")
Back to Journals » Journal of Inflammation Research » Volume 15
Interstitial Lung Disease as an Extraintestinal Manifestation of Crohn’s Disease in the Time of COVID-19: A Rare Case Report and Review of the Literature
Authors Li L, Liu P, Niu X, He C
Received 9 July 2022
Accepted for publication 24 September 2022
Published 10 October 2022 Volume 2022:15 Pages 5733—5737
DOI https://doi.org/10.2147/JIR.S380879
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Ning Quan
Lin Li,* Pengwei Liu,* Xiaoping Niu, Chiyi He
Departments of Gastroenterology, The First Affiliated Hospital of Wannan Medical College, Wuhu, 241001, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Xiaoping Niu; Chiyi He, Departments of Gastroenterology, Yijishan Hospital of Wannan Medical College, Wuhu, 241001, People’s Republic of China, Email [email protected]; [email protected]
Introduction: Recently, the extraintestinal manifestations of Crohn’s disease (CD) have attracted more and more attention, among which interstitial lung disease (ILD) is a rare extraintestinal manifestation. Clinical presentation is polymorphic and pathogenesis remains unclear. The purpose of this article is to elaborate on these rare extraintestinal manifestations of CD, and the importance of short-term chest computed tomography (CT) for differential diagnosis is emphasized.
Case Presentation: A 27-year-old male patient, who is a student, presented with chief complaints of “loose stools for 4 months, intermittent low-grade fever for 1 month”. The next day, he developed a high fever with a body temperature of 39.8°C. A chest CT scan revealed multiple patellar ground glass shadows which suggested ILD. In the time of Corona virus disease (COVID-19), novel coronavirus pneumonia was first suspected according to the patient’s history and symptoms, but laboratory examinations did not confirm. Colonoscopy showed multiple ulcers between the sigmoid colon to the terminal ileum, and pathology found epithelioid granuloma in submucosa. Moreover, a total gastrointestinal CT angiography showed that segmental leaping thickening of the bowel. Based on the above results, we ultimately made a diagnosis of CD. After using systemic steroid therapy, his fever was quickly relieved, and a follow-up chest CT showed that multiple patellar ground glass shadows were almost completely absorbed. Then, infliximab was used, and a repeat colonoscopy showed that intestinal ulcers were significantly improved.
Conclusion: ILD is a rare extraintestinal manifestation of CD and reveals the excellent response to systemic steroid therapy. Manifestations of pulmonary disease associated with IBD are polymorphic; therefore; clinicians should be more vigilant regarding IBD-related ILD, especially when infectious causes have been excluded in the time of COVID-19. For those with ILD related to IBD, a short-term follow-up CT would be crucial.
Keywords: Crohn’s disease, interstitial lung disease, steroid, infliximab
Introduction
Crohn’s disease (CD) is a chronic inflammatory disease of the intestine, of unknown etiology, which is characterized by a discontinuous, segmental manifestation and implication of all intestinal layers. Extra-intestinal manifestations of CD, characterized by inflammatory conditions outside the digestive tract, occur in about 25% of patients.1 Peripheral arthritis, erythema nodosum, pyoderma gangrene, episcleritis, anterior uveitis, oral recurrent ulcer, and ankylosing spondylitis are the most common extra-intestinal manifestations.2 However, inflammatory bowel disease (IBD)-related lung diseases are increasingly recognized. IBD-related respiratory diseases have a variety of clinical manifestations, which can involve the airway and lung interstitial pulmonary vessels, and usually appear several years preceding the diagnosis of IBD.3,4 Ulcerative colitis (UC) is more likely to involve the respiratory system than CD, and lung involvement can aggravate the condition of IBD and is a risk factor for poor prognosis.5
The clinical symptoms of IBD-associated lung disease are hidden, which increases the difficulty of diagnosis. Zhao et al6 found that only 2.7% of IBD patients had respiratory symptoms. Karadag et al7 reported that 15 UC patients were complicated with ground-glass changes in the lungs, but none of them felt uncomfortable. During the time of Corona virus disease (COVID-19), the imaging signs of novel coronavirus pneumonia can also present as interstitial lung disease (ILD), which is difficult to distinguish from the extraintestinal manifestations of CD.
