")
Back to Journals » Patient Preference and Adherence » Volume 16
Intention to Use and Predictors of Use of Maternity Waiting Home among Pregnant Women in Hargeisa City Health Centers, Somaliland
Authors Aden M, Azale T, Tadie C
Received 12 March 2022
Accepted for publication 20 June 2022
Published 30 June 2022 Volume 2022:16 Pages 1595—1603
DOI https://doi.org/10.2147/PPA.S358952
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Johnny Chen
Mohamed Aden,1 Telake Azale,2 Chalie Tadie3
1Ministry of Plan and National Development, Hargeisa, Somaliland; 2Department of Health Education and Behavioral Sciences, College of Medicine and Health Sciences, University of Gondar, Gondar, Ethiopia; 3Department of Health Systems and Policy, College of Medicine and Health Sciences, University of Gondar, Gondar, Ethiopia
Correspondence: Telake Azale, Email [email protected]
Background: Maternity waiting homes (MWHs) can help women receive the necessary obstetric care and referral if needed. However, there is a lack of evidence on whether women have the desire to stay away from their homes and the sociocultural predictors of their decision in Somaliland.
Objective: The purpose of this study was to measure predictors of the intention of women to stay in MWHs using the theory of planned behavior in Hargeisa city, Somaliland.
Methods: A facility-based cross-sectional study was conducted from in April 2021 in Hargeisa health facilities among 422 randomly selected participants using an interviewer-administered and structured questionnaire. Data were transferred to Epi Data 4.6 and exported to SPSS 20 for further analysis. Descriptive, bivariate, and multivariate binary logistic regression analyses were used. ORs with 95% CIs were used to assess associations, and statistical significance was set at P< 0.05.
Results: A total of 245 (58%, 95% CI 53.1%– 62.8%) pregnant women intended to use an MWH. Multivariate analysis revealed that education (AOR 5.40, 95% CI 3.01– 9.69), experience of using an MWH (AOR 3.80, 95% CI 2.32– 6.27), multigravidity (AOR 2.2, 95% CI 1.16– 4.29), subjective norms (AOR 1.8, 95% CI 1.05– 3.11), indirect attitudes toward use of MWHs (AOR 1.9, 95% CI 1.01– 3.92), and indirect subjective norms (AOR 2.0, 95% CI 1.16– 3.60) were significantly associated with intention to use an MWH.
Conclusion: Using an MWH is not the preference of many women. Personal characteristics, such as education, multigravidity, and perceived social pressure are important predictors of intention to use MWHs. It is important to raise the awareness of women and the community about the benefits of using MWHs in the early management of obstetric complications.
Keywords: maternity waiting home, intention, Somaliland, pregnant women, theory
Introduction
Following the implementation of the Millennium Development Goals, deaths of mothers as a result of pregnancy and childbirth complications globally has decreased by >35%. However, there are still >800 deaths per day as a result of pregnancy and childbirth complications.1 Low- and middle-income countries account for about 94% of these deaths.2 Excess and preventable deaths in low-resource settings is a reflection of the huge gap in health-service access and capacity between poor and rich countries.3 Women in low-resource settings have more pregnancies than women in rich countries.3 The more pregnancies a woman has, the more likely that she will develop complications related to pregnancy and childbirth.2 The maternal mortality ratio is 230 per 100,000 live births in developing countries, whereas in developed countries it is only 16 per 100,000 live births.4 Just two WHO regions account about 86% of maternal deaths (sub-Saharan Africa 62% and South Asia 24%).2
The three delays — delay in decision-making, delay in seeking care, and delay in receiving treatment — are the main causes of maternal mortality.5–7 The adoption of maternity waiting homes (MWHs) by the WHO was intended to reduce diseases and deaths among mothers and children through prevention of delays in reaching a health facility. The use of MWHs improves access to health care for pregnant and postpartum women and helps them get information to help them plan the place of delivery from health-care providers, as well as education about child immunization.8–13 MWH living facilities are situated nearby health institutions, and are designed for pregnant women to stay in during the final days of their pregnancy, creating access to obstetric care, especially for women in rural settings.8,14,15
The introduction of MWHs has enabled a significant reduction in deaths of women and neonates and the prevention of stillbirth in the African continent.16 For example, in Nigeria the use of institutional delivery has increased due to the initiation of MWHs. Moreover, the death of women and the stillbirth rate have decreased by 90% and 85%, respectively.16 There has also been a reduction in deaths of women by half as a result of MWHs in Uganda.12 The establishment of MWHs has increased the use of institutional delivery to about 50% in Eritrea. With the adoption of MWHs, there have been reductions in deaths of women and neonates and improved use of antenatal care (ANC) and institutional delivery services in many African countries, such as Zimbabwe, Tanzania, Ghana, Malawi, and Zambia.8,12,17–19
After the introduction of MWHs in Ethiopia, improvement in the health of women was notable. Women who stayed in MWHs had much-improved stillbirth rates compared to those who didn't use MWHs (17.6 per 1,000 live births versus 191 per 1,000 births).20,21 Maternal mortality rates are among the highest in Somaliland. A recent estimate of the maternal mortality ratio was about 1,000 per 100,000 live births in Somaliland according to the 2011 Multi-Indicator Cluster Survey.22 The adoption of MWHs has improved maternal health services in many African countries. However, coverage for ANC, facility delivery, and postnatal care remain very low.
