")
Back to Journals » International Journal of Nephrology and Renovascular Disease » Volume 13
Inpatient Dialysis Planning During the COVID-19 Pandemic: A Single-Center Experience and Review of the Literature
Authors Mitchell KR, Bomm A , Shea BS , Shemin D, Bayliss G
Received 1 August 2020
Accepted for publication 11 September 2020
Published 21 October 2020 Volume 2020:13 Pages 253—259
DOI https://doi.org/10.2147/IJNRD.S275075
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Pravin Singhal
Kevin R Mitchell,1– 3 Alison Bomm,3,4 Barry S Shea,2,3,5 Douglas Shemin,1– 3 George Bayliss1– 3
1Division of Kidney Diseases and Hypertension, Brown Medicine, Providence, RI, USA; 2Alpert Medical School, Brown University, Providence, RI, USA; 3Department of Medicine, Rhode Island Hospital, Providence, RI, USA; 4Department of Nursing, Rhode Island Hospital, Providence, RI, USA; 5Division of Pulmonary and Critical Care Medicine, Brown Medicine, Providence, RI, USA
Correspondence: George Bayliss APC 9, Rhode Island Hospital, 593 Eddy St, Providence, RI RI 02903, USA
Tel +1-401-444-3284
Fax +1-401-444-3283
Email [email protected]
Background: COVID-19 has created havoc in healthcare systems worldwide, including shortages in equipment and supplies for dialysis in the acute setting.
Methods: We compared our planning and experience at a tertiary care academic medical center to recommendations in the literature.
Results: Published literature and our experience underscored the need to plan for adequate dialysis equipment, particularly for continuous renal replacement therapy in the ICU setting, adequate nursing, and flexible scheduling of chronic patients to accommodate the surge in acute patients. We discovered other “shortages” not mentioned in the literature: shortages in the number of portable reverse osmosis (RO) machines needed to prepare dialysis water, inadequate number of rooms in units designated for COVID-19 patients with plumbing for dialysis, and lack of temperature blending valves on sinks that necessitated using cold water only, and damaging the RO membranes. We identified the need for cooperation between nephrology and critical care medicine, hospital-based and community nephrologists and community dialysis units as well as nephrologists at other hospitals in the region. We turned to guidance from the hospital ethics committee.
Conclusion: Planning for an expected surge in hospitalized patients requiring RRT demands coordination between critical care, dialysis and nursing services as well as community and hospital providers to make certain there are adequate dialysis resources. Our experience suggests that continuous dialysis is in greatest demand early in the illness, and that plans to increase supplies should be put in place. But, planning should also focus on unforeseen hospital-specific infrastructure shortages that can develop over time and hamper intermittent dialysis delivery to all patients who require treatment.
Keywords: dialysis, disaster, planning, coordination
Introduction
The novel coronavirus, first reported in Wuhan, China, and now identified as SARS-CoV-2, has overwhelmed healthcare systems around the world as it spread, uncovering shortcomings in supply chains for mechanical ventilators and personal protection equipment (PPE), like small particle respirator masks (N95). The virus causes significant morbidity and mortality through its effects on vascular endothelium, leading to a surge in acute kidney injury (AKI).1–3 That, in turn, has led to shortages in equipment and supplies for continuous renal replacement therapy (CRRT) and intermittent hemodialysis (IHD) as well as nurses with the specialized skills needed to run IHD acutely and chronically in and out of intensive care units.4 Literature on dialysis planning in the early days of the pandemic was scarce, focusing on disasters of the day like Hurricane Katrina (2005), the Great East Japan earthquake (2011) and Superstorm Sandy (2015). The current literature has centered more on the biology of acute kidney injury. Only as the extent of the strain on dialysis in the acute care setting became clear have nephrologists begun to develop guidelines on how to ready dialysis services for future pandemics.5 As part of its pandemic planning, Rhode Island Hospital, a 719-bed, level 1 trauma center, developed plans for re-allocating dialysis resources in the event of shortages to make certain that everyone who needed dialysis received it. Here we describe our planning and the problems that arose despite that planning. We also review recommendations in the literature and discuss the need to address unforeseen problems. The goal of this single-center review is to help other centers prepare for future increases in COVID-19 cases, whether in the form of a second wave of the pandemic6 or spikes in cases as states and nations ease restrictions on social isolation.7
Methods
In early March Rhode Island had so far avoided the catastrophic unfolding of the virus’ effects on healthcare systems in Europe and New York City, giving time to outline ways to allocate dialysis resources. The nephrology division based its response on projections by the critical care service that Rhode Island Hospital would need to perform upwards of 50 urgent sessions of dialysis per day. Meanwhile, chronic dialysis facilities in the state developed their own initial plans to respond to the appearance of the virus among patients at their facilities, including referring patients to the ED for testing and dialysis rather than chance having the infection spread through their dialysis units. This raised the possibility of additional hospital admissions for chronic dialysis patients suspected of having COVID19, further straining hospital dialysis resources. Nephology and critical care services also worked with the hospital ethics committee on triage guidelines for the care of chronic dialysis patients in the event of acute shortages of ventilators and dialysis machines for patients with COVID-19 associated acute kidney injury.
