")
Back to Journals » International Medical Case Reports Journal » Volume 15
Injection of Botulinum Toxin A in the Lacrimal Gland for Treatment of Epiphora in Crocodile Tears Syndrome – A Case Report
Authors Lima-Fontes M , Leuzinger-Dias M , Falcão-Reis F, Sousa C
Received 17 June 2022
Accepted for publication 1 September 2022
Published 22 September 2022 Volume 2022:15 Pages 537—542
DOI https://doi.org/10.2147/IMCRJ.S379024
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Scott Fraser
Mário Lima-Fontes,1 Mariana Leuzinger-Dias,1 Fernando Falcão-Reis,1,2 Cristina Sousa1
1Department of Ophthalmology, Centro Hospitalar Universitário São João, Porto, Portugal; 2Department of Surgery and Physiology, Faculty of Medicine of University of Porto, Porto, Portugal
Correspondence: Mário Lima-Fontes, Department of Ophthalmology, Centro Hospitalar Universitário São João, Alameda Prof. Hernâni Monteiro, Porto, 4200-319, Portugal, Email [email protected]
Purpose: Crocodile tears syndrome is a rare autonomic synkinesia, in which patients tear excessively in response to salivary stimuli. It usually occurs after idiopathic or traumatic facial palsy, as a result of aberrant reinnervation of the lacrimal gland by salivary efferent fibers from either the seventh or ninth cranial nerve.
Patients and Methods: We report the case of a 54-year-old woman, with a history of left Bell’s palsy, who attended our ophthalmology clinic due to epiphora of the left eye while eating or speaking, for 6 months.
Results: The ophthalmologic evaluation revealed a mild weakening of the frontal and left orbicularis oculi muscles without lagophthalmos. No other abnormalities were found, namely ocular surface swelling, ectropion, or obstruction of the lacrimal outflow system. Schirmer test II in the left eye increased from 12 to 23 mm while the patient was chewing. All these clues led to the diagnosis of crocodile tears syndrome and treatment with botulinum toxin A injection was proposed. One month after the injection of the palpebral lobe of the left lacrimal gland with 6 units of botulinum toxin A, the patient reported an almost complete resolution of the complaints, stated by a decrease in Munk scale and Lac-Q scores. Six months after injection, the patient conveyed recurrence of symptoms and a new treatment session was performed with comparable results.
Conclusion: Since crocodile tears syndrome is rare, it is crucial to increase awareness and knowledge about it among ophthalmologists and other medical doctors. Botulinum toxin is a safe and effective treatment modality, dramatically improving these patients’ quality of life.
Keywords: crocodile tears, gustatory lacrimation, epiphora, lacrimal gland, botulinum toxin A
Introduction
Bogorad syndrome, also called crocodile tears syndrome or gustatory lacrimation, is a rare autonomic synkinesia, in which patients tear excessively in response to salivary stimuli.1 It is thought to result from aberrant reinnervation of the lacrimal gland by salivary efferent fibers from either the seventh or ninth cranial nerve, most commonly in the setting of idiopathic or traumatic facial palsy.2
The treatment of crocodile tears syndrome depends on the severity of the hyperlacrimation and its impact on patients’ quality of life. Treatment options include subtotal resection of the lacrimal gland, glossopharyngeal and facial nerve section at different levels, use of anticholinergic drugs, intraorbital injection of alcohol or cocaine to destroy postganglionic fibers from the sphenopalatine ganglion, and injection botulinum toxin A into the lacrimal gland.3
Botulinum toxin A is an acetylcholine release inhibitor at the neuromuscular junction. It acts by stopping transmission along the aberrantly regenerated parasympathetic nerve fibers to the affected gland.3 It can be administered both transcutaneously and transconjunctivally to the lacrimal gland in crocodile tears syndrome patients. Rare, minor, and transient complications were reported in the literature, including ptosis, superior rectus palsy, and dry eye. The transconjunctival route is proven to have lesser complications than injecting transcutaneously.4
Herein, we report the drastic improvement of a patient diagnosed with Bogorad syndrome and successfully managed with injections of botulinum toxin A.
Materials and Methods
This case report complies with the guidelines for human studies and was conducted ethically in accordance with the World Medical Association Declaration of Helsinki. The patient was informed of her medical condition and gave her written consent to publish this report and accompanying images. Institutional approval was required to publish the case details.
