")
Back to Journals » Drug Design, Development and Therapy » Volume 8
Interleukin 1 inhibition with anakinra in adult-onset Still disease: a meta-analysis of its efficacy and safety
Authors Hong D, Yang Z, Han S, Liang X, Ma K, Zhang X, Sang Y
Received 29 August 2014
Accepted for publication 25 September 2014
Published 25 November 2014 Volume 2014:8 Pages 2345—2357
DOI https://doi.org/10.2147/DDDT.S73428
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Shu-Feng Zhou
Dongsheng Hong,1 Zhihai Yang,1 Shuyin Han,1 Xingguang Liang,1 Kuifen Ma,1 Xingguo Zhang1,2
1Department of Pharmacy, the First Affiliated Hospital of College of Medicine, Zhejiang University, 2College of Pharmaceutical Science, Zhejiang Chinese Medical University, Hangzhou, People’s Republic of China
Background: Anakinra is the first interleukin-1 inhibitor to be used in clinical practice, and recent evidence showed that interleukin-1 plays a pivotal role in the pathogenesis of adult-onset Still disease (AoSD). However, data concerning efficacy with anakinra use in different clinical trials has not been evaluated, and the overall remission of AoSD with anakinra treatment has not been well defined.
Methods: We conducted a search on Embase, PubMed, and the Cochrane Library for relevant trials. Statistical analyses were conducted to calculate the overall remission rates, odds ratios (OR), and 95% confidence intervals (CI), by using either random effects or fixed effect models according to the heterogeneity.
Results: Of the 273 articles that were identified, 265 were excluded. Eight studies were eligible for inclusion. The overall remission rate and complete remission rate of anakinra in AoSD patients were 81.66% (95% CI: 69.51%–89.69%) and 66.75% (95% CI: 59.94%–75.3%), respectively. Compared with the controls, the use of anakinra was associated with a significant remission in AoSD, with an OR of 0.16 (95% CI: 0.06–0.44, P=0.0005). There were also significant reductions of the dosage of corticosteroid (mean difference =21.19) (95% CI: 13.2–29.18, P<0.0001) from anakinra onset to the latest follow up time. Clinical and laboratory parameters were all improved, and anakinra was well tolerated in patients with AoSD. No evidence of publication bias was observed.
Conclusion: Our study has shown that anakinra is effective in remitting the manifestations of AoSD, with reduction of the dose of corticosteroid in patients with AoSD. Further, anakinra therapy was not associated with increased risk of adverse events, and it was well tolerated in patients with AoSD. Further research is still recommended to investigate these findings.
Keywords: interleukin-1 inhibitor, AoSD, anakinra, adverse events, clinical and laboratory parameters, efficacy
Introduction
Adult-onset Still disease (AoSD) is a rare multisystemic inflammatory disorder manifested by a variety of clinical features, including high, spiking fever, evanescent skin rash, hepatosplenomegaly, lymphadenopathy, polyarthritis, and other systemic symptoms.1,2 The pathogenesis of AoSD is currently unclear,3 and the therapeutic strategies of AoSD can be varied according to its clinical presentation.4–6 Nonsteroidal anti-inflammatory drugs (NSAIDs) and corticosteroids are commonly used as first-line agents for AoSD,7,8 and if first-line treatment is ineffective, disease-modifying antirheumatic drugs (DMARDs), such as methotrexate are added.9 Corticosteroids can control the manifestations of AoSD in about 65% of patients,10 and the response to corticosteroids is often quick, within a few hours.11,12 However, corticosteroids easily induce dependence – steroid dependence occurred in 42% of the cases in one study.13 Long-term steroid exposure in patients carries the potential for serious side effects, such as infection.6 Currently, many patients need other options to control the clinical presentation of the disease or to reduce corticosteroid dependence.
Hence, in clinical practice, physicians are often prone to adopt other therapeutic strategies, even in the absence of large-scale clinical trials data. The blockade of the interleukin-1 (IL-1) pathway has emerged as a new therapeutic strategy since recent evidence showed that IL-1 could play a pivotal role in the pathogenesis of AoSD.14–16 Anakinra is the first IL-1 inhibitor to be used in clinical practice.17 Rudinskaya and Trock18 reported the first case of the treatment of AoSD with anakinra in 2003, including just one patient, and it was shown to rapidly improve the clinical symptoms and laboratory disease activity markers of AoSD. To date, there is little information on treatment efficacy of anakinra in AoSD, with a paucity of prospective double-blinded randomized trials, but one important randomized controlled trial (RCT) has demonstrated its rapid efficacy in patients with rheumatoid arthritis.19 Indeed, anakinra is the most commonly described anti-IL-1 agent. In 2007, two case series including eight subjects described a good efficacy of anakinra in steroid- and DMARD-refractory AoSD with systemic symptoms;14,20 however, the data concerning efficacy with anakinra treatment has not been evaluated in different clinical trials, and the overall remission of AoSD with anakinra treatment has not been well defined. AoSD is a rare multisystemic disorder, which if not accurately treated in time, can progress to death. The treatment strategies are poor currently, therefore, we conducted this systematic review and meta-analysis to summarize the results of studies and evaluate the evidence for efficacy and safety of anakinra in AoSD.
Methods
Search strategy and study selection
We searched Embase, PubMed, and the Cochrane Library database from onset to August 15, 2014, using the following search terms treated as Medical Subject Headings (MeSH) terms or free text: (“adult onset Still’s disease” or “adult onset stills disease” or “adult onset Still disease” or “Still’s disease” or “stills disease” or “still disease” or “Still’s Disease, Adult-Onset”) and (“Interleukin 1 Receptor Antagonist Protein” or “anakinra”). Additionally, we searched the clinical trials registry (ClinicalTrials.gov) to obtain information on the registered clinical trials. The detailed search strategy is given in Figure S1.
The following criteria were used for inclusion for study selection: (1) patients were diagnosed with AoSD according to the preliminary classification by Cush et al,21 Yamaguchi et al,22 or Fautrel et al;23 (2) studies that reported the efficacy of anakinra in AoSD patients; and (3) prospective or retrospective studies with or without a control group. Studies were excluded if they did not show sufficient data, such as number of patients with partial response or complete response, results of clinical and laboratory parameters, the dose of corticosteroid in the treatment, or the adverse events for anakinra in AoSD patients.
Data extraction and quality assessment
Data extraction was conducted by two independent investigators (DSH and ZHY), and discrepancies were identified and resolved by consensus. For each study, the following information was extracted: year of publication, first author’s name, treatment arm, mean duration of follow up, number of patients in the treatment and control groups, number of patients with partial response or complete response in the treatment, number of patients with adverse events in the treatment, measurements of clinical and laboratory parameters (including C-reactive protein [CRP], erythrocyte sedimentation rate [ESR], and arthritis symptoms) in the treatment.
A quality score for each study was determined according the earlier reports, using consequential binomial parameters (Table S1).24,25 Each parameter was given a numerical score of 0 or 1, with an overall quality score ranging from 0 to 10. Studies with a quality score of <5 were rated as poor, while those ≥5 were rated as high.
Data synthesis and statistical analysis
For the calculation of remission rate, the number of patients with partial response or complete response in the anakinra group, and the total number of patients receiving anakinra were extracted from the selected clinical trials; for each study, the proportion of patients with remission rates and the 95% confidence interval (CI) were derived. The remission rate of anakinra therapy versus controls was expressed as odds ratio (OR) with 95% CI. Heterogeneity was assessed by using the Q statistic and I2 tests among trials.26 Heterogeneity was considered statistically significant when P<0.1 (for heterogeneity) or I2 >40%.27 If heterogeneity existed, the data was analyzed using a random effects model; if heterogeneity did not exist, a fixed effect model was used. A statistical test with a P-value less than 0.05 was considered significant. The presence of publication bias was evaluated by using funnel plots.27 All statistical analysis was performed by using R software, version 3.0.3 (The R Core Team, Vienna, Austria) (http://www.r-project.org).