There are several factors influencing the decision of women to use MWHs. One of these is women's autonomy in household decision-making as reported in a Kenyan study, where women had to get permission from their husbands to stay in MWHs, and subsequently very few women used them.23 This also applies for many African countries, including Zambia, Ghana, Nigeria, Malawi, Zimbabwe, and Eritrea. Other factors include financial constraints, poor support from family, social support, unfavorable attitudes toward health professionals, fear of increased cost, sociocultural discouragement, and preference for home delivery.8,12,24,25
Somaliland's Ministry of Health has targeted a 75% reduction in maternal death and increasing institutional delivery by 60%. Although the government is trying a lot to improve maternal health, there has been no change in the indices of diseases and deaths of women in the past 5 years.22,26 Moreover, maternal mortality is the third highest in the world. According to a 2020 Central Statistics Department report, the maternal mortality ratio was 396 per 100,000 live births.27 There has been little research on the preferences of women for place of birth in Somaliland.
Intention is believed to be the best and most proximal predictor of behavior.28 The intention of mothers to stay in MWHs is thus an important predictor of use of the service. Accordingly, studies have shown that many pregnant women intended to use MWHs.14,25,29,30 In rural Zambia, 98% of mothers from heath facilities with MWHs showed more interest in using or staying at MWHs than centers without MWHs.25,31 A survey conducted in Kenya showed that more than half (61.1%) the women said that they would stay at MWHs.32 In Zimbabwe, about 65% of women said they were willing to stay in MWHs.12
Studies from southwest Ethiopia have shown that a majority of pregnant women intended to use MWHs in their last week of pregnancy and deliver at a health institution.14,33 However, a nationally representative study in four regions of Ethiopia — Southern Nations, Nationalities, and Peoples’, Amhara, Tigray, and Oromia — reported that about 17% of pregnant women had intentions to stay in MWHs only for postnatal care.34 Few women use them. A Ghanaian study conducted in the same year that MWHs were initiated showed that only one in four spent a single night at an MWH.35 In Kenya, only ten who delivered at a health facility stayed in an MWH.23
Use of Theory of Planned Behavior as Predictor of Intention
The theory of planned behavior developed by Ajzen in 1988 measures intention.36 This theory uses belief, attitude, norm, and control variables that are widely reported to have shown important associations between intention and behavior.28,36 Individual characteristics, including age, sex, education, and health literacy, impact intention through their influence on its precedents.37 Attitudes toward behavior, subjective norms, and perceived behavioral control are major and direct predictors of intention, which directly determines behavior.
Younger women are more likely to have the intention to use MWHs.25,38 Maternal education is a significant predictor of MWH use.6 Ethiopian studies have reported that pregnant women and their husbands with secondary or higher education level use MWHs.33,39 More ANC visits and knowledge of danger signs in pregnancy have been reported as predictors of MWH use in African studies.12,25 Women with a history of cesarean section, any complications during previous delivery or with current high-risk pregnancy symptoms like blurring of vision, severe headaches, or vaginal bleeding generally intented to use MWHs.12,17,23,39 Having experienced complications during past delivery has been found to be an important predictor of MWH use in Ethiopia.21,33 Previous use of facility delivery14,25,33 and MWHs have been reported to positively influence the decision to use MWHs.25
There is a strong association between attitudes and behavior.14,30,40 Women from health facilities with MWHs had more favorable attitudes toward MWH use than those with health facilities without MWHss.18,25 Attitude is an important predictor of behavior through intention. Despite many challenges, high-intention mothers had more positive attitudes toward health workers and maternal health services than low-intention mothers.29 According to Ajzen, the second predictor of behavioral intention is subjective norms. These are beliefs that persons that are close to the individual would approve of his/her behavior and the individual's motivation to comply with whatever their significant others think.28,36
Many studies have reported that important referent individuals’ approval or disapproval, eg, husbands, community leaders, health-development leaders, stakeholders, health workers, traditional birth attendants, and mothers–in-law, was key to using or not using MWHs.14,17,23,25,29,34,41 Studies from Kenya and Zambia have reported that the decision of whether a pregnant woman should use an MWH or not is made by her husband.17,23,25,42 In addition, for younger mothers, in-laws have a major role in making the decision. However, older mothers would be more autonomous in household decision-making. and no one could make the decision on her behalf to stay at MWHs or place of delivery.17,41
Perceived behavioral control is the perception of an individual in his/her capacity to carry out a certain course of action.36 Pregnant mothers' perceived behavioral control is predicted by their belief in the presence of barriers to and facilitators of the desired behavior. These facilitators and barriers include food security, transport access, and the presence or absence of caregivers and family members while in the MWH, weighted by their perceived power or the impact of each control factors to facilitate or inhibit the behavior.28,36 There is little evidence on intention to stay at an MWH in Somaliland. The currents study's objective was to measure the willingness of pregnant mothers to stay at MWHs in Hargeisa health facilities and the predictors of this.
