")
Back to Journals » International Journal of General Medicine » Volume 13
Interventions for Post-Stroke Shoulder Pain: An Overview of Systematic Reviews
Authors Dyer S , Mordaunt DA , Adey-Wakeling Z
Received 9 October 2020
Accepted for publication 27 October 2020
Published 7 December 2020 Volume 2020:13 Pages 1411—1426
DOI https://doi.org/10.2147/IJGM.S200929
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Suzanne Dyer,1,* Dylan A Mordaunt,1,2,* Zoe Adey-Wakeling1,2
1Rehabilitation, Aged and Extended Care, Flinders Health and Medical Research Institute, Flinders University, Adelaide, South Australia, Australia; 2Department of Rehabilitation Medicine, Southern Adelaide Local Health Network, Bedford Park, South Australia, Australia
*These authors contributed equally to this work
Correspondence: Zoe Adey-Wakeling Department of Rehabilitation, Southern Adelaide Local Health Network, Bedford Park 5041, South Australia, Australia
Tel +61 8 8204 5511
Email [email protected]
Background: Shoulder pain following stroke leads to poorer quality of life and daily functioning. Whilst many treatment approaches exist, there is currently no systematic overview of the evidence base for these. This review addressed the question “What is the evidence for interventions for treating hemiplegic shoulder pain?”
Methods: An overview of systematic reviews was performed according to PROSPERO protocol (CRD42020140521). Five electronic databases including Cochrane, MEDLINE, Embase and EmCare were searched to June 2019. Included systematic reviews were those of comparative trials of interventions for hemiplegic shoulder pain in adults, reporting pain outcomes using a validated pain scale. Review quality was assessed with AMSTAR2 and those considered at high risk of bias for four or more items were excluded. The most recent, comprehensive review for each intervention category was included. Outcomes of function and quality of life were also extracted.
Results: Seven systematic reviews of 11 interventions were included, with varied quality. Reviews showed significant benefits in terms of pain reduction for many interventions including acupuncture (conventional 19 trials, electroacupuncture 5 trials, fire needle 2 trials, warm needle 1 trial and bee venom 3 trials), orthoses (1 trial), botulinum toxin injection (4 trials), electrical stimulation (6 trials) and aromatherapy (1 trial). However, the majority of trials were small, leading to imprecise estimates of effect. Findings were often inconsistent across outcome measures or follow-up times. Outcomes from trials of acupuncture were heterogenous with likely publication bias.
Conclusion: A number of systematic reviews indicate significant reductions in pain, with a wide range of treatments appearing promising. However, significant limitations mean the clinical importance of these findings are uncertain. Due to complex etiology, practitioners and health systems must consider the range of potential interventions and tailor their approach to individual presentation, guided by their local circumstances, expert opinion and the growing literature base.
Keywords: shoulder pain, stroke, hemiplegia, systematic review, older adults
Introduction
Shoulder pain is a common debilitating problem after stroke, with a recent meta-analysis indicating an incidence of 10%–22%.1 There appear to be three major etiological groups that may present with hemiplegic shoulder pain (HSP),2 namely central (central post-stroke pain, CPSP), regional (chronic regional pain syndrome, CRPS, or reflex sympathetic dystrophy, RSD), and local mechanical pain.3 The causes of the HSP are numerous, and often overlapping.3 The pathomechanism is thought to be that during the acute and sub-acute phase of stroke, flaccid paresis occurs resulting in potential subluxation of the shoulder, and/or imbalance of shoulder joint control and soft-tissue structure, resulting in altered mechanics of movement and increased susceptibility to injury.4 However, there is a lack of empiric evidence correlating different etiologies with different phases of the natural history. Specific musculoskeletal etiologies are associated with HSP, including rotator cuff tendinitis, adhesive capsulitis, and bicapital tendinitis.4 Glenohumeral subluxation itself has been postulated to be a cause of HSP, although little empiric evidence exists to support this and its presence as a cause is inconsistent.5
A number of predisposing factors are linked with HSP, including incorrect handling, joint subluxation, flaccidity, spasticity, reduced range of motion and poor motor function.4,6 HSP has been demonstrated to be a predictor of poor patient outcomes, including motor outcome, function, depression and quality of life.7–10 The frequency and impact of this complication means that comprehensive assessment and effective treatment modalities are imperative to good patient care. Etiological complexity means that extension of the musculoskeletal evidence base is not always appropriate, and a stroke-specific approach needs to be adopted. Whilst there is a growing number of randomized control trials (RCTs) investigating specific treatment options, guidelines often refer to consensus statements and good practice points due to paucity of high-grade evidence.11,12 The Evidence-Based Review of Stroke Rehabilitation (EBRSR) is an up-to-date review of both pharmacological and non-pharmacological treatments of stroke, that has stronger emphasis on RCT-level evidence for interventions, synthesized in a narrative fashion.13,14 This resource points to a number of interventions with RCT-level evidence supporting efficacy. Australian guidelines for the management of HSP is limited to discussion around strapping, subacromial steroid injection suprascapular nerve block, botulinum toxin injection and electrical stimulation, based on a mix of systematic reviews and trials.12 Canadian Stroke Best Practices recommend treatments specific to defined pain etiologies, including gentle stretching for reduced range, botulinum toxin for spasticity, and subacromial corticosteroid injection for local inflammation.15 Generalized options include analgesia and taping.15
Many existing systematic reviews, including reviews by the Cochrane Collaboration, exist which summarize the evidence individually for the wide range of interventions available to manage HSP. However, a succinct systematic summary of the findings of these reviews across the different types of treatments has not been conducted. An overview of systematic reviews is a rigorous approach considered suitable for summarizing the evidence across the range of interventions.16 This overview aims to provide a systematic summary of the effectiveness of the different interventions available to treat HSP in adults following stroke, in order to compare their relative evidence base. The review question was, “What is the evidence for interventions for treating hemiplegic shoulder pain?” Evidence for treatments conducted in a population of adults (18 or over years) who had hemiplegic shoulder pain post-stroke (ie not following traumatic or developmental brain injuries), was systematically summarized.
Methods
An a-priori protocol was developed and registered on the PROSPERO International Prospective Register of Systematic Reviews (registration number CRD42020140521).17 Changes to protocol following publication were that the outcome of motor impairment was removed due to resource constraints and because this was considered a surrogate for other included outcomes. In the early stages of the review, pain was reprioritized as the primary outcome from a secondary outcome. This manuscript was structured based on the PRISMA statement.18
Inclusion/Exclusion Criteria
Types of Studies
This overview included randomized (RCT) and non-randomized control trials (NRCT). NRCT were defined as trials in which interventions are compared with a control group, using allocation methods that are not truly random or where no attempt at randomization was made. NRCTs were included to widen the range of potentially eligible reviews in order to maximize the generalizability and utility of the findings. Eligibility of systematic reviews for inclusion were not restricted by source. Where multiple reviews existed for an intervention, we included the most recent review addressing the inclusion criteria, except if poor quality (defined as rated as low risk for less than four items on the AMSTAR2 critical appraisal tool for systematic reviews19). Our methods were consistent with those described in the Cochrane Handbook for Systematic Reviews of Interventions and previous overviews.16,20,21
Population
Systematic reviews were included that examined adults (18 years or over) with shoulder pain following stroke, including central, regional and local causes of shoulder pain. Reviews with a wider population, but a clear subgroup analysis of a stroke population, were included. We excluded reviews that assessed children and adolescents (under 18 years) or did not report pain as an outcome.
Intervention and Comparison
Systematic reviews that examined RCTs or NRCTs of either pharmacological or non-pharmacological interventions for the treatment of HSP, in comparison to placebo/sham therapy or usual care, were included.
Outcomes
Systematic reviews reporting outcomes as measured on an internationally recognized and validated pain scale, such as the visual analogue scale (VAS), were included. Reviews were excluded if they did not examine pain as an outcome. Outcomes within included reviews also extracted for this overview were measures of upper limb function, generalized function and quality of life as reported on a recognized and validated scale. We did not place any restriction on duration of follow-up.
