")
Back to Journals » Patient Preference and Adherence » Volume 14
Interventions Incorporating Therapeutic Alliance to Improve Hemodialysis Treatment Adherence in Black Patients with End-Stage Kidney Disease (ESKD) in the United States: A Systematic Review
Authors Blumrosen C, Desta R , Cavanaugh KL , Laferriere HE , Bruce MA , Norris KC , Griffith DM , Umeukeje EM
Received 7 May 2020
Accepted for publication 10 July 2020
Published 17 August 2020 Volume 2020:14 Pages 1435—1444
DOI https://doi.org/10.2147/PPA.S260684
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Johnny Chen
Charlotte Blumrosen,1 Russom Desta,2 Kerri L Cavanaugh,3,4 Heather E Laferriere,5 Marino A Bruce,6 Keith C Norris,7 Derek M Griffith,8 Ebele M Umeukeje3,4
1Case Western Reserve University School of Medicine, Cleveland, OH, USA; 2Meharry Medical College, Nashville, TN, USA; 3Vanderbilt Center for Kidney Disease, Nashville, TN, USA; 4Division of Nephrology, Vanderbilt University Medical Center, Nashville, TN, USA; 5Eskind Biomedical Library, Vanderbilt University Medical Center, Nashville, TN, USA; 6Department of Population Health Science, John D Bower School of Population Health, University of Mississippi Medical Center, Jackson, MS, USA; 7Division of General Internal Medicine and Health Services Research, UCLA, Los Angeles, CA, USA; 8Center for Research on Men’s Health, Vanderbilt University, Nashville, TN, USA
Correspondence: Ebele M Umeukeje
Division of Nephrology, Vanderbilt University Medical Center, Nashville, TN, USA
Tel +1 615 936-3283
Fax +1615 875-5626
Email [email protected]
Background: In the US, Blacks with end-stage kidney disease (ESKD) have a four-fold higher prevalence rate of hemodialysis treatment and higher subsequent rates of hemodialysis treatment nonadherence and hospitalization compared to their White peers. Nonadherence to prescribed dialysis therapy is an underestimated life-threatening behavior, because of its association with increased morbidity and mortality. Few studies have specified and systematically evaluated targeted methods of increasing hemodialysis treatment adherence among Black hemodialysis patients with added focus on therapeutic alliance, a rewarding patient-centered relationship between patients and providers, based on common goals and objectives. This review seeks to evaluate the state of the science to determine the salience of a therapeutic alliance for the development of effective interventions positively impacting hemodialysis treatment adherence among Black patients.
Methods: Medline (via PubMed), Embase (OvidSP), Cumulative Index of Nursing and Allied Health Literature (CINAHL; EBSCOhost), and PsycInfo (ProQuest) databases were used to search for abstracts with the keywords “dialysis”, “therapeutic alliance”, and “treatment adherence and compliance”, including all underlying index terms and alternative variations of terms, in order to cover the entire scope of the field. Only randomized clinical trials and pre/postintervention studies published in the previous 10 years (2009– 2019) and including a proportion of Black patients > 25% were included for review.
Results: Only three intervention studies met these criteria, for a total aggregated sample of 130 — mean age 58.1 years and 53% female. None of these studies was composed exclusively of Black patients (range 62%– 91.3%), nor did they present data specifically for Blacks. Despite the lack of robust data informing strategies to improve hemodialysis adherence among Blacks with ESRD, a limited number of intervention studies have reported positive effects on hemodialysis attendance.
Discussion/Conclusion: Further research is warranted to fill this significant gap in our understanding of theoretically based, therapeutic alliance–enhanced, and culturally tailored hemodialysis treatment–adherence interventions among Blacks.
Keywords: dialysis, adherence, ESKD, African Americans, systematic review, hemodialysis
Introduction
End-stage kidney disease (ESKD) affects over 725,000 people in the US according to the latest US Renal Data Systems Annual Report.1 High morbidity in ESKD results in high hospitalization rate as high as 1.73 per patient year, twice the hospitalizations of other age-matched patients with chronic conditions, with up to 35% rehospitalizations.2 The financial implication is daunting, with ESKD utilizing more than 7% of the Medicare budget at nearly $40 billion each year, while accounting for <1% of the Medicare population.1–4
Nonadherence to prescribed hemodialysis therapy is a strong driver of poor outcomes among hemodialysis patients.5 Missing one or more hemodialysis treatments versus not missing any treatments in 1 month is associated with ~68% higher mortality.6 Up to 35% of hemodialysis patients miss their treatment appointments, and additionally 32% of those who make their hemodialysis appointments leave prior to their scheduled completion.5 Missed treatments are broadly classified into those arising from situations outside a patient’s control, such as transportation challenges and inclement weather, and those within a patient’s behavioral decision control, ie. behavioral nonadherence.6 Black patients treated with dialysis have a four-fold higher ESKD prevalence,2 higher rates of nonadherence to prescribed dialysis treatments,7 and four-fold higher hospitalization rates compared to Whites.5 Nonetheless, despite its critical importance, there are scant data describing interventions addressing hemodialysis treatment nonadherence among Blacks.
Health behavior–change interventions are most successful when informed by behavioral theory.8 A theory is a logical collection of ideas and concepts that organize, predict, and explain behavior.9 Theoretical models of behavior facilitate the understanding of health behavior and assessment of effectiveness of an intervention.8 In the context of improving patient adherence in chronic illness, application of behavioral theory has been recommended to aid better understanding of predictors of behavioral nonadherence and inform intervention development.8,10,11 Such behavioral theories such as the theory of planned behavior, common-sense model, and motivational interviewing empower hemodialysis patients, promote patient engagement critical for patient care and improved outcomes, and offer insight into improving adherence in ESKD.12 However, the frequency with which hemodialysis treatment–adherence studies incorporate interventions grounded in these or other pertinent theoretical models is not known.