We present a case of a patient with multiple intestinal ulcers associated with ILD in the time of COVID-19. This case had no pulmonary symptoms, which was consistent with previous studies. The purpose of this article is to elaborate on these rare extraintestinal manifestations of CD and to reveal that IBD-related ILD responds excellently to systemic steroid therapy. Moreover, the importance of short-term follow-up chest computed tomography (CT) for differential diagnosis is emphasized.
Case Presentation
On December 9, 2020, a 27-year-old male patient, who is a student, presented with chief complaints of “loose stools for 4 months, intermittent low-grade fever for 1 month”, and he was admitted to the Departments of Gastroenterology, The First Affiliated Hospital of Wannan Medical College. His complaints did not include abdominal pain, abdominal distension, bloody purulent stool, cough, expectoration, chest tightness and shortness of breath. And a physical examination revealed no abnormalities. This patient has just returned from Japan (November 2, 2020) and has been quarantined for 14 days twice. In Japan, colonoscopy (October 7, 2020) showed multiple ulcers between the sigmoid colon to the terminal ileum (Figure 1A–D), and pathology found that inflammatory cell infiltration in intestinal mucosa and epithelioid granuloma in submucosa (Figure 1E). Regular use of mesalazine did not significantly improve the symptoms of loose stools. Meanwhile, taking levofloxacin orally was not effective for his fever.
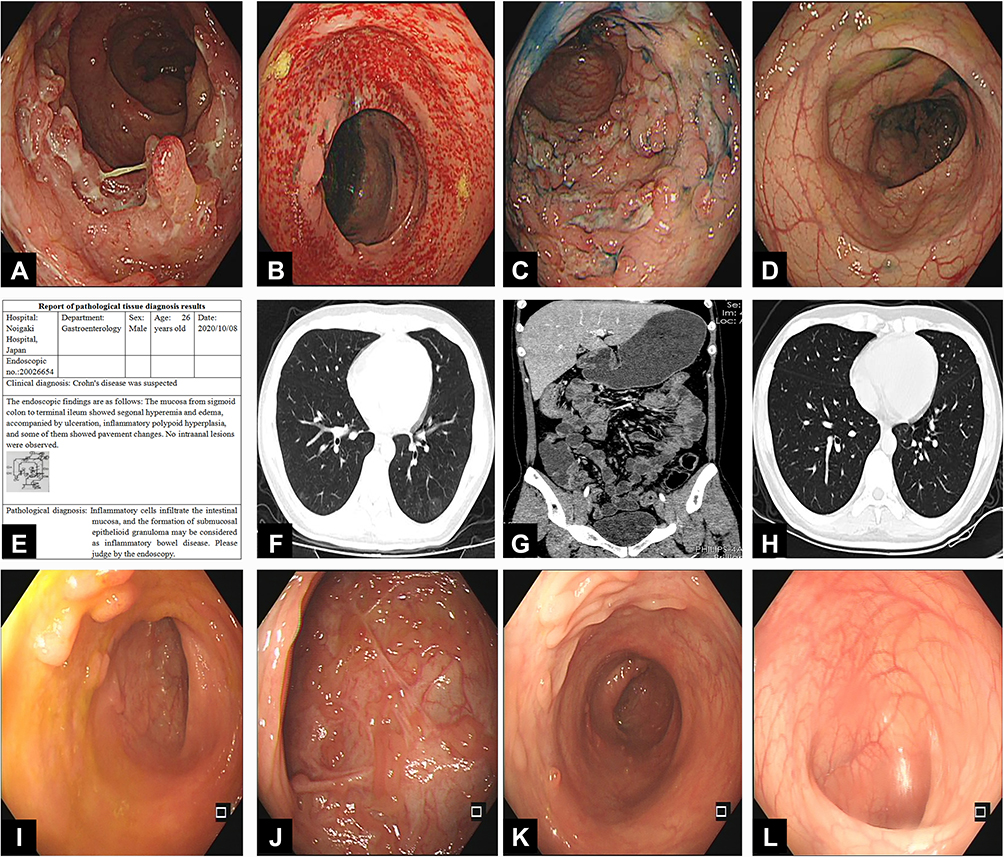 |
Figure 1 (A–D) Colonoscopy showed segmental intestinal disease; (E) pathology found inflammatory cell infiltration in intestinal mucosa, epithelioid granuloma in submucosa; (F) chest CT scan showed multiple patchy ground-glass shadows; (G) a total gastrointestinal CT angiography showed segmental leaping thickening in part of colon; (H) a repeat chest CT scan after systemic steroid therapy; (I–L) a repeat colonoscopy after three infliximab treatments. |
Laboratory investigations revealed a normocytic anaemia (hemoglobin 92g/L), hypoproteinemia (albumin 28.8g/L), raised inflammatory markers (C-reactive protein (CRP) 72.9mg/L, erythrocyte sedimentation rate (ESR) 74mm/h) and thrombocytosis (PLT 675*10^9/L). Examination of pathogenic microorganisms suggested that rubella virus immunoglobulin G (IgG) was 208.5IU/mL and cytomegalovirus IgG was 184.4U/mL, which were exceeds the normal limit. Fecal bacteria proportion showed that gram-positive coccus 10%, gram-positive bacillus 10%, gram-negative bacillus 80%, and no fungal spores were found. Fecal occult blood (OB) is negative, and no obvious abnormality was observed in tuberculosis antibody (TB-AB), tuberculous infection with T cells (T-sport), purified protein-derived tuberculin (PPD), blood coagulation, routine before blood transfusion and tumor markers.
