")
Back to Archived Journals » Innovation and Entrepreneurship in Health » Volume 2
Innovations in the design of mental health services for young people: an Australian perspective
Authors McGorry P
Received 18 May 2015
Accepted for publication 15 July 2015
Published 14 December 2015 Volume 2015:2 Pages 107—113
DOI https://doi.org/10.2147/IEH.S68179
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 5
Editor who approved publication: Professor Rubin Pillay
Patrick D McGorry
Orygen, The National Centre of Excellence in Youth Mental Health, Parkville, VIC, Australia
Abstract: Youth mental health reform has become a major growth point in mental health reform in Australia and in several other countries internationally. This is based on a growing appreciation of the epidemiological data, new knowledge of the developmental changes during the transition to adulthood, growing concern from parents and young people themselves at the neglect of their major health needs during this stage of life, and, perhaps decisively, the economic imperatives. Young people on the threshold of productive life are not realizing their full potential owing to the impact of untreated or poorly treated mental ill-health on their psychosocial, educational, and vocational development. Yet this issue, while of obvious importance to societies around the world, has only come to the fore through entrepreneurial and reform-oriented thinking within the mental health field in a number of regions of the world. Such thinking has been embraced by policymakers in some societies and by the general public; however, it has been challenged and resisted by sections of the mental health profession. It is of equal importance to understand the sociology of such a reform process as to assemble the evidence and know-how to engineer and evolve the reform itself. This paper describes our experience in conceptualizing, designing, advocating for, and guiding such reform in Australia, aspects of which have now been adopted in other jurisdictions, notably Ireland, the UK, and Canada.
Keywords: youth mental health, early intervention, pre-emptive psychiatry, service reform, clinical staging, psychosocial development
Introduction
While mental health issues are the key health concern for young people today, contributing 45% of the total burden of disease for those aged between 10 and 24 years,1 adolescents and young adults have the poorest access to mental health care of all ages across the life span. For example, the most recently available Australian data showed that in 2008 only 13% of young men aged between 16 and 24 years with a mental health issue had accessed professional help, with this figure increasing to approximately 30% for young women.2 Other large-scale studies, such as the US National Comorbidity Survey Adolescent Supplement,3 have shown similar results. Investigation of the epidemiology and age of onset of the major mental disorders has shown that the number of new cases peaks in late adolescence/early adulthood, with 75% of all new onsets appearing before the age of 25 years.4 Because this peak occurs during the critical developmental window of emerging adulthood5 and subsequently impacts the most productive years of adult life, the World Economic Forum has recently calculated that among all the noncommunicable diseases, mental illness poses the greatest threat to worldwide gross domestic product over the next 20 years, clearly surpassing cancer and rivaling even cardiovascular disease.6
Despite these statistics indicating their need for mental health care, young people have poor access to, and engagement with, primary and specialist mental health care. They are notably reluctant to seek help for emotional concerns from mainstream health services.7,8 There are many reasons for this, but one of the key barriers is the structure and culture of our existing health services. Our primary care services are largely geared to catering for physical ill-health, and because young children and older adults bear most of the physical health burden, their needs are considered first in the design of these services. Consequently, they are typically alienating, or at best “off-key”, to young people, who fail to engage.9
Young people and their families who seek help from the specialist mental health system face an even more difficult situation. This is primarily the result of poor resourcing and inappropriate system design. Young people’s complex and evolving symptom profiles often do not meet the narrow criteria required for acceptance, particularly into an adult service, despite the significant distress and impairment they experience.9 This is because the adult services are designed around the needs of older adults with well-established illness, while the child and adolescent services largely focus on the needs of younger children within their family, educational, and social contexts, with an artificially imposed age cutoff of 18 years.10 This represents a fatal design flaw, not only because of the differences in their culture, focus, and therapeutic approach, but also because the discontinuity falls right within the age range where the incidence of new onsets peaks,11 rendering the system weakest where it should be strongest. Furthermore, transitions from one “system” to the next are hugely problematic, with many falling between the cracks.