A Schirmer test under topical anesthesia was used to assess tear volume. The severity of epiphora was graded according to the Munk scale.5 The lacrimal symptom questionnaire (Lac-Q) was used to determine the social and lifestyle impact of epiphora.6 Higher scores in Munk score and Lac-Q represent higher severity of symptoms and impact in quality of life.
Botulinum toxin A (Botox, Allergan, Dublin, Ireland) was reconstituted with sterile, preservative-free 0.9% sodium chloride solution diluted to a concentration of 50 units/1 mL. Each patient received topical Oxybuprocaine Hydrochloride 0.4% w/v (Anestocil, Edol, Lisbon, Portugal) before injection. The lateral upper eyelid was manually distracted away from the globe, while the patient looked down and to the opposite side to expose the palpebral lobe of the lacrimal gland. A transconjunctival injection of 6 units of botulinum toxin A using a 27-gauge needle on a 1-mL syringe was given into the palpebral lobe.7
Results
We present the case of a 54-year-old woman, who attended a general ophthalmology clinic complaining of painless epiphora in the left eye while speaking or eating, with 6 months of evolution. The patient had been diagnosed with Bell’s palsy on the left side one year earlier but recovered from the motor deficit with physical therapy. She had no other relevant medical history.
The ophthalmological evaluation revealed mild weakening of the left orbicularis oculi and frontal muscles without lagophthalmos. No other abnormalities were found, including inflammation of the ocular surface, ectropion, or obstruction of the tear outlet system.
A Schirmer test was performed under topical anesthesia for 5 minutes and the result was 12 mm for the left eye. The same test was then repeated while the patient was chewing, and the result was 23 mm (Figure 1A).
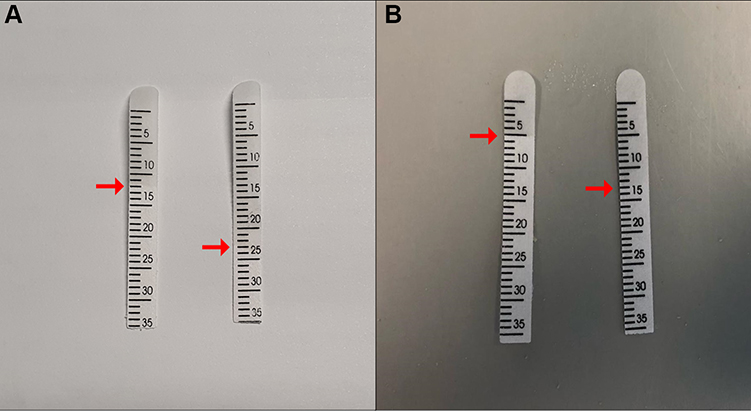 |
Figure 1 5-minute Schirmer Test under topical anesthesia: (A) before treatment; (B) 1 month after treatment. In both examinations, the test was performed in normal conditions (left strip in (A and B) and then repeated while the patient was chewing (right strip in (A and (B). Red arrows indicate test results. |
All these clues led to the diagnosis of Bogorad syndrome and treatment with botulinum toxin injection in the lacrimal gland was proposed.
Two weeks after the transconjunctival injection of 6 units of botulinum toxin in the palpebral lobe of the left lacrimal gland (Figure 2), the patient reported a decrease in perceived tearing, and 1 month after the treatment there was an almost complete resolution of the complaints.
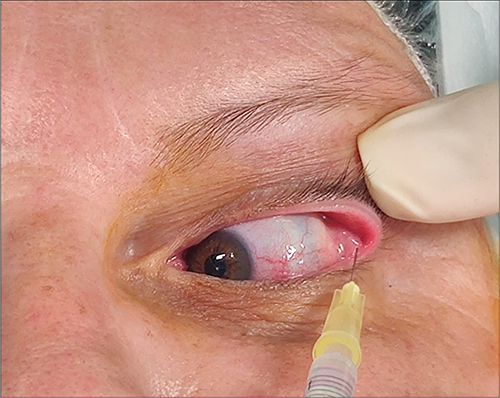 |
Figure 2 Transconjunctival injection of the left lacrimal gland palpebral lobe with 6 units of botulinum toxin A. |
Schirmer test was repeated under the same previous conditions, and the result was 5 and 12 mm, respectively (Figure 1B).
Munk scale was used for epiphora grading and the patient noted a reduction of the symptoms from a score of 4 to 1 with treatment (Table 1).
