the main exposure routes to EDCs, are similar among family members, their body concentrations of EDCs tend to be similar as well. Therefore, interventions that target and promote changes not only for individuals but also for families are required. In addition, considering that the concentration of dust in the house showed a significant positive correlation with the concentration of urine, it is necessary to raise awareness of the use of plastic goods and various constructions inside the house that may cause the release of EDCs in the home environment.
Since this study analyzed the intervention programs based on the literature published in academic journals, there is a limit to the actual intervention programs implemented in areas such as schools or communities. In addition, some relevant studies may have been excluded from the analysis since gray literature such as theses were not included in the search. Nevertheless, this study is meaningful in that it presented the direction of intervention studies and policies to reduce exposure to EDCs and suggested promoting education based on the results of analysis on trends in Korean and international studies regarding management of EDCs. In the future, more research is recommended on evaluating the effectiveness of interventions that target reducing exposure to EDCs, by considering the demographic and health-related confounders that may influence results, such as age, sex, education level, body mass index, smoking, and drinking. Conducting a systematic review would be possible as a sufficiently large amount of intervention studies with the same type of EDCs as an outcome variable exist.
Conclusion
This study was conducted to present the direction of future research by analyzing the trends of intervention studies on the management of EDCs using the research method of scoping review.
Although the number of intervention studies conducted has been increasing recently, it is still insufficient in numbers, and most of the studies targeted single groups, which makes it difficult to confirm the effectiveness of the interventions. In addition, as most of the interventions have been carried out in a way that researchers provide substitutes for diets, or household or personal products, the types of interventions were limited, and the role of the participants remained passive. Nearly half of the target studies provided the interventions for less than ten days, with short-term studies dominating. The effectiveness of the interventions showed contradictory research results, and it was confirmed that the concentration of EDCs in the body tended to be similar in the family.
Based on the study results, the following suggestions are made for future research. First, it is necessary to expand the design of randomized controlled trials to confirm the effectiveness and validity of interventions and to provide better evidence for them. Second, a participant-centered study should be conducted that delivers information on EDCs and leads the participants to practice reducing exposure to EDCs on their own. Third, it is necessary to subdivide vulnerable groups in consideration of the health effects of EDCs and expand research on specific subgroups. Fourth, interventions that target families as units to reduce exposure to EDCs in daily life are needed.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, literature search, analysis, and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This research was supported by Basic Science Research Program through the National Research Foundation (NRF) funded by the Ministry of Education (No.2019R1F1A1062769, 2020R1A6A1A03041989) and the Brain Korea 21 FOUR Project funded by the NRF of Korea, Yonsei University College of Nursing (No.F21JB7504007).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Diamanti-Kandarakis E, Bourguignon JP, Giudice LC, et al. Endocrine-disrupting chemicals: an Endocrine Society scientific statement. Endocr Rev. 2009;30(4):293–342. doi:10.1210/er.2009-0002
2. Zoeller RT, Brown TR, Doan LL, et al. Endocrine-disrupting chemicals and public health protection: a statement of principles from the Endocrine Society. Endocrinology. 2012;153(9):4097–4110. doi:10.1210/en.2012-1422