Critical Care Planning
Intensivists planned for a maximum surge of up to 200–300 critically ill COVID patients, with up to 200 needing mechanical ventilation at Rhode Island Hospital. Potential dialysis needs were based on reports of AKI occurring in up to 29% of ICU patients with COVID-19 and the need for RRT in up to 17%.8,9 These numbers are similar to prior data suggesting that 30–40% of acute respiratory distress syndrome (ARDS) patients develop AKI, with roughly half of those needing RRT. Thus, it was estimated that under a maximum surge of COVID-19 at our hospital, up to 50 patients may need RRT simultaneously.
The critical care services decided to rely on CRRT as the initial dialysis modality and the ICU nurses who were already familiar with Baxter Prisma dialysis machines and would already be caring for patients, thus reducing the need for scarce PPE. Critically ill patients would be transitioned to intermittent HD as they stabilized and neared extubation. The hospital initially had five Baxter machines and hoped to obtain more but planned to limit treatments to 8–12 hours per patient per machine to increase the number of patients who could receive treatment with prolonged intermittent RRT in the event of extreme need. Planning was further complicated when Baxter reported that due to the increase in demand for its products, it was forced to ration deliveries of its premixed Prisma dialysate and replacement fluid to 110% of a hospital’s demand over the previous six months.10 We developed an algorithm for transitioning from CRRT to IHD (Box 1). Further plans were made to reduce the amount of replacement fluid and dialysate to stretch supplies by cutting clearance to 20 mL/kg per hour from our standard 25 mL/kg per hour as well as using alternate sources, like citrate-based dialysate from compounding pharmacies or buffered crystalloid solutions like lactated Ringers as replacement fluid.
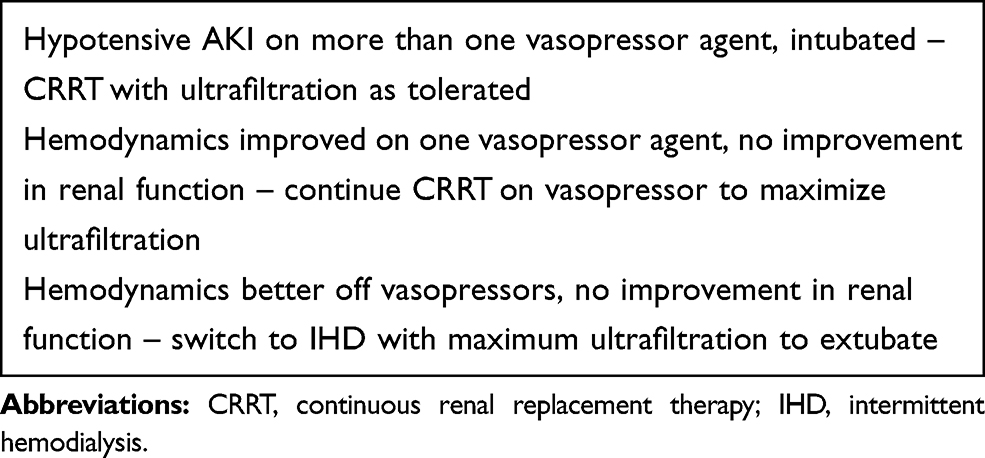 |
Box 1 Algorithm/Criteria for CRRT in Intubated COVID-19 Patients |
Intermittent acute and chronic hemodialysis planning: We designed an algorithm for allocating intermittent dialysis based largely on the number of trained dialysis nurses at the start of the pandemic (six), number of dialysis machines (18), and portable RO machines (six). The goal was to develop a tiered response to cut back on dialysis for non-critically ill patients, including chronic dialysis patients, to meet the need for all chronic and acute IHD (Table 1). In addition to limiting the time per session and number of sessions per week, we planned to dialyze patients who were positive for the coronavirus in their rooms on designated COVID-19 floors in the main hospital, away from the hospital’s inpatient dialysis unit. This required dialysis nurses to identify all the rooms in the hospital with faucets that would allow them to hook up dialysis machines and a mechanism to provide the information to bed control when assigning patients to rooms. Nurses would need to be physically present in the rooms during dialysis to monitor patients and machines.
