")
Back to Journals » Nature and Science of Sleep » Volume 12
Insomnia Symptoms and Their Association with Anxiety and Poor Sleep Hygiene Practices Among Ethiopian University Students
Authors Manzar MD , Noohu MM , Salahuddin M, Nureye D , Albougami A , Spence DW , Pandi-Perumal SR , Bahammam AS
Received 22 January 2020
Accepted for publication 15 July 2020
Published 13 August 2020 Volume 2020:12 Pages 575—582
DOI https://doi.org/10.2147/NSS.S246994
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Steven A Shea
Md Dilshad Manzar,1 Majumi M Noohu,2 Mohammed Salahuddin,3,4 Dejen Nureye,3 Abdulrhman Albougami,1 David Warren Spence,5 Seithikurippu R Pandi-Perumal,6 Ahmed S Bahammam7,8
1Department of Nursing, College of Applied Medical Sciences, Majmaah University, Al Majmaah, Saudi Arabia; 2Centre for Physiotherapy and Rehabilitation Sciences, Jamia Milia Islamia, New Delhi, India; 3Mizan-Tepi University, Mizan-Aman, Ethiopia; 4Department of Bio-Molecular Sciences, Pharmacology Division, University of Mississippi, Oxford, MS, USA; 5Independent Researcher, Toronto, ON, Canada; 6Somnogen Canada Inc, Toronto, ON, Canada; 7The University Sleep Disorders Center, College of Medicine, King Saud University, Riyadh, Saudi Arabia; 8The Strategic Technologies Program of the National Plan for Sciences and Technology and Innovation in Saudi Arabia (MED511-02-08), Riyadh, Saudi Arabia
Correspondence: Md Dilshad Manzar Department of Nursing, College of Applied Medical Sciences
Majmaah University, Al Majmaah 11952, Saudi Arabia
Email [email protected]
Objective: There is a paucity of research evidence available regarding the impact of anxiety and sleep hygiene on insomnia and related sleep complaints among collegiate students in lower-income countries. The purpose of this study was to investigate if insomnia and insomnia-related sleep complaints are associated with anxiety, age, and sleep hygiene practices among a sample of university students in Ethiopia.
Design, Measures, Setting, and Participants: The participants were young adults (n=525; mean age 21.5 ± 3.0 years; mean BMI of 20.7 ± 2.7kg/m2). Young collegiate adults at Mizan-Tepi University in southwestern Ethiopia were randomly selected to participate in this cross-sectional study. The measures included the Leeds Sleep Evaluation Questionnaire-Mizan (LSEQ-M), the Generalized Anxiety Disorder– 7 Scale (GAD-7), and the Sleep Hygiene Index (SHI). Descriptive statistics, binary logistic regression, and multiple linear regressions were used.
Results: Insomnia was associated with young age group (≤ 25 years) (odds ratio (OR) = 2.20, 95% confidence interval (CI) 1.04– 4.66), higher GAD-7 (anxiety) (OR = 1.05, 95% CI 1.0– 1.10) and SHI (poor sleep hygiene) (OR = 1.15, 95% CI 1.05– 1.26) scores. All four insomnia-related sleep complaints were associated with increasing GAD-7 scores, as well as higher SHI scores (p< 0.001).
Conclusion: Insomnia was associated with younger age group (≤ 25 years), higher anxiety level, and poor sleep hygiene. Four major sleep complaints in insomnia, ie, sleep onset problems, poor sleep quality, awakening problems, and daytime disturbances, were all associated with higher anxiety levels and poor sleep hygiene.
Keywords: sleep, sleepiness, daytime dysfunction, young adults, low-income country
Introduction
People with insomnia often report having difficulties with initiating and maintaining sleep, early morning awakenings, and sleep that is not refreshing. The high incidence of the condition is not helped by a prevailing attitude among many patients that insomnia is only one of the many challenges of life and is therefore not a “real” health problem that necessitates consultation with medical professionals.1,2 A consequence of the under-reporting of insomnia is that many medical professionals fail to diagnose insomnia symptoms, and thus remedial measures are often not taken to address the condition.3
Insomnia is a common sleep disorder affecting a significant proportion of the general population.4 Collegiate students are reported to have high rates of insomnia. In a systematic review, Jiang, et al5 reported that insomnia had a weighted mean prevalence of 18% among this group, which is higher than its rate of occurrence in the general population. Byrd et al6 found that the prevalence of insomnia among college students in Ethiopia was as high as 61%, while another study found it to be 44.7%.7 Insomnia symptoms are not only widespread, but they can also impact life adjustment. Sleep disturbances are known to affect both academic and workplace performance.8 Additionally, sleep plays a vital role in cognitive functions such as judgment, as well as memory consolidation and recall, factors which are vital for academic performance.9,10 Insomnia in college students is associated with psychological conditions such as depression and anxiety, as well as with certain behaviors such as substance abuse and poor sleep habits.6,11 Substance abuse has been found to affect many aspects of sleep health.11 Anxiety is one of the most commonly reported general mental disorders in university students. Anxiety disorders can arise from or can be exacerbated by various psychological issues or challenging situations in life. Among college or university students in particular these can include fears or concerns about academic performance, thoughts about the future, and other social pressures.12 Poor sleep hygiene practices can affect both sleep quality and quantity, which in turn can affect daytime functioning.13 While these life adjustment challenges frequently occur among college students, they often go unacknowledged by the students themselves, and the broader health implications of inadequate sleep are frequently devalued.