Search Strategy and Selection of Included Studies
We searched MEDLINE, CINAHL, Cochrane, PsycINFO, EmCare and PROSPERO, Database of Abstracts of Reviews of Effect (DARE) and the NHS Economic Evaluation Database (NHS EED) databases from inception to June 26, 2019. The full electronic search strategy is included in the supplementary materials (Table S1) and was designed by a specialist librarian. We identified and selected existing systematic reviews for inclusion based on our pre-specified criteria and accepted these systematic reviews as complete. We did not repeat the searches, determine eligibility or reassess risk of bias for individual studies, or search for additional trials.
Citations and abstracts were downloaded from the respective database and aggregated within Endnote.22 This library was then imported into Covidence23 for title and abstract and full-text screening. Two authors independently assessed citations for eligibility against inclusion and exclusion criteria and discrepancies were resolved by discussion and in consultation with a third author as necessary. Full-text articles for any systematic reviews that were identified as potentially meeting the eligibility criteria were retrieved and assessed against the eligibility criteria independently by the same two authors. Potentially eligible reviews were classified based on intervention approach. The most recent reviews with the closest and broadest applicability to the study question were selected for inclusion. However, reviews rated as low risk of bias for less than four items of the AMSTAR2 quality appraisal tool were excluded.19
Data Collection and Analysis
Data Extraction
Pre-defined data on review characteristics and meta-analysis outcomes were extracted into Covidence, with additional data extraction conducted using Microsoft Excel (see PROSPERO record for details).23,24 Data extraction was performed in duplicate with resolution of discrepancies by discussion or involvement of a third reviewer as necessary. If the systematic review included data from RCTs and also other study designs, data were only extracted for the RCTs and NRCTs. Where a systematic review considered more than one intervention, only the data relevant to the inclusion criteria for this overview were extracted. Where systematic reviews addressed a wider population than the criteria for this review, only outcomes related to stroke patients with HSP were extracted. Where RCTs of studies with a number of comparators were included, data were extracted only for the placebo/sham/usual care controlled trials.
For this overview, the original review author's assessments of risk of bias of individual studies were accepted; summary information on risk of bias of individual studies was extracted.
For reviews including a meta-analysis, the mean difference (MD), standardized mean difference (SMD), 95% confidence intervals (CIs) and I2 measure of heterogeneity for pooled summary estimates was extracted, when reported. Where individual studies were not pooled, or an existing meta-analysis was considered inappropriate due to extremely high heterogeneity, we extracted study outcomes for individual trials. In selected cases, original trial reports were retrieved where required data could not be obtained from reviews or otherwise required clarification (ie Pandian et al25 from the Appel et al review26).
Quality Assessment
Two authors independently assessed the quality of the included reviews using the AMSTAR2, a 16-item systematic review critical appraisal tool, using Covidence.19,23 Discrepancies were resolved by discussion or involvement of a third reviewer as necessary. This is consistent with Cochrane guidelines for overviews that recommend quality assessment should be based on assessments reported in the included systematic reviews.16 We used the Grading of Recommendations Assessment, Development, and Evaluation (GRADE) framework to guide narrative synthesis.27
Data Synthesis
We have narratively summarized the effects of the interventions, tabulating outcome effects as pooled estimates with SMD where appropriate, or for individual studies where pooling was not performed or not considered appropriate. For meta-analyses reporting a mean difference, we calculated the SMD to enable approximate comparison of effect size across different interventions, although as this approach does not represent an indirect meta-analysis and direct head-to-head comparison of interventions, this must be interpreted with caution. Fixed effects meta-analysis was used where heterogeneity was low as indicated by I2 = 0, otherwise random effects was used. Novel additional meta-analyses were conducted where it was apparent that this was possible, either by using a generic inverse variance meta-analysis,28 or where extraction of additional information from the primary trial enabled pooling. Standard deviations (SDs) were calculated from 95% CIs or standard errors (SEs) if necessary. Meta-analysis across different outcome measures is only considered appropriate where data are either only trial endpoint or change from baseline data.16 Where meta-analyses pooled trial endpoint and change from baseline data for a single outcome measure the MD is therefore presented. SMDs for interventions were not summarized graphically as planned in the protocol due to the paucity of evidence and as some interventions are presented as MD where the trial data are a mix of endpoint and change data. Where pooling was considered inappropriate or not possible, data were summarized for individual trials graphically or in Table 2. All analyses were completed in Review Manager 5.4.23