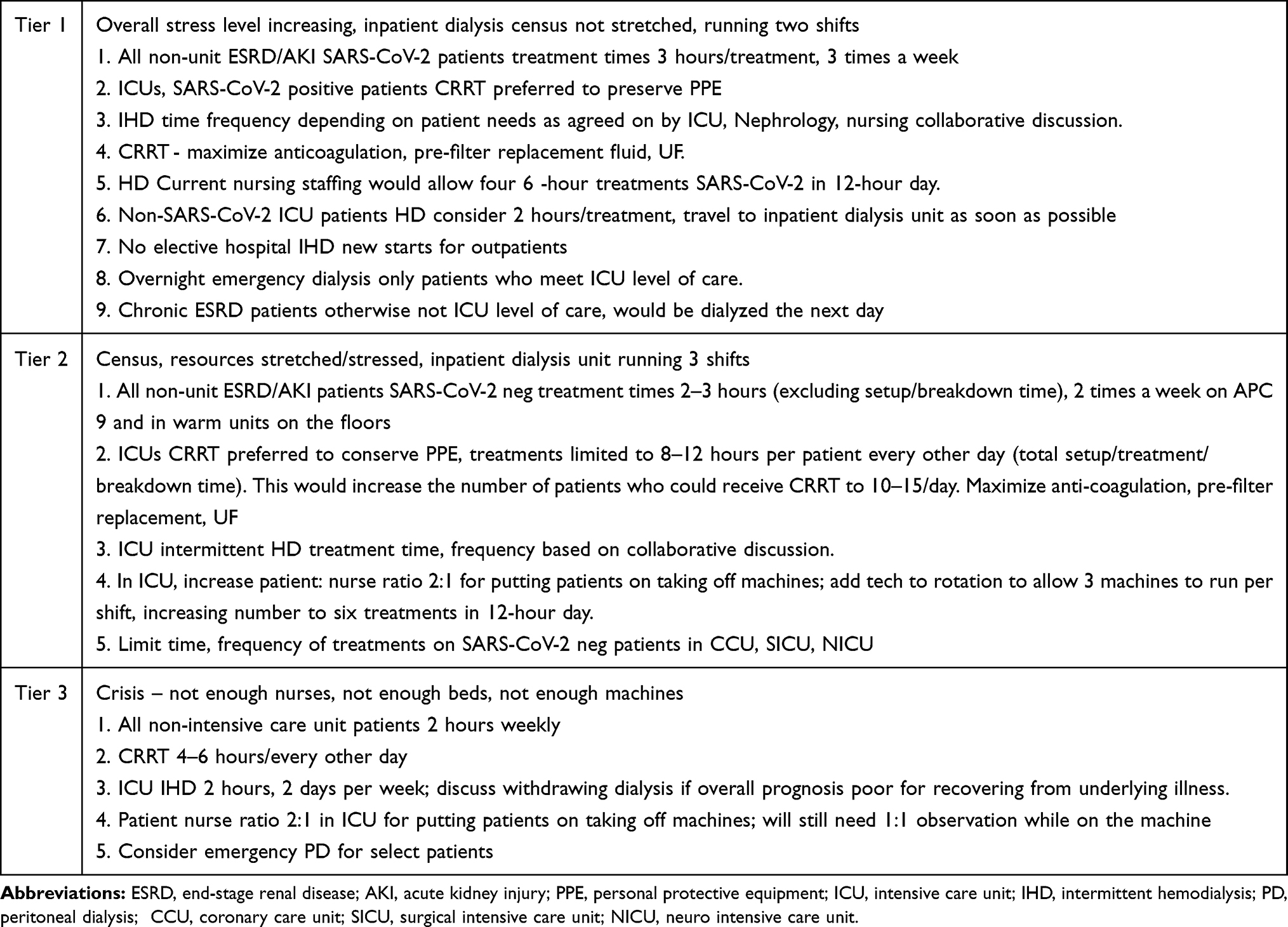 |
Table 1 Tiered Algorithm for Limiting Dialysis Treatments to Increase Resources |
To minimize potentially preventable hospital admissions, chronic dialysis patients in the hospital’s two outpatient units were encouraged to attend their regular outpatient sessions without fail since there was no way to guarantee they would get dialysis if they missed a session and presented to the ED in urgent need of dialysis.
Members of all nephrology groups credentialed at Rhode Island Hospital were asked to review and comment on the plan for rationing dialysis resources. Their concerns included the increased risk of hyperkalemia and hypervolemia that chronic ESRD patients would face from less time on dialysis and fewer sessions as well as the detrimental effects of decreased clearance. They acknowledged the need to limit exposure of nurses to infected patients and prevent staff burnout.
Ethical concerns: just as decisions would have to be made about allocation of ventilators and ICU beds, decisions would have to be made about allocation of dialysis resources in the event that the hospital’s ability to care for patients was taxed beyond its limits by SARS-CoV-2. Planning considered the hospital ethics committee guidelines on the need for allocation of critical care resources.
Results
As of June 24, Rhode Island had 16,772 positive cases, including 103 who were hospitalized, 18 in ICUs and 17 on ventilators, down from a peak of 376 hospitalized, 98 in ICUs and 62 on ventilators in late April and early May. Statewide fatalities totaled 920, of which 29% occurred in hospitals and 62% occurred in long-term care facilities.11