Methods
We conducted an institution-based cross-sectional study in Hargeisa between April 4 and May 2, 2021. The city has one general hospital (public), one TB general hospital, eight public health centers that provide MWH services, and seven private hospitals.43 Women with ANC follow-up at the health centers of Hargeisa were included in the study.
Sampling
We recruited 422 pregnant women from the eight public health centers providing MWH services. We selected every seventh women using systematic sampling, considering the total number of pregnant women attending ANC to be 3,280.
Measurements
Pregnant mothers' intention to stay at MWHs was measured using the constructs of the theory of planned behavior. It was measured by four questions on a two-point Likert scale. Other constructs, such as subjective norms, attitudes, and perceived behavioral control were used as predictors of intention, along with demographic and obstetric factors. Attitudes toward MWHs were measured by four items with five-point Likert scales and dichotomized as favorable and unfavorable.26 Subjective norms were measured by four items with five response categories rated as likely or unlikely.34 Perceived behavioral control was assessed using four items with five responses, then rated into two categories: confident or not confident.10,26
Data Collection
We collected the data through face-to–face interviews using a questionnaire that had been tested and standardized. The questionnaire included demographics, obstetric characteristics, and theory of planned behavior–based questions. The response variable was intention to use an MWH in the last weeks of the index pregnancy. The theory of planned–behavior constructs had 52 specific questions in total.14,28 We prepared the questionnaire in English, then then it was translated into Somalian by native speakers who also were fluent in English. There was also a reverse translation by other experts into the source language, English. We recruited six female nurses with diplomas who were trained for data collection. The supervisors were two male nurses. Data collectors and supervisors received 2 days’ training that focused on the interview instrument and ethical principles.
Data Analysis
We used Epi Data 4.6 for data entry and coding. We the data were exported and analyzed using SPSS 20. Bivariate and multivariate binary logistic regression analyses were carried out. The constructs of the theory of planned behavior were separately measured as subdomains and predictors of intention, which was the outcome variable. Predictor variables with P<0.25 were fitted into the final model. The variance-inflation factor (VIF) was used to check if there were mulicollinearities among the independent variables. Its value in this study was 1.2, implying no multicollinearity. The Hosmer–Lemeshow goodness-of-fit test was used to check model fitness, resulting in P=0.897, indicates that the model was a good fit. Strengths of association between outcome and predictors were determined by ORs, and 95% CIs, with P<0.05 indicating statistical significance.
Results
Sociodemographics
All the 422 participants took the interview. Mean age was 30±7.76 years. A total of 133 (31.5%) were aged 20–29 years. Two-thirds (278, 6%) had had a formal education. Almost all (416, 98.6%) were married. In sum, 181 (42.9%) had a monthly family income of US$101–150 (Table 1).
 |
Table 1 Sociodemographics of participants (n=422) |
About three-quarters (302, 74.5%) of the study participants had had their last child at a health institution. A total of 166 (39%) had had two or more ANC visits, 178 (42%) had used an MWH, and 361 (86%) had favorable attitudes toward MWHs. Regarding subjective norms, 277 (66%) respondents believed that their significant others would approve of their use of MWHs. For perceived behavioral control, 74% were confident that they would use MWHs.
A total of 268 (64%) of the respondents agreed that staying at an MWH would enable them to receive skilled birth attendance and prevent pregnancy- and childbirth-related complications. Outcome evaluation revealed that 255 (60%) agreed that it was important to stay at an MWH so as to safely deliver and to have a healthy baby. In sum, 255 (60.4%) women believed that the HEWs would encourage them to use an MWH. Only 85 (20%) confirmed that their husbands should approve if they were to use MWHs.