3. Geens T, Roosens L, Neels H, Covaci A. Assessment of human exposure to Bisphenol-A, Triclosan and Tetrabromobisphenol-A through indoor dust intake in Belgium. Chemosphere. 2009;76(6):755–760. doi:10.1016/j.chemosphere.2009.05.024
4. Bach C, Dauchy X, Chagnon MC, Etienne S. Chemical compounds and toxicological assessments of drinking water stored in polyethylene terephthalate (PET) bottles: a source of controversy reviewed. Water Res. 2012;46(3):571–583. doi:10.1016/j.watres.2011.11.062
5. Guart A, Bono-Blay F, Borrell A, Lacorte S. Migration of plasticizers phthalates, bisphenol A and alkylphenols from plastic containers and evaluation of risk. Food Addit Contam Part a Chem Anal Control Expo Risk Assess. 2011;28(5):676–685. doi:10.1080/19440049.2011.555845
6. Sweeney T. Is exposure to endocrine disrupting compounds during fetal/post-natal development affecting the reproductive potential of farm animals? Domest Anim Endocrinol. 2002;23(1–2):203–209. doi:10.1016/S0739-7240(02)00157-1
7. Hu WY, Shi GB, Hu DP, Nelles JL, Prins GS. Actions of estrogens and endocrine disrupting chemicals on human prostate stem/progenitor cells and prostate cancer risk. Mol Cell Endocrinol. 2012;354(1–2):63–73. doi:10.1016/j.mce.2011.08.032
8. Boas M, Feldt-Rasmussen U, Main KM. Thyroid effects of endocrine disrupting chemicals. Mol Cell Endocrinol. 2012;355(2):240–248. doi:10.1016/j.mce.2011.09.005
9. Lind PM, Lind L. Endocrine-disrupting chemicals and risk of diabetes: an evidence-based review. Diabetologia. 2018;61(7):1495–1502. doi:10.1007/s00125-018-4621-3
10. Braun JM, Kalkbrenner AE, Calafat AM, et al. Impact of early-life bisphenol A exposure on behavior and executive function in children. Pediatrics. 2011;128(5):873–882. doi:10.1542/peds.2011-1335
11. Perera F, Nolte ELR, Wang Y, et al. Bisphenol A exposure and symptoms of anxiety and depression among inner city children at 10–12 years of age. Environ Res. 2016;151:195–202. doi:10.1016/j.envres.2016.07.028
12. Mallozzi M, Leone C, Manurita F, Bellati F, Caserta D. Endocrine disrupting chemicals and endometrial cancer: an overview of recent laboratory evidence and epidemiological studies. Int J Environ Res Public Health. 2017;14(3):334. doi:10.3390/ijerph14030334
13. Yuan M, Bai MZ, Huang XF, et al. Preimplantation exposure to bisphenol A and triclosan may lead to implantation failure in humans. Biomed Res Int. 2015;2015:184845. doi:10.1155/2015/184845
14. Hajizadeh Y, Moradnia M, Kiani Feizabadi G, et al. The sex specific association between maternal urinary paraben levels and offspring size at birth. Environ Sci Pollut Res. 2021;28:36029–36038. doi:10.1007/s11356-021-13175-3
15. Hajizadeh Y, Kiani Feizabadi G, Ebrahimpour K, et al. Urinary paraben concentrations and their implications for human exposure in Iranian pregnant women. Environ Sci Pollut Res. 2020;27(13):14723–14734. doi:10.1007/s11356-020-07991-2
16. Kelly M, Connolly L, Dean M. Public awareness and risk perceptions of endocrine disrupting chemicals: a qualitative study. Int J Environ Res Public Health. 2020;17(21):77–78. doi:10.3390/ijerph17217778
17. Kim SH, Jun EY. Factors influencing behavior of reducing exposure to endocrine disrupting chemicals in breastfeeding mothers. Korean J Women Health Nurs. 2018;24(4):423–434. doi:10.4069/kjwhn.2018.24.4.423
18. Marguillier E, Beranger R, Garlantezec R, et al. Endocrine disruptors and pregnancy: knowledge, attitudes and practice of perinatal health professionals. A French multicentre survey. Eur J Obstet Gynecol Reprod Biol. 2020;252:233–238. doi:10.1016/j.ejogrb.2020.06.032
19. Yilmaz B, Terekeci H, Sandal S, Kelestimur F. Endocrine disrupting chemicals: exposure, effects on human health, mechanism of action, models for testing and strategies for prevention. Rev Endocr Metab Disord. 2020;21(1):127–147. doi:10.1007/s11154-019-09521-z
20. Arksey H, O’Malley L. Scoping studies: towards a methodological framework. Int J Soc Res Methodol. 2005;8(1):19–32. doi:10.1080/1364557032000119616
21. Armstrong R, Hall BJ, Doyle J, Waters E. Scoping the scope of a cochrane review. J Public Health. 2011;33(1):147–150. doi:10.1093/pubmed/fdr015
22. Peters, M. D., Marnie, C., Tricco, A. C., Pollock, D., Munn, Z., Alexander, L., ... & Khalil, H. (2020). Updated methodological guidance for the conduct of scoping reviews. JBI Evidence Synthesis, 18(10), 2119-2126.