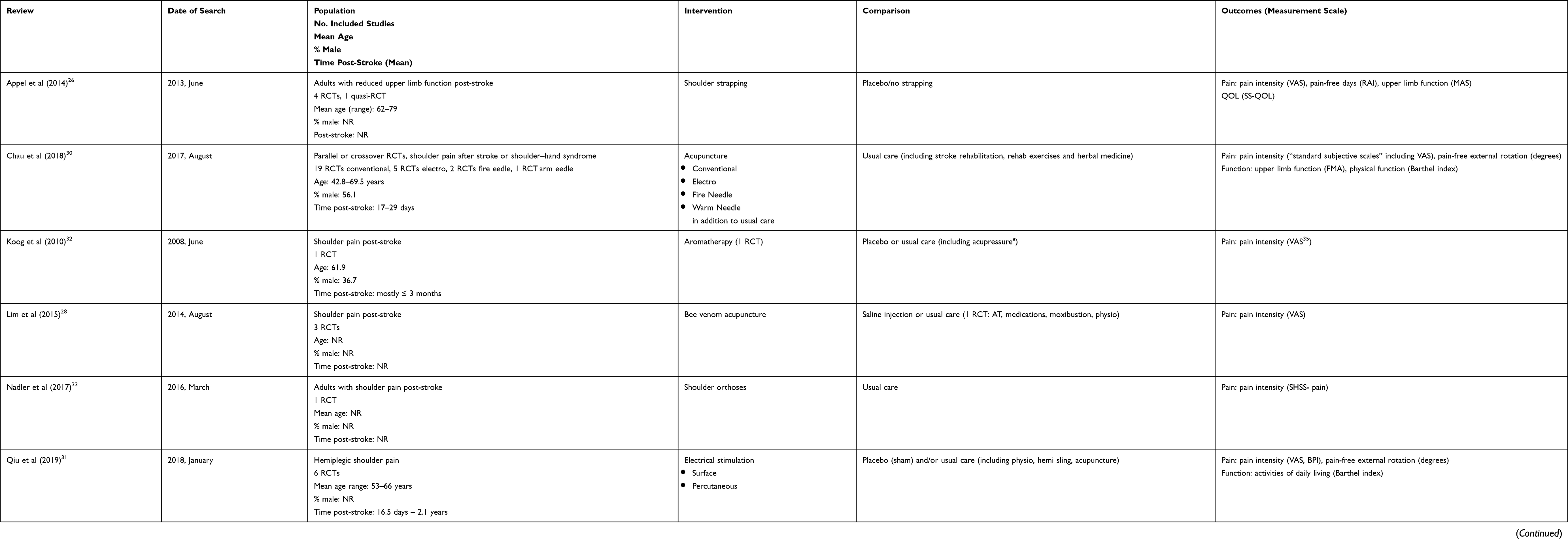 |
Table 1 Characteristics of Included Systematic Reviews, for Eligible Interventions |
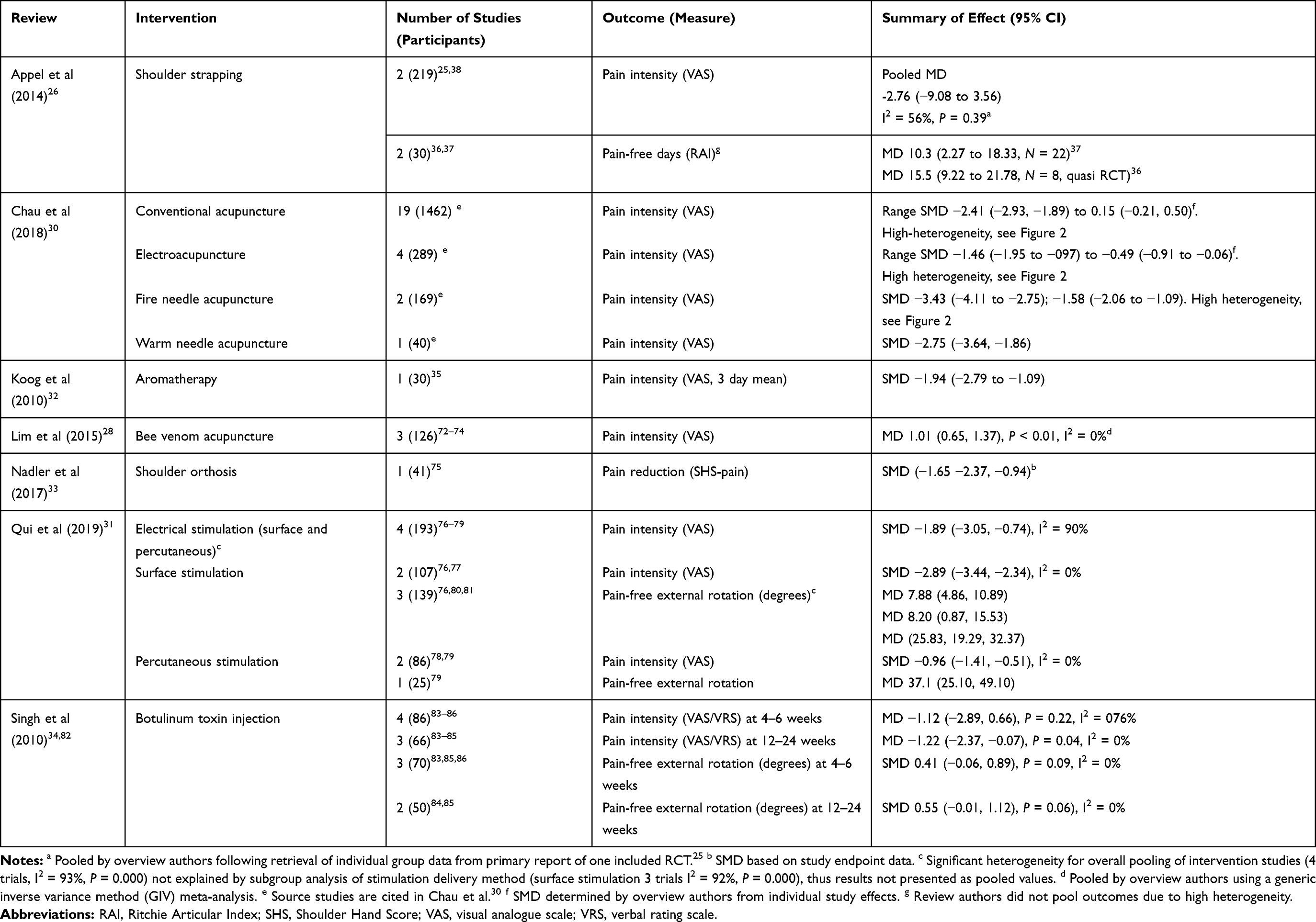 |
Table 2 Effectiveness of HSP Interventions on Outcome of Pain |
Results
Review and Primary Study Selection
The database searches retrieved 273 citations. After exclusion of duplicates, 131 citations from the searches were screened against the inclusion criteria (Figure 1). Seven systematic reviews were included (Table 1), examining 11 interventions. Summaries of the intervention effects on pain are presented in Table 2. A list of key excluded reviews with reasons is provided in the supplementary materials. No review was included for biofeedback therapy as the single identified review had a systematic search to 2002, which was considered likely to be outdated.29 Three of the reviews examined more than one intervention; only data for the interventions that were included in this overview (based on recency and quality on a per intervention basis) were extracted.30–32
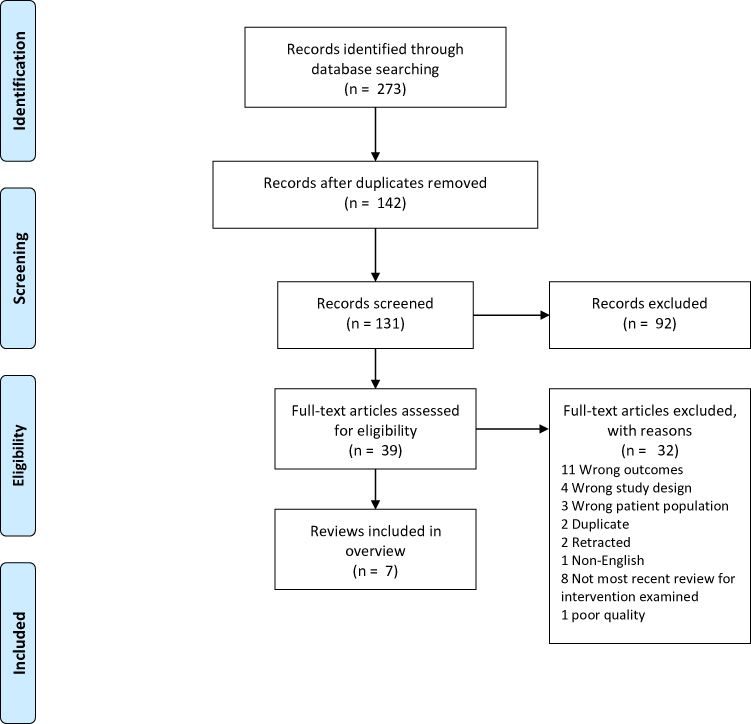 |
Figure 1 Study selection flowchart.18Note: Adapted from Moher D, Liberati A, Tetzlaff J, Altman DG. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. PLoS Med. 2009;6(7):e1000097. © 2009 Moher et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License.18 |
Characteristics of the Included Reviews
Table 1 summarizes the characteristics of the included reviews. Ten of the included interventions examined non-pharmacological interventions26,28,30–33 and one examined a pharmacological intervention.34
Five reviews provided a comparison to usual care which varied between trials and included pharmacological analgesia, physiotherapy, acupuncture and occupational therapy. Some additional trials included co-interventions in both groups (ie, acupressure with aromatherapy32,35 and moxibustion with bee-venom acupuncture), thus treating these co-interventions as a component of usual care, although the applicability of this is likely to vary by setting.
Methodological Quality
AMSTAR2 assessments for all included reviews are shown in the supplementary materials. All included reviews had some methodological limitations. One review was high risk of bias for the description of the study question,28 four studies did not provide an explicit statement of an a-priori protocol,26,28,30,32 three did not clearly describe their study designs for inclusion28,30,33 and three did not adequately describe their search strategy,26,30,32 with each of these potentially being critical weaknesses of the systematic review design.
Effects of Interventions for HSP
A summary of the effects of the interventions on the outcome of pain is provided in Table 2. The effectiveness of the interventions on function and quality of life outcomes are summarized in the supplementary materials.
Strapping
Appel and colleagues reported a systematic review of shoulder strapping, which included five studies25,36–39 eligible for inclusion in this overview.26 These were two trials25,38 for a total of 219 patients on pain intensity, two studies36,37 reporting 30 patients on pain-free days, one study reporting 12 patients on quality of life39 and three studies reporting 117 patients on upper limb function (activity limitation).37–39 Strapping was defined as any strapping applied to the shoulder with therapeutic intent. A number of different strapping materials were identified at two main anatomical sites (the glenohumeral and scapular joints). Data were pooled from two trials reporting pain intensity; however, no statistically significant difference was found (Table 2, MD −2.76, 95% CI −9.08 to 3.56, I2 = 56%, P = 0.39, N = 219). Two small trials (one with inadequate randomization) reporting data on pain-free days reported significant improvements in pain but had significant risk of bias (Table 2, N = 30). No significant difference was found between treatment and control arms for pooled data from three trials on upper limb function (activity limitation; SMD 0.26, 95% CI −0.11 to 0.62, N = 117, supplementary Table S3) or a single feasibility study examining quality of life (MD 0.54, 95% CI −1.29 to 2.37, N = 8; supplementary Table S2).
This review was assessed as having a few methodological items at high risk of bias and the four RCTs and one quasi-RCT included showed variable risk of bias. There was also inconsistency in the measurement of pain using different measures of pain-free days and pain intensity, study endpoint and change from baseline data resulting in inconsistency in assessment plus imprecision in the effect estimates due to the low numbers of participants enrolled in the trials.