Slightly less than two-thirds (61%) of participants said a shortage of food would impair their decision to use MWHs, while 179 (43%) expressed uncertainty about the presence of support from the family in terms of accompanying them to the shelter and that this would hinder their use. We found that 222 (53%) respondents were confident in using an MWH if they were had enough food, while 236 (69%) supported the idea of using MWHs if they had someone at home caring for the rest of the family.
Intention of to Stay at MWHs
About six in ten (245, 58%, 95% CI 53.1–62.8) participants had the intention to use MWHs.
Predictors of Intention to Stay at MWHs
Multivariate analysis revealed that education, history of MWH use, gravidity, subjective norms, both direct and indirect, and indirect attitudes were statistically significantly associated with intention to use MWHs. The final model was fitted to explain the independent factors associated with intention to use MWHs in the study setting, and Hosmer and Lemeshow goodness of fit showed P=0.897. Those with a formal education had 5.4 times the odds of intending to use MWH of those who did not (AOR 5.4, 95% CI 3.01–9.69). Previous use of MWHs was significantly associated with intention to use one. Previous users of MWHs had 3.8 times the odds of intention to stay at a MWH of those who had not (AOR 3.8, 95% CI 2.32–6.27).
The odds of intention to use MWHs were 2.2 times higher among multigravida than primigravida women (AOR 2.2, 95% CI 1.164.29) and 1.8 times higher among pregnant women who had favorable subjective norms than those with unfavorable subjective norms (AOR 1.8, 95% CI 1.05–3.11). Positive attitudes toward MWHs showed 1.9 times the odds of intention to stay at one compared to those with negative attitudes (AOR 1.9, 95% CI 1.01–3.92). Those who believed that significant others would encourage their use of an MWH were twice as likely to have intentions to use one than those who believed their significant others would not approve of their use (AOR 2.0, 95% CI 1.16–3.60). (Table 2)
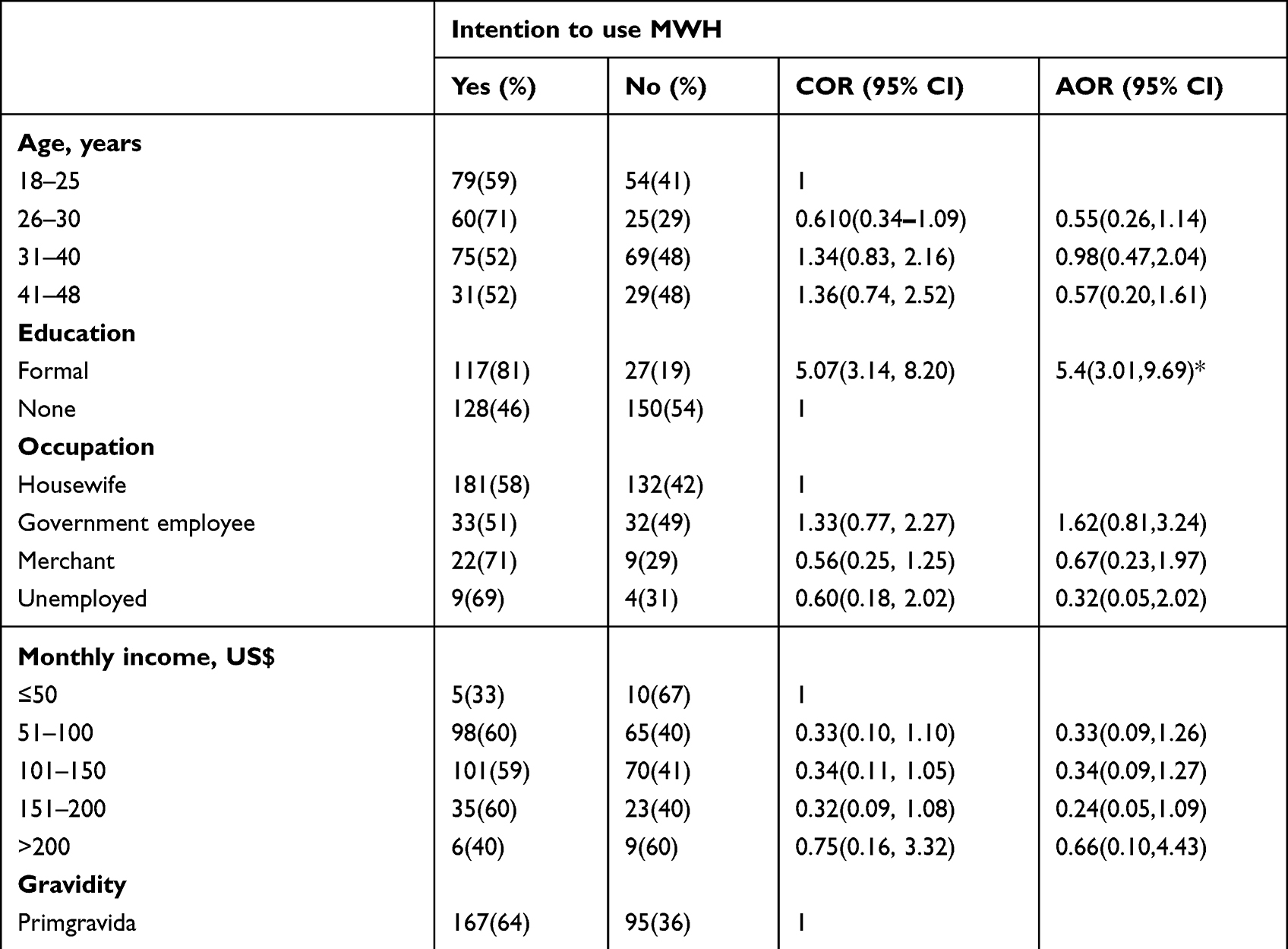 |
Table 2 Multivariate logistic regression analysis of associations between intention of pregnant women to use MWHs and predictors (n=422) |
Discussion
Despite MWHs’ proven effectiveness in preventing maternal and perinatal mortality in low- and middle-income countries, many low-income countries haven't yet implemented it widely. It is not even well understood whether pregnant women intend to use MWHs or factors predicting this. The current study measured the intention of pregnant women to stay in MWHs in Hargeisa, Somaliland using the theory of planned behavior as predictors of intention. Intention is believed to be an immediate predictor of behavior and its antecedents, including norms, attitudes, and perceived behavioral control predicting intention along with basic characteristics of the individual that can modify beliefs, attitudes, subjective norms, self-efficacy, and predict intention. Accordingly, six in ten pregnant women (245, 58%, 95% CI 53.1–62.8) intended to use MWHs. Education, multigravidity, previous use of MWHs, and subjective norms were found to be significant predictors of intention to use MWHs.