Results
Description of studies
A total of 273 potentially studies were reviewed, and 265 were excluded (Figure 1). The remaining eight studies,13,28–34 with 134 subjects, that met our inclusion criteria were included in our analyses. The major baseline characteristics of the eight studies are listed in Table 1. The studies included one RCT29 and seven observational studies.13,28,30–34 The geographical distribution of these studies was over various countries, with four studies from France,13,28,31,34 two from Greece,32,33 and one from Italy.30 One RCT included 22 patients from ten centers in Finland, Norway, and Sweden.29 These studies were all published between 2010 and 2014, and the dose of anakinra was 100 mg/day. The sample size of each study ranged from six to 28 treated patients. The majority of the studies were of good quality (mean quality score =6), as shown in the detailed information given in Table S1.
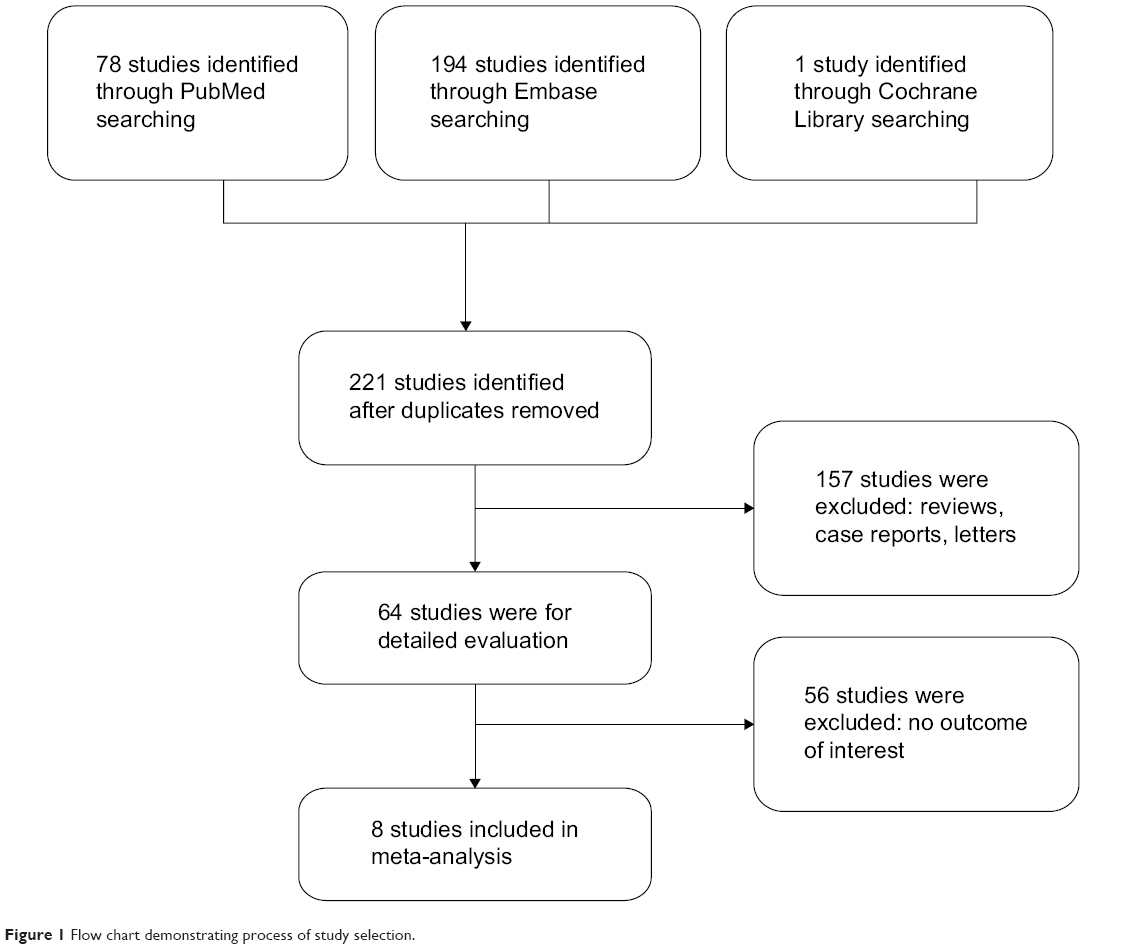 | Figure 1 Flow chart demonstrating process of study selection. |
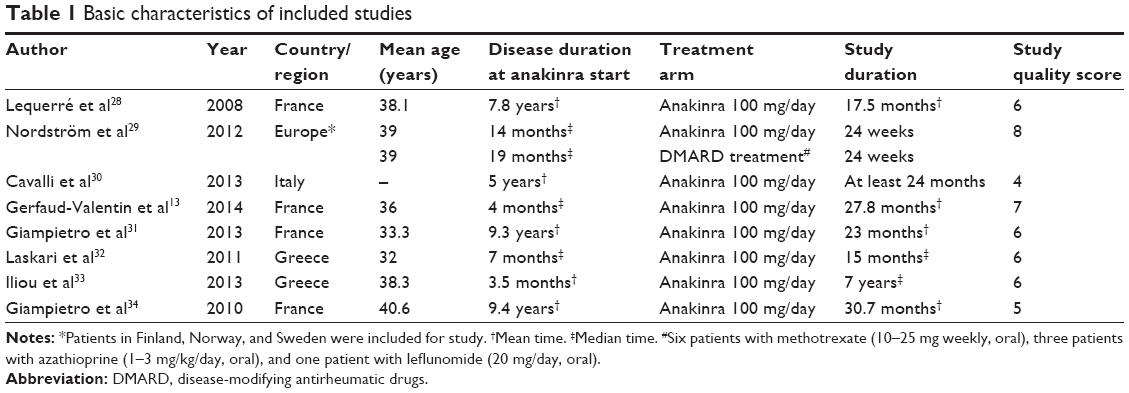 | Table 1 Basic characteristics of included studies |
We performed this meta-analysis in accordance with the guidelines of the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) Statement (Table S2).35
Efficacy of anakinra in AoSD patients
Eight studies,13,28–34 with a total of 134 subjects, investigated the effect of anakinra in AoSD remission. The remission rate at latest follow up was significantly increased in all studies, ranging from 50% to 100%. The highest remission rate was seen in the study by Iliou et al33 in which ten out of 44 patients (22.7%) were treated with anakinra, and a response was achieved in all of them. The complete remission rate ranged from 57% to 84%, and the highest complete remission rate was reported by Laskari et al32 who found a complete response for all disease-related symptoms (clinical and laboratory) within a median 3 months, in 80% of patients. Based on the data from these studies, the overall remission rate and complete remission rate of anakinra in AoSD patients were 81.66% (95% CI: 69.51%–89.69%) and 66.75% (95% CI: 56.94%–75.3%), respectively (Figure 2).