Acupuncture
Chau et al (2018) reported a systematic review of 29 RCTs of acupuncture, including manual/conventional/traditional/balanced acupuncture,40–58 electroacupuncture,59–62 fire needle acupuncture63,64 and warm needle acupuncture,65 capturing a large number of patients.30 Acupuncture was broadly defined as insertion of an acupuncture needle into acupoints. Included trials assessed the effectiveness of acupuncture in addition to usual therapy. These trials tended to be more recent, with the design of this systematic review including Chinese language studies listed in the Wanfang Index. Studies were assessed using the Joanna Briggs Institute (JBI) Critical Appraisal Checklist for RCTs.66 The risk of bias items addressing blinding were considered not applicable, but where sham is used as the control treatment blinding of participants at least should be feasible. There was wide variability in the risk of bias assessment of included studies. The review was considered of moderate quality, with some elements considered at high risk of bias (including concerns about the comprehensiveness of the search strategy and lack of reporting on funding sources of the included trials, see supplementary materials).
Conventional Acupuncture
Conventional acupuncture was defined as including traditional acupuncture (ie insertion of an acupuncture needle into acupoints) and balanced acupuncture (insertion of an acupuncture needle into the peripheral nerves) in the review by Chau and colleagues.30 Nineteen studies were identified reporting on pain intensity and upper limb function following conventional acupuncture, with each trial enrolling a total of 123 patients or less.40–46,48,49,51–58,67,68 Five trials of conventional acupuncture reported on physical function outcomes. The authors reported that meta-analysis was not appropriate due to high statistical heterogeneity and that the intervention regimens were highly heterogenous. Individual study findings are summarized graphically in Figure 2; the review authors reported findings using “vote counting”, which is not generally considered an appropriate method for summation.16 The intervention effects on pain ranged from SMD −2.41 (95% CI −2.93, −1.89) to 0.15 (−0.21, 0.50). There were a large number of relatively small studies reporting statistically significant reductions in pain; however, a funnel plot shows some asymmetry on visual inspection, indicating some likelihood of publication bias (see supplementary materials Figure S1).16
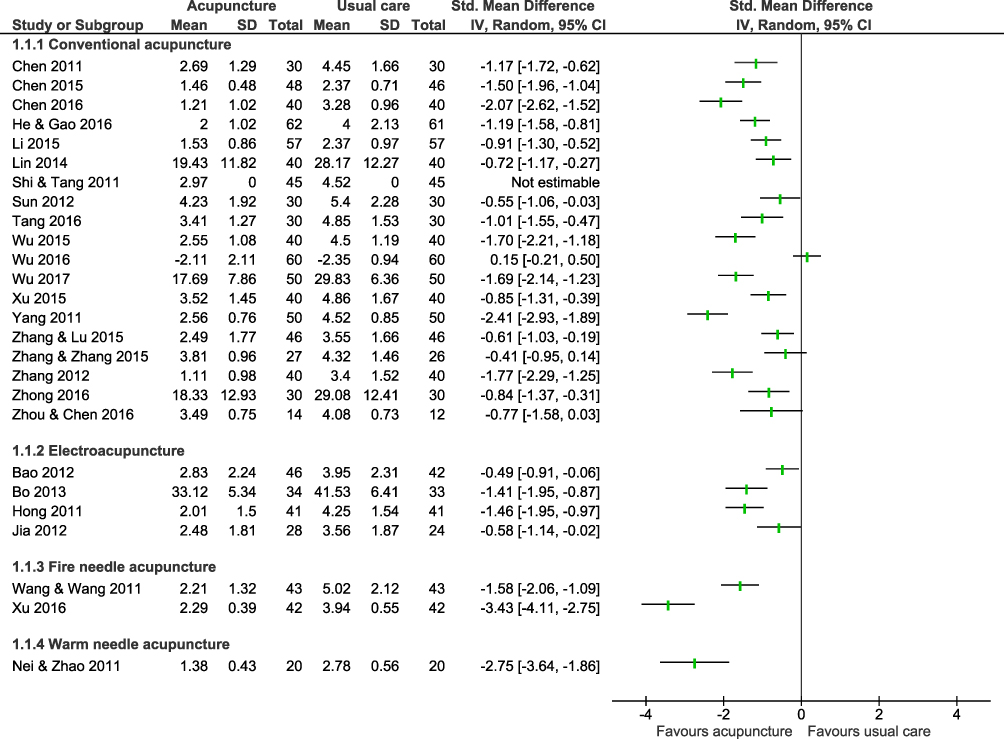 |
Figure 2 Forest plot of acupuncture trial effects on shoulder pain. Note: Data from Chau et al 2018.30 |
Similarly, there was a large number of relatively small studies reporting effects of conventional acupuncture on upper limb function, with many showing statistically significant effects (range of study effects SMD 0.32, 95% CI −0.10, 0.73 to SMD 1.52, 95% CI 1.07, 1.97; supplementary materials Figure S2). Five trials reported outcomes of physical function (supplementary Table S2 and Figure S3), with lower heterogeneity between study effects (I2 = 49%, P = 0.10) and a pooled SMD of 0.41 (95% CI 0.15 to 0.68).
The review authors’ assessment of the risk of bias of the included trials indicated some limitations in the trials; five of 19 did not clearly report true randomization and eight of 19 did not clearly have adequate follow-up. Blinding was not assessed. Overall, there was some evidence of a positive effect of conventional acupuncture; however, the possibility of publication bias, inconsistency between trials and risk of bias in some individual trials indicates there is uncertainty in this finding.
Electroacupuncture
There were five studies of electroacupuncture identified in the Chau review, defined as the application of electrical stimulation applied to the inserted needles.30,59–62,69,70 There was high heterogeneity reported in the outcomes of pain intensity (SMD range −1.46 95% CI −1.95, −097 to SMD −0.49 95% CI −0.91, −0.06, Figure 2), upper limb function (range SMD 0.36, 95% CI −0.19, 0.91 to SMD 2.68, 95% CI 1.90, 3.46; supplementary Figure S2) and physical function (range SMD 0.45 95% CI0.02, 0.87 to SMD 1.39, 95% CI 0.90, 1.87; supplementary Table S2 & Figure S3). Risk of bias assessment demonstrated variability in the quality of the included studies and there were relatively few participants in the trials.
Fire Needle Acupuncture
There were two RCTs of fire needle acupuncture (169 participants),63,64 defined as a treatment in which the acupuncture needles are heated before insertion into the acupoints.30 Both studies reported on pain intensity and upper limb function. There was high heterogeneity (95%) identified amongst the pain intensity outcomes, so studies are not pooled and are displayed in Figure 2. There was a significant improvement in upper limb function (SMD 1.19, 95% CI 0.76, 1.63, I2 = 43%, P < 0.001). Risk of bias was assessed as relatively low for the two included studies.
Warm Needle Acupuncture
There was one RCT (40 participants) of warm needle acupuncture, defined as a treatment that combines traditional moxibustion in which a small amount of moxa is placed on the acupuncture needle after insertion.30,65 Moxibustion is the application of heat to a part of the body through the burning of dried plant materials near the skin.71 This study reported a statistically significant reduction in pain with the intervention (MD −2.75, 95% CI −3.64, −1.86). Risk of bias was assessed as being moderate for the included study; however, the number of participants was very low.
Bee Venom Acupuncture
Lim et al28 reported a systematic review that identified three trials of bee venom acupuncture eligible for this overview.72–74 Two of these trials were placebo-controlled RCTs,72,74 whilst one compared bee venom acupuncture with usual care.73 Pooled outcomes for pain indicated a statistically significant reduction (MD 1.01, 95% CI 0.65–1.37, P = <0.01, 3 trials, I2 = 0%). However, the number of patients for which outcomes data was available was low (126 patients).
This systematic review had a number of items at high risk of bias (supplementary materials) and the risk of bias of individual trials indicated a number of quality items as unclear. There was moderate statistical heterogeneity, with very low numbers of patients in the included trials.