The finding of this study is in line with studies conducted in Eastern Gurage Zone and Jimma, which reported 55.1% and 57.3%, respectively,14,33 and similar to a study in Zambia (57.1%). However, this finding was higher than a study done in four regions of Ethiopia, where only 17% of participants intended to stay at MWHs34 and other study conducted in southwest Ethiopia, where 48.8% intended to use MWHs.44 In Ethiopia, there are wide variations in women's decision-making and cultural differences in preference of place of delivery. These variations result in differences in maternal health-service use, intention to use MWHs, an using a facility for delivery.45,46
The proportion of women who intended to stay at an MWH in the current study was lower than the 98% reported in Zambia.25 This was also lower than results in studies in other African countries: 90% in Ghana,10 66.6% in Zimbabwe,42 and 94% in Zambia.12 In spite of the perception that using MWHs is costly, about two-thirds (66.1%) of Kenyan women were very willing to stay at one.32 Generally, compared to many African countries, maternal health-service use is lower in Somaliland.47 We found that participants of the current study who had attended formal education had 5.4 times the odds of intending to stay at MWHs of those who had not. This finding is consistent with those from other low- and middle-income countries that reported that women with better education (high school and above) would be willing to stay at MWHs.6,25,33,39
Women who stayed at MWHs in their pregnancies had 3.8 times the odds of intending to stay at MWHs of those who had not. Not only previous use of MWHs predicts subsequent use but the behavior of health professionals and the services provided influence decision.48–50 Positive attitudes toward MWHs are an independent predictor of intention to use one. Those who had positive attitudes toward MWHs were 1.9 times more likely to be willing to use one. This association between positive attitudes and intention is supported by other studies in Ethiopia and Zambia.14,25,29,30
Despite the low ANC coverage and the fact that less than a quarter of deliveries take place at health facilities in Somaliland, the proportion of women who intended to stay at MWHs was fairly high. This implies that ANC gives women the opportunity to understand the benefits of facility delivery, although there is value perceived in traditional birth attendants in terms of the caring during normal labor. There is still a need to increase the uptake of antenatal services to provide women with knowledge about danger signs in pregnancy and birth preparedness.