There have been few studies regarding the association between insomnia, insomnia related sleep complaints, and important factors that may affect these symptoms, in particular, the conditions of psychological anxiety and/or sleep hygiene practices among college or university students from lower-income countries. None of the previous studies investigating insomnia and its correlates used a standard questionnaire tool for screening insomnia that has been validated in Ethiopians. The present study was carried out to investigate these issues more closely. In particular, the study sought to determine the extent of the association between insomnia symptoms and some key factors which have previously been shown in general population samples to have deleterious effects on sleep. Thus, the study objectives were:
- To find if subjective insomnia is associated with anxiety, age, and sleep hygiene among college students in Ethiopia.
- To find if insomnia related sleep complaints, ie, difficulty in sleep onset, poor sleep quality, awakening problems, and daytime disturbances are associated with anxiety and sleep hygiene practices among college students in Ethiopia.
Participants and Methods
Participants
A sample of 700 students was initially selected to enroll in a cross-sectional study. Thirty-eight of the selected individuals declined to participate, 23 were excluded, 17 were deleted for person-level missing values, and 97 did not attend the interview. The screening process was carried out after 1–2 weeks of recruitment. The survey questionnaires were administered in hard copy during one-on-one meetings. A final dataset of 525 young collegiate adults with a mean age of 21.5 ± 3.0 years and a mean body mass index of 20.7 ± 2.7kg/m2 was used in the analysis. Participants were selected by simple random sampling using a lottery method from the pool of students registered at Mizan-Tepi University, Mizan-Aman city (located in South-western Ethiopia). The self-reported account of taking psychoactive medications or who had memory problems were excluded. This was done to remove memory-related bias in the self-reported measures used in this study.
Procedure
The study was reviewed and approved by the Institutional Review Board of the College of Health Sciences, Mizan-Tepi University, Ethiopia. As part of the recruitment and screening process, full disclosures were made to the participants. These include: (i) a detailed explanation about the major objective and procedures, (ii) that their participation was voluntary, and (iii) that they had the right to discontinue at any stage. All participants were asked to read and sign forms relating to their informed consent to serve as research subjects and consent to allow the publication of masked data about their performance as per the Helsinki declaration and Good Ethical Practices Convention. The study questionnaire package consisted of the Generalized Anxiety Disorder-7 scale (GAD-7),14 the Leeds Sleep Evaluation Questionnaire-Mizan (LSEQ-M),7 the Sleep Hygiene Index,15 and a semi-structured socio-demographics inventory. The survey questionnaire package was in English because participants were young collegiate adults from an Ethiopian university, where the medium of instruction is English. Moreover, there are more than 80 languages in Ethiopia, and proficiency in reading in the official language, ie, Amharic, is not consistent.
Measures
Insomnia and Related Sleep Complaints: Leeds Sleep Evaluation Questionnaire-Mizan (LSEQ-M)
Insomnia and related sleep complaints were screened by the Leeds Sleep Evaluation Questionnaire – Mizan (LSEQ-M) because this tool has been shown to possess adequate internal consistency, discriminative validity, and factorial validity in Ethiopian university students.7 LSEQ-M is an English version of the original LSEQ that has been adapted for screening of insomnia in students; it has 10 items, all of which are scored on a 100 mm response line, a format known as a visual analog scale (VAS).7 Responses for each individual LSEQ-M item (0–100 VAS) are divided by 10 to obtain scores in the range of 0–10. The LSEQ-M total score with a range of 0–100 is generated by adding all such scores (0–10 range) for all the 10-items.7 Lower LSEQ-M scores are indicative of subjective insomnia at a cut-off score of 52.6 with a sensitivity of 94%, and specificity of 80%.7 The LSEQ-M factors represent four different insomnia complaints. Factor-1 of the LSEQ-M has three items and is referred to as LSEQ-GTS (range: 0–30); this measure sleep onset problems. Factor-2 of the LSEQ-M has two items and is referred to as LSEQ-QOS (range: 0–20); this measures sleep quality. Factor-3 of the LSEQ-M has two items and is referred to as LSEQ-AFS (range: 0–20); this measure awakening problems. Factor-4 of the LSEQ-M has two items and is referred to as LSEQ-BFW (range: 0–20); this measure daytime disturbances.7,16 Lower scores for the LSEQ-M factors, ie, LSEQ-GTS score, LSEQ-QOS, LSEQ-AFS, and LSEQ-BFW indicated difficulty in sleep onset, poor sleep quality, awakening problems, and daytime disturbances.7,16
Generalized Anxiety Disorder–7 Scale
