")
Back to Journals » Risk Management and Healthcare Policy » Volume 15
Initial Psychometric Development of the Fear and Anxiety to COVID-19 Scale in Nursing Professionals: An Occupational Health Assessment Tool
Authors Morgado-Toscano C, Allande-Cussó R , Fagundo-Rivera J , García-Iglesias JJ , Climent-Rodríguez JA, Navarro-Abal Y, Gómez-Salgado J
Received 28 July 2022
Accepted for publication 13 September 2022
Published 14 October 2022 Volume 2022:15 Pages 1947—1957
DOI https://doi.org/10.2147/RMHP.S384080
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Jongwha Chang
Cristina Morgado-Toscano,1 Regina Allande-Cussó,2 Javier Fagundo-Rivera,3 Juan Jesús García-Iglesias,4 Jose Antonio Climent-Rodríguez,5 Yolanda Navarro-Abal,5 Juan Gómez-Salgado4,6
1Health Sciences Doctorate School, University of Huelva, Huelva, Spain; 2Department of Nursing, University of Seville, Seville, Spain; 3Centro Universitario de Enfermería Cruz Roja, University of Seville, Seville, Spain; 4Department of Sociology, Social Work and Public Health, Faculty of Labour Sciences, University of Huelva, Huelva, Spain; 5Department of Social, Evolutionary and Educational Psychology, Faculty of Labour Sciences, University of Huelva, Huelva, Spain; 6Safety and Health Postgraduate Programme, Universidad Espíritu Santo, Guayaquil, Ecuador
Correspondence: Regina Allande-Cussó, Department of Nursing, University of Seville, Sevilla, 41009, Spain, Email [email protected] Juan Gómez-Salgado, Department of Sociology, Social Work and Public Health, Faculty of Labour Sciences, University of Huelva, Avenida Tres de marzo s/n, 21007, Huelva, Spain, Email [email protected]
Objective: The effects caused by COVID-19 on the physical and mental health show the need to renew and create tools that specifically measure the fear and anxiety caused by the pandemic in healthcare professionals. The aim of the study was to measure fear and anxiety of COVID-19 in the nursing population group using a specific assessment scale.
Methods: A descriptive, cross-sectional study was carried out in Spain based on questionnaires. The sample was selected by non-probabilistic snowball sampling. Univariate and bivariate descriptive analyses were performed. For qualitative variables, a categorical regression analysis was performed.
Results: The sample consisted of 1012 nurses residing in Spain, 86.6% of whom were women, with a mean age of 40.84 years (SD = 11.51). The bivariate analysis revealed statistically significant differences in the mean score of the scale and the variables sex, level of education, m2 of the dwelling, and work area.
Conclusion: The validation of this scale provides a new management tool that should enable managers to assess anxiety and fear among their nurses, whether in the current COVID-19 pandemic or in other possible epidemiological situations to come.
Keywords: COVID-19, anxiety, fear, nurses, mental health
Introduction
The new coronavirus disease (COVID-19) was detected for the first time in December 2019 in Wuhan, Hubei province (China), this being the first case of pneumonia caused by this new coronavirus.1 Spain, like many other countries in the world, presented a high number of cases at the beginning of the pandemic; therefore, the Spanish government, following the Royal Decree of State of Alarm, ordered a nationwide emergency measure of house confinement to prevent the spread of the infection.2 COVID-19 disease can cause a highly variable symptomatology, in some cases even being asymptomatic.3
Throughout history, other epidemics have occurred at earlier historical moments, such as smallpox or the Plague, which resulted in a large number of deaths and, therefore, the associated suffering.4 One thing that makes COVID-19 stand out among previous pandemics is the amount of information available on confirmed cases and mortality worldwide.5 In a situation as rare as this one, the channels and tools used by health authorities to provide information on the number of infections, number of deaths, risks, available treatment, vaccination, preventive measures, etc. may generate a state of anxiety, fear or frustration in the population, which in turn can lead to serious mental health problems.6 Given the initial uncertainty and lack of knowledge regarding the epidemiology and prognosis of COVID-19, the term “coronaphobia” came to appear, defined as a state of fear of contagion and social contact among the population.7
Healthcare professionals have been one of the population groups with the highest number of quantified cases, related to direct exposure to diagnosed cases of COVID-19 during their professional activity.8 Additionally, they have suffered from stress and work overload due to the high incidence of cases. This was compounded by long working hours due to shortage of healthcare personnel, restructuring of services, and lack of protection due to lack of materials, with the consequent risk of contagion.9 Protective factors such as job satisfaction, high self-esteem, and perceived social support have also been described.10