The need for system reform
Fundamental system reform is urgently required to improve young people’s access to mental health care, as well as the quality and continuity of the care they receive. A specific service stream able to accommodate the unique clinical, developmental, and psychosocial needs of young people is appropriate for two major reasons: firstly, young people in the early stages of a mental illness tend to present with blends of comorbidities of variable intensity and stability, particularly substance abuse and challenging personality traits, which require an integrated model of care.9 Services that acknowledge these complex and evolving patterns of morbidity and symptomatic fluidity and that are able to manage them appropriately and sensitively are necessary. Secondly, developmentally appropriate approaches are essential for the management of emerging disorders; young people’s individual and group identity and understanding of their social world needs to be central to any service model.12,13 Practically, this means creating a new youth mental health model that links with, but is separate in culture, skills, and expertise from, systems for younger children and older adults.14 This type of model tackles the issues of poor access to, and engagement with, care and the difficult transition between the current service streams15 and has the potential to overcome these major flaws in our existing system. The key principles and features of youth mental health services are summarized in Figure 1. Ideally, to respond to the high incidence and prevalence of mental health issues in young people, different service levels that cover the full spectrum, complexity, and severity of illness are required, including e-health, primary care or enhanced primary care services for those with mild to moderate mental health issues, through to more specialized services for those with complex and more severe forms of illness.16
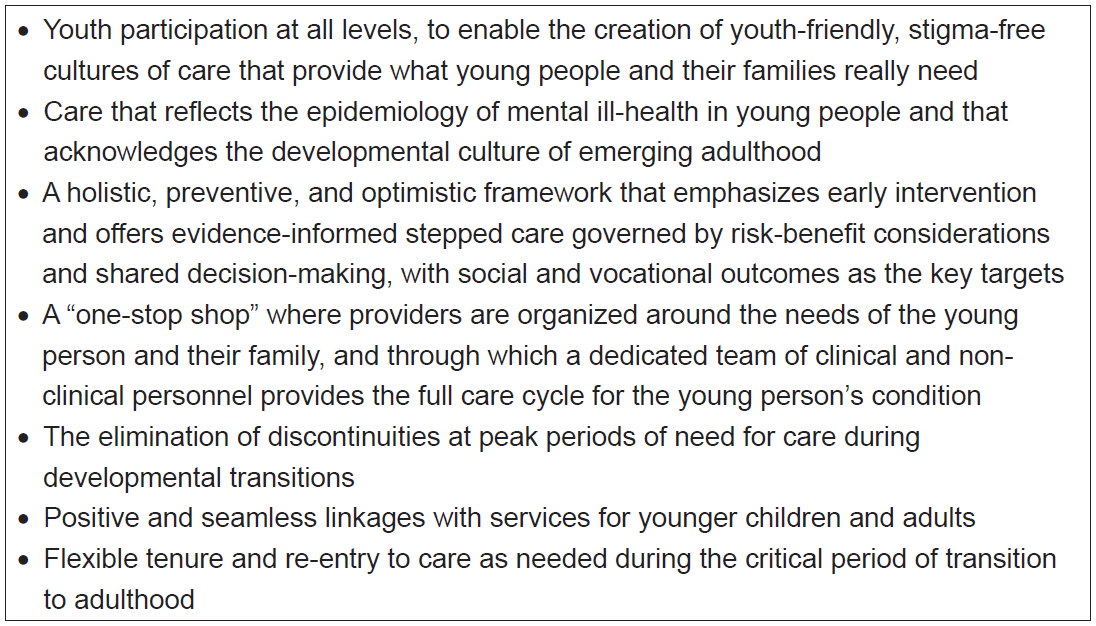 | Figure 1 Key principles for youth mental health services. |
Although more than 50% of young people will experience mental ill-health during the transition to adulthood,12,17–19 much of this mental ill-health is mild to moderate in nature. For many young people, these issues tend to resolve by the late 20s.19 However, if left untreated and unsupported, even short-lived or moderate mental ill-health typically comes with a substantial cost to the young person, in terms of poor social functioning, underachievement, and educational or vocational failure, as well as a significant risk of persistence, self-harm, or even premature death. The argument that illness can resolve as young people mature is not a valid reason to fail to provide safe, secure care that is appropriate to the stage of illness throughout the period of need. Physical ill-health, such as asthma, in young people is readily treated, even though it too often resolves over time. Furthermore, for the not insignificant proportion of young people whose mental health issues do not in fact resolve with time but persist and/or worsen, compelling evidence demonstrates that persistent mental health problems in adolescence significantly increase the risk of mental illness in adulthood.9,17–19 It is this risk that underpins the momentum for early intervention, with the ultimate aim of preempting and preventing the emergence of serious and enduring illness.