The Generalized Anxiety Disorder–7 (GAD-7) scale is one of the most commonly used questionnaire tools to evaluate respondents’ levels of anxiety. The questionnaire has 7-items; these are scored according to increasing weekly frequency of the respondent’s reported anxiety-related symptoms, ie, where ‘0ʹ stands for “not at all sure” to ‘4ʹ for “nearly every day”.14 The GAD-7 scale global score is obtained by adding all the individual item scores, which may range from 0 to 21. A higher GAD-7 total score suggests a greater severity of the anxiety symptoms.14,17 Kroenke et al showed that the scale has diagnostic validity for the screening of anxiety disorders with adequate sensitivity (68%) and specificity (88%).17 The questionnaire has been validated in various populations across the world.14,17,18
Sleep Hygiene Index (SHI)
Sleep hygiene refers to a range of psychological, attitudinal, and behavioral factors, much of which is under self-control, and which may broadly affect sleep quality. The Sleep Hygiene Index (SHI) is a self-report measure of sleep hygiene practices developed by Mastin and his two colleagues in 2006. The 13-item questionnaire is widely used in research and in clinical practice.15 The SHI has been shown to have adequate construct validity and reliability, internal consistency, and test re-test reliability.15 The SHI was used in the present study with slight modifications, ie, the scoring method for SHI items was dichotomized so that there were two possible responses (Yes/No) for each of the 13 items. A response of “No” was scored as ‘0ʹ, while “Yes” was recorded as ‘1ʹ. Scores for each of the 13 items were added to get the SHI total score. A higher SHI total score was indicative of poor sleep hygiene practices. As determined by the “greatest lower bound to reliability” (glb) ratio of 0.84, the modified SHI with dichotomized scoring for its items was found to have adequate reliability in this study population.19
Socio-Demographic Questionnaire
Apart from the abovementioned validated questionnaire tools, this study also employed a semi-structured inventory to collect information related to the participants’ socio-demographic characteristics. There were open-ended questions for age, height, weight, and the percentage of classes attended; responses for gender, years of university education, and types of accommodation were recorded by closed-ended items. The presence of chronic health conditions was also recorded. These included any history of AIDS, diabetes, epilepsy, hypertension, tuberculosis, cardiovascular complications, and any other chronic diseases.
Statistical Analysis
All of the statistical analyses in this study were performed using the SPSS statistical package, version 23.0. Participants’ characteristics were described using the mean ± SD, percentage, and frequency. The relationship between insomnia and participants’ characteristics was assessed using a Chi-square test or Fisher’s exact test for categorical variables and the Student’s independent t-test for continuous variables. Finally, the binary regression method was used after establishing its assumptions in the study data. For the logistic regression model several outcomes or conditions were observed: (i) there were no multivariate outliers as determined by the Mahalanobis distance; Χ2 (9) = 27.88, p<0.001, (ii) observations were independent, (iii) no issue of multicollinearity among independent variables as determined by the Spearman correlation coefficients occurred, and (iv) two variables (age and BMI) were converted into categorical variables because these were not linearly related to the log odds. The dichotomized measure of insomnia/non-insomnia (normal) served as the dependent variable; the independent variables were: age groups, GAD-7 total score, and SHI total score; the covariates were: BMI (kg/m2) categories, gender, attendance (percentage of lectures attended), chronic health conditions, type of accommodation, and years of university education.
All the covariates and independent variables, with the exception of BMI, gender, chronic health conditions, and attendance, were significantly correlated with insomnia. However, BMI, gender, chronic health conditions, and attendance were used as covariates or predictors because earlier studies have shown them to be related to poor sleep and/or insomnia.20–23 Furthermore, multiple linear regression analyses (backward method) were performed to determine association individually for each of the four insomnia related complaints with anxiety, poor sleep hygiene, and other socio-demographic characteristics.
Results
Participants’ Characteristics
The prevalence of insomnia symptoms was high, with 42.9% of the participating students having this condition. Most of the students (88.6%) were in the age group of ≤25 years (Table 1). Less than one-fifth of the participants were underweight (Table 1). Most of the young Ethiopian collegiate adults participating in the study were males (80.8%) (Table 1). About two-thirds of them were enrolled in their first or second years of university education (Table 1). About one-tenth of the students reported having chronic diseases/conditions (Table 1). The average values of attendance, GAD-7 total score, and SHI total score were 95.2 ± 7.1, 7.3 ± 4.4, and 6.6 ± 2.3, respectively (Table 1).