This study is not without limitations, however. The intention to use MWHs was measured among pregnant women who sought ANC at the health facilities. The results would be different if the intention was measured at the community level including women who don't receive ANC, because those who visit health facilities have better awareness of danger signs in pregnancy and the benefits of facility delivery. However, we believe that women who don't visit health facilities for ANC don't have information about MWHs, and this could make it difficult to measure intention. In addition, this iwa a cross-sectional study and can't tell us about any causal relationship between intentions and the other subdomains of the theory, where reverse causation may also be there.
Conclusion
In this study, nearly six in ten pregnant women were willing to stay at MWHs during their last weeks of gestation. Taking into account existing maternal health-service use in Somaliland, this may be considered high. However, this intention doesn't guarantee actual use of MWHs, as there are several barriers between intention and behavior. Education, previous use of MWHs, multigravidity, and positive norms were important predictors of intention. It is necessary to create public awareness of the benefits of using MWHs to reduce negative social pressure toward their use.
Abbreviations
ANC, antenatal care; MWH, maternity waiting home; SN, subjective norm; VIF, variance-inflation factor; WHO, World Health Organization.
Ethics Approval and Informed Consent
Ethics clearance was obtained from the ethics review committee of the College of Medicine and Health Sciences, University of Gondar and from Hargeisa District Health Office. Participants under the age of 18 years were also allowed by the ethics committee to give consent as mature minors, because they were married and in charge of a family. A formal letter of permission to do the research was received from the Hargeisa District Health Office. The participants were given information about the purpose of the study, their right to decline or withdraw at any time, and refrain from answering any question they didn’t want to. Those who agreed to participate gave written consent before the interview. The interview took place at a private room after the participants had finished ANC. Personal identifiers were excluded from the questionnaire, and we used codes instead. The data were protected by passwords, and the hard copies were kept in a locked cupboard. We followed the principles of the Declaration of Helsinki.
Acknowledgments
The authors are grateful to the University of Gondar for covering the cost of the data collection. We acknowledge the Hargeisa District Health Office for giving us permission to conduct the study. We would like to thank the data collectors, supervisors, and study participants for their time and effort.
Authors' Contributions
All authors made a significant contribution to the work, including conception, study design, execution, acquisition of data, analysis, and interpretation, drafted, and written, substantially revised, and critically reviewed the article, have agreed on the journal to which the article will be submitted, reviewed and agreed on the final version of the article for submission, and agree to take responsibility and be accountable for the contents of the article.
Disclosure
The authors declare that they do not have any conflicts of interest.
References
1. World health organization. New Global Targets to Prevent Maternal Deaths: Access to a “Continuum of Care” Needed, Before, During and After Pregnancy and Childbirth. Geneva Switzerland: World Health Organization; 2021.
2. World Health Organization, UNICEF, United Nations Population Fund, Bank TW. Trends in Maternal Mortality: 2000 to 2017. Geneva: World health organization; 2019.
3. World Health Organization. Maternal Mortality. Geneva: World Health Organization; 2021.
4. World Health Organization. Trends in Maternal Mortality: 1990–2015: Estimates from WHO, UNICEF, UNFPA, World Bank Group and the United Nations Population Division. Geneva: World Health Organization; 2015.
5. Berhan Y, Berhan A. Commentary: reasons for persistently high maternal and perinatal mortalities in Ethiopia: Part III–perspective of the “three delays” model. Ethiop J Health Sci. 2014;24(4):137–148. doi:10.4314/ejhs.v24i0.12S
6. Gabrysch L, Campbell O. Still too far to walk: literature review of the determinants of delivery service use. BMC Pregnancy Childbirth. 2009;9(34). doi:10.1186/1471-2393-9-34
7. UNFPA. Giving birth should not be a matter of life and death; 2012.
8. Lori Jody R, Wadsworth Anna C, Munro Michelle L, Rominski S. Promoting access: the use of maternity waiting homes to achieve safe motherhood. Midwifery. 2013;29(10):1095–1102. doi:10.1016/j.midw.2013.07.020
9. UNICEF. Innovative approaches to maternal and newborn health compendium of case studies in United Nations children’s fund. New York: UNICEF; 2013.
10. Adigun OT, Mngomezulu TP. Occupational stress among teachers of learners with special needs. J Community Psychol. 2022;50:1185–1197. doi:10.1002/jcop.22712
11. Meshesha B, Dejene G, Hailemariam T. The role of maternity waiting area in improving obstetric outcomes: a comparative cross-sectional study, Jinka Zonal Hospital, Southern Regional State. Women’s Health Care. 2017;6(6):e34.