Aromatherapy
One RCT of aromatherapy35 including 30 patients was identified in a moderate-quality systematic review by Koog and colleagues.32 The trial was given a score of 7/10 using the Physiotherapy Evidence Database (PEDro) quality rating tool by the review authors. Although a significant reduction in pain was observed immediately after the intervention (SMD −1.94, 95% CI −2.79 to −1.09), the extremely small size of the trial (n = 30) creates great uncertainty in the findings.
Orthoses
For the systematic review on orthoses, one small trial of shoulder orthoses was included which reported on pain reduction using a validated scale (n = 41).75 Shoulder orthoses (Neurolux) were proximal support only around the humerus. Note that when compared to strapping/taping, orthoses do not require a skilled practitioner to apply, can be applied quickly, and worn for greater length of time without reapplication or risk of tape irritation. Pain was reported on the Shoulder Hand Sub-Score (SHSS) pain sub-scale rather than using a more conventional tool such as VAS. An effect was reported on pain intensity (SMD −1.65, 95% CI −2.37, −0.94) favoring intervention.75 Overall the quality of this systematic review showed a few high risk of bias areas. The review authors rated the RCT providing data on pain as 7 of 9 for quality on the PEDro risk of bias tool. This study provides some evidence of benefit, however with very low precision due to the small numbers of patients in the single trial conducted.
Electrical Stimulation
The included systematic review for electrical stimulation reported on surface stimulation, percutaneous stimulation and combined (pooled) groups.31 This systematic review included six studies.76–81 Electrical stimulation was not clearly defined; however, included studies assessed the application of a current transcutaneous or percutaneously. The authors reported pooled data on outcomes of pain intensity, pain-free external rotation and activities of daily living (Table 2 and supplementary materials). Pooling of data across surface and percutaneous electrical stimulation showed high statistical heterogeneity between trials for the pain intensity (I2 = 90%, P = 0.000) which appeared to be explained by differences in the effect size in subgroups according to intervention delivery method (ie, percutaneous and surface stimulation). Both surface stimulation and percutaneous stimulation reduced pain intensity, with surface stimulation producing a greater effect size (Table 2, surface stimulation SMD −2.89, 95% CI −3.44 to −2.34, 2 trials; percutaneous stimulation SMD −0.96, 95% CI −1.41, −0.51, 2 trials). Similarly, pooling across intervention types for pain-free external rotation demonstrated significant inconsistency between trial results which in this instance was not explained by subgroup analyses by stimulation delivery method. For pain-free external rotation, the single trial of percutaneous stimulation appeared to produce a greater effect, which was inconsistent with findings for pain intensity. Pooled analysis of three trials reporting function outcomes also demonstrated an improvement with electrical stimulation with moderate heterogeneity (MD 8.96, 95% CIs 5.26, 12.66, I2 = 45%; supplementary material Table S3). Differences in follow-up times or other variations in intervention methods are plausible explanations for the observed heterogeneity between trials; these were mentioned but not explored in subgroup analyses. The authors raised concerns of potential publication bias.
Overall, the quality of this systematic review was assessed as being relatively high (see supplementary materials). Risk of bias for individual trials within the review were assessed using PEDro and scores ranged from 5 to 7 of the maximum score of 10, indicating moderate quality. For the 193 participants pooled across the four RCTs, there was inconsistency for one outcome due to high statistical heterogeneity, inconsistency between the relative effects of the different delivery methods between different pain outcomes and imprecision due to low numbers of participants.
Botulinum Toxin Injection
The included review of botulinum toxin injection was broader than this overview. The population included arthritis; however, data extracted for this overview were from studies in patients with post-stroke spasticity.34,82 Four trials (86 patients) of intramuscular botulinum toxin injection were included. The authors pooled trial data on outcomes of pain intensity and pain-free external rotation at 4–6 weeks83–86 and 12–24 weeks (Table 2). 83–85 At 4–6 weeks there was no significant effect on pain intensity (4 trials, MD −1.12, 95% CI −2.89, 0.66, P = 0.22); however, there was high statistical heterogeneity (I2 = 76%, heterogeneity p = 0.006). A reduction in pain at 12–24 weeks and pain-free external rotation at both follow-up times was observed with borderline statistical significance and greater consistency between trials (12–24 week pain intensity MD −1.22, 95% CI −2.37, −0.07, 3 trials, P = 0.04, I2 0%; pain-free external rotation at 4–6 weeks 3 trials, SMD 0.41, 95% CI -0.06, 0.89, P = 0.09, I2 0% and at 12–18 weeks 2 trials SMD 0.55, 95% CI −0.01, 1.12, P = 0.06, I2 0%).83,85,86 However, there was low precision in the estimate of these effect sizes.
Overall, the quality of this Cochrane Collaboration systematic review was considered high, with no items considered as being at high risk of bias. However, there were very low numbers of patients in the trials and a very small effect size.
Discussion
This overview identified seven systematic reviews with 11 interventions to improve HSP. The quality of the systematic reviews varied considerably, with quality of included studies within each of the systematic reviews varying even more so. Some highly limited data showed significant benefits in terms of pain reduction for many interventions including orthoses, botulinum toxin injection, electrical stimulation, aromatherapy and acupuncture (conventional, electroacupuncture, fire needle, warm needle and bee venom). However, these findings were often not consistent across outcome measures, follow-up times, subgroup analyses or outcomes. The majority of trials within the area are small, leading to imprecise estimates of the effect size and making the body of evidence prone to small-study effects.16 Many of the studies included critical limitations, such as missing data, high statistical heterogeneity, poor study quality, very low numbers or a very low effect size. Concerns about publication bias also exist, based on visualization of a funnel plot for acupuncture (the only intervention with sufficient trials to enable this approach, see supplementary materials) and as raised by the review authors.31 Fewer studies reported on function and only one study in one review (of shoulder strapping) reported on quality of life. Thus, overall, the evidence base is considered inadequate to inform clear evidence-based recommendations for treatment approaches and the effectiveness of the treatments examined in the identified reviews is considered uncertain. Therefore, individual trials, clinical expert opinion and other factors such as resources must also play a role in guiding treatment decisions.
It is evident from this overview that there are a number of areas that are either inadequately covered by existing systematic reviews, or for which there are no systematic reviews. Systematic reviews were identified for some additional interventions, however they were either assessed as having critically poor quality (ultrasound-guided steroid injection),87 were too old to be meaningful (biofeedback),29 or did not compare the intervention with placebo or usual care (steroid).32 No systematic reviews were identified for shoulder positioning and range of motion exercises; however, these generally fall into the category of usual care. Slow-stroke massage trials either do not use a clear pain scale,88 or were not compared with placebo or usual therapy.35,89,90 No systematic reviews were identified for robotic-assisted physical therapy,91 cryotherapy,92 extracorporeal shockwave therapy,93 inferential current therapy,94,95 repetitive transcranial magnetic stimulation,96 hyaluronic acid injection,67 suprascapular nerve block,97 segmental neurotherapy98 or other pharmacological therapies such as gabapentin, and therefore a SR looking specifically at these interventions may be worth undertaking.
The EBRSR covers studies for stroke rehabilitation including hemiplegic shoulder pain that are not included in existing systematic reviews.13 This resource summarizes graded evidence as (i) likely to be beneficial, (ii) may be beneficial, (iii) mixed literature, (iv) may not be beneficial and (v) not beneficial. Therapies that are likely to be beneficial in reducing HSP, but which are not covered by systematic reviews, include transcranial magnetic stimulation, acupressure and massage.13 Additional therapies that may be effective for reducing pain but are not covered in published systematic reviews include taping, extracorporeal shockwave therapy and interferential current therapy.13 A 2018 systematic review of treatment of CRPSoutlines an expanding role for peripheral sympathetic blockade, and trial supporting short courses of oral steroids and bisphosphonates. Whilst CRPS is considered a etiological subcategory of HSP, this systematic review was not included as it did not specifically address hemiplegic shoulder pain.99 The effect of such therapies on reducing HSP warrant consideration and further research.