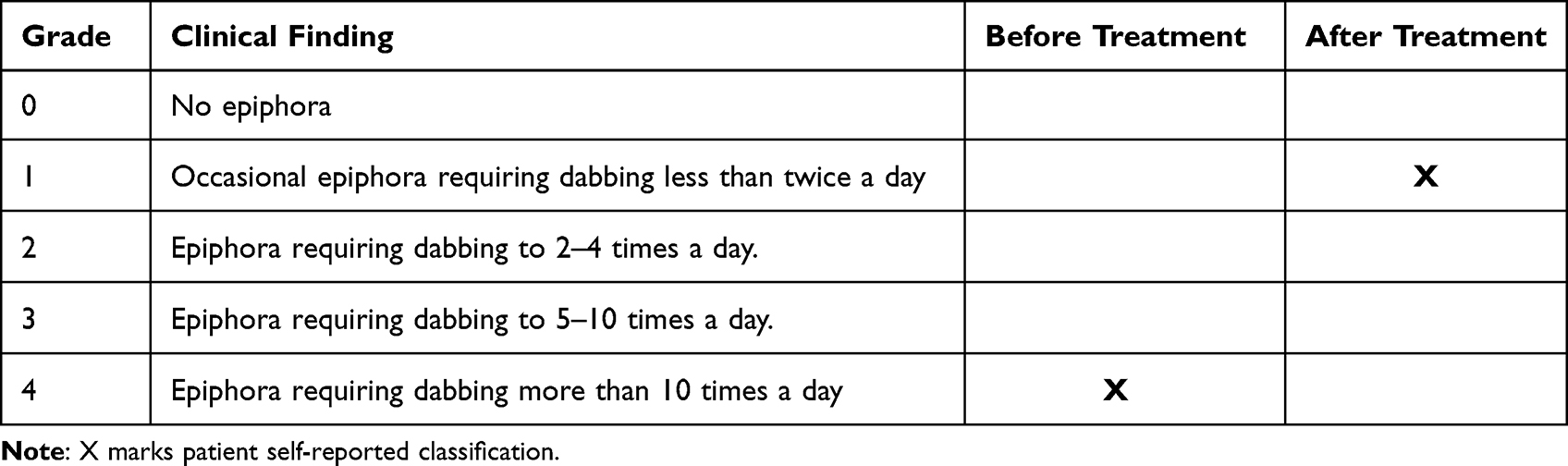 |
Table 1 Self-Reported Complaints in Accordance with Munk Scale, Before and 1 Month After the First Botulinum Toxin-A Injection |
The social impact was also assessed using the lacrimal symptom questionnaire (Lac-Q) and a score of 12 and 4 was reported by the patient before and 1 month after treatment, respectively (Tables 2 and 3).
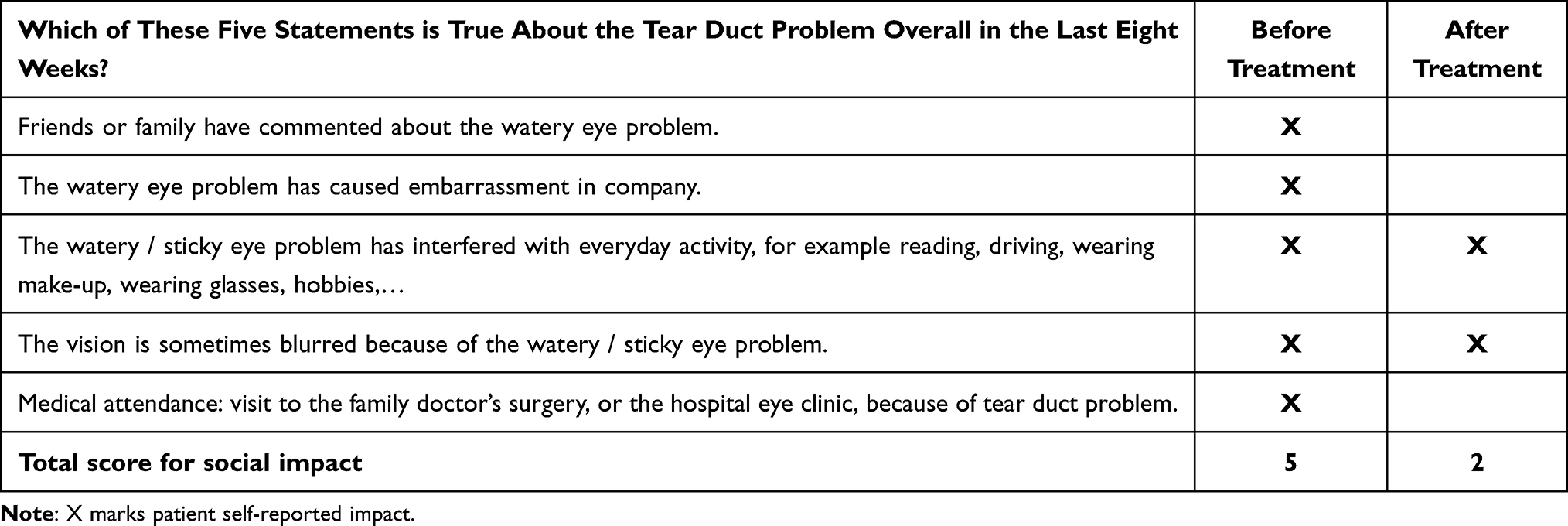 |