A study based on the psychological distress of healthcare workers during the pandemic, conducted by Gomez-Salgado et al, revealed a high prevalence of psychological distress among professionals who had provided services during the pandemic. The same study concluded that professionals who had been on the frontline during the COVID-19 pandemic suffered more mental health problems than other health professionals in the same category. For example, anxiety levels were lower in nurses working in primary care. This may have been related to the implementation of telemedicine in these services.11
Another study carried out in Spain by Erquicia et al12 also showed the emotional impact of the COVID-19 pandemic on healthcare professionals, especially nurses, because they provide direct care to patients suffering from COVID-19. Along the same lines, a study in China at the beginning of the pandemic already showed the presence of emotional distress and fear in nurses of different hospitals in the country.13 Another study performed in Portugal with nurses showed the same results, with a greater presence of emotional distress in nurses than in the general population, given their healthcare activity in direct contact with patients suffering from COVID-19.14 Furthermore, Hamama et al15 provided the same data about nurses in Israel, also considering the need to study these professionals’ feelings so as to provide the necessary emotional support.
The effects of COVID-19 on the physical and mental health have generally been studied using items created specifically ad hoc for the cross-sectional studies.8–12 With all this, there is a need to renew and create tools that specifically measure the fear and anxiety caused by the pandemic in the general population, and more specifically in nursing professionals. One of the first scales designed for this purpose was the Fear of COVID-19 (FCV-19). It is a scale designed by Ahorsu et al and initially composed of ten items which, after a validation process in Iran, were eventually seven.16 After the publication of the FCV-19 scale, which demonstrated good psychometric properties, it has been validated in different countries. In the case of Spain, it was validated by Martínez-Lorca et al on a group of university students.17
In Spain, a group of researchers designed the Anxiety and Fear of COVID-19 (AMICO) Assessment Scale, based on the initial version of FCV-19 10 items, which was composed of 16 items and measured not only fear but also anxiety about COVID-19. This scale proved to be a reliable and valid tool to be used as a screening instrument in Spain.18
In this context, the aim of the present study is the adaptation of the AMICO scale for its adaptation and validation for specific use in nursing professionals in Spain, as this has been one of the sectors most punished at all levels by COVID-19.
Methods
Design
A descriptive cross-sectional study was carried out in Spain based on questionnaires, according to the classification by Herzog et al.19 The study period was from March to June 2021.
Population and Sample
In Spain, 287,101 nurses were registered as of 2019.20 For this study, a sample of at least 270 was estimated, with a confidence level of 95%, a precision of 3%, and an expected loss ratio of 25%. Finally, the type of sampling offered the opportunity to obtain a total sample of 1012 subjects from all regions of Spain, increasing the statistical power from 84% to 90.5%. The inclusion criterion was to carry out a professional activity in the field of nursing in Spain. Questionnaires not fully completed were excluded from the final sample.
Variables
Socio-demographic variables (sex, age, province, marital status, educational level, monthly income, number of cohabitants, m2 of dwelling) were included, as well as questions related to COVID-19 contact and infection and self-perception of health status. Work variables such as work situation and area of work were also included. Finally, the AMICO scale was also included as a variable.
Instruments
The Anxiety and Fear of COVID-19 (AMICO) scale was used. It consists of 16 items distributed in two factors (anxiety and fear), explaining 64% of the variance (KMO test = 0.94; Bartlett's test p = 0.001). The responses for these 16 items range from 1, being the lowest self-reported level, to 10, being the highest self-reported level. The total score of the scale can be obtained by calculating the mean score from the responses, with the value ranging from 1 to 10 points.7 The reliability of the scale showed a Cronbach’s alpha value of 0.92 and convergent validity with the STAI (State-Trait Anxiety Inventory) scale, which measures the anxiety construct.21 Likewise, the AMICO scale obtained a sensitivity of 90.48% and a specificity of 76%.18
Procedure
A non-probabilistic snowball sampling was carried out. For the recruitment of the sample subjects, an online questionnaire was developed using the GoogleForms© application. This included information on the study and on the items related to the study variables.