The number of patients requiring acute and chronic dialysis due to COVID-19 has so far amounted to 53 patients for hemodialysis with two additional patients requiring PD. At the peak some 44 patients required dialysis. Of the 30 patients with acute kidney injury requiring dialysis, 27 required CRRT initially, 22 were transitioned to hemodialysis. Five patients died before they could be transitioned off CRRT, and 15 patients died on IHD. The first 18 patients requiring CRRT experienced circuit clotting, prompting the need for an anticoagulation protocol. Eight patients experienced renal recovery, although one patient who recovered kidney function developed recurrent sepsis and subsequently died.
Among the 26 chronic ESRD patients admitted to the hospital with COVID-19, 3 required CRRT initially, and two of those patients died. A third patient died before she could be dialyzed, and a fourth patient died on intermittent HD. A failed kidney transplant patient was admitted for placement of a PD catheter and subsequently tested positive for COVID-19. A second patient on PD chronically was admitted with COVID-19 and subsequently died from complications of the disease.
Early problems identified included the shortage of Prisma machines and supplies. Consumption of Prismasate dialysate and replacement fluid increased to 3246 bags of solution in the year through May 30, 2020, from 423 bags in the same period a year earlier in the hospital’s main medical ICU. The hypercoagulability of COVID-19 patients became clear early as CRRT circuits clotted and needed to be replaced frequently. Dialysis and ICU services introduced a heparin protocol and started to rely on anti-Factor Xa levels rather than adjusted prothrombin time to judge the adequacy of anticoagulation. Prismasate supplies were rationed by decreasing replacement fluid and dialysate dosing to 20mL/kg per hour as opposed to the typical 25mL/kg per hour, excluding down time related to filter clotting. Clotting of filters was avoided by keeping anti-Factor Xa levels >0.40. Dialysis circuit heparin dose was lowered when patients were on systemic heparin with a 1000-unit priming dose and bolus of 3000 units.