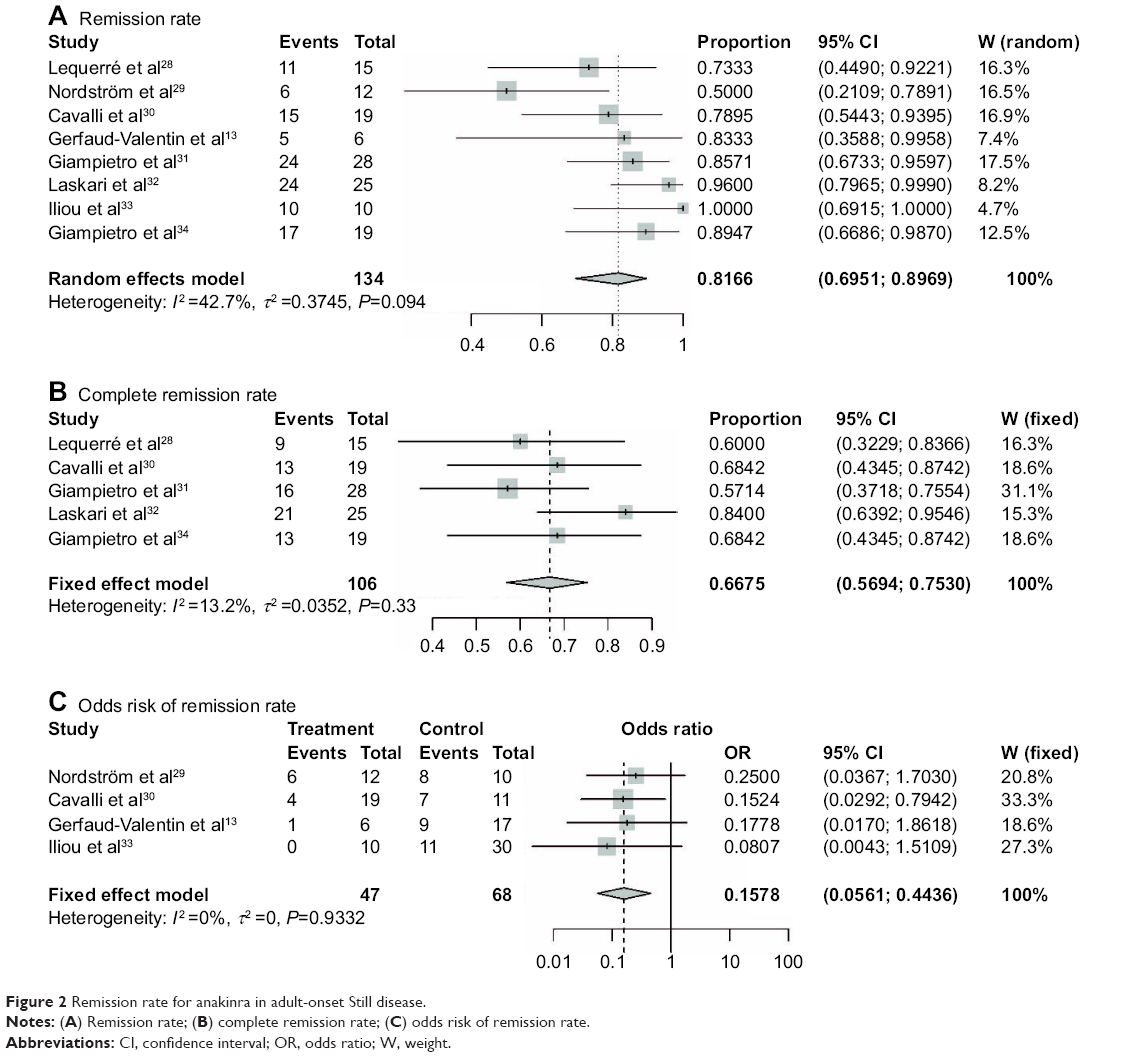 | Figure 2 Remission rate for anakinra in adult-onset Still disease. |
Of note, to investigate the specific contribution of anakinra to the AoSD and exclude the influence of confounding factors, we determined the OR of anakinra in AoSD patients. Figure 2 shows the forest plot for the four controlled studies13,29,30,33 that investigated the remission effect of anakinra in AoSD patients. As can be seen from this figure, the meta-analysis of these studies suggests that anakinra was associated with significant remission in AoSD when compared with controls (OR=0.16, 95% CI: 0.06–0.44, P=0.0005) (Figure 2), according to the fixed effects model.
Efficacy of anakinra as a steroid-sparing agent
Six studies,28–32,34 with a total of 105 subjects, showed the effect of anakinra as a steroid-sparing agent. The average dose of corticosteroid was reduced in the anakinra-treated patients of all six studies, although the exact values for the change between baseline and latest follow up were described just in two studies.
Two studies,28,31 showed the definite changes of corticosteroid dose from anakinra onset to latest follow up time, and the pooled analysis showed a significant reduction of the dosage of corticosteroid (mean difference =21.19 mg/day) (95% CI: 13.2–29.18, P<0.0001) (Figure 3). The cases of discontinued use of steroid was reported in three studies,28,29,32 and the overall frequency of discontinuance of oral corticosteroids was 36.9% (95% CI: 24.01%–51.98%) (Figure 3). The controlled trial by Nordström et al29 also showed that three patients on anakinra, but none on DMARD, were able to discontinue oral corticosteroids.
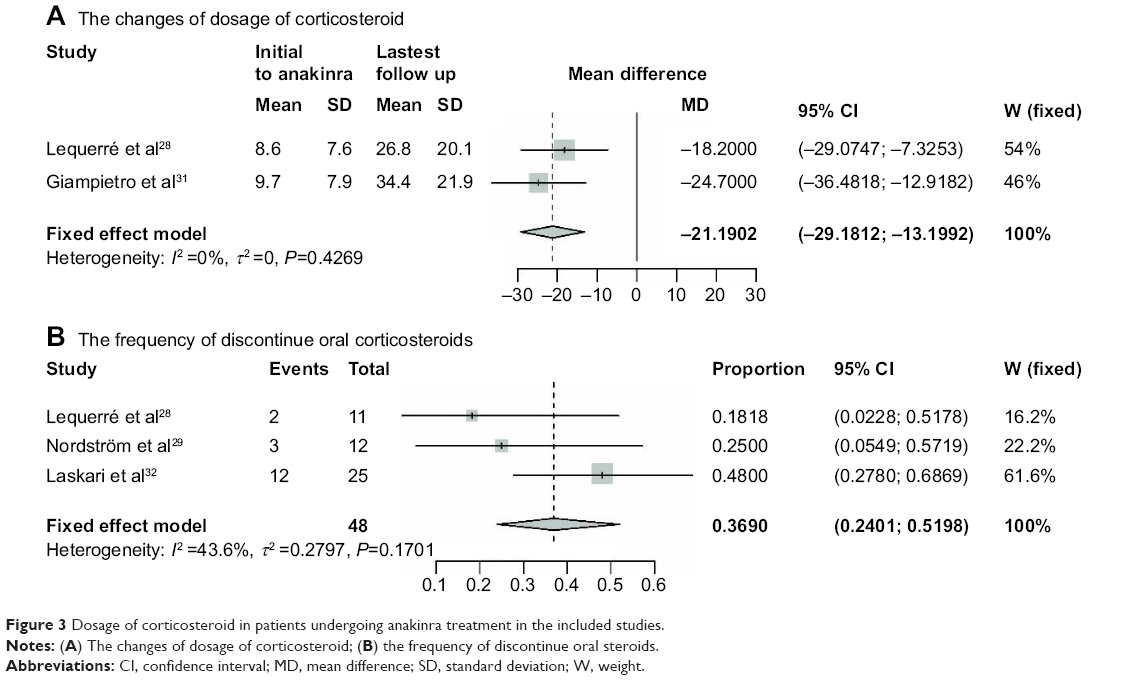 | Figure 3 Dosage of corticosteroid in patients undergoing anakinra treatment in the included studies. |
Efficacy of anakinra on clinical and laboratory parameters
Four studies28,29,31,32 investigated the changes of CRP, and the conclusion was consistent. The values of CRP were markedly declined over long duration of follow up in patients treated with anakinra (Table 2).