The next day (December 10, 2020), the patient developed a high fever with a body temperature of 39.8°C. A chest high resolution computed tomography (HRCT) was urgently performed and result showed infectious lesions in the upper lobe of the right lung and the lower lobe of both lungs, with multiple patchy ground-glass shadows and nodular ground-glass shadows, which suggested interstitial pneumonia (Figure 1F). Then, multiple novel coronavirus (2019-nCoV) pneumonia nucleic acid test was performed, and the results were all negative. Despite the empirical antibiotic and antiviral therapy that was started, his fever remained.
On the third day after admission (December 12, 2020), laboratory investigations revealed that fecal OB was positive and hemoglobin dropped from 92g/L to 84g/L. On the other hand, fecal general flora, Salmonella and Shigella culture were all negative. Acid-fast bacilli and general bacterial cultures in sputum were also negative. Gastroscopy showed chronic superficial gastritis. A total gastrointestinal CT angiography showed that segmental leaping thickening in part of jejunum, distal ileum, ileocecal, ascending colon and transverse colon, proliferation of peripheral small vessels, multiple enlarged lymph nodes around the diseased intestine and at the root of mesenteric vessels (Figure 1G). Pelvic magnetic resonance revealed no abnormalities, which suggested that the patient was without an internal fistula.
Based on the above evidences, this patient was finally diagnosed with CD, according to the World Gastroenterology Organization.8 According to the Montreal classification of IBD9 and Harvey and Bradshaw’s simplified Crohn’s disease activity index (CDAI) method,10 this patient was classified as A2L3B1, and his CDAI was 433.
Then, we used steroids 50mg/d, and the temperature was returned to normal quickly. A follow-up chest CT after 5 days (December 15, 2020) showed that multiple patellar ground glass shadows were almost completely absorbed under the pleura of the lower lobe of both lungs (Figure 1H). Then, infliximab was used. We can see the inflammatory markers were decreased gradually; however, nutritional status indicators were increased gradually. Meanwhile, fecal OB was negative and stool property returned to normal. A repeat colonoscopy after 4 months (April 19, 2021) revealed multiple hyperplastic small polyps in the terminal ileum, ascending colon, transverse colon and descending colon, with some scars (Figure 1I–L). And repeat laboratory investigations after 4 months showed that hemoglobin was 132g/L, platelet was 253*10^9/L, albumin 44.3g/L, CRP 0.88mg/L, ESR 4.7mm/h. He gained 10kg in weight.