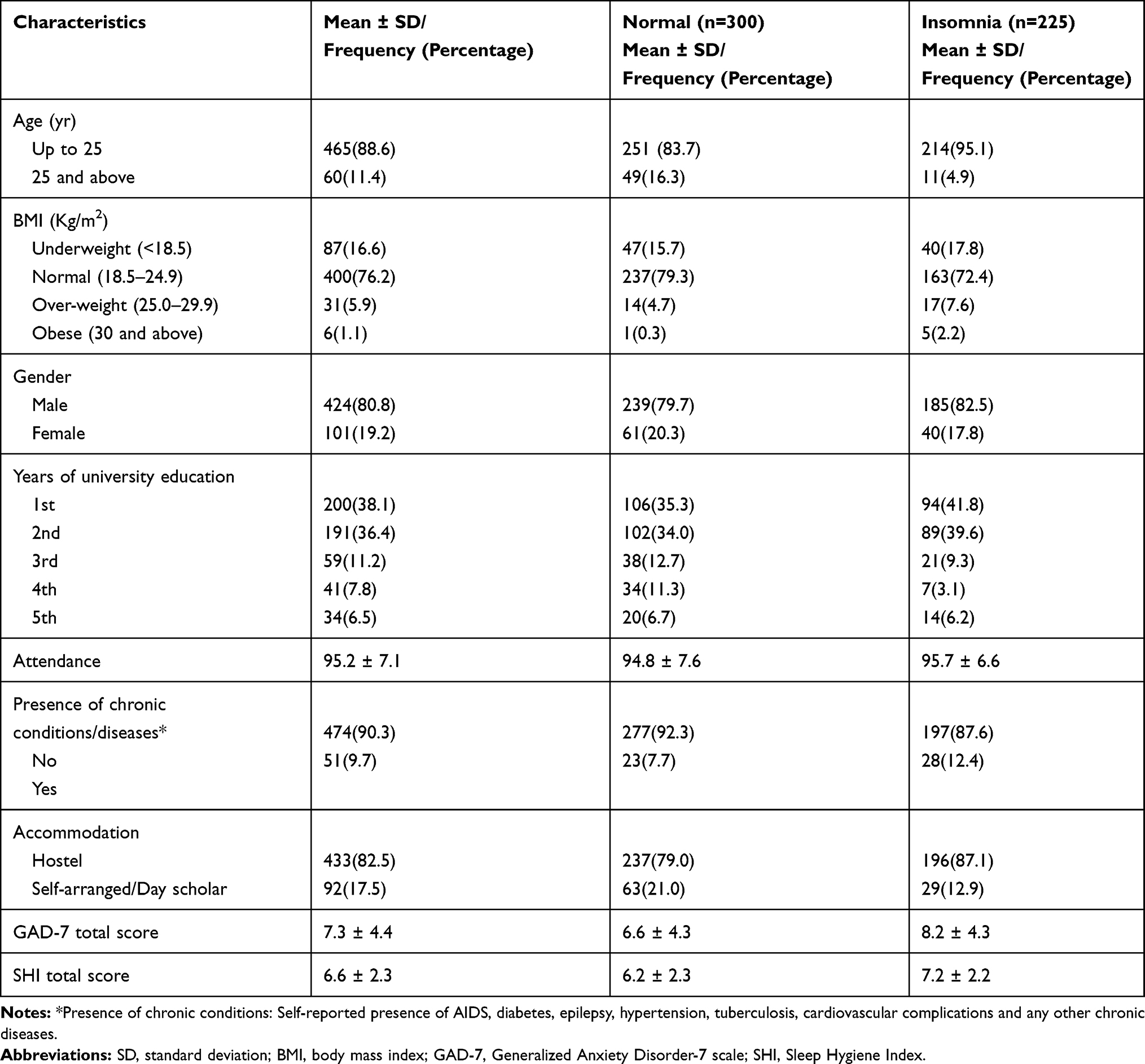 |
Table 1 Participants’ Characteristics and Their Relationship with Insomnia in Ethiopian Collegiate Young Adults |
Binary Logistic Regression: Association of Insomnia with Generalized Anxiety Disorder and Sleep Hygiene
Table 2 presents the findings of the binary logistic regression. The regression model was adjusted for BMI (kg/m2) categories, gender, attendance (percentage of lectures attended), chronic health conditions, type of accommodation, and years of university education. The model explained about 15.1% of the variance in the classification of insomnia. The prediction had an accuracy of 62.6% in the classification of insomnia; it was significant in comparison to a model with intercept only; χ2(14, N = 525) = 62.62, p < 0.001. Insomnia was associated with the age group of ≤25 years (odds ratio (OR) = 2.20, 95% confidence interval (CI) 1.04–4.66), increasing scores of the GAD-7 scale (OR = 1.05, 95% CI 1.0–1.10) and increasing scores of SHI (OR = 1.15, 95% CI 1.05–1.26) score (Table 2).