Therapeutic alliance is an indirect predictor of nonadherence and self-care in ESKD.13 In this alliance, the patient and provider prioritize patient-identified behaviors and beliefs and agree on intervention objectives by building confidence, skills, and motivation to implement and sustain behavioral change.8 The likelihood of behavior change–intervention effectiveness is contingent upon the development of a therapeutic alliance, or a shared understanding of the behavioral problem between the patient and provider. Improved therapeutic alliance is key to optimizing patient activation, an unaddressed opportunity in kidney-disease management.14 Patient activation is very low among ESKD patients,15 and Black patients with ESKD have lower patient-activation scores than their White peers.16 Enhancing patient activation and self-care by strengthening therapeutic alliance could be an important strategy to mitigate racial/ethnic disparities in hemodialysis treatment adherence and improve overall outcomes for patients with ESKD.17
Despite the substantial evidence of reduced hemodialysis treatment adherence among Blacks, no report to our knowledge has systematically reviewed the hemodialysis treatment–adherence literature specifically on Blacks to garner input that will inform clinical practice and research. Nor do there appear to be any reports that have undertaken an assessment of the application of theoretical frameworks or the inclusion of therapeutic alliance to enhance the success of interventions targeting improvement in hemodialysis treatment adherence. The purpose of this paper is to systematically review experimental and quasiexperimental interventions employing a therapeutic alliance strategy to improve hemodialysis treatment adherence including among Blacks with ESKD undergoing hemodialysis, and to investigate the use of health-behavior theories to enhance the rationale and understanding of the findings specific to the tested interventions.
Methods
This systematic review followed the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) checklist. Studies were limited to randomized trials and pre–post intervention studies published in English as fulltext articles between January 2009 and July 2019 evaluating interventions to improve adherence to hemodialysis in ESKD-patient populations comprised of over 25% Blacks. The timeline of this review was driven by the need to focus on more recent literature, especially given the existence of a previous systematic review of interventions to improve adherence to dialysis treatment, medication, fluid, and diet, which included randomized controlled trials conducted up to 2008, though not specific to the population of interest.18 The cutoff of 25% Blacks in the selected studies was chosen because it inspired enough confidence that there were enough Blacks in the sample to deduce that the findings were applicable to our population of interest. The review was registered with, the International Prospective Register of Systematic Reviews (PROSPERO; CRD42019145736).
Data Sources and Searches
Electronic database searches were performed on Medline (via PubMed), Embase (OvidSP), Cumulative Index of Nursing and Allied Health Literature (CINAHL; EBSCOhost), and PsycInfo (ProQuest) for relevant articles using standard search terms. Medline MeSH terms included combinations of “renal dialysis” or “hypertension” or “kidney failure, chronic” or “renal insufficiency” and “therapeutic alliance” or “motivational interviewing” or “social support” or “directive counselling” or “patient care team” or “patient care management” and “hospitalization/statistics and numerical data” OR “patient compliance” OR “treatment adherence and compliance”, including all underlying index terms and alternative variations of terms, in order to cover the entire scope of the field. Search results were restricted to English-language articles from 2009 to 2019. The search strategy used for Medline and other databases is provided in Appendices 1–4. Titles and abstracts were evaluated by two independent reviewers (CB and RD) to identify articles to be included in the final review. Disagreement was resolved by discussion among all the authors until consensus was reached. Additionally, references of articles included and other previous reviews were hand-searched for articles that may have been missed by the database searches.
Study Selection
Studies that described adult patients living with ESKD who were undergoing hemodialysis were considered. Studies were included if they described a pre–post quasiexperimental or experimental design, had >25% Blacks in the study population, reported data on one of the measures of hemodialysis adherence (hemodialysis attendance or length of hemodialysis session as a predefined primary or secondary outcome), and were conducted in the US. The reported measure of adherence could be indirect (self-reported adherence) or direct (chart review of attendance). Studies that assessed surrogate measures of treatment adherence, such as hospitalizations, morbidity, and mortality, were assessed in order to ensure an exhaustive search of hemodialysis treatment–adherence intervention studies.
Data Extraction and Quality Assessment
A standard checklist developed by the full team of authors was used to extract the following data from the studies included: publication year, first author’s name, journal, study design, number of participants, study-population characteristics, study location, enrollment period and criteria, intervention type, adherence measure, underlying theoretical model of behavior, and measures of adherence before and after the intervention. If the intervention resulted in improvement in the prespecified adherence measure, the study outcome was considered positive. One author (CB) extracted the information and another author (RD) verified its accuracy. An assessment of bias in included studies was done using modified versions of the Cochrane RoB 2.0 and ROBINS tools, modified by the team of authors, refined by two authors, and then utilized for evaluation of included studies.
Data Synthesis and Analysis
We provide detailed description of the study design, study measures, outcome measures, methodology, theoretical framework, therapeutic alliance, and main findings of each study. Studies were included if they met the inclusion criteria. In addition to summarizing each study and identifying the limitations of our review, we describe patterns that emerged from looking across the studies and then discuss the strengths and weaknesses of this body of literature.