The complexity and relative nonspecificity of young peoples’ symptom profiles mean that different treatment approaches are required than those for full-threshold illness. Simpler and safer forms of intervention are the first step, and they need to be tailored to the early stages of illness, and aim to be preemptive, with a strong preventive focus. This sits comfortably within a clinical staging approach, which differentiates earlier and milder clinical phenomena from those that accompany illness extension and progression, and thus enables an agnostic, rather than a traditional diagnostic approach to treatment, at least in the early stages of illness.20 Here, it is the persistence of symptoms, distress, and functional impairment, as well as the risk or reality of comorbid alcohol and substance abuse21 and self-harm and suicidal ideation22 that indicate a need for care, both on immediate clinical grounds as well as the risk of progression of illness.9 This explicit acknowledgment of the early stages of illness and need for care provides a more clinically useful framework than other diagnostic reforms. Clinical staging is sensitive and tied to risk/benefit considerations and facilitates the selection of safer interventions early on. It may have particular relevance in the context of youth mental health, where the onset of mental ill-health and illness is most common, and full-threshold syndromes according to traditional systems of diagnosis are often not yet apparent, even though the need for care is.12
New models for youth mental health care
Care for the majority of young people is perhaps best provided in the context of stigma-free, youth-friendly primary or enhanced primary care structures; while those with more severe or established illness need more rapid and direct access to specialized youth mental health services. Over the last few years, reform in the delivery of youth mental health services has been gaining ground, inspired in no small part by the success of the early psychosis movement and its service reforms.12,13,16,23–26 In a groundbreaking first step in youth mental health, in 2006 the Australian Federal Government established headspace, the National Youth Mental Health Foundation, which was tasked with devising and building a national youth mental health service stream designed to provide highly accessible, youth-friendly centers that promote and support early intervention for mental and substance use disorders in young people.27 Each center is operated by an independent local consortium of service providers, commissioned through and contracted with the headspace national office, based in Melbourne. Each headspace center functions as an integrated, multidisciplinary practice that provides four core service streams: mental health, drug and alcohol services, primary care (general health, sexual health), and vocational/educational assistance, with a mix of staff that comprises medical, nursing, allied health, and specialist practitioners. Other needs are met through referral to linked agencies, which are often represented in the local consortium, such as specialist mental health and housing services. This welcoming and holistic “one-stop shop” venue aims to minimize the stigma often associated with traditional and specialist mental health services, and to provide clear and accessible pathways to a range of local services relevant to young people.27 The therapeutic approach centers on brief psychosocial interventions, which are used as first-line therapy with the aim of preventing the development of sustained illness (for example, Parker et al).28 Medication is used as an additive or second-line therapy, and only if the young person does not respond to initial psychosocial interventions, or presents at the outset with more severe symptoms and/or high levels of risk. This stepped care model ensures that care is safe and linked to the actual stage of illness, and offers a preemptive approach to therapeutic intervention. In addition to the current 74 walk-in centers available around the country, headspace also runs a nationwide online support service (eheadspace; http://www.eheadspace.org.au) where young people can talk with a mental health professional either online or by telephone and access assessment and therapeutic care, and headspace school support, a suicide postvention program for schools affected by the suicide of a student.