The link to access the questionnaire was sent by e-mail to members of different official nursing organisations that do not allow the admission of professionals from other disciplines. They should also have agreed to be contacted for research purposes. The Spanish General Council of Nursing also assisted in the process. All subjects who were sent the information were duly informed of the purpose of the survey and the possibility of participating in it voluntarily, anonymously, and confidentially.
Data Analysis
The descriptive univariate and bivariate analyses were carried out using the IBM SPSS v. 26© statistical software.22 The Kolmogorov–Smirnov test was initially performed, obtaining a p-value of < 0.005, so a non-normal data distribution was considered. Therefore, non-parametric tests were used. The Mann–Whitney U and Kruskal–Wallis tests were used for contrast tests. Kendall’s Tau-b test was also used to study the correlation between two quantitative variables.
Cronbach’s alpha calculation was performed for the reliability study. In addition, an exploratory factor analysis was carried out to study the dimensional structure of the scale. For this purpose, the maximum likelihood extraction method and varimax rotation were selected, eliminating items with loadings < 0.05.
Finally, for the study of the relationship between the study variables, and given their qualitative nature, a categorical regression analysis (CATREG) was carried out. This method quantifies the categorical data by assigning numerical values to the categories to obtain an optimal linear regression equation for the transformed variables.23 CATREG analysis includes characteristic aspects of classical regression analysis: coefficient of determination (R2), variance, regression analysis, and significance of model parameters.24 For the calculation, the optimal scaling option was selected in the SPSS© software 26.0.22
Ethical Aspects
The relevant authorisation for this study was obtained from the Research Ethics Committee of the Regional Government of Andalusia (Ref. PI 036/20). In addition, authorisation was also obtained from the Spanish General Council of Nursing. This study also complies with the Helsinki Declaration of Ethical Principles in Human Research Guidelines.25
All participants in the sample agreed to participate on a voluntary basis. Informed consent was obtained from all the participants included in the study. The confidentiality of data and anonymity of the participants was ensured by respecting at all times Spanish Organic Law 3/2018 of 5 December on data protection, as well as the confidentiality of the study by ticking a specific box for this purpose. After ticking a box offering their consent, participants were allowed to access the questionnaire. Otherwise, they would not have access to it.
In addition, the informed consent form explained that the participant could contact the main researcher if psychological support was needed after completing the questionnaire. The full name and e-mail address of this contact were provided. The research team took on the responsibility of responding to these requests in a confidential manner and providing the necessary psychological care to the participant.
Results
Descriptive Analysis
The total study sample consisted of 1012 nurses who were residing in Spain. As can be seen in Table 1, of the total sample, 86.6% were women and 13.4% were men. The age of the sample ranged from 19 to 68 years, with a mean of 40.84 years (SD = 11.51). Regarding the educational level, 44.9% had a degree in Nursing and 24.4% a specialty in Nursing. The remaining 30% had a master’s degree or a doctorate. Of the 1012 people in the sample, 88.5% were working full time and only 0.2% were on furlough. Regarding the area of work, most of the sample was working in specialised care (38.8%). The majority of the sample had not had the disease. However, most of them had been isolated at some point due to close contact with a positive patient.
 |
Table 1 Description of the Sample Profile with Respect to the Study Variables |
For the total AMICO variable, a mean score of 6.31 (SD = 1.84) was obtained, with a range of scores from 1.13 to 10 (Table 1). On the other hand, the Kolmogorov–Smirnov test, with a significance of 0.000, revealed that the distribution of the scores obtained on the AMICO scale did not follow a normal distribution, so non-parametric tests were performed. In the bivariate analysis for the total AMICO variable, statistically significant differences were found in the mean score of the scale and the sex, educational level, m2 of dwelling, and work area variables. Females showed the highest levels of fear and anxiety in the AMICO scale (6.4), compared to males (5.8) (Table 2).