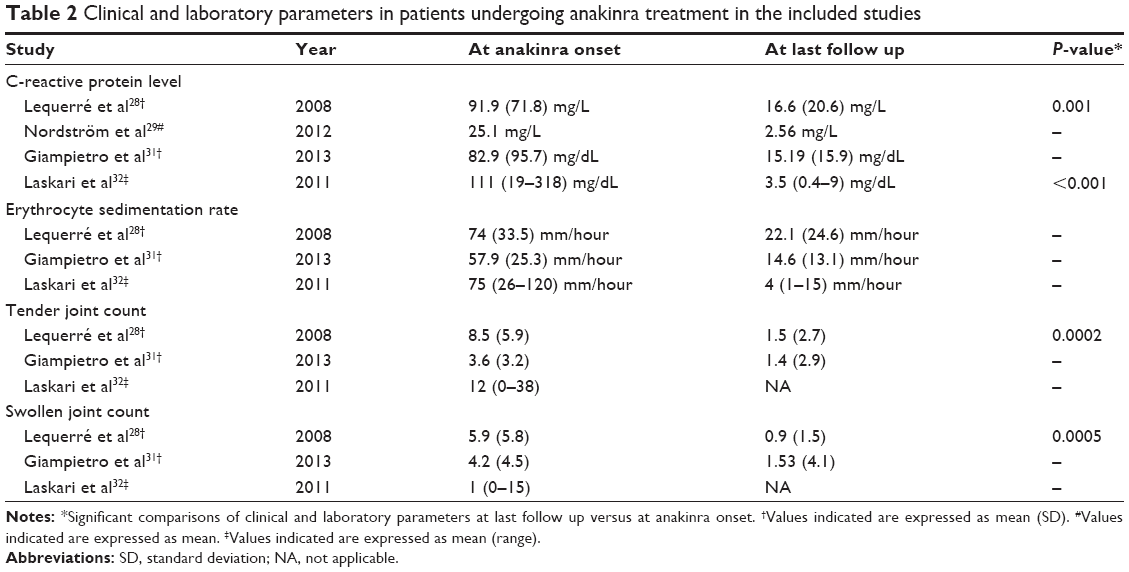 | Table 2 Clinical and laboratory parameters in patients undergoing anakinra treatment in the included studies |
Three studies28,31,32 have clear descriptions of the change in ESR in patients treated with anakinra. All three studies reported a diminution in the average value of ESR, from anakinra onset to latest follow up, and the greatest change was seen in an uncontrolled study in which the mean level of ESR was 75 mm/h at anakinra onset was decreased to 4 mm/h at the last visit (Table 2).
Three studies28,31,32 observed the effect of anakinra on arthritis symptoms (tender joint count [TJC] and swollen joint count [SJC]). Of these, three studies,28,31,32 with uncontrolled and open design, were able to demonstrate marked improvement in these parameters with anakinra for AoSD when values for the last visit were compared with those at anakinra onset. Compared with baseline, in a study by Lequerré et al28 the patients in the anakinra arm had statistically lower parameters of arthritis symptoms (P=0.0002 for TJC and P=0.0005 for SJC) (Table 2).
Safety of anakinra in AoSD patients
Five studies28,29,31,32,34 reported the adverse events related to anakinra use in AoSD patients, and showed it was well tolerated in all study populations. The mainly adverse event was skin rash in five subjects in three studies,28,31,34 which led to the withdrawal of anakinra. Three patients developed a severe urticarial reaction after the first treatment (one patient at 1.5 months and two patients at 3 months), leading to discontinued therapy.32 One open, randomized, and multicenter study29 noted that three patients had serious adverse events, the state of patients with AoSD worsened in two out of ten patients in the control (DMARD) group and only one out of 12 patients on anakinra.
The incidence of adverse events ranged from 5.26% to 13.33%, and the overall incidence was 9.54% (95% CI: 5.03%–17.36%) (Figure 4) according to pooled analysis.28,29,31,32,34 Further, we performed the pooled analysis to acquire the incidence of rash with anakinra in AoSD patients (proportion =8.56%) (95% CI: 3.60%–19.03%) (Figure 4).28,31,34
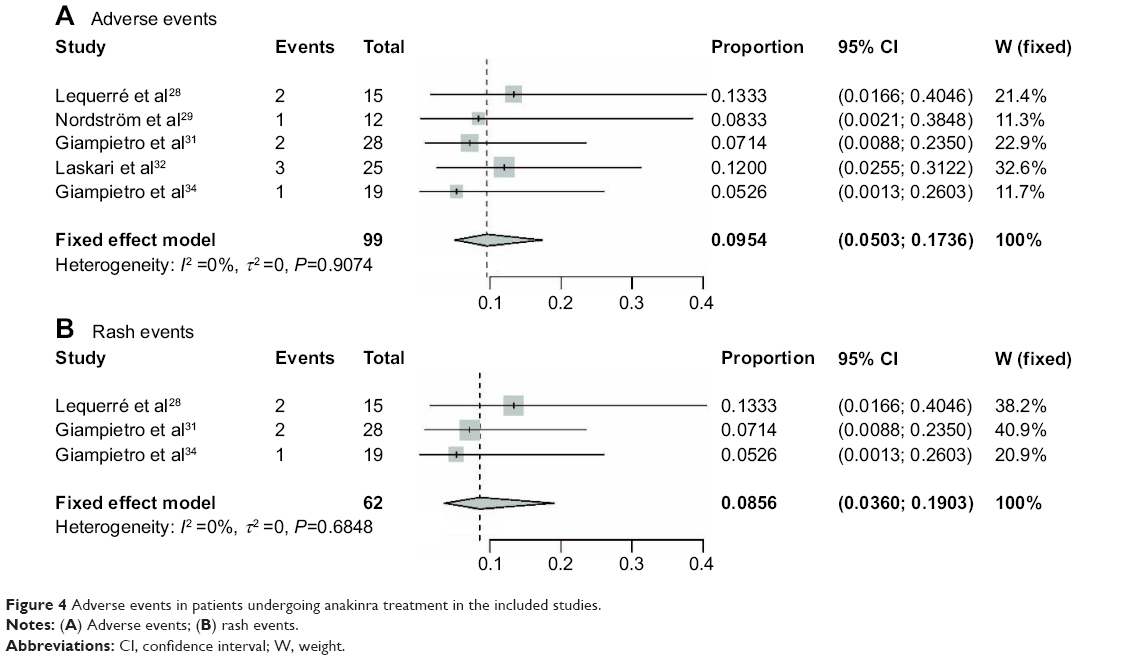 | Figure 4 Adverse events in patients undergoing anakinra treatment in the included studies. |
Publication bias
No significant evidence of publication bias was observed for the remission rates with anakinra in AoSD patients, in the analysis by funnel plot (Figure 5).
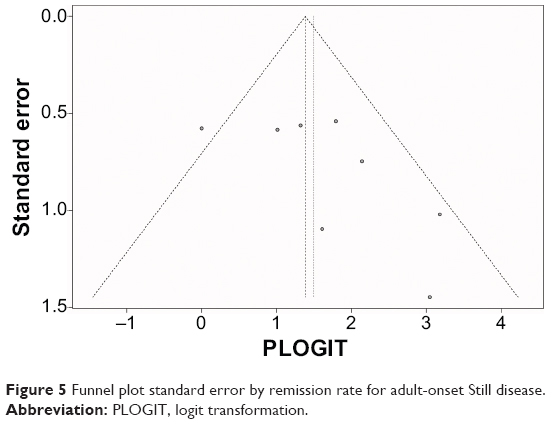 | Figure 5 Funnel plot standard error by remission rate for adult-onset Still disease. |
Discussion
The main objective of this meta-analysis was to evaluate the evidence for the use of anakinra in AoSD. The highest strength of clinical evidence comes from RCTs, but there is a lack of such high-strength trials explaining the effects of anakinra in AoSD. The reason for the absence of RCTs among patients with AoSD are challenges related to the disease, such as (1) the difficulty of identification and initial diagnosis of AoSD, which makes it difficult to conduct planned treatments; (2) the prevalence of the disease is rare, with an annual incidence of 0.16 cases per 100,000 people,36 leading to difficulty in recruiting sufficient numbers of patients; and (3) the heterogeneity of clinical symptoms. Hence, we strictly applied inclusion criteria to collect the data from clinical trials and included observational studies for the pooled analysis, to increase the clinical samples and to improve the statistical power of the findings, and provide more valuable and accurate insights into the treatment efficacy of anakinra in AoSD.