Results
Search Results
Electronic searches to identify relevant articles were completed on July 2, 2019 using the aforementioned search strategies. The broad electronic database search retrieved 854 citations, of which 70 potential studies were identified based on the inclusion criteria. After the abstracts for these 70 citations had been read, 22 studies were deemed eligible based on the inclusion and exclusion criteria. Hand-searching of references from systematic reviews pertinent to the topic did not yield any additional studies. Of these 22 papers, three were found tomeet all the inclusion and exclusion criteria fully. Primary reasons for excluding the other 19 papers were failure to include hemodialysis treatment adherence as an outcome, failure to provide information on race categories in the demographics, and study location outside the US, predominantly in countries without any Blacks in the population (Figure 1).
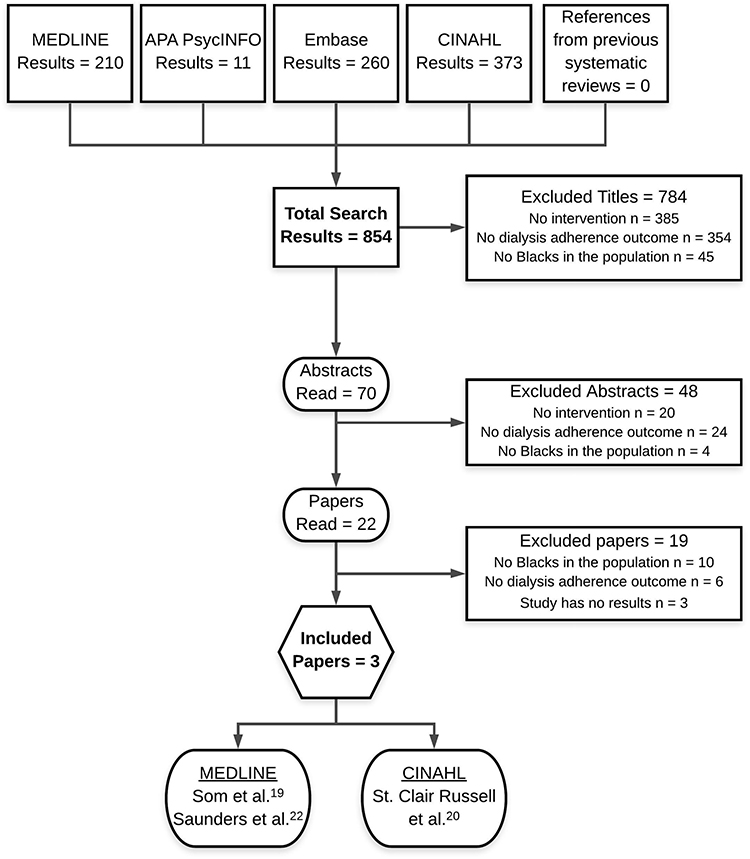 |
Figure 1 Flow diagram showing data sources and study-selection process. |
Study Characteristics
Of the three studies included in this review, one was a randomized controlled trial with a crossover design,19 while the other two were pre–post single-arm intervention studies (Table 1).20,21 All three studies were conducted in university-affiliated hemodialysis centers. Sample sizes ranged from 19 to 65 participants. Mean age was 58.1±6.9 years,and female patients constituted a slight majority (53%±8.9%) of the study participants. All studies recruited patients undergoing in-center hemodialysis, with the