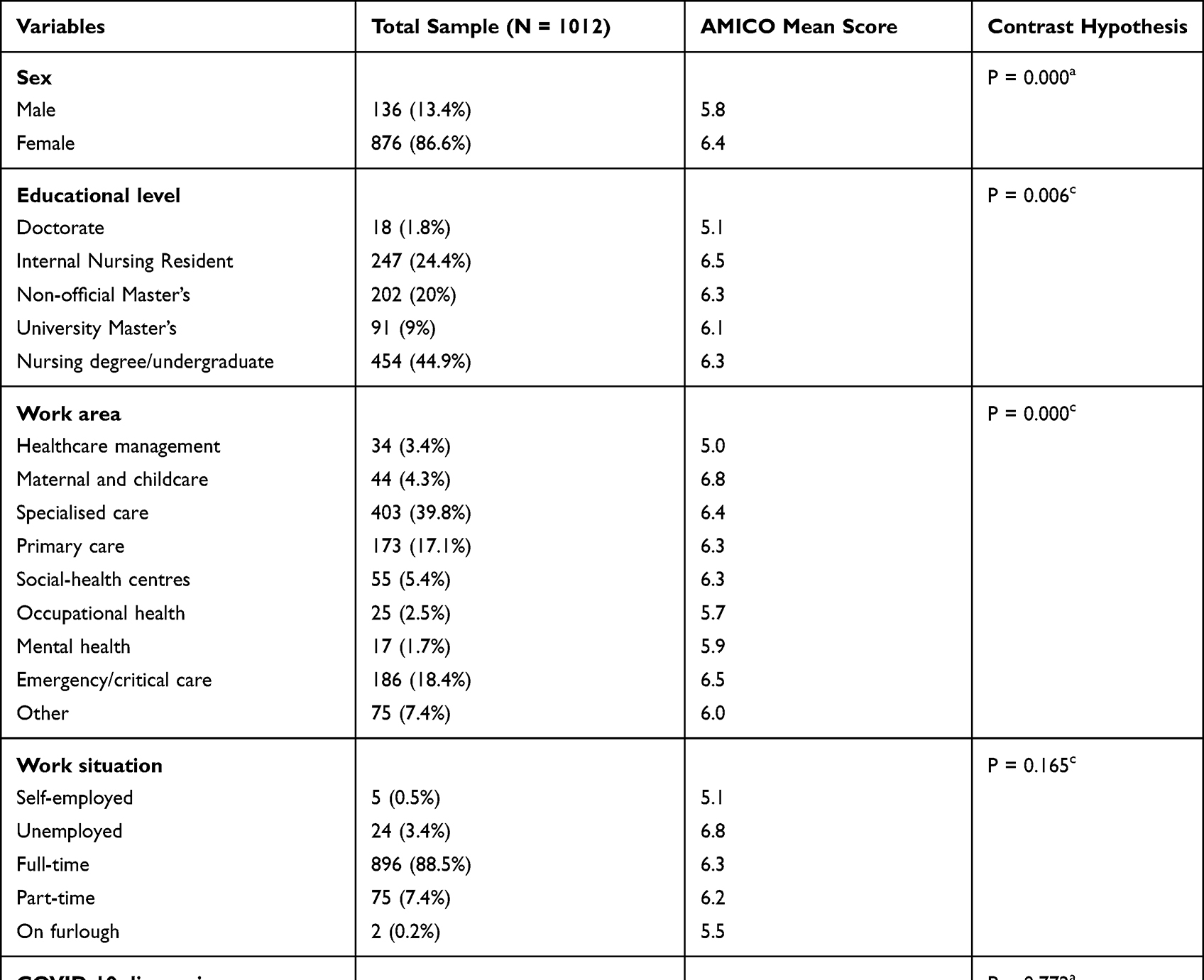 |
Table 2 Bivariate Analysis Regarding the AMICO Score and Study Variables |
With regard to the educational level, it is worth noting that people with a doctorate were those who showed the lowest level of fear and anxiety in the results (5.1). As refers to work situations, the lowest scores for the AMICO scale were obtained by those who were self-employed (5.1), with the highest scores for fear and anxiety being obtained by those who worked full-time (6.8). As for the area of work, nurses working in the mother and child area scored the highest on this scale (6.8), with those in management positions scoring the lowest (5).
Psychometric Analysis
The Kaiser-Meyer-Olkin test (KMO) obtained a value of 0.948, and the Bartlett’s test of sphericity obtained a statistically significant value (p < 0.001). Exploratory factor analysis (EFA) was performed, from which 2 factors (anxiety and fear) were extracted. Items two and fourteen were removed from the dimensional structure as they had loadings below 0.5 (Table 3). The reliability study of the scale revealed an overall Cronbach’s alpha value of 0.92, of 0.92 for factor 1 (anxiety), and 0.90 for factor 2 (fear).