The majority of the young people using headspace services, even when highly distressed, are experiencing mild to moderate levels of mental ill-health and are in the early stages of illness; however, at most headspace sites, there is also a substantial subset of young people with more complex, severe, and enduring problems, who currently are unable to gain access to the traditional child and adolescent mental health services (CAMHS)/adult system.29 To begin to address this need, in 2011 the Australian Government funded the creation of up to nine “enhanced headspace” services, which are now beginning to deliver evidence-based early psychosis services, offering early detection, acute care during an initial psychotic episode, and recovery-focused continuing care featuring multimodal interventions to support the young person (and their family) to maintain or regain their social, academic, and/or career trajectory during the critical first 2–5 years following the onset of a psychotic illness.30 The first of these enhanced services (known as hYEPPs or headspace Youth Early Psychosis Programs) commenced operation in 2013, embedded with clusters of headspace centers at a regional level and drawing on their links with locally available services. It is hoped that they will ultimately be expanded to cover not only all headspace communities, but also the full diagnostic spectrum in young people with any severe mental illness.
A comprehensive sample of 22,000 young people assessed by headspace nationally revealed that headspace appears to be successfully addressing the issues of access and engagement,29 a conclusion further evidenced by the heavy demand for eheadspace services from across the nation. However, headspace is still a work in progress. Important gaps remain, notably the fact that more than half of the Australian community is not yet covered, as the current level of funding does not yet allow full national coverage. Furthermore, access rates for young men, some ethnic populations, and young adults, while improved, are still too low, and the program does not yet adequately cover those with serious mental illness. More specialized care for the more complex subset of young people who can access care via the headspace portal is also an urgent funding priority.
The long-term aim of these reforms is to develop a nationwide youth mental health stream of care that fully integrates care for young people with other service systems; notably education, employment, housing, and justice, in order to provide a seamless coverage of mental health care from puberty to mature adulthood at around 25 years of age, with soft transitions with child and adult mental health care and links with other mainstream services as appropriate. This system acknowledges biopsychosocial development and recognizes the complexity and challenges faced by young people as they become independent adults, as well as the burden of disease imposed on this age group by poor mental health. In fact, with its multidisciplinary approach, it also deliberately seeks to blur the distinctions between traditionally separate tiers of primary and specialist care, including some aspects of acute care, in recognition of the complexity of the presentation of much of the mental ill-health apparent in young people, allowing a flexible and appropriate response for each individual, depending on their own unique needs.
The Australian National Mental Health Commission, in its 2013 Report Card on National Mental Health and Suicide Prevention,31 has explicitly recommended that “national, systematic and adequately funded early intervention approaches must remain [but that] this must be accompanied by robust evaluation to support investment decisions, with a focus on implementation, outcomes and accountability”. Clearly, the success of Australia’s reforms will ultimately only be able to be determined after careful and repeated evaluation, and evidently more high-grade health services research is necessary to develop, refine, adapt, and evaluate this new service model. An independent evaluation has just been completed, and this will no doubt inform the further evolution of the headspace model. However, the indications are that the model is justified, not only purely on the grounds of the significant improvement it offers in terms of access to care, which has been acknowledged by policymakers both nationally and internationally, but also indications of early benefit for the majority of patients.32,33 Similar youth mental health models, based on the headspace approach, have now been implemented in other countries, such as the UK,13 Ireland,13 Denmark, and Singapore,25,26 and are proposed for Canada, the United States, and Israel. These various services have been adapted to their local contexts and offer somewhat different models of care to headspace, but all have in common the key principles of youth-focused, multidisciplinary comprehensive care in a stigma-free, community-based center.
The challenge of change: achieving transformational reform
The process of initiating and sustaining these reforms in youth mental health shares some characteristics with the earlier wave of reform in early psychosis. Here, innovative and entrepreneurial thinking have provided proof of their value in mental health care, with the successful evidence-informed upscaling of early intervention in psychosis, now available in specialized services across hundreds of locations and numerous national health systems.34–38 This thinking has inspired the development of new youth mental health models with the potential to create significant savings, in terms of both human suffering and economic costs to society.13
However, psychiatry and the mental health field more generally remains conservative, and entrepreneurial thinking, even when committed to the principles of evidence-informed health care, is often viewed with suspicion. This is to a large extent due to our historical legacy. Psychiatry and the mental health field more generally have been characterized by immunity to reform from the 19th century through to the late 20th century. The asylum era and psychoanalysis were 19th century ideas that threw a heavy shadow over reform. We also witnessed a series of “great and desperate cures”, which, guided by enthusiasm more than evidence, took the field down some dark pathways and harmed many patients. The current status quo, which is narrow and under pressure, reacts badly to change, and this is even more so since deinstitutionalization, which general consensus considers as largely botched, short-changing patients and society as a whole. We do have a way forward at the macro level, but we need to overcome a number of genuine obstacles.