12. Lonkhuijzen V, Jelle S, Roosmalen V. Maternity waiting facilities for improving maternal and neonatal outcome in low-resource countries. PMC. 2012;10:CD006759.
13. Lori JR, Perosky J, Munro-Kramer ML, et al. Maternity waiting homes as part of a comprehensive approach to maternal and newborn care: a cross-sectional survey. BMC Pregnancy Childbirth. 2019;19(1):228. doi:10.1186/s12884-019-2384-6
14. Getnet E, Lakew G, Abraham G. Intention to use maternity waiting home among pregnant women in Jimma District, Southwest Ethiopia. Global J Inc. 2016;16(6):1–9.
15. ETHIOPIAN Emergency Obstetric and Newborn Care (EmONC). Assessment 2016. Addis Ababa, Ethiopia; 2017.
16. Abubakar S, Adamu D, Hamza R, Galadima JB. Determinants of home delivery among women attending antenatal care in Bagwai Town, Kano Nigeria. Afr J Reprod Health. 2017;21(4):73–79. doi:10.29063/ajrh2017/v21i4.8
17. Sialubanje C, Massar K, van der Pijl Marit SG, Kirch E, Hamer D, Ruiter R. Improving access to skilled facility-based delivery services: women’s beliefs on facilitators and barriers to the utilisation of maternity waiting homes in rural Zambia. Reprod Health. 2015;12(1):64–67. doi:10.1186/s12978-015-0051-6
18. Peggy S, Chibuye S, Bazant W, Namratha R, Timothee F. Experiences with and expectations of Maternity waiting homes in Luapula Province, Zambia: a mixed-methods, cross-sectional study with women, community groups and stakeholders. BMC Pregnancy Childbirth. 2018;18(42):54.
19. Fogliati P, Straneo M, Mangi S, Azzimonti G, Kisika F, Putoto G. A new use for an old tool: maternity waiting homes to improve equity in rural childbirth care Results from a cross-sectional hospital and community survey in Tanzania. Health Policy Plan. 2017;32:1354–1360. doi:10.1093/heapol/czx100
20. Braata F, Vermeiden T, Getneta G, Schifferc R, van den T, Jelle S. Comparison of pregnancy outcomes between maternity waiting home users and non-users at hospitals with and without a maternity waiting home: retrospective cohort study. Int Health. 2018;1–7. doi:10.1093/inthealth/ihx046
21. Gaym A, Pearson L, Soe K. Maternity waiting homes in Ethiopia–three decades experience. Ethiop Med J. 2012;50(3):209–219.
22. Somaliland MoNPaD. Somaliland multiple indicator cluster survey 2011. Final report; 2014.
23. Mramba L, Nassir F, Ondieki C, Kimanga D. Reasons for low utilization of a maternity waiting home in rural Kenya. Int J Gynecol Obstet. 2010;108(2):152–153. doi:10.1016/j.ijgo.2009.08.029
24. Andemichael G, Haile B, Kosia A, Mufunda J. Maternity waiting homes: a panacea for maternal/neonatal conundrums in Eritrea. J Eritrean Med Assoc. 2009;4(1):18–21.
25. Cephas S, Karlijn M, Hamer D, Robert R. Personal and environmental factors associated with the utilisation of maternity waiting homes in rural Zambia BMC Pregnancy and Childbirth. BMC Pregnancy Childbirth. 2017;17(1):136.
26. Somaliland RO, Health MO. National health policy.
27. The Somaliland health and demographic survey. Ministry of Planning and National Development. Hargeisa: Somaliland Government. Somaliland: Central Statistics Department; 2020.
28. Glanz K, Rimer B, Viswanath K. Health Behavior and Health Education: Theory, Research, and Practice.
29. Sialubanje C, K. M, Hamer H, Ruiter RAC. A Personal and environmental predictors of the intention to use maternal healthcare services in Kalomo, Zambia. Health Educ Res. 2014;29(6):1028–1040. doi:10.1093/her/cyu057
30. Lera T, Admasu B, Dirar A. Intention to use institutional delivery and associated factors among ANC attendants in Wollaita Soddo Town, Southern Ethiopia: a cross-sectional community based study, application of theory of planned behavioral model. Am J Public Health Res. 2017;5(4):89–97. doi:10.12691/ajphr-5-4-1
31. Scott A, Vian T, Kaiser L, Nogoma T, Mataka K, Henry E. Listening to the community: using formative research to strengthen maternity waiting homes in Zambia. PLoS One. 2018;13(3):e0194535. doi:10.1371/journal.pone.0194535
32. Ware AR. Knowledge, attitude and practice of mothers towards skilled delivery services in a maternity waiting home in Merti District, Isiolo County. Prime J Soc Sci. 2015;4(8):1140–1154.