The pathophysiological processes underlying AoSD are not completely understood. The role of proinflammatory cytokines has been mentioned because high levels of IL-1, IL-6, and tumor necrosis factor (TNF)-α have been observed in patients with AoSD.37,38 In patients with AoSD, serum levels of IL-6 are raised and correlate with systemic symptoms, such as fever, hepatic dysfunction, and raised serum CRP levels.39,40 Tocilizumab, an IL-6 inhibiting agent, was found to control the disease activity in some patients with AoSD.41 IL-1, a cytokine inducing release of IL-6 and upstream molecules in the inflammatory cascade,42 may represent a suitable target for the treatment of AoSD.
The results of this pooled analysis suggest significant increases in remission rates among anakinra-treated patients. The remission rates included partial or complete remission. Partial remission was mainly defined as improvement in some related clinical or laboratory manifestations of AoSD, and complete remission was defined as the resolution of all clinical and biologic AoSD symptoms, under anakinra treatment.43,44 The remission rate is widely used in AoSD clinical trials owing to its importance to the prognostic evaluation of AoSD.9,45,46 A significant increase in the remission rate was reported by all the included studies, and we also found that anakinra significantly increased remission in AoSD when compared with controls. Some of the included studies31 also reported that patients who had previously failed to respond to conventional therapy with corticosteroids, NSAIDs, and DMARDs had a long-lasting remission of AoSD under anakinra treatment.
The steroid-sparing effect of anakinra was demonstrated in six of the included studies, and significant reduction was reached from anakinra onset to the latest follow up in two of them.28,31 Steroid is effective in controlling AoSD, and the response to steroid is often quick, within a couple of hours or a few days.47,48 However, steroid dependence easily occurs and can induce adverse events. According to Gerfaud-Valentin et al13 of 51 patients treated with steroids, 49 received them as a first- or second-line treatment, and 75% of patients developed various adverse events, such as Cushing syndrome (n=19), osteoporosis (n=8), aseptic osteonecrosis (n=5), corticosteroid-induced diabetes (n=4), high blood pressure (n=4), cataracts (n=3), psychiatric disorders (n=3), and infectious diseases (n=2). Furthermore, the steroid used in AoSD would increase the risk of infectious complications and of serious harm associated with long-term steroid treatment.49–51 Hence, reducing the dose of steroids used is beneficial for patient with AoSD.
Among the clinical and laboratory parameters, reduced CRP and ESR levels, and improved arthritis symptoms (TJC and SJC) have all been shown to relate with activity of disease, and these parameters are routinely used in clinical practice to monitor patients with AoSD.52,53 Patients with AoSD tend to have higher CRP and ESR levels, and arthritis damage symptoms, with higher TJC and SJC, compared with those without AoSD. Three of the included studies28,31,32 showed that anakinra could normalize the level of ESR and improve arthritis symptom parameters; four of the included studies28,29,31,32 showed that anakinra could normalize the level of CRP. Hence, on the base of available data, it is possible to conclude that anakinra is beneficial in improving clinical and laboratory parameters among patients with AoSD.
AoSD is associated with a higher risk of infection, and some AoSD treatment agents, such as corticosteroid,54 may be associated with an increased risk of infection, rather than a decreased risk of infection. In one recent study,55 9.8% AoSD patients in the long-term prednisone-treated group died because of pulmonary infection, and the mortality rate in this study was higher than that in other reports.29,33 Deaths in AoSD patients owing to infections were also reported by other studies.56,57 In all of the included studies, the adverse event of infection was not reported in any of patients treated with anakinra, and anakinra as initial therapy was not associated with increased the risk of infection in patients of AoSD. This meta-analysis showed that the main adverse event was skin rash, and according to Nordström et al29 anakinra-treated patients had a lower risk of infection than the control (DMARD) group. Hence, based on the existing data, anakinra was well tolerated in patients with AoSD.
Compared with other biologics, anakinra had higher remission rates with patients of AoSD. In study by Gerfaud-Valentin et al13 of 17 patients on other biologics, only eight (47%) had successful control of the disease; however, anakinra led to remission in five of six (83%) patients after a mean follow up of 27.8 months. In another study by Cavalli et al30 15 of 19 patients with AoSD responded to anakinra (79%), and only four of eleven patients responded to other biologics, including tocilizumab, etanercept, and adalimumab (36%).
Our meta-analysis strictly applied inclusion criteria to collect the relevant literature of AoSD patients treated with anakinra, and significant heterogeneity was not observed. However, some limitations did exist. First, as pointed out earlier, there was paucity of well-designed trials on the use of anakinra in patients with AoSD. The quality assessment of studies was indeed high, but the sample sizes in all included studies were small. Although some of included studies showed statistically significant results, these may not translate to clinical practice directly. Second, there were many case reports58–60 that described the effect of anakinra in patients with AoSD, and analysis of those report might have obtained other useful information, but we choose to exclude case reports due to their low strength of evidence. Third, the included studies were performed at various international institutions by different investigators and may have had some bias in reporting the types of result, suggesting publication and language bias may have existed. Finally, all eight studies included in the analysis were from Europe, and limitations related to environment and race may have existed.
Finally, despite these limitations, the present meta-analysis provides some clinical reference for the treatment of AoSD. Corticosteroids are the first-line treatment for rapid remission of relevant symptoms of AoSD; then, if manifestations of AoSD are improved, the dose of corticosteroid could be reduced, and anakinra, as second-line agent, could be introduced.
Conclusion
Our study has shown that anakinra is effective in remission of the manifestations of AoSD, with reduction of the dose of corticosteroid in patients with AoSD. Further, anakinra therapy was not associated with increased risk of adverse events in patients of AoSD and was well tolerated in patients with AoSD. Further research is still recommended to investigate these findings.
Acknowledgments
This work was supported by the National Natural Science Foundation of China (grant number 81100277), Zhejiang TCM KEY research fund projects (grant number 2013ZZ009 and 2013ZA078), and the Zhejiang Provincial Education Department Research Fund Project (grant number Y201225107).
Disclosure
The authors report no conflicts of interest in this work.