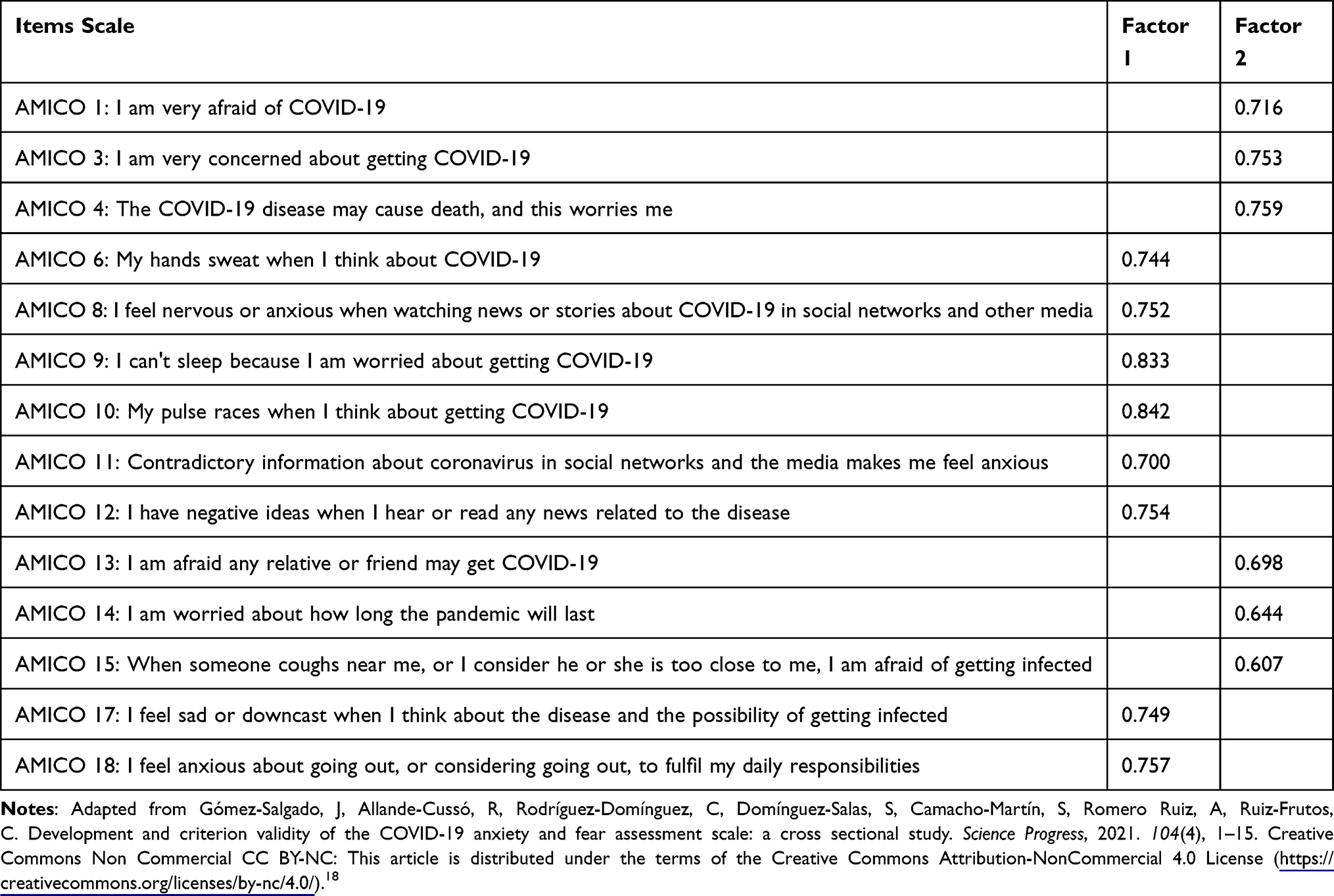 |
Table 3 Exploratory Factor Analysis of the Dimensional Structure |
Regression Analysis
The calculation of the categorical regression (CATREG) was performed, firstly, with the mean total score of the AMICO questionnaire as the dependent variable, and then, with the rest of the variables, showing that only the sex, square metres, and area in which they carried out their work variables were significant (Table 4). The R2 value was 0.65, indicating that 65% of the variance is explained by the regression model designed. Therefore, as female nurses who were working in the emergency and critical care, hospital care, and maternal and childcare areas had the highest AMICO scale scores, the regression model indicates that this relationship is significant and predicts these higher scores. Thus, women scored 0.1 times higher than men, and those working in emergency and critical care and maternal and childcare scored 0.12 times higher on the AMICO scale.