exception of the mentor group in the study by St Clair Russell et al, who could also be home-hemodialysis patients or transplant recipients who had previously been dialyzed in the in-center hemodialysis facility.20 Percentage of Black subjects in the studies ranged from 62% to 91.3%, and none of the studies exclusively targeted hemodialysis-adherence improvement in Blacks with ESKD.
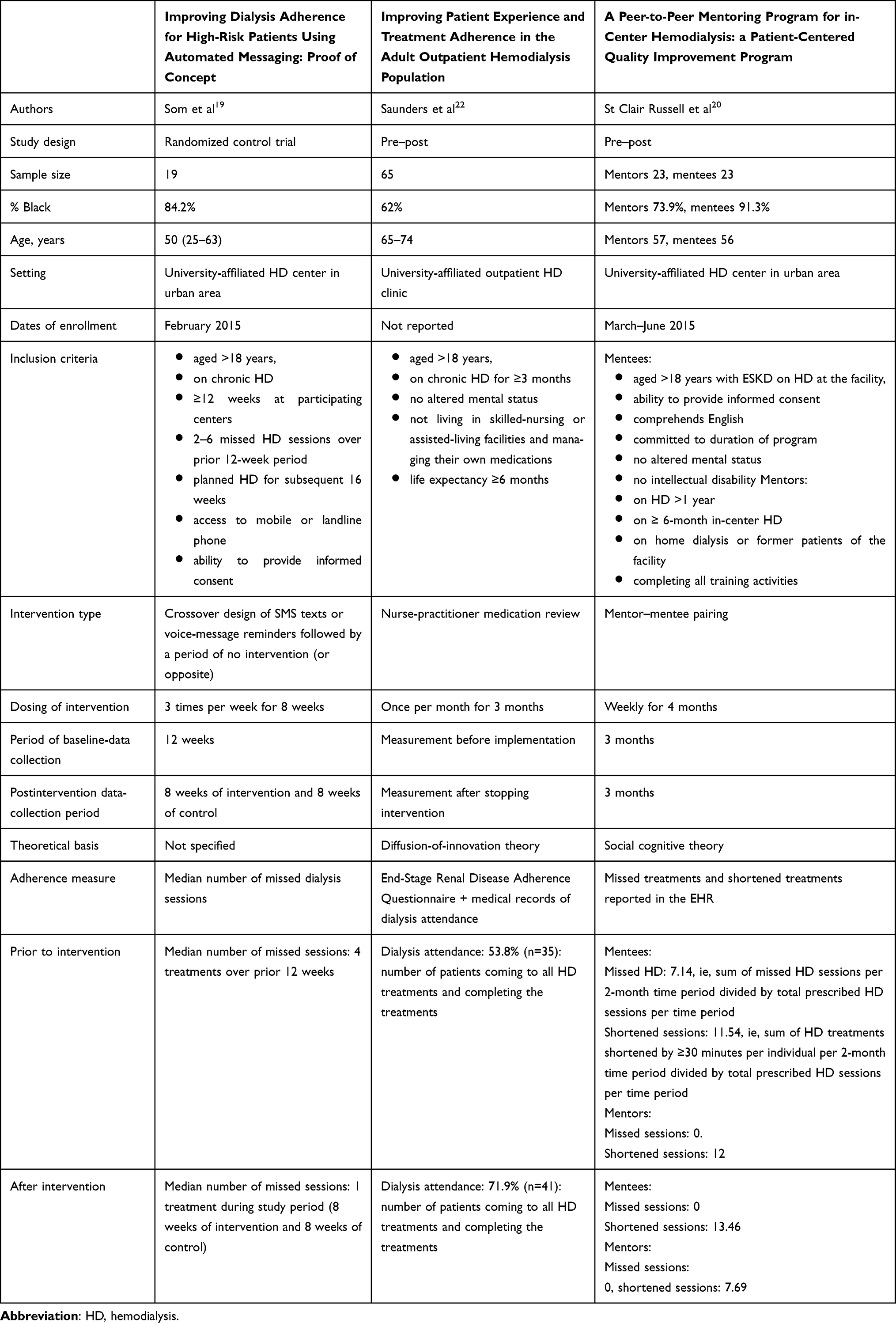 |
Table 1 Descriptive Characteristics of Intervention Studies Assessing HD-Treatment Adherence in Populations with >25% Blacks |
Risk of Bias
The overall risk of bias was judged medium20 and high22 for the pre–post studies and low for the randomized controlled trial.19 The most common risk of bias in all three studies was in the domain of bias in measurement of outcome, given the chance of the outcome measure being influenced by the knowledge of the intervention received. Additional details of the risk-of-bias assessment of individual studies and scoring system are provided in Table 2 and Appendix 5.
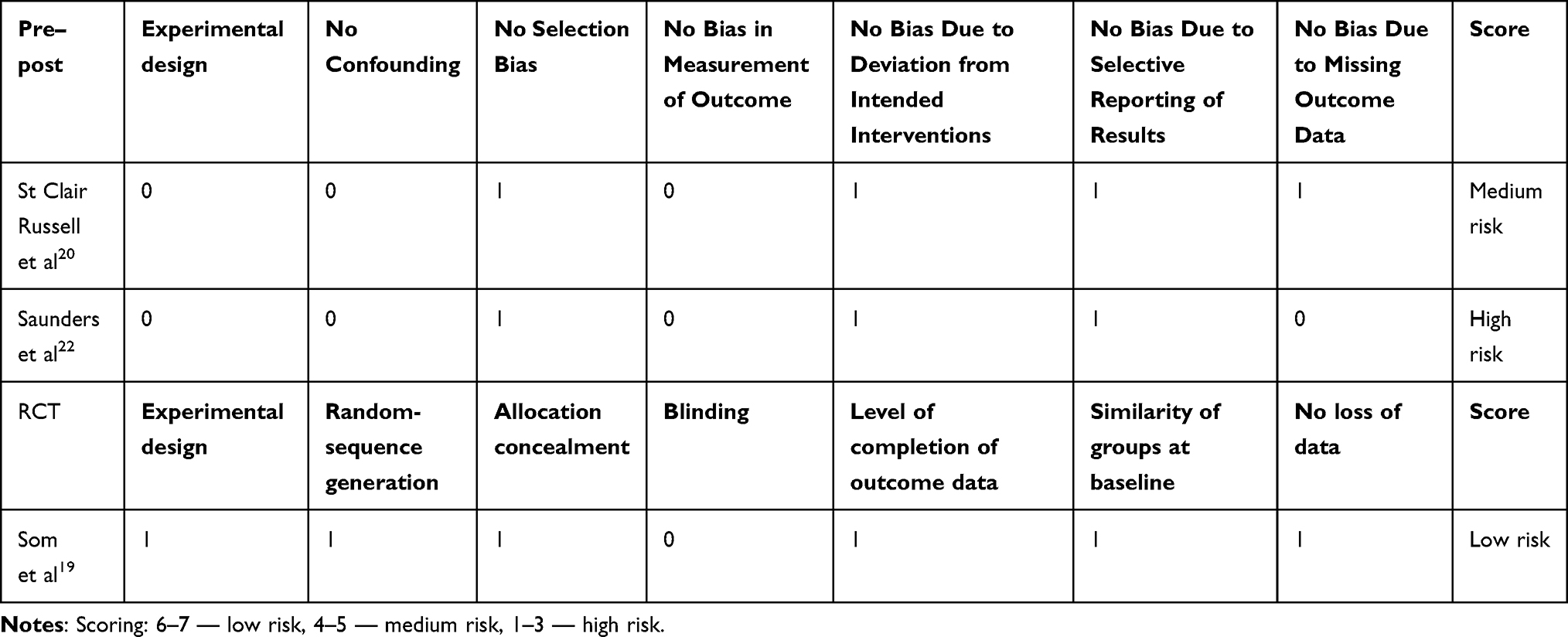 |
Table 2 Assessment of Risk of Bias |
Interventions
The first study evaluated the impact of mentoring.20 St Clair Russell et al conducted a single-arm, 4-month, peer-to-peer mentoring program to improve self-management behaviors of hemodialysis patients. Improvement in adherence metrics, such as missed and shortened treatments and hospitalizations, were monitored.20 In addition to basic kidney information, mentors were trained in leadership, communication skills, relationship-building, and active listening.