Table 2 Part 1 of the Lacrimal Symptom Questionnaire (Lac-Q). Social and Lifestyle Impact of Tear Duct Problem, Before and 1 Month After the First Botulinum Toxin-A Injection |
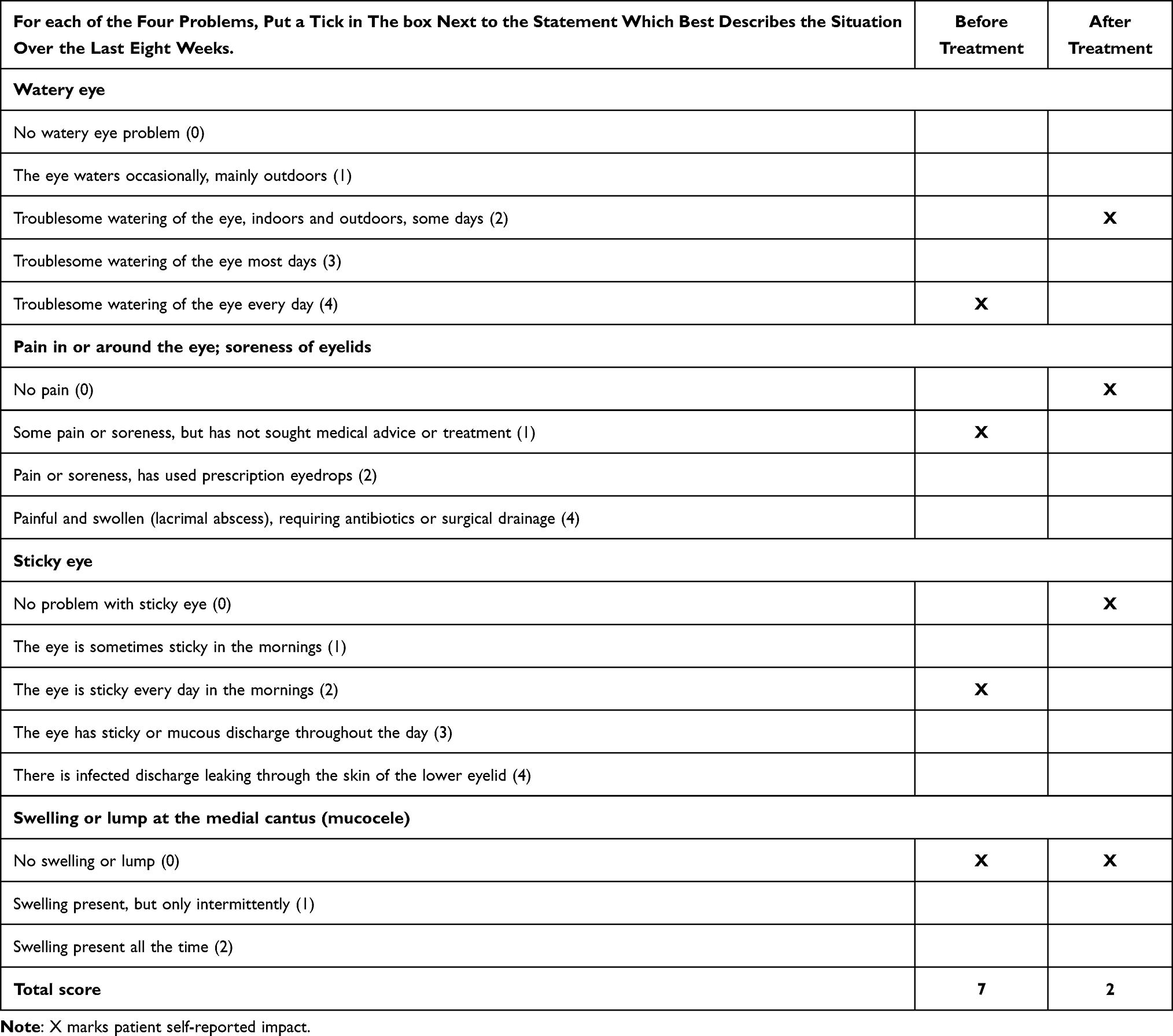 |
Table 3 Part 2 of the Lacrimal Symptom Questionnaire (Lac-Q). Classification of Left Eye Complaints, Before and 1 Month After the First Botulinum Toxin-A Injection |
Recurrence of the symptoms was detected 6 months after botulinum toxin treatment, and a new injection was performed with similar reported results.