Limits on time per chronic hemodialysis session and the number of sessions to two per week were imposed after a drop in the number of dialysis nurses, acutely to 4, and an increase in the need for IHD due to COVID19 patients who were no longer critically ill and required IHD rather than CRRT. While nephrologists were aware of the potential ill effects of under dialysis in all patients, nephrology fellows evaluated patients on a daily basis to assess how much dialysis they needed based on acuity, using the algorithm as a guideline rather than a fixed set of rules.
Initial concerns about an influx of chronic dialysis patients from the outpatient units eased as the operators of the state’s outpatient units (American Renal Associates, DaVita, Fresenius and Rhode Island Hospital) took steps to cohort patients with SARS-CoV-2 on separate COVID-19 shifts in line with recommendations from the Centers for Disease Control and Prevention.12 Physicians seeing patients at Rhode Island Hospital’s two outpatient units had to register with the Rhode Island Department of Health’s online registration for testing to allow nurses at the unit to place an order for outpatient SARS-CoV-2 testing at one of the state’s drive-in testing sites for any patient suspected of the having the virus.
For COVID-19 patients on IHD, high-efficiency NR250 dialysis filters were used since many patients were considered in high catabolic states. In the acute setting using membranes with the larger surface area and dialyzing 180 min per session would typically allow patients to be dialyzed every other day. Nephrology fellows assessed patients daily for volume status and clearance needs. To meet concerns about hyperkalemia, a second potassium binder, zirconium cryosilicate (Lokelma), was added to the hospital formulary to provide an alternative to sodium polystyrene sulfonate (Kayexalate), the hospital’s primary formulary binding resin, if patients could not tolerate Kayexalate. Once more COVID-19 patients requiring IHD were transferred to the general medical floors from the ICUs, a shortage of rooms with appropriate plumbing appeared. With a drop in the number of COVID-19 patients requiring ICU level of care, 2 rooms in one of the secondary ICUs – a surgical step-down unit – were repurposed into satellite dialysis units since these rooms were already specifically plumbed for dialysis. The dialysis unit had to purchase more portable RO machines and increase repairs of existing ones due to accelerated deterioration of the membranes as evidenced by increased bacterial colony counts and endotoxin levels in the water. That problem was due in part to a lack of temperature controls on faucets, requiring the use of cold water only. The hospital has since retrofitted faucets to allow RO machines to be hooked up in all rooms in potential “warm (COVID-19) units” and identified rooms already plumbed for dialysis that will be set aside as satellite dialysis units in the main hospital building for COVID-19 patients outside of the ICUs requiring intermittent hemodialysis.
Ethical Considerations
The nephrology service took the position that access to dialysis is like access to any other lifesaving therapy during a crisis and that the same standards that apply to access to ventilators must apply to access to dialysis. The service sought to design policies in line with those drafted by the Rhode Island Hospital Ethics Committee and spelled out in the RI Department of Health Crisis Standards of Care: duty to care, duty to steward resources, consistency, fairness, transparency, proportionality, accountability. End-stage renal disease with hemodialysis dependency has been included in the criteria for excluding patients from lifesaving measures in the event of extreme shortage.13 Data from patients with SARS-CoV-1 and ESRD suggested poor outcomes from infection with that coronavirus variant.14 Early data from Spain suggested that ESRD patients there with COVID-19 also did poorly.15 We observed a relatively low rate of deaths among ESRD patients admitted with COVID-19 compared to patients with acute kidney injury who subsequently required dialysis. There were no emergency ethics consults related to access to dialysis due to shortages related to COVID-19, according to the head of the hospital ethics committee.
Dialysis was not diverted from patients without COVID-19 who needed it. The hospital continued to perform deceased donor kidney transplants since those are considered essential surgery by CMS and the transplant community.16,17 One concern was the risk of delayed graft function requiring dialysis, reported as high as 43.5% in some studies.18 The dialysis service provided IHD to four patients post-transplant as needed (out of a total of 12 deceased donor kidney transplants during the worst of the pandemic through May). At the same time, the transplant service made efforts to make certain that patients were dialyzed at their outpatient units before they were called in for a transplant to minimize the need for immediate dialysis in the event of DGF and by being selective in which potential recipients were called in and which organs were accepted.