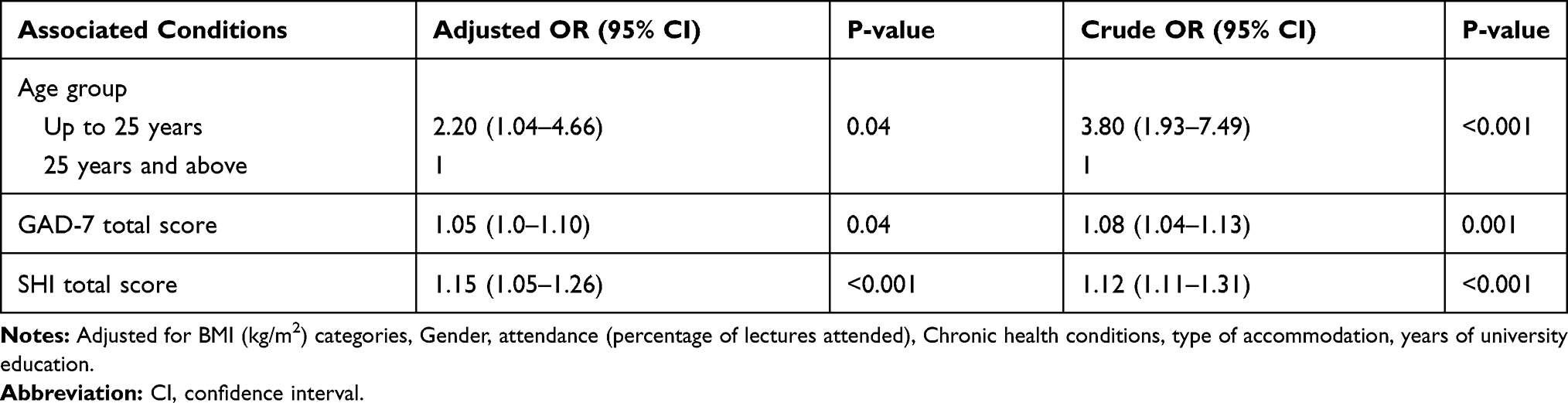 |
Table 2 Binary Logistic Regression: Association of Insomnia with the Generalized Anxiety Disorder-7 Scale (GAD-7) and Sleep Hygiene Index (SHI) in Ethiopian Collegiate Young Adults |
Multiple Linear Regression: Association of the Four Subjective Insomnia Related Complaints with GAD-7 Score and SHI Score
Table 3 shows the results of the multiple regression analysis of the four LSEQ-M factors with anxiety, poor sleep hygiene, and other socio-demographic characteristics in the study population. A higher GAD-7 Score (increasing level of anxiety) was associated with all the four insomnia related complaints, ie, difficulty in sleep onset (lower LSEQ-GTS score), poor sleep quality (lower LSEQ-QOS score), awakening problems (lower LSEQ-AFS score) and daytime disturbances (lower LSEQ-BFW score). Higher SHI score (poor sleep hygiene) was associated with three insomnia related complaints, ie, difficulty in sleep onset (lower LSEQ-GTS score), awakening problems (lower LSEQ-AFS score) and daytime disturbances (lower LSEQ-BFW score). Effect sizes (Cohen’s f2) for all the four insomnia related complaints were very small, ie, less than 0.02 (Table 3).