Som et al initiated an intervention consisting of automated short message service (SMS) texts or voice messages delivered thrice weekly to the patient’s preferred phone number.19 These messages included details about the subject’s upcoming hemodialysis session, a message of encouragement highlighting the clinic’s supportive role, and an option for direct call routing to the hemodialysis center if the patient could not attend their scheduled hemodialysis. Data on missed treatments and hospitalizations were documented.
Saunders et al implemented a nurse practitioner–led education-and-feedback intervention to improve self-management in adults with ESKD on chronic hemodialysis at an outpatient hemodialysis unit.22 A unique addition to this study was the provision of concurrent pharmacist access, known to improve adherence by reducing the risk of medication-record discrepancies and medication-related problems.23 These different interventions targeted various barriers faced by ESKD patients, especially Black patients, including lack of social or emotional support and limited health literacy preventing an in-depth understanding of medications and importance of hemodialysis treatments.
Health-Behavior Theories and Therapeutic Alliance
Theory-informed interventions were tested in two of the three studies, and the underlying theories were social cognitive theory20 and diffusion-of-innovation theory.22 One of the studies incorporated a multidisciplinary care–focused therapeutic alliance in the form of nurse practitioner–led education and access to a pharmacist, resulting in improved overall self-management practices, including hemodialysis-treatment adherence, among other benefits.22 The remaining two studies incorporated therapeutic alliance via text message and peer mentoring.
Outcome Assessment
All the studies described adherence to hemodialysis treatment in terms of attendance at sessions, but two of the three studies also reported patients’ shortening of hemodialysis sessions as a component of treatment adherence.20,22 These studies also reported other ESKD measures of adherence, including medications and/or fluid restrictions, but these details were not included in this review.
Outcome Efficacy
All three trialed interventions were effective in improving at least one of the hemodialysis treatment–adherence outcome measures, ie, attendance at hemodialysis and/or completion of hemodialysis treatments. Only one of the interventions yielded mixed results, with positive results in the domain of attendance, but not in that of reduction in number of shortened sessions.20
Discussion
The purpose of this paper was to systematically review intervention studies designed to increase hemodialysis treatment adherence through improved patient–clinician interactions that included a significant number of Black patients with ESKD receiving hemodialysis. We found very limited published literature on this critical and timely topic associated with ESKD morbidity and mortality. All three studies incorporated therapeutic alliance via text messaging, peer mentoring, or nurse practitioner–led intervention.19,20,22
The likelihood of successfully enacting a positive behavior change and solving a clinical problem often depends on the use of appropriate theoretical models.9 Two of the three studies included in this review were informed by theory: social cognitive theory20 and diffusion-of-innovation theory.22 St Clair Russell et al used the social cognitive theory as the premise for designing a peer-to-peer mentoring program to improve adherence and self-management practices among hemodialysis patients.20 This theory has proven successful in improving adherence in other chronic conditions, such as HIV, by empowering HIV-positive patients and promoting the need for establishing supportive relationships to encourage adherence.24 St Clair Russell et al operationalized the social cognitive theory by successfully identifying and improving key mediators, including self-efficacy, perceived social support, and hemodialysis social support, using the peer-to-peer mentoring program.20 By pairing a poorly adherent hemodialysis patient with an already-adherent hemodialysis patient, the intervention was designed to achieve an improvement in hemodialysis adherence. Unique aspects of the social cognitive theory, including vicarious reinforcement or reinforcement by rewarding adherence and observational learning or modeling24,25 led to the observed improvement in self-efficacy and self-management behaviors.
Saunders et al22 applied the diffusion-of-innovation theory to enhance existing medication-reconciliation processes and improve patient outcomes.26 The diffusion-of-innovation theory has been historically used in intervention development, and evidence for its use is backed by robust conceptual and empirical data.27 It was successfully operationalized in this study:27 the simple but powerful act of thorough mediation reconciliation led by the nurse practitioner at each hemodialysis session was “the innovation” that led to a cascading positive effect on several adherence outcomes, including hemodialysis treatment adherence among the “adopters”, ie, the hemodialysis patients who quickly accepted and adopted the “diffusion” of self-management practices into the “social system”, ie, the outpatient hemodialysis unit, leading to improved communication between patients and members of the health-care team and improved patient outcomes.27,28
Changing health behavior is very complex, and even though the effectiveness and salience of behavior-change interventions can be enhanced by adapting interventions for minorities,29,30 none of the three studies in this review was designed specifically to consider factors that may increase the salience and impact of the intervention for Blacks; however, even with the appropriate and effective use of health-behavior theory, considerable literature suggests that augmenting the theory guiding the behavioral intervention with program-planning approaches that explicitly consider cultural or ethnic factors (eg, PEN-3),31,32 approaches that are specifically designed to enhance the cultural sensitivity of the intervention,33,34 or cultural tailoring may enhance the salience and impact of the intervention. Cultural tailoring of interventions, a recognized priority for health promotion among racial/ethnic minorities,33,35 ensures that behavioral interventions reach subcultural groups, in order to reduce health disparities effectively.29,35–37 Cultural tailoring can be integrated into the therapeutic relationship between patients and providers. This critical relationship consistently predicts the outcome of the intervention38 and reflects the strong bond between patients and providers.39
None of the existing studies focused on Blacks with ESKD, nor did any report adherence outcomes separately by race. Lack of representation of Blacks in clinical and biomedical research is a fundamental problem,40 especially given the unique historical and ongoing experiences that lead to fundamental sociocultural differences and medical mistrust that influence health outcomes.41–43 Although few studies6,–44-46 have focused on specific barriers to adherence present in Black ESKD populations, none has proposed mechanisms for addressing these unique barriers to improve hemodialysis adherence and its health outcomes. Since the majority of the patients included in all three studies were Black, at best we can only extrapolate the results of these studies to estimate how Black hemodialysis patients would respond to the tested interventions. The absence of any studies focusing on interventions targeting hemodialysis-adherence improvement among Blacks exposes an unmet need in hemodialysis care.