Recent systematic reviews of acupuncture and electrical stimulation have drawn heavily from Chinese- and Korean-language databases, increasing considerably the number of identified trials for these interventions; however, the majority are still small and include some methodological concerns. The lack of assessment of blinding of participants in the review by Chau et al creates a gap in the understanding of the level of bias of the acupuncture trials.30 Many of the treatments included in systematic reviews were evaluated compared with or in addition to usual care rather than compared directly with placebo or sham therapy. The nature of usual care is highly variable in different settings and over time, so estimates of the additional benefit of reviewed interventions may be influenced by this.
Two main dimensions of pain measurement were identified in the systematic reviews – pain-free days and pain intensity. This is pain that is not elicited but occurs spontaneously. The most commonly used outcome measurement for pain was pain intensity, measured by VAS. Although these are both pain measures, they are a related but distinct construct. Pain elicited on passive movement of the shoulder joint by an examiner, reported as degrees of movement, is both a movement outcome and an alternative dimension of pain (ie tenderness elicited by passive movement).
Only the Cochrane Collaboration review of botulinum toxin injection conducted analyses according to the length of follow-up time.34 The current overview question was about improving HSP, implicitly at any timepoint rather than in the long term. However, ultimately the goal in the treatment of most patients is sustainable improvement in an outcome, either by repeated administration of the intervention or by a lasting effect. Many studies and reviews do not clearly answer the question about long-term improvements in pain, leaving this as an area for potential future study.
A number of interventions were identified that may improve pain in clinical practice. However, the methodological weaknesses mean that the body of evidence is still unconvincing in terms of the validity of these findings. In additional to methodological limitations, part of the inconsistency in the estimates of the effectiveness of individual interventions may be due to the multifactorial etiology of presentation and sequelae. That is, the effects of single interventions across a patient cohort may not show a strong effect on average.
There are also wider health technology considerations, in terms of potential harms, costs and capacity development that should be taken into account. Orthoses and strapping are interventions that are routinely used by medical and non-medical health practitioners for a variety of reasons. They are routinely available, low-cost, and have a low staff training burden. The evidence supporting these interventions is highly limited, so there is still uncertainty about whether they provide benefit in terms of alleviating pain. These interventions could work if applied correctly and routinely and warrant further study. Australian Stroke Guidelines cite a weak recommendation for strapping.12 The EBRSR evidence reviews conclude that shoulder taping may improve pain; this review includes trials newer than those identified in the 2014 systematic review by Appel and colleagues.13,26
Electrical stimulation and acupuncture are interventions which are also widely available and of relatively low cost for the tools and consumables. Acupuncture, in particular, requires training and certification. In the wider Australian health system these are routinely available, albeit not necessarily in traditional inpatient and outpatient stroke rehabilitation environments. The episodic nature of both make these more amenable as a sustained form of intervention; however, the subsequent impact on a practitioner’s time would be substantial.
Botulinum toxin is likely to be the most expensive of the interventions at any single point in time, although given that this needs to be administered less frequently than the other interventions, there is a degree of convenience and relatively less impact that may lend itself to being a sustainable solution. There was some evidence of possible reduction in pain due to this intervention; however, the low precision of the effect and small number of patients in the trials means there is still some uncertainty in this finding.
Conclusions
There are a number of systematic reviews that have been undertaken on the available interventions for HSP. These reviews report predominantly on non-pharmacological therapies, that in general include highly limited evidence of variable quality. Therefore, clear evidence-based recommendations on treatments are difficult based on this overview. The systematic assessment of potential associations of HSP and prophylactic interventions warrants further exploration, as prevention is the ultimate clinical goal. However, based on individual trial findings and expert opinion, there is a growing evidence base on which clinicians can refer. Due to complex etiology, recommendations regarding a single intervention or a hierarchy of interventions across this patient cohort may not be clinically appropriate. Instead, clinicians must consider the range of potential interventions and tailor their approach to individual presentation.
Acknowledgments
Jenni Suen is gratefully acknowledged for research assistance and Shannon Brown for designing the search strategies. Maria Crotty is acknowledged for contribution to development of the concept for the study.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work. SM Dyer and DA Mordaunt made equal contributions as first authors of this work.
Funding
No funding was provided for this work.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Anwer S, Alghadir A. Incidence, prevalence, and risk factors of hemiplegic shoulder pain: a systematic review. Int J Environ Res Public Health. 2020;17:14.
2. Treister AK, Hatch MN, Cramer SC, Chang EY. Demystifying poststroke pain: from etiology to treatment. PM R. 2017;9(1):63–75.
3. Bender L, McKenna K. Hemiplegic shoulder pain: defining the problem and its management. Disabil Rehabil. 2001;23(16):698–705.
4. Wanklyn P, Forster A, Young J. Hemiplegic shoulder pain (HSP): natural history and investigation of associated features. Disabil Rehabil. 1996;18(10):497–501.
5. Paci M, Nannetti L, Rinaldi LA. Glenohumeral subluxation in hemiplegia: an overview. J Rehabil Res Dev. 2005;42(4):557–568.
6. Lindgren I, Jönsson AC, Norrving B, Lindgren A. Shoulder pain after stroke: a prospective population-based study. Stroke. 2007;38(2):343–348.
7. Jönsson AC, Lindgren I, Hallström B, Norrving B, Lindgren A. Prevalence and intensity of pain after stroke: a population based study focusing on patients’ perspectives. J Neurol Neurosurg Psychiatry. 2006;77(5):590–595.
8. Snels IA, Dekker JH, van der Lee JH, Lankhorst GJ, Beckerman H, Bouter LM. Treating patients with hemiplegic shoulder pain. Am J Phys Med Rehabil. 2002;81(2):150–160.
9. Jang SH, Yi JH, Chang CH, et al. Prediction of motor outcome by shoulder subluxation at early stage of stroke. Medicine (Baltimore). 2016;95(32):e4525.
10. Adey-Wakeling Z, Liu E, Crotty M, et al. Hemiplegic shoulder pain reduces quality of life after acute stroke: a prospective population-based study. Am J Phys Med Rehabil. 2016;95(10):758–763.
11. Intercollegiate Stroke Working Party. National Clinical Guideline for Stroke. Royal College of Physicians: London; 2016.
12. Stroke Foundation. (Australian) Clinical Guidelines for Stroke Management; 2017. Available from: https://app.magicapp.org/#/guideline/WE8wOn/section/jXNMen.
13. Canadian Stroke Network. The stroke rehabilitation evidence-based review: 19th edition; 2018. Available from: www.ebrsr.com.
14. Teasell RW, Foley NC, Bhogal SK, Speechley MR. An evidence-based review of stroke rehabilitation. Top Stroke Rehabil. 2003;10(1):29–58.
15. Heart and Stroke Foundation of Canada. Rehabilitation and Recovery following Stroke. 5.3 Management of Shoulder Pain & Complex Regional Pain Syndrome (CRPS) following Stroke; 2019. Available from: https://www.strokebestpractices.ca/recommendations/stroke-rehabilitation/management-of-shoulder-pain-complex-regional-pain-syndrome-crps-following-stroke.
16. Higgins J, Thomas J, Chandler J, et al. Cochrane handbook for systematic reviews of interventions version 6.0; 2019. Available from: www.training.cochrane.org/handbook.
17. Overview of interventions for hemiplegic shoulder pain: a systematic review of systematic reviews. PROSPERO: International prospective register of systematic reviews.; 2019.
18. Moher D, Liberati A, Tetzlaff J, Altman DG. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. PLoS Med. 2009;6(7):e1000097.
19. Shea BJ, Reeves BC, Wells G, et al. AMSTAR 2: a critical appraisal tool for systematic reviews that include randomised or non-randomised studies of healthcare interventions, or both. BMJ. 2017;358:j4008.
20. Dyer SM, Harrison SL, Laver K, Whitehead C, Crotty M. An overview of systematic reviews of pharmacological and non-pharmacological interventions for the treatment of behavioral and psychological symptoms of dementia. Int Psychogeriatr. 2018;30(3):295–309.
21. Laver K, Dyer S, Whitehead C, Clemson L, Crotty M. Interventions to delay functional decline in people with dementia: a systematic review of systematic reviews. BMJ Open. 2016;6(4):e010767.
22. EndNote X9 [computer program]. Version 19: Thomson Reuters; 2019.
23. Review Manager (RevMan) [computer program]. Version 5.3: The Nordic Cochrane Centre, The Cochrane Collaboration; 2014.