References
Kontzias A, Efthimiou P. Adult-onset Still’s disease: pathogenesis, clinical manifestations and therapeutic advances. Drugs. 2008;68(3):319–337. | ||
Gerfaud-Valentin M, Jamilloux Y, Iwaz J, Seve P. Adult-onset Still’s disease. Autoimmun Rev. 2014;13(7):708–722. | ||
Efthimiou P, Paik PK, Bielory L. Diagnosis and management of adult onset Still’s disease. Ann Rheum Dis. 2006;65(5):564–572. | ||
Pay S, Türkçapar N, Kalyoncu M, et al; Ankara Rheumatology Study Group. A multicenter study of patients with adult-onset Still’s disease compared with systemic juvenile idiopathic arthritis. Clin Rheumatol. 2006;25(5):639–644. | ||
Franchini S, Dagna L, Salvo F, Aiello P, Baldissera E, Sabbadini MG. Efficacy of traditional and biologic agents in different clinical phenotypes of adult-onset Still’s disease. Arthritis Rheum. 2010;62(8):2530–2535. | ||
Kim HA, Sung JM, Suh CH. Therapeutic responses and prognosis in adult-onset Still’s disease. Rheumatol Int. 2012;32(5):1291–1298. | ||
Krzossok S, Benck U, van der Woude FJ, Braun C. [Disseminated intravascular coagulation, perimyocarditis and bilateral pleural empyema in adult Still’s disease]. Dtsch Med Wochenschr. 2004;129(47):2535–2537. German. | ||
Hot A, Toh ML, Coppéré B, et al. Reactive hemophagocytic syndrome in adult-onset Still disease: clinical features and long-term outcome: a case-control study of 8 patients. Medicine (Baltimore). 2010;89(1):37–46. | ||
Fautrel B, Borget C, Rozenberg S, et al. Corticosteroid sparing effect of low dose methotrexate treatment in adult Still’s disease. J Rheumatol. 1999;26(2):373–378. | ||
Nagashima T, Iwamoto M, Matsumoto K, Minota S. Interleukin-18 in adult-onset Still’s disease: treatment target or disease activity indicator? Intern Med. 2012;51(4):449; author reply 451. | ||
Kato T, Kobayashi T, Nishino H, Hidaka Y. Double-filtration plasmapheresis for resolution of corticosteroid resistant adult onset Still’s disease. Clin Rheumatol. 2006;25(4):579–582. | ||
Yip CMS, Lee TL, Chan HB, Lau YL. Macrophage activation syndrome after initiation of corticosteroid and etanercept in a patient with adult onset Still’s disease. HK J Paediatr. 2008;13(3):174–179. | ||
Gerfaud-Valentin M, Maucort-Boulch D, Hot A, et al. Adult-onset still disease: manifestations, treatment, outcome, and prognostic factors in 57 patients. Medicine (Baltimore). 2014;93(2):91–99. | ||
Kötter I, Wacker A, Koch S, et al. Anakinra in patients with treatment-resistant adult-onset Still’s disease: four case reports with serial cytokine measurements and a review of the literature. Semin Arthritis Rheum. 2007;37(3):189–197. | ||
Raffeiner B, Botsios C, Dinarello C, Ometto F, Punzi L, Ramonda R. Adult-onset Still’s disease with myocarditis successfully treated with the interleukin-1 receptor antagonist anakinra. Joint Bone Spine. 2011;78(1):100–101. | ||
Hoshino T, Ohta A, Yang D, et al. Elevated serum interleukin 6, interferon-gamma, and tumor necrosis factor-alpha levels in patients with adult Still’s disease. J Rheumatol. 1998;25(2):396–398. | ||
Giampietro C, Fautrel B. Anti-interleukin-1 agents in adult onset Still’s disease. Int J Inflam. 2012;2012:317820. | ||
Rudinskaya A, Trock DH. Successful treatment of a patient with refractory adult-onset still disease with anakinra. J Clin Rheumatol. 2003;9(5):330–332. | ||
Fleischmann RM, Schechtman J, Bennett R, et al. Anakinra, a recombinant human interleukin-1 receptor antagonist (r-metHuIL-1ra), in patients with rheumatoid arthritis: A large, international, multicenter, placebo-controlled trial. Arthritis Rheum. 2003;48(4):927–934. | ||
Kalliolias GD, Georgiou PE, Antonopoulos IA, Andonopoulos AP, Liossis SN. Anakinra treatment in patients with adult-onset Still’s disease is fast, effective, safe and steroid sparing: experience from an uncontrolled trial. Ann Rheum Dis. 2007;66(6):842–843. | ||
Cush JJ, Medsger TA, Christy WC, Herbert DC, Cooperstein LA. Adult-onset Still’s disease. Clinical course and outcome. Arthritis Rheum. 1987;30(2):186–194. | ||
Yamaguchi M, Ohta A, Tsunematsu T, et al. Preliminary criteria for classification of adult Still’s disease. J Rheumatol. 1992;19(3):424–430. | ||
Fautrel B, Zing E, Golmard JL, et al. Proposal for a new set of classification criteria for adult-onset still disease. Medicine (Baltimore). 2002;81(3):194–200. | ||
Singal AK, Fontana RJ. Meta-analysis: oral anti-viral agents in adults with decompensated hepatitis B virus cirrhosis. Aliment Pharmacol Ther. 2012;35(6):674–689. | ||
Singal AK, Salameh H, Kuo YF, Fontana RJ. Meta-analysis: the impact of oral anti-viral agents on the incidence of hepatocellular carcinoma in chronic hepatitis B. Aliment Pharmacol Ther. 2013;38(2):98–106. | ||