The current reality is that despite its much greater projected impact on human suffering and productivity over the next 20 years, mental health continues to be seriously underfunded in comparison with cancer, cardiovascular disease, diabetes, and other noncommunicable diseases. As health expenditure continues to rise worldwide, we must increasingly consider our spending priorities and channel future health funding into those areas that will benefit people and society the most. This will require a reorganization of our health care system that makes value – defined as the best outcomes for clients for the lowest cost – the overarching goal.39 Since approaches that deliver better mental health are best positioned to deliver value at a lower cost than other health expenditures, these should be strongly prioritized. This means affirmative action and preferential investment in mental health care.9 Obvious priorities in this area that will produce health gain and value include achievable prevention targeting younger children and parenting, and early intervention strategies for emerging mental ill-health in children and especially in young people. Mental health care needs to shift its focus from our historical, and largely palliative, approach to care to a more preemptive and preventive focus to enable the greatest potential public health gains.
How can this be achieved? The first step is to respect and nurture innovation and the entrepreneurial spirit. Innovation is a vital ingredient if we are to dispel the current largely palliative mindset in mental health care. Innovation encompasses new thinking, new treatments, and new service models, all of which we desperately need. It is driven by a genuine need for change and requires creativity, reasonable evidence, independent champions, and substantial public involvement to enable new resources and systems of care to be developed and implemented. The establishment of headspace is an example of this process: it was inspired by the need for change, designed and championed by a group of clinician scientists and translational researchers, demanded by the public, and progressively funded by the Australian Government. The scaling up literature,40,41 again a body of knowledge that cuts across many fields of endeavor, bears witness to the key elements that are required for success in achieving transformational reform. There are often serious threats and resistance to such reform. “Merchants of doubt”42 representing vested interests may undermine the credibility of reform and reformers, and need to be recognized and responded to. Issues of power and control may overwhelm or even derail the original objectives of the reforms. Innovation in health care is hard won and too often fragile. Mental health needs innovation more than any other area at a number of levels; the youth mental health reforms represent green shoots that must be carefully nurtured.
Conclusion
The best opportunity for obtaining real benefits in mental health care lies in system reform based on the principles of early intervention and a priority focus on the developmental period of greatest need and capacity to benefit from investment, emerging adulthood. This by no means argues against investments in earlier or later life stage care, which are also essential. Indeed, international health and welfare organizations such as the World Health Organization43 and United Nations Children’s Fund44 recommend a strong focus on adolescent health, including mental health, and the provision of adolescent-friendly health services as necessary for future development and prosperity. A number of leaders, policymakers, and service developers are now working together to create international momentum to address the mental health needs of young people and their families (http://www.iaymh.org/). The arguments for this type of transformational reform are resonating strongly with the community and with policymakers, and it is hoped that the 21st century clinical infrastructure and cultures of care, such as headspace, that result from these efforts will be able to reduce the lifelong impact of mental ill-health on our health, happiness, and prosperity over the next two decades and on into the future.
Disclosure
Professor McGorry is the Executive Director of Orygen, the National Centre of Excellence in Youth Mental Health. He played a leading role in the design and establishment of headspace, the National Youth Mental Health Foundation, and is currently the Director of the headspace Board. The author reports no other conflicts of interest in this work.