In order to make a significant impact on improving hemodialysis treatment adherence, studies need to be rigorously designed with a well-defined target population, appropriate intervention, well-informed and precise intervention dose and duration, and adherence-specific intervention. Strategic efforts to recruit nonadherent subjects are necessary to increase the likelihood of achieving a measurable effect among a sample eligible to benefit from the intervention, and this was done in one of the studies.19,47 Two of the three studies in this systematic review included younger patients in their mid-50s19,20 while patients in the third study were mostly in their mid-60s to mid-70s.22 Though no obvious efforts were made to recruit a certain age-group, the two studies that included younger patients were notably those that utilized technology19 and peer-to-peer mentoring,20 suggesting that younger patients were perhaps more interested in enrolling in these types of studies. Careful consideration of participants’ age ranges will inform the choice of likely effective interventions and increase study enrollment and generalizability of study findings. This is especially relevant, since younger age has been identified as a unique predictor of dialysis-treatment nonadherence.6
The intervention dose varied by frequency of delivery across the three studies. It is unclear if the frequency of intervention delivery was informed by prior formative research (preferred) or such considerations as patient burden and budgetary and timeline considerations.48 Duration of delivery of adherence interventions in all three studies was brief and follow-up relatively short, ranging 2–4 months. Long duration of delivery and follow-up, preferably up to 2 years, with multiple time points of outcome assessment and use of reinforcement strategies aid optimal assessment of adherence-behavior change in the setting of ESKD.18,49 Interventions in the studies in this review were at risk of being too diffuse, because of multiple adherence targets, ie diet, medication, and hemodialysis treatment. While interventions can be designed to target change in multiple behaviors relevant to a specific outcome of interest,50,51 the ideal intervention should be hemodialysis treatment adherence–specific, rather than being bundled into a complex multilevel intervention targeting heterogeneous outcomes, because this limits the ability to draw meaningful conclusions regarding the efficacy of any intervention.
Strengths
This review revealed a significant gap in knowledge about improving hemodialysis nonadherence in Blacks with ESKD, despite the association between hemodialysis treatment nonadherence and increased morbidity and mortality in this vulnerable population. Studies in this review reported at least one of the same measures of adherence (eg, attendance at hemodialysis), thereby allowing for standardized assessment and comparison of results. They demonstrated an improvement in adherence, with one of the studies even demonstrating improvement in a nonadherent population.
Limitations
The major limitation in this systematic review is that most studies describing interventions to improve hemodialysis treatment adherence did not report the percentage of Blacks in the sample or outcome data by race. Other limitations include the small samples of all interventions, limiting power and increasing the risk of type II error,26 brief study follow-up periods, limiting the ability to demonstrate sustained effects, lack of study populations comprised of 100% Blacks with ESRD, limiting the ability to make definitive conclusions about the most helpful types of interventions for this population, and heterogeneity of included outcomes, increasing chances of observed improvement in hemodialysis treatment adherence simply due to chance.49
Conclusion
A few, but important, studies suggest that such interventions as text-message reminders, medication reconciliation, and peer mentoring may be effective in improving hemodialysis treatment adherence among Blacks, noting possible variations in the suitability and effectiveness of these interventions for younger versus older patients. Given the disproportionate burden of ESKD and worse hemodialysis treatment–adherence metrics in Blacks compared to Whites, there is a pressing need for studies with a specific focus on improving hemodialysis treatment adherence among Black patients and reporting outcomes by race. These studies should be guided by theoretical models of behavior informing intervention development, incorporate therapeutic alliance strategies, and employ cultural tailoring. Eliminating the persistent devastating problem of nonadherence to hemodialysis treatments requires investment in building an evidence base to justify innovation and evolution in the delivery of hemodialysis.
Acknowledgments
This work was presented as a poster at the 2019 Vanderbilt University Medical Center SRTP program supported by T35DK007383. It was supported in part by NIH NIDDK 1K23DK114566-01A1 (Umeukeje), NIA-3K02AG059140-02S1 (Bruce), and NIH R01DK03935-01A1 (Cavanaugh). KN is supported in part by NIH research grants ULITR001881 and P30AG021684. The project described was supported by the National Center for Research Resources (grant UL1 RR025975-01) and is now at the National Center for Advancing Translational Sciences (grant 2 UL1 TR000445-06). The content is solely the responsibility of the authors, and does not necessarily represent the official views of the NIH.
Disclosure
Kerri L Cavanaugh reports grants from the NIH outside the submitted work. The authors report no other possible conflicts of interest in this work.
References
1. National Institutes of Health NIoDaDaKD. 2018 USRDS Annual Data Report: Epidemiology of Kidney Disease in the United States. Bethesda, MD; 2018.