24. Excel [computer program]. Version 365: Microsoft; 2019.
25. Pandian JD, Kaur P, Arora R, et al. Shoulder taping reduces injury and pain in stroke patients: randomized controlled trial. Neurology. 2013;80(6):528–532.
26. Appel C, Perry L, Jones F. Shoulder strapping for stroke-related upper limb dysfunction and shoulder impairments: systematic review. NeuroRehabilitation. 2014;35(2):191–204.
27. Guyatt G, Oxman AD, Akl EA, et al. GRADE guidelines: 1. Introduction—GRADE evidence profiles and summary of findings tables. J Clin Epidemiol. 2011;64(4):383–394.
28. Lim SM, Lee S-H. Effectiveness of bee venom acupuncture in alleviating post-stroke shoulder pain: a systematic review and meta-analysis. J Integr Med. 2015;13(4):241–247.
29. Page T, Lockwood C. Prevention and management of shoulder pain in the hemiplegic patient. JBI Lib Syst Rev. 2003;1(4):1–28.
30. Chau JPC, Lo SHS, Yu X, et al. Effects of acupuncture on the recovery outcomes of stroke survivors with shoulder pain: a systematic review. Front Neurol. 2018;9:30.
31. Qiu H, Li J, Zhou T, Wang H, Li J. Electrical stimulation in the treatment of hemiplegic shoulder pain: a meta-analysis of randomized controlled trials. Am J Phys Med Rehabil. 2019;98(4):280–286.
32. Koog YH, Jin SS, Yoon K, Min B-I. Interventions for hemiplegic shoulder pain: systematic review of randomised controlled trials. Disabil Rehabil. 2010;32(4):282–291.
33. Nadler M, Pauls M. Shoulder orthoses for the prevention and reduction of hemiplegic shoulder pain and subluxation: systematic review. Clin Rehabil. 2017;31(4):444–453.
34. Singh JA, Fitzgerald PM. Botulinum toxin for shoulder pain. Cochrane Database Syst Rev. 2010;(9):CD008271.
35. Shin BC, Lee MS. Effects of aromatherapy acupressure on hemiplegic shoulder pain and motor power in stroke patients: a pilot study. J Altern Complement Med. 2007;13(2):247–251.
36. Ancliffe J. Strapping the shoulder in patients following a cerebrovascular accident (CVA): a pilot study. Aust J Physiother. 1992;38(1):37–40.
37. Griffin A, Bernhardt J. Strapping the hemiplegic shoulder prevents development of pain during rehabilitation: a randomized controlled trial. Clin Rehabil. 2006;20(4):287–295.
38. Hanger HC, Whitewood P, Brown G, et al. A randomized controlled trial of strapping to prevent post-stroke shoulder pain. Clin Rehabil. 2000;14(4):370–380.
39. Appel C, Mayston M, Perry L. Feasibility study of a randomized controlled trial protocol to examine clinical effectiveness of shoulder strapping in acute stroke patients. Clin Rehabil. 2011;25(9):833–843.
40. Tang D, Wu WP, Sun XH. A randomized controlled trial on the effects of meridians-based acupuncture combined with function training for shoulder hand syndrome after stroke. J Clin Acupunt Moxi. 2016;32:26–29.
41. Wu MB, Liao RX, Yang HH, Li N, Ling HL, Liu XH. Observation on the clinical effects of the internal and external combined with sequential therapy for treating shoulder-hand syndrome. China Med Pharm. 2016;6:13–17.
42. Wu JY, Ye BY, Xue XH, Huang SE, Lin ZC, Hong JC. Observations on the efficacy of wrist-ankle acupuncture plus continuous exercise therapy for post-stroke shoulder pain. Shang J Acupunct Moxi. 2015;34:409–411.
43. Wu DJ, Wu ZJ, Liu WY. Effects of acupuncture combined with rehabilitation for patients with shoulder hand syndrome after stroke. J Pract Tradit Chin Med. 2017;33:169–170.
44. Xu F, Li HL, Zhang Z. A randomized controlled trial ont eh effectiveness of acupuncture combined with rehabilitation for post-stroke shoulder hand syndrome. Chin J Trauma Disabil Med. 2015;23:141–142.
45. Yang WH, Yang GF, Han SK. Effects of acupuncture combined with herbal medicine treatments for post-stroke shoulder hand syndrome. J Emerg Tradit Chin Med. 2011;20(1404):1405012.
46. Zhang XR, Lu WX. The effects of acupuncture combined with rehabilitation for stage I shoulder hand syndrome patients. China Med Eng. 2015;23:200.
47. Zhang ZY, Zhang MB. A randomized controlled trial on the effects of acupuncture combined with traditional Chinese medicine syndrome differentiation treatment on hemiplegic shoulder pain. J Pract Tradit Chin Intern Med. 2015;29:23–25.
48. Zhang ZX, Zhang Y, Yu TY, Gao HY. The effects of acupuncture on Jiantong point combined with exercise for post-stroke shoulder pain patients. Shandong Med J. 2012;52:82–83.
49. Zhong CQ, Ni DL, Lim WJ, Chen FH. Effects of acupuncture combined with rehabilitation for patients with hand shoulder syndrome after stroke. Hainan Med J. 2016;27:1687–1688.
50. Zhou XY, Chen WG. Effects of intradermal needle retention combined with acupuncture for patients with post-stroke shoulder pain. Med Forum. 2016;20:4875–4876.
51. Sun YZ, Wang YJ, Wang W. Effect of acupuncture plus rehabilitation training on shoulder-hand syndrome due to ischemic stroke. J Acupunct Tuina Sci. 2012;10:109–113.
52. Shi DK, Tang XS. Carpus-ankle acupuncture combined with physical therapy for patients with post-stroke shoulder pain: a randomized controlled trial. J Changdu Uni Tradit Chin Med. 2011;34:33–35.
53. Lin HX, Ye GQ, Liao HX, Lin FY, Liang BJ. Acupuncture combined with rehabilitation training in the treatment of shoulder-hand syndrome after stroke. World Chin Med. 2014;9(84):85–88.
54. Li B. Treating 57 cases of stroke shoulder-hand syndrome by acupuncture. Chin J Chin Med. 2015;7:40–41.
55. He SS, Gao SY. Evaluation of abdominal acupuncture and rehabilitation treatment for shoulder-hand syndrome (period 1) after stroke. J Clin Acupunt Moxi. 2016;32:11–13.
56. Chen J. Effects of acupuncture combined with exercise for patients with post-stroke shoulder pain. Womens Health Res. 2016;9:79–81.
57. Chen Y, Huang TS, Liu KC. Clinical research of using acupuncture and rehabilitation training in the treatment of post-stroke shoulder-hand syndrome stage I. J Sichuan Tradit Chin Med. 2015;33:150–152.
58. Chen HX, He MF, Xie RM. Clinical observation on the combination of abdominal acupuncture and rehabilitation in treating omalgia after stroke. J Nanjing Univ Tradit Chin Med. 2011;27:333–335.
59. Bao YH, Wang YW, Chu JM, Zhu GX, Wang CM, Hou HM. Effects of electro-acupuncture combined with rehabilitation on improving upper extremity function for patients with post-stroke shoulder pain. Chin J Tradit Med Sci Tech. 2012;19:59–60.
60. Bu L, Xu HQ, Tan WJ, Di RK. Effects of electro-acupuncture combined with scapular control training on shoulder pain and upper limbs function in hemiplegia patients. Glob Tradit Chin Med. 2013;6:246–247.
61. Hong LR, Chen B, Yu SM, Huang XS, Wang JP, Xia Y. Efficacy of acupuncture plus rehabilitation training in treating shoulder-hand syndrome after hemiparalysis. Med J Chin Peoples Armed Police Forces. 2011;22:658–660.
62. Jia CJ, Ni GX, Tan H, Zhang X. Effects of acupuncture combined with rehabilitation for stroke survivors with stage I shoulder hand syndrome. J Changchun Univ Tradit Chin Med. 2012;4:711–712.