The number of patients needing hospital dialysis emergently overnight dropped. The no-show rate at the hospital’s two outpatient units dropped to 3.6% in the first four weeks of April from 5.3% in February, before the pandemic struck, and 4.5% in April 2019. It dropped to 3.5% in May from 4.5% in May 2019. In the period March through June 2020, only 4 people were admitted to the hospital emergently for dialysis because they missed their outpatient session compared to 14 people in March through June 2019. It is not possible to say whether the drop was because nephrologists had warned people not to skip dialysis; admissions overall to the hospital were down in March–June 2020 compared to March–June 2019. The hospital’s two outpatient dialysis units had 2 people per week dialyzing on a separate COVID-19 outpatient shift in mid-April, increasing to 7 per week at the peak in late May before dropping to 0 in late June.
Efforts to hire more dialysis nurses resulted in several experienced dialysis nurses joining the hospital staff over the summer.
Discussion
At the beginning of the crisis in March, there was a lack of information on how to plan for potential shortages in dialysis. But the need for such planning became glaringly clear as shortages of dialysis services became significant worldwide.19
The American Society of Nephrology recently published its recommendations on managing dialysis resources during contingency planning pre-crisis20 while other centers began sharing their experience with dialysis rationing.21 The ASN’s “practical ideas for increasing dialysis surge capacity” included fluid restriction, use of potassium binding resins, and “total nephron blockade” to increase urine output; limiting intermittent dialysis times to 3 hours, twice weekly (Monday–Thursday; Tuesday–Friday; Wednesday–Saturday). They also provided a “recipe” for creating one’s own replacement fluid with NS, D5%, KCl as needed, NaHCO3, MgCl2 and CaCl2; as well as recommendations for sustained low-efficiency dialysis and prolonged intermittent renal replacement (PIRRT) for 8–12 hours at a higher clearance of 40–50 mL/kg per hour. There are little data on short-term outcomes with reduced frequency of dialysis,22 and it is usually discussed as an option in resource-poor settings.23
Others have suggested peritoneal dialysis as an alternative to HD during periods of resource stress. Again, the subject has been discussed in the context of expanding dialysis resources where poverty is the main driver of scarcity.24 In terms of crisis, nephrologists at New York’s Mount Sinai Hospital described their experience in putting together an acute PD service to meet the overwhelming need for renal replacement.25 We have discussed the possibility of using urgent start PD in select patients with AKI who were stable and out the ICU. Urgent start PD would be used if access to intermittent hemodialysis became stretched to the point that we would not be able to provide dialysis to all who needed it outside of the critical care setting. Our surgeons and interventional radiologists have offered to place PD catheters. But use would be limited in part by the limited number of nurses trained in PD on the floors.
Our PD experience during the pandemic was limited to one patient returning to PD after transplant failure and a second patient chronically on PD admitted with respiratory failure. The patient returning to PD was hospitalized to start PD because the outpatient PD unit had been closed due to several of the staff testing positive for the novel coronavirus. Her COVID-19 diagnosis was made coincidentally after she was admitted for catheter placement. She did ambulatory PD without difficulty and was discharged home. The patient on chronic PD was admitted in respiratory distress and COVID-19-associated acute respiratory distress syndrome. He continued PD and, despite efforts to increase ultrafiltration to remove volume, ultimately died of respiratory failure after his family elected to end aggressive care.