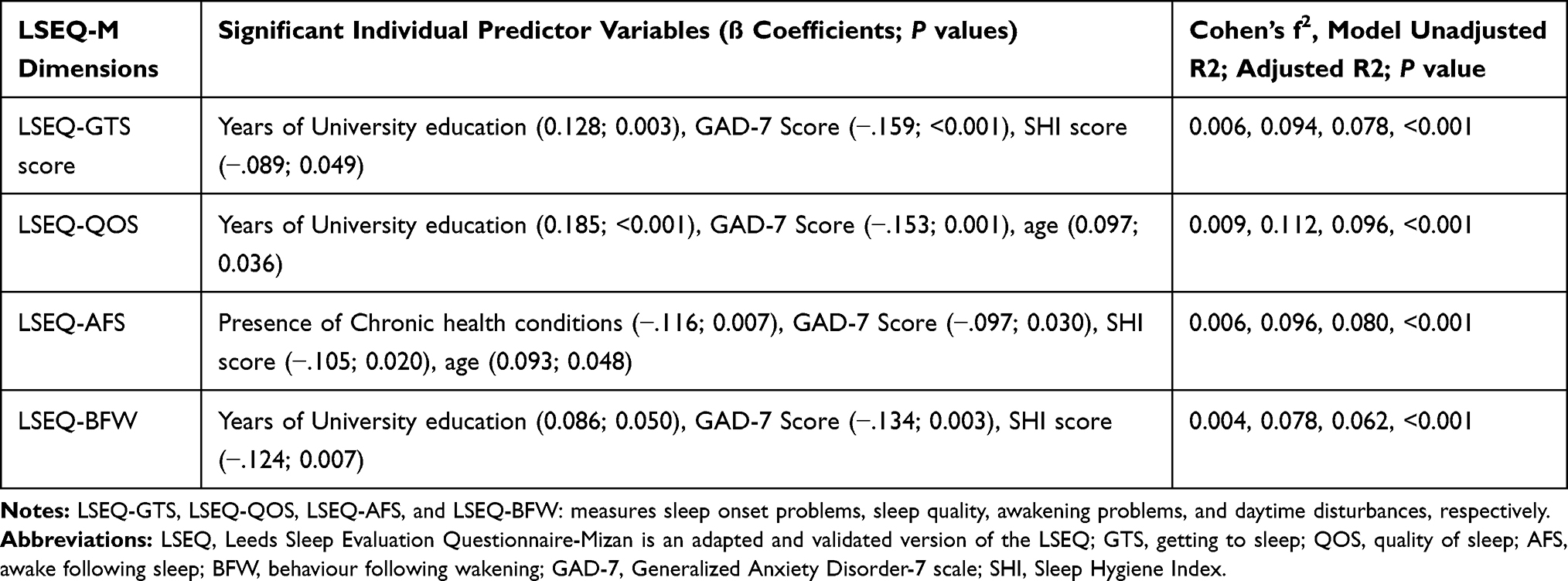 |
Table 3 Multiple Linear Regression: Associated Factors of Sleep Complaints in Insomnia |
Discussion
This is the first study to investigate the association between insomnia, insomnia related sleep complaints with poor sleep hygiene and anxiety level in a population of African university students using standardized and validated questionnaires for all three measures. Insomnia and increasing severity of insomnia related sleep complaints had a significant association with higher anxiety levels and poor sleep hygiene practices in the study population. This consistency of the relationship between insomnia and its related complaints in this study population is similar in generality to the conclusions of a recent meta-analysis which found that insomnia predicts 3.23 times higher chances of developing anxiety disorders in insomniacs.24 Similarly, a meta-analysis concluded that sleep hygiene-based interventions have a significant and positive effect on sleep quality, sleep onset duration, sleep rhythms, and sleep problems.25 Therefore, these two measures, ie, higher anxiety level and poor sleep hygiene practices seem to be consistent predictors of subjective insomnia and related complaints across different populations remaining unaffected by the moderating/mediating effect of other socio-demographic characteristics.24,25
The study showed that younger students (those up to 25 years of age) were associated with insomnia (in both bivariate and multivariate analysis) as well as insomnia complaints of poor sleep quality and awakening problems. This finding is similar to that reported by a large nationwide student health survey in Norway. Similar, to the findings of this study, the Norwegian survey found that the university students in the age group of 18 to 25 years had a higher prevalence of insomnia than those in the age group of 26 to 35 years.26 This consistency in age-pattern of insomnia in university students in Africa and Europe indicates the involvement of similar patho-psychophysiological mechanisms at play, whose impact is evident in spite of socio-economic disparities.26 In brief, the relationship between subjective insomnia with a higher level of anxiety, poor sleep hygiene, and those students with less than 25 years of age was further strengthened by significant association of all four insomnia related sleep complaints with these three variables, ie, anxiety, sleep hygiene, and age.
With regard to the findings, that the younger students had more incidences of insomnia and insomnia related sleep complaints, there are some factors that might have been responsible for precipitating the conditions. For example, younger students, who are experiencing university life for the first time, are required to make some major adjustments: these include sudden changes in their sleeping environment, an unfamiliar type of accommodation, the anxiety of staying away from family, a transition to higher academic standards of performance, and family and peer pressure to excel in studies.27 All these factors can impose chronic stress on the participants, which in turn, results in insomnia related complaints and chronic sleep loss. It is well-known that chronic sleep loss (either self-imposed or imposed by external circumstances) and associated sleepiness and daytime impairments result in poor academic performance, personal physical and mental health, and safety considerations.9 The university health centers in low-income countries may better have regular screening for insomnia, sleep hygiene practices, and anxiety among college students. More importantly, the modifiable risk factors of insomnia such as sleep hygiene may help in targeted strategizing to manage insomnia in this population. Student-centric counseling sessions may be better implemented to sensitize and educate about managing sleep hygiene practices and other modifiable risk factors to help decrease the onset of anxiety and insomnia, which may hopefully prevent further negative secondary outcomes.