63. Wang X, Wang WQ. Clinical studies on the effectiveness of fire needle treatment for patients with shoulder hand syndrome. Guangming J Chin Med. 2011;26(4):754–756.
64. Xu ZQ, Wang SX, Zhou ZH. Clinical studies on fire needle treatment of stroke shoulder-hand syndrome stage I. Chin J Chin Med. 2016;31:753–755.
65. Nie W, Zhao H. Clinical study on the treatment of shoulder-hand syndrome by warming and dredging triple energizer plus rehabilitation training. Shanghai J Acupunct Moxi. 2011;30:217–219.
66. Porritt K, Gomersall J, Lockwood C. JBI’s systematic reviews: study selection and critical appraisal. Am J Nurs. 2014;114(6):47–52.
67. Huang Y-C, Leong C-P, Wang L, et al. The effects of hyaluronic acid on hemiplegic shoulder injury and pain in patients with subacute stroke: a randomized controlled pilot study. Medicine. 2016;95(49):e5547–e5547.
68. Han SK. Effect of Buqi Huatan Tongluo recipe combined with interior-exterior meridians acupuncture for patients with should-hand syndrome after stroke. J New Chin Med. 2011;43:97–99.
69. Bao YH, Wang YW, Chu JM, Zhu GX, Wang CM, Hou HM. Effects of electro-acupuncture combined with rehabilitation for patients with post-stroke shoulder pain. Chin Arch Tradit Chin Med. 2011;29:2536–2539.
70. Yang D, Xie M, Zhang CE, Ye BY, Song GM. Effects of electro-acupuncture combined with rehabilitation for patients with should hand syndrome. Liaoning J Tradit Chin Med. 2009;36:1770–1771.
71. Choe S, Cai M, Jerng UM, Lee J-H, Efficacy T. Underlying mechanism of moxibustion in preventing cognitive impairment: a systematic review of animal studies. Exp Neurobiol. 2018;27(1):1–15.
72. Park J-M, et al. Effectiveness of bee venom acupuncture on shoulder pain after stroke. J Korean Oriental Med. 2007;28:11–24.
73. Lee D, Lee G, Yeom S, Kim D, Kim D. A clinical study of bee venom acupuncture therapy on shoulder pain patients in stroke sequelae. J Korean Acupunct Moxibustion Soc. 2006;23:69–80.
74. Park Y, Jun H, Chae Y, Park H, Kim B, Chang I. The effects of seet bee venom pharmacopuncture on post-stroke hemiplegic shoulder pain. J Korean Acupunct Moxibustion Soc. 2011;28:37–47.
75. Hartwig M, Gelbrich G, Griewing B. Functional orthosis in shoulder joint subluxation after ischaemic brain stroke to avoid post-hemiplegic shoulder-hand syndrome: a randomized clinical trial. Clin Rehabil. 2012;26(9):807–816.
76. Ekim A, Armagan O, Oner C. [Efficiency of TENS treatment in hemiplegic shoulder pain: a placebo controlled study]. Agri. 2008;20(1):41–46.
77. Mao Y, Xue L, Xue J. Efficacy of low frequency electric stimulation plus acupuncture for hemiplegia and shoulder pain. Med J Qilu. 2016;31:592–593.
78. Chae J, Yu DT, Walker ME, et al. Intramuscular electrical stimulation for hemiplegic shoulder pain: a 12-month follow-up of a multiple-center, randomized clinical trial. Am J Phys Med Rehabil. 2005;84(11):832–842.
79. Wilson RD, Gunzler DD, Bennett ME, Chae J. Peripheral nerve stimulation compared with usual care for pain relief of hemiplegic shoulder pain: a randomized controlled trial. Am J Phys Med Rehabil. 2014;93(1):17–28.
80. Leandri M, Parodi CI, Corrieri N, Rigardo S. Comparison of TENS treatments in hemiplegic shoulder pain. Scand J Rehabil Med. 1990;22(2):69–71.
81. Fu M, Kong S. Efficacy observation on functional electrical stimulation for shoulder pain after stroke. Chinese Manipul Rehabil Med. 2015;(6):11–14.
82. Singh JA, Fitzgerald PM. Botulinum toxin for shoulder pain: a cochrane systematic review. J Rheumatol. 2011;38(3):409–418.
83. de Boer KS, Arwert HJ, de Groot JH, Meskers CG, Mishre AD, Arendzen JH. Shoulder pain and external rotation in spastic hemiplegia do not improve by injection of botulinum toxin A into the subscapular muscle. J Neurol Neurosurg Psychiatry. 2008;79(5):581–583.
84. Kong KH, Neo JJ, Chua KS. A randomized controlled study of botulinum toxin A in the treatment of hemiplegic shoulder pain associated with spasticity. Clin Rehabil. 2007;21(1):28–35.
85. Marco E, Duarte E, Vila J, et al. Is botulinum toxin type A effective in the treatment of spastic shoulder pain in patients after stroke? A double-blind randomized clinical trial. J Rehabil Med. 2007;39(6):440–447.
86. Yelnik AP, Colle FM, Bonan IV, Vicaut E. Treatment of shoulder pain in spastic hemiplegia by reducing spasticity of the subscapular muscle: a randomised, double blind, placebo controlled study of botulinum toxin A. J Neurol Neurosurg Psychiatry. 2007;78(8):845–848.
87. Tao W, Fu Y, Hai-Xin S, Yan D, Jian-Hua L. The application of sonography in shoulder pain evaluation and injection treatment after stroke: a systematic review. J Phys Ther Sci. 2015;27(9):3007–3010.
88. Mok E, Woo CP. The effects of slow-stroke back massage on anxiety and shoulder pain in elderly stroke patients. Complement Ther Nurs Midwifery. 2004;10(4):209–216.
89. Li N, Tian F, Wang C, et al. Therapeutic effect of acupuncture and massage for shoulder-hand syndrome in hemiplegia patients: a clinical two-center randomized controlled trial. J Tradit Chin Med. 2012;32(3):343–349.
90. Shin BC, Lim HJ, Lee MS. Effectiveness of combined acupuncture therapy and conventional treatment on shoulder range of motion and motor power in stroke patients with hemiplegic shoulder subluxation: a pilot study. Int J Neurosci. 2007;117(4):519–523.
91. Jeon HJ, An S, Yoo J, Park NH, Lee KH. The effect of Monkey Chair and Band exercise system on shoulder range of motion and pain in post-stroke patients with hemiplegia. J Phys Ther Sci. 2016;28(8):2232–2237.
92. Partridge CJ, Edwards SM, Mee R, van Langenberghe H. Hemiplegic shoulder pain: a study of two methods of physiotherapy treatment. Clin Rehabil. 1990;4(1):43–49.
93. Kim SH, Ha KW, Kim YH, et al. Effect of radial extracorporeal shock wave therapy on hemiplegic shoulder pain syndrome. Ann Rehabil Med. 2016;40(3):509–519.
94. Jan F, Naeem A, Malik AN, Amjad I, Malik T. Comparison of low level laser therapy and interferential current on post stroke shoulder pain. J Pak Med Assoc. 2017;67(5):788–789.
95. Suriya-amarit D, Gaogasigam C, Siriphorn A, Boonyong S. Effect of interferential current stimulation in management of hemiplegic shoulder pain. Arch Phys Med Rehabil. 2014;95(8):1441–1446.
96. Choi GS, Chang MC. Effects of high-frequency repetitive transcranial magnetic stimulation on reducing hemiplegic shoulder pain in patients with chronic stoke: a randomized controlled trial. Int J Neurosci. 2018;128(2):110–116.
97. Adey-Wakeling Z, Crotty M, Shanahan EM. Suprascapular nerve block for shoulder pain in the first year after stroke: a randomized controlled trial. Stroke. 2013;44(11):3136–3141.
98. Ratmansky M, Defrin R, Soroker N. A randomized controlled study of segmental neuromyotherapy for post-stroke hemiplegic shoulder pain. J Rehabil Med. 2012;44(10):830–836.
99. Duong S, Bravo D, Todd KJ, Finlayson RJ, Tran Q. Treatment of complex regional pain syndrome: an updated systematic review and narrative synthesis. Can J Anaesth. 2018;65(6):658–684.
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.