Rhode Island Hospital’s planning has been driven by an expected surge in the number of patients requiring dialysis that exceeded the hospital’s usual capacity to dialyze chronic and acute patients. To date, we have not seen the expected rise in acute patients or experienced a surge in chronic patients with COVID-19 requiring dialysis. But our plan has been tested in other ways as unforeseen shortages arose. This review is limited by being the experience of a single center. Rhode Island has been hard hit by the coronavirus pandemic, but many of the deaths have been in long-term care facilities and not in hospitals (62% versus 29%).10
Since many experts expect a second wave of the virus to strike in the fall and winter, there may still be a need to put our plan into place in full, including severe rationing of dialysis. Our experience so far has shown: an increased need for CRRT early with transition to IHD as the disease runs its course in patients and the community; an ongoing need to evaluate patients on a daily basis to assess their need for dialysis and deployment of nursing resources early; emergency access to rooms with adequate plumbing for dialysis in “warm” units and establishment of satellite dialysis units in COVID-19 areas specifically plumbed for dialysis; adequate supplies from dialysis machines to dialysate and replacement fluids and portable RO machines; contingency plans for emergency PD in cooperation with surgeons and radiology in event of extreme need. We have increased supplies for CRRT and plan to be able to provide adequate clearance to all patients who require CRRT of 25 mL/kg per hour.
The shortage of dialysis nurses is a chronic one, not limited to Rhode Island. There is a need to recognize the uncertainty nurses face as they spend considerable time at the bedside during dialysis with patients infected with the virus.26
Cooperation with outpatient dialysis units is essential to make certain patients do not miss sessions and understand the potential implications for their health if they do. Rhode Island Hospital warned other hospitals in the region about possible limits on transfers if dialysis resources were strapped. The Korean Society of Nephrology and Korea Society of Dialysis recently published their recommendations on preventing secondary transmission of the virus among chronic hemodialysis patients, including “interhospital transfer is basically prohibited during outbreak.”27 We have shared our experience with nephrologists at other hospitals in and near Rhode Island to see if we can develop a regional response to critical dialysis needs.
Conclusion
Our experience demonstrates that the need to plan allocation of potentially scare dialysis resources during the COVID-19 pandemic. Such planning has required collaboration between nephrology and intensive care services to identify potential needs; cooperation between hospital and community nephrologists to develop a plan for allocation of resources; cooperation with outpatient dialysis units to maintain safe dialysis operations in the community and limit the need for emergency hospital dialysis from preventable admissions. Identification and correction of structural limits to dialysis within the hospital required ongoing open communication with the hospital administration and infection control experts.
Author Contributions
All authors made substantial contributions to conception and design, acquisition of data, analysis and interpretation of data; took part in drafting the article and revising it critically for important intellectual content; agreed on the journal to which the article will be submitted; gave final approval of the version to be published; and agree to be accountable for all aspects of the work.
Disclosure
The authors confirm that they have no conflicts of interest and that the contents of this paper have not been published elsewhere in full or in abstract form.
References
1. Cheng Y, Luo R, Wang K, et al. Kidney disease is associated with in-hospital death of patients with COVID-19. Kidney Int. 2020;97:829–838. doi:10.1016/j.kint.2020.03.005
2. Pei G, Zhang Z, Peng J, et al. Renal involvement and early prognosis in patients with COVID-19 pneumonia. J Am Soc Nephrol. 2020;
3. Han H, Yang L, Liu R, et al. Prominent changes in blood coagulation of patients with SARS-CoV-2 infection. Clin Chem Lab Med. 2020;58:1116–1120. doi:10.1515/cclm-2020-0188
4. Goldfarb DS, Benstein JA, Zhdanova O, et al. Impending shortages of kidney replacement therapy for COVID-19 patients. CJASN. 2020;15:880–882. doi:10.2215/CJN.05180420
5. Division of Nephrology, Columbia University Vagelos College of Physicians. Disaster responses to the COVID-19 pandemic for patients with kidney disease in New York City. JASN. 2020;31:1372–1379.
6. Maxouris C. US could be in for “a bad fall and a bad winter” if it’s unprepared for a second wave of corona virus, Fauci warns. CNN Health. 2020. https://www.cnn.com/2020/04/29/health/us-coronavirus-wednesday/index.html.
7. Pence M. There isn’t a Coronavirus “second wave.”. Wall Street J. 2020. Available from: https://wsj.com/articles/there-isn't-a-coronavirus-second-wave-11592327890. Accessed October 11, 2020.