Insomnia can be caused by psychological stressors, such as anxiety, and, further, that this relationship is bi-directional: sleep problems result in daytime sleepiness and can impair memory functions and cognitive efficiency. Affected individuals thus have a reduced ability to solve academic or employment-related problems, which ultimately leads to further anxiety.9 Firm conclusions regarding this bidirectionality cannot always be made due to its basic complexity. However, the best existing evidence suggests insomnia is bidirectionally related to anxiety and depression.28 People with insomnia typically report having high levels of depression, anxiety, stress, and a poor quality of life.11 These symptoms, in turn, may have broader effects on health.4
The present study focused on measurable associations between insomnia and anxiety, but nevertheless, certain limitations prevent the broad generalizability of the findings. It was not possible for instance to establish whether the high levels of anxiety that were found among a large proportion of the subjects were a contributing factor to their poor sleep hygiene or possibly were a consequence of it. Other limitations in the study were that the study did not measure and adjust the model with some of the important co-variates of insomnia, such as physical activity, academic performance, other mental conditions, history of substance abuse, etc. This missing out of some of the important co-variates most likely explains the low variance, especially in the multiple regression models. The notable strength of the study was that insomnia, anxiety, and sleep hygiene were measured by standardized tools.
Conclusion
There was a high prevalence of insomnia, which is associated with both anxiety and poor sleep hygiene in Ethiopian college students.
Abbreviations
GAD-7, Generalized Anxiety Disorder-7 scale; LSEQ-M, Leeds Sleep Evaluation Questionnaire-Mizan; SHI, Sleep Hygiene Index; VAS, Visual Analog Scale; GLB, greatest lower bound to reliability; BMI, body mass index; AIDS, acquired immunodeficiency syndrome; SD, standard deviation.
Data Sharing Statement
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Ethics Approval and Consent to Participate
The study was approved by the Human Institutional Ethics Committee Mizan-Tepi University, and written informed consent was obtained from all participants. All authors have approved the final draft.
Consent to Publish
The participants provided informed consent to publish.
Acknowledgments
We are grateful to the participants of the study. The authors extend their appreciation to the Deanship of Scientific Research at Majmaah University for funding this work under Project Number No (RGP-2019-40).
Author Contributions
All authors made substantial contributions to conception and design, acquisition of data, or analysis and interpretation of data; took part in drafting the article or revising it critically for important intellectual content; gave final approval of the version to be published; and agree to be accountable for all aspects of the work.
Funding
The authors extend their appreciation to the Deanship of Scientific Research at Majmaah University for funding this work under Project Number No (RGP-2019-40).
Disclosure
SRP is a stockholder, and the President and Chief Executive Officer of Somnogen Canada Inc., a Canadian corporation. He declares that he has no competing interests that might be perceived to influence the content of this article. This affiliation of SRP with Somnogen Canada Inc., a Canadian Corporation, does not alter the authors’ adherence to Nature and Science of Sleep. SRP has received royalty support from for his role as an editor-in-chief and/or an editor of various academic volumes. All remaining authors declare that they have no proprietary, financial, professional or other personal interest of any nature in any product, service and/or company that could be construed or considered to be a potential conflict of interest that might have influenced the views expressed in this paper.
References
1. Blunden S, Lushington K, Lorenzen B, Ooi T, Fung F, Kennedy D. Are sleep problems under-recognised in general practice? Arch Dis Child. 2004;89(8):708–712. doi:10.1136/adc.2003.027011
2. Almeneessier AS, Alamri BN, Alzahrani FR, Sharif MM, Pandi‑Perumal SR, Bahammam AS. Insomnia in primary care settings: still overlooked and undertreated? Aljohara. J Nat Sci Med. 2018;1:64–68. doi:10.4103/JNSM.JNSM
3. Saddichha S, Diagnosis and treatment of chronic insomnia. Ann Indian Acad Neurol. 2010;13(2):94–102. doi:10.4103/0972-2327.64628
4. Winkelman JW. Insomnia disorder. N Engl J Med. 2015;373(15):1437–1444. doi:10.1056/NEJMcp1412740
5. Jiang XL, Zheng XY, Yang J, et al. A systematic review of studies on the prevalence of insomnia in university students. Public Health. 2015;129(12):1579–1584. doi:10.1016/j.puhe.2015.07.030
6. Byrd KL, Gelaye B, Tadesse MG, Williams MA, Lemma S, Berhane Y. Sleep disturbances and common mental disorders in college students. Heal Behav Policy Rev. 2014;1(3):229–237. doi:10.14485/hbpr.1.3.7
7. Manzar MD, Salahuddin M, Maru TT, et al. Validation of the adapted Leeds sleep evaluation questionnaire in Ethiopian university students. Health Qual Life Outcomes. 2018;16(1):1–8. doi:10.1186/s12955-018-0876-0
8. Chiang Y-C, Arendt S, Zheng T, Hanisch K. The effects of sleep on academic performance and job performance. Coll Stud J. 2014;48(1):72.