2. Mathew AT, Strippoli GF, Ruospo M, Fishbane S. Reducing hospital readmissions in patients with end-stage kidney disease. Kidney Int. 2015;88(6):1250–1260. doi:10.1038/ki.2015.307
3. Chan KE, Lazarus JM, Wingard RL, Hakim RM. Association between repeat hospitalization and early intervention in dialysis patients following hospital discharge. Kidney Intl. 2009;76(3):331–341. doi:10.1038/ki.2009.199
4. Himmelfarb J. The HEMO study - where do we go from here? Curr Opin Nephrol Hypertens. 2003;12(6):587–591. doi:10.1097/00041552-200311000-00003
5. Denhaerynck K, Manhaeve D, Dobbels F, Garzoni D, Nolte C, De Geest S. Prevalence and consequences of nonadherence to hemodialysis regimens. Am J Crit Care. 2007;16(3):
6. Al Salmi I, Larkina M, Wang M, et al. Missed hemodialysis treatments: international variation, predictors, and outcomes in the dialysis outcomes and practice patterns study (DOPPS). Am J Kidney Dis. 2018;72(5):634–643.
7. Curtin RB, Svarstad BL, Keller TH. Hemodialysis patients’ noncompliance with oral medications. Nephrol Nurs. 1999;26(3):
8. Heath G, Cooke R, Cameron E, Theory-Based A. Approach for developing interventions to change patient behaviours: a medication adherence example from paediatric secondary care. Healthcare (Basel, Switzerland). 2015;3(4):1228–1242.
9. Sirur R, Richardson J, Wishart L, Hanna S. The role of theory in increasing adherence to prescribed practice. Physiother Can. 2009;61(2):68–77.
10. Campbell NC, Murray E, Darbyshire J, et al. Designing and evaluating complex interventions to improve health care. BMJ (Clinical Research Ed). 2007;334(7591):455–459. doi:10.1136/bmj.39108.379965.BE
11. Rosenstock IM. Historical origins of the health belief model. Health Educ Monogr. 1974;2(4):328–335. doi:10.1177/109019817400200403
12. Phillips RL. Nonadherence in individuals on hemodialysis: a discussion of three theories to improve adherence. J Nephrol Soc Work. 2015;38(1).
13. Fuertes JN, Rubinstein S, Reyes M, et al. The physician-patient working alliance in hemodialysis treatment. Behav Med (Washington, DC). 2017;43(4):242–250. doi:10.1080/08964289.2015.1122569
14. Laster M, Shen JI, Norris KC. Kidney disease among African Americans: a population perspective. Am J Kidney Dis. 2018;72(5):S3–S7. doi:10.1053/j.ajkd.2018.06.021
15. Van Bulck L, Claes K, Dierickx K, et al. Patient and treatment characteristics associated with patient activation in patients undergoing hemodialysis: a cross-sectional study. BMC Nephrol. 2018;19(1):126. doi:10.1186/s12882-018-0917-2
16. Hibbard JH, Greene J, Becker ER, et al. Racial/ethnic disparities and consumer activation in health. Health Aff. 2008;27(5):1442–1453. doi:10.1377/hlthaff.27.5.1442
17. Eneanya ND, Winter M, Cabral H, et al. Health literacy and education as mediators of racial disparities in patient activation within an elderly patient cohort. J Health Care Poor Underserved. 2016;27(3):1427–1440. doi:10.1353/hpu.2016.0133
18. Matteson ML, Russell C. Interventions to improve hemodialysis adherence: a systematic review of randomized-controlled trials. Hemodial Int. 2010;14(4):370–382. doi:10.1111/j.1542-4758.2010.00462.x
19. Som A, Groenendyk J, An T, et al. Improving dialysis adherence for high risk patients using automated messaging: proof of concept. Sci Rep. 2017;7(1):4177. doi:10.1038/s41598-017-03184-z
20. St Clair Russell J, Southerland S, Huff ED, Thomson M, Meyer KB, Lynch JR. A peer-to-peer mentoring program for in-center hemodialysis: a patient-centered quality improvement program. Nephrol Nurs J. 2017;44(6):481–496.
21. Brown EA, Bekker HL, Davison SN, Koffman J, Schell JO. Supportive care: communication strategies to improve cultural competence in shared decision making. Clin J Am Soc Nephrol. 2016;11(10):1902–1908. doi:10.2215/CJN.13661215
22. Saunders J, Ahmadzadeh S, Bush M, Wright R, Granger B. Improving patient experience and treatment adherence in the adult, outpatient hemodialysis population. J Nurs Care Qual. 2019;34(4):330–336.
23. Ghimire S, Lee K, Jose MD, Castelino RL, Zaidi STR. Adherence assessment practices in haemodialysis settings: a qualitative exploration of nurses and pharmacists’ perspectives. J Clin Nurs. 2019;28(11–12):2197–2205.
24. Adefolalu AO. Cognitive-behavioural theories and adherence: application and relevance in antiretroviral therapy. South Afr J HIV Med. 2018;19(1):762. doi:10.4102/sajhivmed.v19i1.762
25. Cavanaugh KL, Osborn CY, Tentori F, Rothman RL, Ikizler TA, Wallston KA. Performance of a brief survey to assess health literacy in patients receiving hemodialysis. Clin Kidney J. 2015;8(4):462–468. doi:10.1093/ckj/sfv037
26. Greenhalgh T, Stramer K, Bratan T, Byrne E, Mohammad Y, Russell J. Introduction of shared electronic records: multi-site case study using diffusion of innovation theory. Br Med J. 2008;337:a1786.