References
Gore FM, Bloem PJ, Patton GC, et al. Global burden of disease in young people aged 10–24 years: a systematic analysis. Lancet. 2011; 377(9783):2093–2102. | |
Slade T, Johnston A, Teesson M, et al. The Mental Health of Australians 2: Report on the 2007 National Survey of Mental Health and Wellbeing. Canberra, Australia: Department of Health and Ageing; 2009. | |
Merikangas KR, He JP, Burstein M, et al. Service utilization for lifetime mental disorders in US adolescents: results of the National Comorbidity Survey-Adolescent Supplement (NCS-A). J Am Acad Child Adolesc Psychiatry. 2011;50(1):32–45. | |
Kessler RC, Berglund P, Demler O, Jin R, Merikangas KR, Walters EE. Lifetime prevalence and age-of-onset distributions of DSM-IV disorders in the National Comorbidity Survey Replication. Arch Gen Psychiatry. 2005;62(6):593–602. | |
Arnett JJ. Emerging Adulthood. The Winding Road from the Late Teens through the Twenties. New York, NY: Oxford University Press; 2004. | |
Bloom DE, Cafiero ET, Jane-Llopis E, et al. The Global Economic Burden of Non-communicable Disease. Geneva, Switzerland: World Economic Forum; 2011. | |
Patton GC, Hetrick SE, McGorry P. Service responses for youth onset mental disorders. Curr Opin Psychiatry. 2007;20(4):319–324. | |
Rickwood DJ, Deane FP, Wilson CJ. When and how do young people seek professional help for mental health problems? Med J Aust. 2007;187(7 Suppl):S35–S39. | |
McGorry PD, Purcell R, Hickie IB, Jorm AF. Investing in youth mental health is a best buy. Med J Aust. 2007;187(Suppl 7):S5–S7. | |
Patel V, Flisher AJ, Hetrick S, McGorry P. Mental health of young people: a global public health challenge. Lancet. 2007;369(9569):1302–1313. | |
McGorry PD, Purcell R, Goldstone S, Amminger GP. Age of onset and timing of treatment for mental and substance use disorders: implications for preventive intervention strategies and models of care. Curr Opin Psychiatry. 2011;24(4):301–306. | |
McGorry PD. The specialist youth mental health model: strengthening the weakest link in the public mental health system. Med J Aust. 2007;187(7 Suppl):S53–S56. | |
McGorry PD, Bates T, Birchwood M. Designing youth mental health services for the 21st century: examples from Australia, Ireland and the UK. Br J Psychiatry. 2013;202:s30–s40. | |
McGorry P. Should youth mental health become a specialty in its own right? Yes. BMJ. 2009;339:b3373. | |
Singh SP, Paul M, Ford T, et al. Process, outcome and experience of transition from child to adult mental healthcare: multiperspective study. Br J Psychiatry. 2010;197(4):305–312. | |
Purcell R, Goldstone S, Moran J, et al. Toward a twenty-first century approach to youth mental health care: some Australian initiatives. Int J Mental Health. 2011;40(2):72–87. | |
Copeland W, Shanahan L, Costello EJ, Angold A. Cumulative prevalence of psychiatric disorders by young adulthood: a prospective cohort analysis from the Great Smoky Mountains Study. J Am Acad Child Adolesc Psychiatry. 2011;50(3):252–261. | |
Gibb SJ, Fergusson DM, Horwood LJ. Burden of psychiatric disorder in young adulthood and life outcomes at age 30. Br J Psychiatry. 2010;197(2):122–127. | |
Patton GC, Coffey C, Romaniuk H, et al. The prognosis of common mental disorders in adolescents: a 14-year prospective cohort study. Lancet. 2014;383:1401–1411. | |
McGorry PD, Purcell R, Hickie IB, Yung AR, Pantelis C, Jackson HJ. Clinical staging: a heuristic model for psychiatry and youth mental health. Med J Aust. 2007;187(7 Suppl):S40–S42. | |
Hermens DF, Scott EM, White D, et al. Frequent alcohol, nicotine or cannabis use is common in young persons presenting for mental health care: a cross-sectional study. BMJ Open. 2014;3:e002229. | |
Scott EM, Hermens DF, Naismith SL, et al. Thoughts of death or suicidal ideation are common in young people aged 12 to 30 years presenting for mental health care. BMC Psychiatry. 2012;12:234. | |