23. Munn Z, Peters MD, Stern C, et al. Systematic review or scoping review? Guidance for authors when choosing between a systematic or scoping review approach. BMC Med Res Methodol. 2018;18(1):1–7. doi:10.1186/s12874-018-0611-x
24. Rudel RA, Gray JM, Engel CL, et al. Food packaging and bisphenol A and bis (2-ethyhexyl) phthalate exposure: findings from a dietary intervention. Environ Health Perspect. 2011;119(7):914–920. doi:10.1289/ehp.1003170
25. Yang M, Lee HS, Hwang MW, Jin M. Effects of Korean red ginseng (Panax Ginseng Meyer) on bisphenol A exposure and gynecologic complaints: single blind, randomized clinical trial of efficacy and safety. BMC Complement Altern Med. 2014;14(1):1–9. doi:10.1186/1472-6882-14-265
26. Barrett ES, Velez M, Qiu X, Chen SR. Reducing prenatal phthalate exposure through maternal dietary changes: results from a pilot study. Matern Child Health J. 2015;19(9):1936–1942. doi:10.1007/s10995-015-1707-0
27. Harley KG, Kogut K, Madrigal DS, et al. Reducing phthalate, paraben, and phenol exposure from personal care products in adolescent girls: findings from the HERMOSA intervention study. Environ Health Perspect. 2016;124(10):1600–1607. doi:10.1289/ehp.1510514
28. Hagobian T, Smouse A, Streeter M, Wurst C, Schaffner A, Phelan S. Randomized intervention trial to decrease bisphenol A urine concentrations in women: pilot study. J Womens Health. 2017;26(2):128–132. doi:10.1089/jwh.2016.5746
29. Galloway TS, Baglin N, Lee BP, et al. An engaged research study to assess the effect of a ‘real-world’dietary intervention on urinary bisphenol A (BPA) levels in teenagers. BMJ open. 2018;8(2):e018742. doi:10.1136/bmjopen-2017-018742
30. Peng CY, Tsai EM, Kao TH, et al. Canned food intake and urinary bisphenol a concentrations: a randomized crossover intervention study. Environ Sci Pollut Res Int. 2019;26(27):27999–28009. doi:10.1007/s11356-019-05534-y
31. Rutkowska A, Olsson A, Piotrowska-Szypryt M, Namieśnik J. Changes in daily life reduce indoor exposure to selected endocrine disruptors in the home environment: a pilot intervention study. Acta Biochim Pol. 2020;67(2):273–276. doi:10.18388/abp.2020_5369
32. van der Meer TP, Thio CH, van Faassen M, et al. Endocrine disrupting chemicals during diet-induced weight loss–a post-hoc analysis of the LOWER study. Environ Res. 2021;192:110262. doi:10.1016/j.envres.2020.110262
33. Harley KG, Calderon L, Nolan JE, et al. Changes in Latina women’s exposure to cleaning chemicals associated with switching from conventional to “green” household cleaning products: the LUCIR intervention study. Environ Health Perspect. 2021;129(9):97001. doi:10.1289/EHP8831
34. Kim JH, Kwak JM, Kang H. Web-based behavioral intervention to reduce exposure to phthalate metabolites, bisphenol A, triclosan, and parabens in mothers with young children: a randomized controlled trial. Int J Hyg Environ Health. 2021;236:113798. doi:10.1016/j.ijheh.2021.113798
35. Park S, Chung C. Effects of a dietary modification intervention on menstrual pain and urinary BPA levels: a single group clinical trial. BMC Womens Health. 2021;21(1):1–9. doi:10.1186/s12905-021-01199-3
36. Sessa F, Polito R, Monda V, et al. Effects of a plastic-free lifestyle on urinary bisphenol A levels in school-aged children of Southern Italy: a pilot study. Front Public Health. 2021;9:4. doi:10.3389/fpubh.2021.626070
37. Hajizadeh Y, Kiani Feizabadi G, Feizi A, Ebrahimpour K. The association of personal care products uses and dietary habits with the urinary concentration of parabens in Iranian adults. Int J Environ Health Res. 2022;32(4):291–807. doi:10.1080/09603123.2020.1798362
38. Hajizadeh Y, Kiani Feizabadi G, Feizi A. Dietary habits and personal care product use as predictors of urinary concentrations of Parabens in Iranian adolescents. Environ Toxicol Chem. 2020;39(12):2378–2388. doi:10.1002/etc.4861
39. Cho TJ, Lee H. Current status and tasks of endocrine disruptor management in Korea. J Law Polit. 2018;18(2):73–107. doi:10.17926/kaolp.2018.18.2.73
40. Bang DY, Kyung M, Kyung M, Kim MJ, et al. Human risk assessment of endocrine disrupting chemicals derived from plastic food containers. Compr Rev Food Sci Food Saf. 2012;11(5):453–470. doi:10.1111/j.1541-4337.2012.00197.x
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.