Discussion
ILD was a rare extraintestinal manifestation associated with IBD.11 In 1976, Kraft first proposed that IBD can involve the respiratory tract, manifested as bronchitis, bronchiectasis, and chronic obstructive pulmonary disease.12 Pulmonary manifestations, despite being considered rare with an unknown prevalence, are increasingly recognized.13 Recently, Eliadou et al5 found that UC was more likely to involve ILD than CD. More than 50% of cases were drug-related, these drugs included mesalazine, golimumab, methotrexate, vedolizumab and infliximab. A large-scale study of the safety of infliximab in rheumatic patients showed that the probability of developing ILD was 0.5%.14 The symptoms of drug-related ILD included cough, shortness of breath, fever and lethargy with a mean duration of symptoms of 6.3 weeks, however symptoms were relieved after systemic steroid therapy. Patients can present with almost all histopathological patterns of ILD. Schwaiblmair et al15 reported that extremes of age, sex, ethnicity, oxygen, dose of medication, drug interaction and underlying lung disease were risk factors for developing drug-related lung disease.
In this study, our case had no pulmonary symptoms, which was consistent with previous studies6,7 but was not consistent with drug-related ILD mentioned above. This patient had negative virology and bacterial screen, and his fever improved rapidly after the administration of steroids. Therefore, we excluded the possibility of drug-induced ILD in this patient.
Clinical presentation of pulmonary disease associated with IBD is polymorphic and pathogenesis remains unclear. On the CT, pulmonary manifestations related to IBD are scattered, nonsegmental, unilateral or bilateral foci of consolidation, ill-defined centrilobular nodules, large irregular nodules, lung parenchymal mass-like lesions.16 However, the CT findings of our case were multiple patchy ground-glass shadows and nodular ground-glass shadows, which were similar to a reported case with novel coronavirus pneumonia.17 However, the main manifestations of novel coronavirus-associated pneumonia are thickening and blurring of lung texture and interweaving into a network, accompanied by ground glass shadow, patchy nodular or mass consolidation. In this case, both the empirical antibiotic and antiviral therapies were not effective, after diagnosing with CD, steroid therapy was used. A follow-up chest CT 5 days later showed that the pulmonary lesions had almost been cured. Thus, it is important to recognize these manifestations because they may mimic other diseases, leading to incorrect treatment. In addition, a short-term follow-up CT would be crucial.
This case had a high fever, did this fever relate to bowel disease activity or extraintestinal manifestations of CD? The fever was not relieved despite both antibiotic and antiviral therapies were used. On the other hand, during the period of fever, his intestinal manifestations were not aggravated. However, after using steroid therapy, his fever quickly relieved. Therefore, we concluded that his fever was related to the ILD associated with CD.
Colonic ulcers or interstitial lung disease, which comes first? Previous reported studies3,4 revealed that respiratory involvement may precede presentation of bowel disease by months or years. However, ILD appeared nearly 4 months after intestinal symptoms of CD in this case, which was consistent with another research.18
Overall, the prognosis of this patient is good as it responds well to treatment with systemic steroids and infliximab followed. The use of steroids is effective in treating the clinical symptoms of pulmonary involvement, and the symptoms of intestinal ulcers of CD are responding well to biological agent therapy.
Conclusions
In conclusion, as shown in Table 1, ILD is a rare extraintestinal manifestation, and only systemic steroid therapy is effective. Manifestations of pulmonary disease associated with IBD are polymorphic; therefore, clinicians should be more vigilant regarding IBD-related ILD and to avoid incorrect treatment, when infectious causes have been excluded especially in the time of COVID-19. Early recognition and treatment are important. For those with ILD related to IBD, a short-term follow-up CT would be crucial.
 |
Table 1 All Points Summarized in This Article |
Data Transparency
All information about the patient comes from the Department of Gastroenterology and Infection, Yijishan Hospital of Wannan Medical College. The data underlying this article are available in the article and will be shared on reasonable request to the corresponding author.
Ethics Approval and Consent to Participate
This study was approved by the Institutional Ethical Review Committee of the First Affiliated Hospital of Wannan Medical College. Written informed consent to publish the case details was obtained from the patient.
Acknowledgments
We sincerely thank the department of radiology and infection in our hospital for providing information.
Funding
No funding was received for this study.
Disclosure
The authors have no competing interests to declare that are relevant to the content of this article.