Zintzaras E, Ioannidis JP. Heterogeneity testing in meta-analysis of genome searches. Genet Epidemiol. 2005;28(2):123–137. | ||
Higgins JPT, Green S, editors. Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0. Oxford: The Cochrane Collaboration; 2011 [updated March 2011]. Available from: www.cochrane-handbook.org. Accessed October 8, 2014. | ||
Lequerré T, Quartier P, Rosellini D, et al; Société Francophone pour la Rhumatologie et les Maladies Inflammatoires en Pédiatrie (SOFREMIP); Club Rhumatismes et Inflammation (CRI). Interleukin-1 receptor antagonist (anakinra) treatment in patients with systemic-onset juvenile idiopathic arthritis or adult onset Still disease: preliminary experience in France. Ann Rheum Dis. 2008;67(3):302–308. | ||
Nordström D, Knight A, Luukkainen R, et al. Beneficial effect of interleukin 1 inhibition with anakinra in adult-onset Still’s disease. An open, randomized, multicenter study. J Rheumatol. 2012;39(10):2008–2011. | ||
Cavalli G, Franchini S, Berti A, et al. Efficacy and safety of biologic agents in adult-onset Still’s disease: A long-term follow-up of 19 patients at a single referral center [abstract]. Arthritis Rheum. 2013;65 Suppl 10:S2028. | ||
Giampietro C, Ridene M, Lequerre T, et al; CRI (Club Rhumatismes et Inflammation). Anakinra in adult-onset Still’s disease: long-term treatment in patients resistant to conventional therapy. Arthritis Care Res (Hoboken). 2013;65(5):822–826. | ||
Laskari K, Tzioufas AG, Moutsopoulos HM. Efficacy and long-term follow-up of IL-1R inhibitor anakinra in adults with Still’s disease: a case-series study. Arthritis Res Ther. 2011;13(3):R91. | ||
Iliou C, Papagoras C, Tsifetaki N, Voulgari PV, Drosos AA. Adult-onset Still’s disease: clinical, serological and therapeutic considerations. Clin Exp Rheumatol. 2013;31(1):47–52. | ||
Giampietro C, Ridene M, Fautrel B, Bourgeois P. Long term treatment with anakinra in patients with adult-onset Still disease [abstract]. Arthritis Rheum. 2010;62 Suppl 10:S902. | ||
Moher D, Liberati A, Tetzlaff J, Altman DG; PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. J Clin Epidemiol. 2009;62(10):1006–1012. | ||
Magadur-Joly G, Billaud E, Barrier JH, et al. Epidemiology of adult Still’s disease: estimate of the incidence by a retrospective study in west France. Ann Rheum Dis. 1995;54(7):587–590. | ||
Choi JH, Suh CH, Lee YM, et al. Serum cytokine profiles in patients with adult onset Still’s disease. J Rheumatol. 2003;30(11):2422–2427. | ||
Chen DY, Lan JL, Lin FJ, Hsieh TY. Proinflammatory cytokine profiles in sera and pathological tissues of patients with active untreated adult onset Still’s disease. J Rheumatol. 2004;31(11):2189–2198. | ||
Fautrel B. Adult-onset Still disease. Best Pract Res Clin Rheumatol. 2008;22(5):773–792. | ||
Sekkach Y, Elqatni M, Khattabi AE, et al. [Antagonists of interleukin-6 (tocilizumab), in adult refractory still disease]. Presse Med. 2011;40(7–8):e333–e337. French. | ||
Rech J, Ronneberger M, Englbrecht M, et al. Successful treatment of adult-onset Still’s disease refractory to TNF and IL-1 blockade by IL-6 receptor blockade. Ann Rheum Dis. 2011;70(2):390–392. | ||
Tsakiri N, Kimber I, Rothwell NJ, Pinteaux E. Interleukin-1-induced interleukin-6 synthesis is mediated by the neutral sphingomyelinase/Src kinase pathway in neurones. Br J Pharmacol. 2008;153(4):775–783. | ||
Kim YJ, Koo BS, Kim YG, Lee CK, Yoo B. Clinical features and prognosis in 82 patients with adult-onset Still’s disease. Clin Exp Rheumatol. 2014;32(1):28–33. | ||
Kong XD, Xu D, Zhang W, Zhao Y, Zeng X, Zhang F. Clinical features and prognosis in adult-onset Still’s disease: a study of 104 cases. Clin Rheumatol. 2010;29(9):1015–1019. | ||
Jung KH, Kim JJ, Lee JS, et al. Interleukin-18 as an efficient marker for remission and follow-up in patients with inactive adult-onset Still’s disease. Scand J Rheumatol. 2014;43(2):162–169. | ||
Fujii T, Akizuki M, Kameda H, et al. Methotrexate treatment in patients with adult onset Still’s disease – retrospective study of 13 Japanese cases. Ann Rheum Dis. 1997;56(2):144–148. | ||
Ghosal A, Pal RB, Das SK, Das T. An unusual presentation of adult onset Still’s disease. Med J Malaysia. 2012;67(5):532–533. | ||
Lim E, Chng HH. Adult-onset Still’s disease in an oriental population: manifestations, course and outcome in 16 patients. Ann Acad Med Singapore. 1998;27(1):11–15. | ||
Yeh HM, Liu MF, Chang KK, Liu SM, Chen CH. Adult-onset Still’s disease complicated with hemophagocytic syndrome. J Formos Med Assoc. 2010;109(1):85–88. | ||