27. Dearing JW. Applying diffusion of innovation theory to intervention development. Res Soc Work Pract. 2009;19(5):503–518. doi:10.1177/1049731509335569
28. Lien AS-Y, Jiang Y-D. Integration of diffusion of innovation theory into diabetes care. J Diabetes Investig. 2017;8(3):259–260. doi:10.1111/jdi.12568
29. Barrera M, Castro FG, Strycker LA, Toobert DJ. Cultural adaptations of behavioral health interventions: a progress report. J Consult Clin Psychol. 2013;81(2):196–205. doi:10.1037/a0027085
30. Resnicow K, Jackson A, Braithwaite R, et al. Healthy body/healthy spirit: a church-based nutrition and physical activity intervention. Health Educ Res. 2002;17(5):562–573. doi:10.1093/her/17.5.562
31. Airhihenbuwa CO. Health and Culture: Beyond the Western Paradigm. Thousand Oaks (CA): Sage Publictions; 1995.
32. Iwelunmor J, Newsome V, Airhihenbuwa CO. Framing the impact of culture on health: a systematic review of the PEN-3 cultural model and its application in public health research and interventions. Ethn Health. 2014;19(1):20–46. doi:10.1080/13557858.2013.857768
33. Resnicow K, Baranowski T, Ahluwalia JS, Braithwaite RL. Cultural sensitivity in public health: defined and demystified. Ethn Dis. 1999;9(1):10–21.
34. Resnicow K, Soler R, Braithwaite RL, Ahluwalia JS, Butler J. Cultural sensitivity in substance use prevention. J Community Psychol. 2000;28(3):271–290. doi:10.1002/(SICI)1520-6629(200005)28:3<271::AID-JCOP4>3.0.CO;2-I
35. Kreuter MW, Lukwago SN, Bucholtz RD, Clark EM, Sanders-Thompson V. Achieving cultural appropriateness in health promotion programs: targeted and tailored approaches. Health Educ Behav. 2003;30(2):133–146. doi:10.1177/1090198102251021
36. Harvey RD, Afful SE. Racial typicality, racial identity, and health behaviors: a case for culturally sensitive health interventions. J Black Psychol. 2010;37(2):164–184. doi:10.1177/0095798410376244
37. Henderson S, Kendell E, See L. The effectiveness of culturally appropriate interventions to manage or prevent chronic disease in culturally and linguistically diverse communities: a systematic review. Health Soc Care Community. 2011;19:225–249.
38. Martin DJ, Garske JP, Davis MK. Relation of the therapeutic alliance with outcome and other variables: a meta-analytic review. J Consult Psychol. 2000;68(3):438–450. doi:10.1037/0022-006X.68.3.438
39. Catty J, Winfield H, Clement S. The therapeutic relationship in secondary mental health care: a conceptual review of measures. Acta Psychiatr Scand. 2007;116(4):238–252. doi:10.1111/j.1600-0447.2007.01070.x
40. Oh SS, Galanter J, Thakur N, et al. Diversity in clinical and biomedical research: a promise yet to be fulfilled. PLoS Med. 2015;12(12). doi:10.1371/journal.pmed.1001918.
41. Smedley BD, Stith AY, Nelson AR, eds. Unequal Treatment: Confronting Racial and Ethnic Disparities in Health Care. Washington DC: 2002 by the National Academy of Sciences; 2003.
42. Sullivan LS. Trust, risk, and race in American medicine. Hastings Cent Rep. 2020;50(1):18–26.
43. Powell W, Richmond J, Mohottige D, Yen I, Joslyn A, Corbie-Smith G. Medical mistrust, racism, and delays in preventive health screening among African-American men. Behav Med (Washington, DC). 2019;45(2):102–117.
44. Chan KE, Thadhani RI, Maddux FW. Adherence barriers to chronic dialysis in the United States. J Am Soc Nephrol. 2014;25:2642–2648.
45. Joshi S, Gaynor JJ, Bayers S, et al. Disparities among Blacks, Hispanics, and Whites in time from starting dialysis to kidney transplant waitlisting. Transplantation. 2013;95(2):309–318.
46. Chenitz KB, Fernando M, Shea JA. In-center hemodialysis attendance: patient perceptions of risks, barriers, and recommendations. Hemodial Int. 2014;18(2):364–373.
47. Bosworth HB. Patient Treatment Adherence: Concepts, Interventions, and Measurement: Lawrence Erlbaum Associates. Psychology Press; 2006.
48. Voils CI, King HA, Maciejewski ML, Allen KD, Yancy WS, Shaffer JA. Approaches for informing optimal dose of behavioral interventions. Ann Behav Med. 2014;48(3):392–401.
49. Murali KM, Mullan J, Roodenrys S, Hassan HC, Lambert K, Lonergan M. Strategies to improve dietary, fluid, dialysis or medication adherence in patients with end stage kidney disease on dialysis: a systematic review and meta-analysis of randomized intervention trials. PLoS One. 2019;14(1):e0211479.
50. Allegrante JP, Peterson JC, Boutin-Foster C, Ogedegbe G, Charlson ME. Multiple health-risk behavior in a chronic disease population: what behaviors do people choose to change? Prev Med. 2008;46(3):247–251.
51. Blissmer B, Prochaska JO, Velicer WF, et al. Common Factors Predicting Long-Term Changes in Multiple Health Behaviors. 1. National Institutes of Health NIoDaDaKD: 2018 USRDS Annual Data Report: Epidemiology of Kidney Disease in the United States. MD: United States Renal Data System Bethesda; 2018.
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.