No complications occurred after the two described procedures.
Discussion
Bogorad suggested in 1928 the term “crocodile tears syndrome” to describe gustatory hyperlacrimation, derived from the traditional belief that a crocodile sheds tears before devouring its victim.1 Over the years, several cases were described, the majority occurring after idiopathic or traumatic facial nerve palsy, as was the case of our patient, but also in congenital disorders, such as Duane’s retraction syndrome, Ramsay–Hunt syndrome, Dandy-Walker syndrome and Wildervanck syndrome.8
The pathogenesis of this syndrome is being unveiled by some theories. Consistently across the literature, it is believed that in the recovery period following facial nerve injury, the regenerating salivary nerve fibers undergo synkinesis or are misdirected via the greater superficial petrosal nerve to innervate the lacrimal gland instead of the submandibular gland. This results in excitation of the lacrimal gland to produce ipsilateral tearing rather than causing salivation by any stimuli of smell or taste of food.4
After the description of a few patients with crocodile tears syndrome and concomitant lateral rectus palsy or co-existing Duane retraction syndrome, Spiers et al raised the hypothesis of a congenital cause for this syndrome, specifically the existence of a lesion in the pons adjacent to the abducens nerve.9
Ephaptic interactions, in which electric fields generated by a specific neuron alter the excitability of neighboring neurons as a result of their anatomical and electrical proximity, may also occur in demyelinated but intact lacrimal fibers by efferent impulses in the salivary secretomotor fibers of the facial nerve.3
Over the years, numerous different treatments were described to treat excessive tearing, some of which were radical and permanent such as excision of the palpebral lobe of the lacrimal gland, cutting of the chorda tympani nerve, denervation of the lacrimal gland either by dissection or diathermy, and sphenopalatine ganglion blockage by alcohol or cocaine.4
In 1998, Boroojerdi et al first published the use of botulinum toxin in the treatment of gustatory hyper lacrimation.10 Since then, some isolated case reports and small case series were published.3,10–13
Botulinum toxin A affects neurotransmission by inhibiting the release of acetylcholine at the neuromuscular junction and cholinergic autonomic nerve terminals.3 Injection in the lacrimal gland can be delivered through both transcutaneous and transconjunctival routes. In the transcutaneous approach, the toxin is injected into the orbital lobe, whereas in the transconjunctival approach, it is injected under direct observation into the palpebral lobe of the lacrimal gland.14 The transconjunctival approach has the advantage of injecting a relatively lower dose into the gland by direct visualization, thus resulting in fewer complications.15
The exact dosage of botulinum toxin A to reach the maximum improvement in crocodile tears syndrome is not well established, with reports using doses ranging from 2.5 to 60 units.3,10–13 The higher doses seem to have no additional benefit in terms of efficacy or duration.2 The minimum dose reported having successfully reduced tears in functional outflow obstruction was 2.5 units.16 Pattanayak et al published an interesting case series in which patients with Bogorad syndrome were treated with two injections of 5 units of botulinum toxin transconjunctivally administered into the lacrimal gland within an interval of 1 week. All six patients showed complete or partial disappearance of reflex lacrimation while chewing. However, two patients developed transient ptosis.16
In our clinical case, the palpebral lobe of the left lacrimal gland was injected with 6 units of botulinum toxin A, which is in line with the small dosages adopted in the more recent studies.8,16 The patient reported a dramatic improvement in excessive tearing and quality of life, as stated by the notorious changes in auto-reported scores in the Munk scale and Lac-Q. To our knowledge, this is the first time these validated scales are applied to evaluate the results of botulinum toxin A injection in this setting.