Birchwood M, Singh SP. Mental health services for young people: matching the service to the need. Br J Psychiatry Suppl. 2013;54:s1–s2. | |
Illback RJ, Bates T. Transforming youth mental health services and supports in Ireland. Early Interv Psychiatry. 2011;5(Suppl 1):22–27. | |
Rao S, Pariyasami S, Tay SA, et al. Support for Wellness Achievement Programme (SWAP): a service for individuals with at-risk mental state in Singapore. Ann Acad Med. 2013;42(10):552–555. | |
Verma S, Poon LY, Lee H, Rao S, Chong SA. Evolution of early psychosis intervention services in Singapore. East Asian Arch Psychiatry. 2012;22(3):114–117. | |
McGorry PD, Tanti C, Stokes R, et al. Headspace: Australia’s National Youth Mental Health Foundation – where young minds come first. Med J Aust. 2007;187(7 Suppl):S68–S70. | |
Parker AG, Hetrick SE, Jorm AF, et al. The effectiveness of simple psychological and exercise interventions for high prevalence mental health problems in young people: a factorial randomised controlled trial. Trials. 2011;12:76. | |
Rickwood DJ, Telford NR, Parker AG, Tanti CJ, McGorry PD. Headspace – Australia’s innovation in youth mental health: who are the clients and why are they presenting? Med J Aust. 2014;200(2):108–111. | |
Hughes F, Stavely H, Simpson R, Goldstone S, Pennell K, McGorry P. At the heart of an early psychosis centre: the core components of the 2014 Early Psychosis Prevention and Intervention Centre model for Australian communities. Australas Psychiatry. 2014;22(3):228–234. | |
Mental Health Council of Australia. A Contributing Life: The 2013 National Report Card on Mental Health and Suicide Prevention. Sydney, Australia: Australian Government National Mental Health Commission; 2013. | |
Rickwood DJ, Mazzer KR, Telford NR, Parker AG, Tanti CJ, McGorry PD. Changes in psychological distress and psychosocial functioning in young people visiting headspace centres for mental health problems. Med J Aust. 2015;202(10):537–542. | |
Rickwood DJ, Telford NR, Mazzer KR, Parker AG, Tanti CJ, McGorry PD. The services provided to young people through the headspace centres across Australia. Med J Aust. 2015;202(10):533–536. | |
Chan SK, So HC, Hui CL, et al. 10-year outcome study of an early intervention program for psychosis compared with standard care service. Psychol Med. 2014:1–13. | |
Hegelstad WT, Larsen TK, Auestad B, et al. Long-term follow-up of the TIPS early detection in psychosis study: effects on 10-year outcome. Am J Psychiatry. 2012;169(4):374–380. | |
Nordentoft M, Rasmussen JO, Melau M, Hjorthoj CR, Thorup AA. How successful are first episode programs? A review of the evidence for specialized assertive early intervention. Curr Opin Psychiatry. 2014; 27(3):167–172. | |
van der Gaag M, Smit F, Bechdolf A, et al. Preventing a first episode of psychosis: meta-analysis of randomized controlled prevention trials of 12 month and longer-term follow-ups. Schizophr Res. 2013;149:56–62. | |
Norman RM, Manchanda R, Malla AK, Windell D, Harricharan R, Northcott S. Symptom and functional outcomes for a 5 year early intervention program for psychoses. Schizophr Res. 2011;129(2–3):111–115. | |
Porter ME. What is value in health care? N Engl J Med. 2010;363(26):2477–2481. | |
Bradach J. Going to Scale: The Challenge of Replicating Social Programs. Stanford, CA: Stanford Social Innovation Review. 2003:19–25. | |
Cooley L, Kohl R. Scaling Up – From Vision to Large-Scale Change: A Management Approach for Practitioners. Arlington, VA: Management Systems International; 2006. | |
Oreskes N, Conway E. Merchants of Doubt. London, UK: Bloomsbury; 2010. | |
World Health Organization. Adolescent Friendly Health Services: An Agenda for Change. Geneva, Switzerland: World Health Organization; 2002. | |
UNICEF. Adolescence: An Age of Opportunity. New York, NY: UNICEF; 2011. |
 © 2015 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2015 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.