9. Haile YG, Alemu SM, Habtewold TD. Insomnia and its temporal association with academic performance among University students: a cross-sectional study. Biomed Res Int. 2017;2017:1–7. doi:10.1155/2017/2542367
10. Stickgold R. Sleep-dependent memory consolidation. Nature. 2005;437:1272–1278. doi:10.1038/nature04286
11. Taylor DJ, Bramoweth AD, Grieser EA, Tatum JI, Roane BM. Epidemiology of insomnia in college students: relationship with mental health, quality of life, and substance use difficulties. Behav Ther. 2013;44(3):339–348. doi:10.1016/j.beth.2012.12.001
12. Eisenberg DL, Gollust SE, Golberstein E, Hefner JL. Prevalence and correlates of depression, anxiety, and suicidality among university students. Am J Orthopsychiatry. 2007;77(4):534–542. doi:10.1037/0002-9432.77.4.534
13. Gellis LA, Park A, Stotsky MT, Taylor DJ. Associations between sleep hygiene and insomnia severity in college students: cross-sectional and prospective analyses. Behav Ther. 2014;45(6):806–816. doi:10.1016/j.beth.2014.05.002
14. Spitzer RL, Kroenke K, Williams JB, Lowe B. A brief measure for assessing generalized anxiety disorder: the GAD-7. Arch Intern Med. 2006;166(10):1092–1097. doi:10.1001/archinte.166.10.1092
15. Mastin DF, Bryson J, Corwyn R. Assessment of sleep hygiene using the sleep hygiene index. J Behav Med. 2006;29(3):223–227. doi:10.1007/s10865-006-9047-6
16. Tarrasch R, Laudon M, Zisapel N. Cross‐cultural validation of the Leeds sleep evaluation questionnaire (LSEQ) in insomnia patients. Hum Psychopharmacol. 2003;18(8):603–610. doi:10.1002/hup.534
17. Kroenke K, Spitzer RL, Williams JBW, Monahan PO, Löwe B. Anxiety disorders in primary care: prevalence, impairment, comorbidity, and detection. Ann Intern Med. 2007;146(5):317–325. doi:10.7326/0003-4819-146-5-200703060-00004
18. Bártolo A, Monteiro S, Pereira A. Factor structure and construct validity of the generalized anxiety disorder 7-item (GAD-7) among Portuguese college students. Cad Saude Publica. 2017;33(9):e00212716. doi:10.1590/0102-311x00212716
19. Trizano-Hermosilla I, Alvarado JM. Best alternatives to Cronbach’s alpha reliability in realistic conditions: congeneric and asymmetrical measurements. Front Psychol. 2016;7:1–8. doi:10.3389/fpsyg.2016.00769
20. Sivertsen B, Krokstad S, Øverland S, Mykletun A. The epidemiology of insomnia: associations with physical and mental health. The HUNT-2 study. J Psychosom Res. 2009;67(2):109–116. doi:10.1016/j.jpsychores.2009.05.001
21. Sivertsen B, Pallesen S, Sand L, Hysing M. Sleep and body mass index in adolescence: results from a large population-based study of Norwegian adolescents aged 16 to 19 years. BMC Pediatr. 2014;14(1):1–11. doi:10.1186/1471-2431-14-204
22. Manzar MD, Zannat W, Kaur MHM, Hussain ME. Sleep in university students across years of university education and gender influences. Int J Adolesc Med Health. 2015;27(3):341–348. doi:10.1515/ijamh-2014-0037
23. Fernández-Mendoza J, Vela-Bueno A, Vgontzas AN, et al. Nighttime sleep and daytime functioning correlates of the insomnia complaint in young adults. J Adolesc. 2009;32(5):1059–1074. doi:10.1016/j.adolescence.2009.03.005
24. Hertenstein E, Feige B, Gmeiner T, et al. Insomnia as a predictor of mental disorders: a systematic review and meta-analysis. Sleep Med Rev. 2019;43:96–105. doi:10.1016/j.smrv.2018.10.006
25. Friedrich A, Schlarb AA. Let’s talk about sleep: a systematic review of psychological interventions to improve sleep in college students. J Sleep Res. 2018;27(1):4–22. doi:10.1111/jsr.12568
26. Sivertsen B, Vedaa Ø, Harvey AG, et al. Sleep patterns and insomnia in young adults: a national survey of Norwegian university students. J Sleep Res. 2019;28(2):e12790. doi:10.1111/jsr.12790
27. Peltzer KPS, Pengpid S. Nocturnal sleep problems among university students from 26 countries. Sleep Breath. 2015;19(2):499–508. doi:10.1007/s11325-014-1036-3
28. Alvaro PK, Roberts RM, Harris JK. A systematic review assessing bidirectionality between sleep disturbances, anxiety, and depression. Sleep. 2013;36(7):1059–1068. doi:10.5665/sleep.2810
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.