No complications were identified after the two treatments performed on our patient. Minor complications were described in the literature, especially with transcutaneous botulinum toxin A injection, namely ptosis, superior and lateral rectus palsy, and dryness of the treated eye.3,8,13
The effect of botulinum toxin usually peaks in the first week after the injection with a duration of effect persisting up to 3–6 months.8,12 Recurrence of symptoms was reported by our patient 6 months after the first injection. A similar treatment was performed with comparable results. There is a paucity of studies with extended follow-up periods to assess the long-term efficacy and safety of repeated injections of botulinum toxin A in the lacrimal gland. Moreover, repeated minor trauma of the injection could eventually impair lacrimal gland function.2
Conclusion
Since crocodile tear syndrome is a rare entity, it is important to increase awareness and knowledge about it among ophthalmologists. Even though it is a benign condition, it has the potential to severely affect patients’ quality of life. Botulinum toxin A injection is a very safe and effective treatment for excessive tearing. However, long-term studies are needed to assess the efficacy and complications of this treatment after repeated injections.
Acknowledgments
The authors would like to thank the patient of this report.
Disclosure
The authors declare no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
References
1. Bogorad FA. The symptom of crocodile tears Introduction and translation by Austin Seckersen. J Hist Med Allied Sci. 1979;34(1):74–79. doi:10.1093/jhmas/XXXIV.1.74
2. Barañano DE, Miller NR. Long term efficacy and safety of botulinum toxin A injection for crocodile tears syndrome. Br J Ophthalmol. 2004;88(4):588–589.
3. Montoya FJ, Riddell CE, Caesar R, Hague S. Treatment of gustatory hyperlacrimation (crocodile tears) with injection of botulinum toxin into the lacrimal gland. Eye. 2002;16(6):705–709.
4. Modi P, Arsiwalla T. Crocodile tears syndrome. In: StatPearls. Treasure Island (FL): StatPearls Publishing Copyright ©; 2021.
5. Munk PL, Lin DT, Morris DC. Epiphora: treatment by means of dacryocystoplasty with balloon dilation of the nasolacrimal drainage apparatus. Radiology. 1990;177(3):687–690.
6. Mistry N, Rockley TJ, Reynolds T, Hopkins C. Development and validation of a symptom questionnaire for recording outcomes in adult lacrimal surgery. Rhinology. 2011;49(5):538–545.
7. Ziahosseini K, Al-Abbadi Z, Malhotra R. Botulinum toxin injection for the treatment of epiphora in lacrimal outflow obstruction. Eye. 2015;29(5):656–661.
8. Pattanayak S, Sharma PK, Samikhya S, Khuntia I, Patra K. Transconjunctival botulinum toxin injection into the lacrimal gland in crocodile tears syndrome. Indian J Ophthalmol. 2022;70(4):1339–1342.
9. Spiers AS. Syndrome of ”crocodile tears”. Pharmacological study of a bilateral case. Br J Ophthalmol. 1970;54(5):330–334.
10. Boroojerdi B, Ferbert A, Schwarz M, Herath H, Noth J. Botulinum toxin treatment of synkinesia and hyperlacrimation after facial palsy. J Neurol Neurosurg Psychiatry. 1998;65(1):111–114. doi:10.1136/jnnp.65.1.111
11. Riemann R, Pfennigsdorf S, Riemann E, Naumann M. Successful treatment of crocodile tears by injection of botulinum toxin into the lacrimal gland: a case report. Ophthalmology. 1999;106(12):2322–2324. doi:10.1016/S0161-6420(99)90534-1
12. Hofmann RJ. Treatment of Frey’s syndrome (gustatory sweating) and ‘crocodile tears’ (gustatory epiphora) with purified botulinum toxin. Ophthalmic Plast Reconstr Surg. 2000;16(4):289–291.
13. Keegan DJ, Geerling G, Lee JP, Blake G, Collin JR, Plant GT. Botulinum toxin treatment for hyperlacrimation secondary to aberrant regenerated seventh nerve palsy or salivary gland transplantation. Br J Ophthalmol. 2002;86(1):43–46.
14. Falzon K, Galea M, Cunniffe G, Logan P. Transconjunctival botulinum toxin offers an effective, safe and repeatable method to treat gustatory lacrimation. Br J Ophthalmol. 2010;94(3):379–380.
15. Lee AG, Lee S-H, Jang M, Lee SJ, Shin HJ. Transconjunctival versus transcutaneous injection of botulinum toxin into the lacrimal gland to reduce lacrimal production: a randomized controlled trial. Toxins. 2021;13(2):77.
16. Whittaker KW, Matthews BN, Fitt AW, Sandramouli S. The use of botulinum toxin A in the treatment of functional epiphora. Orbit. 2003;22(3):193–198.
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.