References
1. Ephgrave K. Extra-intestinal manifestations of Crohn’s disease. Surg Clin North Am. 2007;87(3):673–680. doi:10.1016/j.suc.2007.03.003
2. Desai D, Patil S, Udwadia Z, Maheshwari S, Abraham P, Joshi A. Pulmonary manifestations in inflammatory bowel disease: a prospective study. Indian J Gastroenterol. 2011;30(5):225–228. doi:10.1007/s12664-011-0129-1
3. Camus P, Colby TV. The lung in inflammatory bowel disease. Eur Respir J. 2000;15(1):5–10. doi:10.1183/09031936.00.15100500
4. Shulimzon T, Rozenman J, Perelman M, Bardan E, Ben-Dov I. Necrotizing granulomata in the lung preceding colonic involvement in 2 patients with Crohn’s disease. Respiration. 2007;74:698–702. doi:10.1159/000092854
5. Eliadou E, Moleiro J, Ribaldone DG, et al. Interstitial and granulomatous lung disease in inflammatory bowel disease patients. J Crohns Colitis. 2020;14(4):480–489. doi:10.1093/ecco-jcc/jjz165
6. Zhao YJ, Xia YJ, Liu ZJ. Clinical evaluation of lung function in 74 patients with inflammatory bowel disease. Chin J Dig. 2014;34(6):379–383. doi:10.3760/cma.j.issn.0254-1432.2014.06.004
7. Karadag F, Ozhan MH, Akçiçek E, Günel O, Alper H, Veral A. Is it possible to detect ulcerative colitis-related respiratory syndrome early? Respirology. 2001;6(4):341–346. doi:10.1046/j.1440-1843.2001.00347.x
8. Bernstein CN, Fried M, Krabshuis JH, et al. World gastroenterology organization practice guidelines for the diagnosis and management of IBD in 2010. Inflamm Bowel Dis. 2010;16(1):112–124. doi:10.1002/ibd.21048
9. Satsangi J, Silverberg MS, Vermeire S, Colombel JF. The Montreal classification of inflammatory bowel disease: controversies, consensus and implication. Gut. 2006;55(6):749–753. doi:10.1136/gut.2005.082909
10. Harvey RF, Bradshaw JM. A simple index of Crohn’s-disease activity. Lancet. 1980;1(8167):514. doi:10.1016/s0140-6736(80)92767-1
11. Black H, Mendoza M, Murin S. Thoracic manifestations of inflammatory bowel disease. Chest. 2007;131:524–532. doi:10.1378/chest.06-1074
12. Kraft SC, Earle RH, Roesler M, Esterly JR. Unexplained bronchopulmonary disease with inflammatory bowel disease. Arch Intern Med. 1976;136:454–459.
13. Casella G, Villanacci V, Di Bella C, Antonelli E, Baldini V, Bassotti G. Pulmonary diseases associated with inflammatory bowel diseases. J Crohns Colitis. 2010;4:384–389. doi:10.1016/j.crohns.2010.02.005
14. Ostör AJ, Chilvers ER, Somerville MF, et al. Pulmonary complications of infliximab therapy in patients with rheumatoid arthritis. J Rheumatol. 2006;33(3):622–628.
15. Schwaiblmair M, Behr W, Haeckel T, Märkl B, Foerg W, Berghaus T. Drug induced interstitial lung disease. Open Respir Med J. 2012;6:63–74. doi:10.2174/1874306401206010063
16. Betancourt SL, Palacio D, Jimenez CA, Martinez S, Marom EM. Thoracic manifestations of inflammatory bowel disease. AJR Am J Roentgenol. 2011;197(3):W452–6. doi:10.2214/AJR.10.5353
17. An P, Song P, Lian K, Wang Y. CT manifestations of novel coronavirus pneumonia: a case report. Balkan Med J. 2020;37(3):163–165. doi:10.4274/balkanmedj.galenos.2020.2020.2.15
18. Xie F, Fang QH, Bu XN. Clinical characteristics of 12 cases of respiratory diseases associated with inflammatory bowel disease. Zhonghua Jie He He Hu Xi Za Zhi. 2018;41(09):724–727.
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.