33. Vermeiden T, Braat F, Medhin G, Gaym A, van den Akker T, Stekelenburg J. Factors associated with intended use of a maternity waiting home in Southern Ethiopia: a community-based crosssectional study. BMC Pregnancy Childbirth. 2018;18(1):38. doi:10.1186/s12884-018-1670-z
34. Gizachew T, Belaynew T, Ali K, Betemariam W, Nebreed Z, Wereta T. Maternity waiting homes in rural health centers of Ethiop: the situation, women’s experiences and challenges. Ethiop J Health Develop. 2016;30(1):19–28.
35. Wilson JB, Collison AH, Richardson D, Kwofie G, Senah KA, Tinkorang EK. The maternity waiting home concept: the Nsawam, Ghana experience. The accra PMM team. Int J Gynaecol Obstet. 1997;59(Suppl 2):S165–S172. doi:10.1016/S0020-7292(97)00162-8
36. Ajzen I. The theory of planned behavior. Organ Behav Hum Decis Process. 1991;50:179–211. doi:10.1016/0749-5978(91)90020-T
37. Ajzen I, Fishbein M. The Influence of Attitudes on Behavior the Handbook of Attitudes Erlbaum. Mahwah, NJ; 2005.
38. Sialubanje C, Massar K, Hamer D, Ruiter C. Understanding the psychosocial and environmental factors and barriers affecting utilization of maternal healthcare services in Kalomo, Zambia a qualitative study. Adv Access. 2014;29(3):521–532.
39. Bayu H, Adefris M, Amano A, Abuhay M. Pregnant women’s preference and factors associated with institutional delivery service utilization in Debra Markos Town, North West Ethiopia: a community based follow up study. BMC Pregnancy Childbirth. 2015;15(1):15–21. doi:10.1186/s12884-015-0437-z
40. Cafiero M. Nurse practitioner’s knowledge, experience, and intention to use health literacy strategies in clinical practice. J Health Commun. 2013;18:70–81. doi:10.1080/10810730.2013.825665
41. Sialubanje C, Massar K, Hamer D, Ruiter RA. Reasons for home delivery and use of traditional birth attendants in rural Zambia a qualitative study. BMC Pregnancy Childbirth. 2015;15(1). doi:10.1186/s12884-015-0652-7
42. Sialubanje C, Massar K, Kirch E, VdP MSG, Hamer D, Ruiter R. Husbands’ experiences and perceptions regarding the use of maternity waiting homes in rural. Zambia Int J Gynecol Obstet. 2016;133(1):108–111. doi:10.1016/j.ijgo.2015.08.023
43. Development MoPa N. Somaliland perception survey; 2015.
44. Yismaw W. Intention to use maternity waiting home among pregnant women in Mettu District. South-Western Ethiopia; 2018.
45. Yesuf EA, Calderon-Margalit R. Disparities in the use of antenatal care service in Ethiopia over a period of fifteen years. BMC Pregnancy Childbirth. 2013;13(1):131. doi:10.1186/1471-2393-13-131
46. Berelie Y, Yeshiwas D, Yismaw L, Alene M. Determinants of institutional delivery service utilization in Ethiopia: a population based cross sectional study. BMC Public Health. 2020;20(1):1077. doi:10.1186/s12889-020-09125-2
47. Mouhoumed HM, Mehmet N. Utilization pattern of antenatal care and determining factors among reproductive-age women in Borama, Somaliland. J Prev Med Hyg. 2021;62(2):E439–e46. doi:10.15167/2421-4248/jpmh2021.62.2.1882
48. Kurji J, Gebretsadik LA, Wordofa MA, et al. Factors associated with maternity waiting home use among women in Jimma Zone, Ethiopia: a multilevel cross-sectional analysis. BMJ Open. 2019;9(8):e028210. doi:10.1136/bmjopen-2018-028210
49. Gezimu W, Bitewa YB, Tesema MT, Wonde TE, Spradley FT. Intention to use maternity waiting home and associated factors among pregnant women in Gamo Gofa zone, Southern Ethiopia, 2019. PLoS One. 2021;16(5):e0251196. doi:10.1371/journal.pone.0251196
50. Kassa BG, Ayele AD, Belay HG, Mihiretie GN, Worke MD, Health G. Utilisation of maternity waiting homes and its associated factors in Ethiopia: systematic reviews and meta-analysis. Clin Epidemiol Global Health. 2021;12:100891.
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.