8. Yang X, Yu Y, Xu J, et al. Clinical course and outcomes of critically ill patients with SARS-CoV-2 pneumonia in Wuhan, Chine: a single-centered retrospective, observational study. Lancet Respir Med. 2020;
9. Guan WJ, Ni ZY, Liang WH, et al. Clinical characteristics of coronavirus disease 2019 in China. New England J Med. 2020;382:1708–1720. doi:10.1056/NEJMoa2002032
10. Knight HL and Cambell G. Protective allocation letter. March 25, 2020. Available from: https://www.nutritioncare.org/uploadedFiles/Documents/Guidelines_and_Clinical_Resources/COVID-19/Protective%20Allocation%20Letter%USHP%20Renal%20032420%20FINAL.pdf. Accessed October 11, 2020.
11. Rhode Island department of health COVID-19 data tracker. Available from: https://ri-department-of-health-covid-19-data-rihealth.hub.arcgis.com/.
12. https://www.cdc.gov/coronavirus/2019-ncov/hcp/dialysis/screening.html.
13. Rhode Island department of health. Crisis standards of care guidelines. https://health.ri.gov/publications/guidelines/crisis-standards-of-care.pdf.
14. Kwan BC, Leung C, Szeto C, et al. Severe acute respiratory syndrome in dialysis patients. J Am Soc Nephrol. 2004;15:1883–1888. doi:10.1097/01.ASN.0000131522.16404.1F
15. Goicoechea M, Sanchez Camara LA, Macias N, et al. COVID-19: clinic course and outcomes of 36 hemodialysis patients in Spain. Kidney Int. 2020;98:27–34. doi:10.1016/j.kint.2020.04.031
16. American Society of Transplant Surgeons. Transplant capacity and testing in the COVID-19 era. Available from: https://asts.org/advocacy/covid-19-resources/asts-covid-19-strike-force/transplant-capacity-and-testing#.XqyAX55Khpg.
17. CMS issues COVID-19 guidance to health care providers. Available from: https://unos.org/news/cms-issues-covid-19-guidance-to-health-care-providers/.
18. Bahl D, Haddad Z, Datoo A, Qazi YA. Delayed graft function in kidney transplantation. Current Opin Organ Transplant. 2019;24:82–86. doi:10.1097/MOT.0000000000000604
19. Kulish N. A Life and Death Battle: 4 Days of Kidney Failure but No Dialysis. The New York Times; 2020 May 1. Available from: nytimes.com/2020/05/01/health/coronavirus-dialysis-death.html. Accessed Oct. 11, 2020
20. Burgner A, Ikizler TA, Dweyer JP. COVID-19 and the inpatient dialysis unit. CJASN. 2020;15:720–722, 2020. doi: 10.2215/CJN.03750320
21. Gallieni M, Sabiu G, Scorza D. Delivering safe and effective hemodialysis in patients with suspected on confirmed COVID-19 infection: a single-center perspective from Italy. Kidney. 2020. 360. doi:10.34067/KID.0001782020
22. MeyerTW, HostetterTH, WatnickS. Twice-weekly hemodialysis is an option for many patients in times of dialysis unit stress. JASN. 2020;31:ccc–ccc. doi:10.1681/ASN.2020030361
23. Savla D, Chertow GM, Meyer T, Anand S. Can twice weekly hemodialysis expand access under resource constraints? Hemodial Int. 2017;21:445–452. doi:10.1111/hdi.12501
24. Niang A, Iyengar A, Luyckx VA. Hemodialysis versus peritoneal dialysis in resource limited settings. Curr Opin Nephrol Hyertens. 2018;27:463–471. doi:10.1097/MNH.0000000000000455
25. El Shamy O, Patel N, Abdelbaset MH, et al. Acute state peritoneal dialysis during the COVID-19 pandemic: outcomes and experiences. JASN. 2020;31:1680–1682. doi:10.1681/ASN.2020050599;.
26. Harwood L. Pandemic uncertainty: considerations for nephrology nurses. Nephrology Nursing J. 2020;47(2):127–130. doi:10.37526/1526-744X.2020.47.2.127
27. Cho JH, Kang SH, Park HC, et al. Hemodialysis with cohort isolation to prevent secondary transmission during a COVID-19 outbreak in Korea. JASN. 2020;31:1398–1408. doi:10.1681/ASN.2020040461
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.