Scholtze D, Varga Z, Imhof A. Post-infection immunocomplex glomerulonephritis and Legionnaires’ disease in a patient with adult Still’s disease during treatment with interleukin 1 receptor antagonist anakinra: a case report. J Med Case Rep. 2011;5:299. | ||
Izumikawa K, Morinaga Y, Kondo A, et al. Adult Still’s disease associated with cytomegalovirus infection. J Infect Chemother. 2007;13(2):114–117. | ||
Puéchal X, DeBandt M, Berthelot JM, et al; Club Rhumatismes Et Inflammation. Tocilizumab in refractory adult Still’s disease. Arthritis Care Res (Hoboken). 2011;63(1):155–159. | ||
Hu Q, Yan Z, Zhong J. Adult-onset Still’s disease: how to make a diagnosis in an atypical case. Rheumatol Int. 2012;32(10):3299–3302. | ||
Menge F, Schacherer C, Wigand R, Brodt R, Caspary WF, Stein J. [Adult-onset Still’s disease. Differential diagnosis in recurrent pharyngitis, fever of unknown original and excessive hyperferritinemia]. Dtsch Med Wochenschr. 1999;124(27):829–832. German. | ||
Zeng T, Zou YQ, Wu MF, Yang CD. Clinical features and prognosis of adult-onset still’s disease: 61 cases from China. J Rheumatol. 2009;36(5):1026–1031. | ||
Ohta A, Yamaguchi M, Tsunematsu T, et al. Adult Still’s disease: a multicenter survey of Japanese patients. J Rheumatol. 1990;17(8):1058–1063. | ||
Michel M, Hayem G, Rat AC, et al. [Fatal infectious complications in 2 patients with adult onset Still disease]. Rev Med Interne. 1996;17(5):407–409. French. | ||
Assimakopoulos SF, Karamouzos V, Papakonstantinou C, Zolota V, Labropoulou-Karatza C, Gogos C. Granulomas formation in lymph nodes, liver and spleen in adult-onset Still’s disease: A case report. J Clin Med Res. 2013;5(2):144–149. | ||
Assimakopoulos SF, Karamouzos V, Papakonstantinou C, Zolota V, Labropoulou-Karatza C, Gogos C. Suppurative necrotizing granulomatous lymphadenitis in adult-onset Still’s disease: a case report. J Med Case Rep. 2012;6:354. | ||
Guignard S, Dien G, Dougados M. Severe systemic inflammatory response syndrome in a patient with adult onset Still’s disease treated with the anti-IL1 drug anakinra: a case report. Clin Exp Rheumatol. 2007;25(5):758–759. |
Supplementary materials
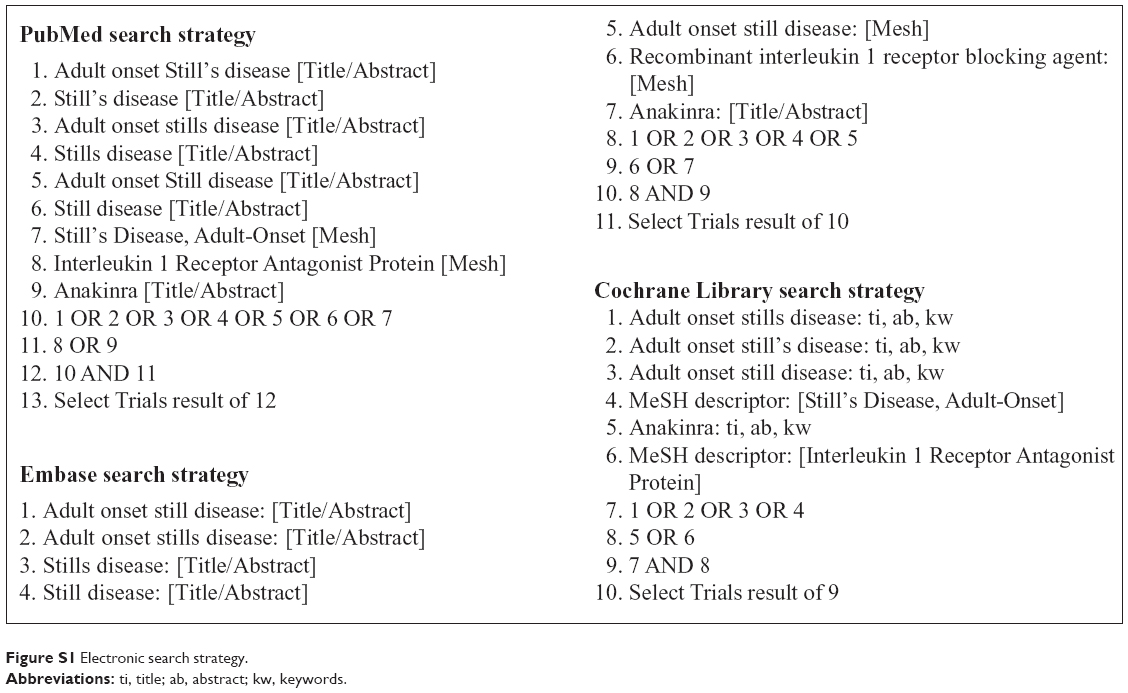 | Figure S1 Electronic search strategy. |
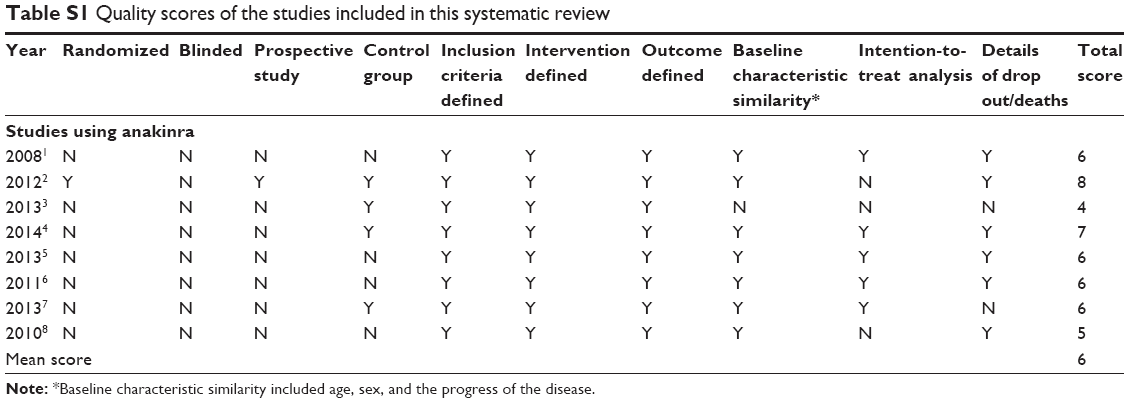 | Table S1 Quality scores of the studies included in this systematic review |
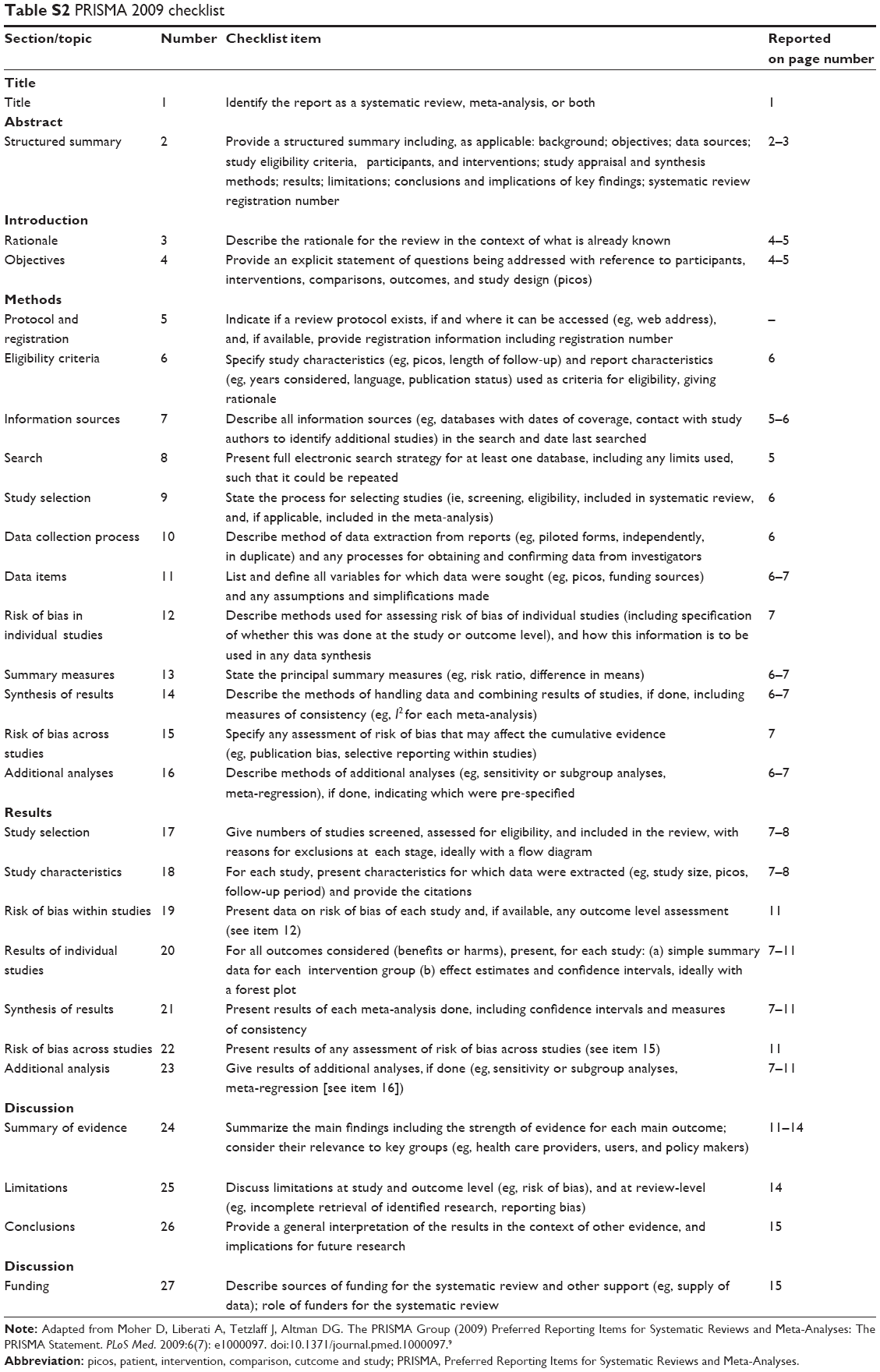 | Table S2 PRISMA 2009 checklist |
References
Lequerré T, Quartier P, Rosellini D, et al; Société Francophone pour la Rhumatologie et les Maladies Inflammatoires en Pédiatrie (SOFREMIP); Club Rhumatismes et Inflammation (CRI). Interleukin-1 receptor antagonist (anakinra) treatment in patients with systemic-onset juvenile idiopathic arthritis or adult onset Still disease: preliminary experience in France. Ann Rheum Dis. 2008;67(3):302–308. | ||
Nordström D, Knight A, Luukkainen R, et al. Beneficial effect of interleukin 1 inhibition with anakinra in adult-onset Still’s disease. An open, randomized, multicenter study. J Rheumatol. 2012;39(10):2008–2011. | ||
Cavalli G, Franchini S, Berti A, et al. Efficacy and safety of biologic agents in adult-onset Still’s disease: A long-term follow-up of 19 patients at a single referral center [abstract]. Arthritis Rheum. 2013;65 Suppl 10:S2028. | ||
Gerfaud-Valentin M, Maucort-Boulch D, Hot A, et al. Adult-onset still disease: manifestations, treatment, outcome, and prognostic factors in 57 patients. Medicine (Baltimore). 2014;93(2):91–99. | ||
Giampietro C, Ridene M, Lequerre T, et al; CRI (Club Rhumatismes et Inflammation). Anakinra in adult-onset Still’s disease: long-term treatment in patients resistant to conventional therapy. Arthritis Care Res (Hoboken). 2013;65(5):822–826. | ||
Laskari K, Tzioufas AG, Moutsopoulos HM. Efficacy and long-term follow-up of IL-1R inhibitor anakinra in adults with Still’s disease: a case-series study. Arthritis Res Ther. 2011;13(3):R91. | ||
Iliou C, Papagoras C, Tsifetaki N, Voulgari PV, Drosos AA. Adult-onset Still’s disease: clinical, serological and therapeutic considerations. Clin Exp Rheumatol. 2013;31(1):47–52. | ||
Giampietro C, Ridene M, Fautrel B, Bourgeois P. Long term treatment with anakinra in patients with adult-onset Still disease [abstract]. Arthritis Rheum. 2010;62 Suppl 10:S902. | ||
Moher D, Liberati A, Tetzlaff J, Altman DG. The PRISMA Group (2009) Preferred Reporting Items for Systematic Reviews and Meta-Analyses: The PRISMA Statement. PLoS Med. 2009:6(7): e1000097. doi:10.1371/journal.pmed.1000097. |
 © 2014 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2014 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.