 |
Table 4 Model Adjustment and Significance of the Regression Analysis |
Discussion
Both fear and anxiety in the face of a threatening or uncertain situation such as the one we have experienced with COVID-19 can lead to extreme reactions such as excessive fear and panic. The flight from Madrid of thousands of people to their second homes outside the Autonomous Community that took place moments before the declaration of the state of alarm and the closure of mobility is a clear example of this type of behaviour.26 In this sense, the manifestations of fear and anxiety due to pandemic stress can produce, in the medium to long term, depressive symptoms, pathological grief, increased likelihood of substance abuse, psychotic symptoms, and post-traumatic stress disorder.27 It is important to note that many of the psychological reactions mentioned above are not pathological. According to the World Health Organisation (WHO), they are ‘natural and normal reactions to the changing and uncertain situation in which we all find ourselves’. However, this does not mean that they should not be treated.28
In the case of nursing professionals, as one of the most exposed professions since the beginning of the pandemic, extreme situations have been experienced for months.29 In addition to the long working hours, there was a lack of staff and resources, a lack of knowledge of the disease, contagion among colleagues, fear of infecting their relatives, etc. All this has led this group to be the focus of several studies to find out the possible consequences of this situation.30
Since, according to the Official State Bulletin of the Public Administration Service, the percentage of employed women working in the Spanish health system is 74.2%, in all the articles reviewed, as in the present study, a large part of the sample was composed of women.31 Also, and in line with the results of the articles reviewed, mental health problems were found to be higher in women than in men. A study conducted in Spain based on the AMICO scale showed that women, in general, have a higher level of anxiety than men, concluding that the prevalence of symptoms of psychological distress and affective disorders in Spain in women amounts to 14% of the population, compared to 7.2% in men.5 The same study also found that around 70% of family caregiving tends to fall on women;9 this percentage may have increased due to the situation of confinement experienced, with the consequent closure of schools and teleworking, which would explain the higher AMICO scale scores for women nurses and the statistically significant difference between the AMICO variable and the square meters of the dwelling.10
The said study also related higher levels of psychological distress with those nurses who worked from home, as compared to those who worked outside, although in the present study the results are the opposite, as those who scored lowest in the AMICO scale were nurses who were in charge of management areas, ie those who had no contact with patients.11
As for the area of work, another study focusing on healthcare professionals by Li et al32 concluded that frontline workers experienced greater mental health deterioration during the pandemic than other healthcare workers who were not so exposed. However, they also report that they suffered less burnout and vicarious trauma.32 This statement can also be extrapolated to the results of the present study, as the regression analysis revealed that nurses who worked in the emergency and critical care, hospital care, and maternal and childcare areas had the highest scores on the AMICO scale, and the regression model indicates that this relationship is significant and predicts these higher scores. Therefore, women scored 0.1 times higher than men, and those working in emergency and critical care and maternal and childcare scored 0.12 times higher on the AMICO scale.
On the other hand, this study concluded that the higher the level of education, the lower the score on the AMICO scale, that is, the higher the level of education, the lower the anxiety, although in the result of the regression analysis presented in the study this variable was not significant. In this sense, a study revealed that there is a relationship between a low level of education and the greater presence of anxiety, depression, and fear in the adult population,33 and in the same vein, another more recent report by the Center for Behavioral Health Statistics and Quality in the United States also pointed to the same idea.34 Perhaps, the higher level of knowledge and the acquisition of advanced academic competencies enhance the ability of nursing professionals to identify scientific evidence and carry out critical thinking processes with respect to the work situations they face. Another aspect involved is the fact of being young as a risk factor for obtaining higher scores in anxiety levels, and this was confirmed by a study through a cross-sectional survey at global level.35 Related to this, another study in Spain revealed that being a healthcare worker under 55 years of age during the pandemic was a risk factor for developing anxiety, depression, insomnia, and stress. After evaluating these data, it can be concluded that experience and confidence help to minimise the stress caused by unforeseen situations.36
Comparing this study with other similar ones at European level, a study conducted in eight European countries using a cross-sectional, multilingual survey and the Depression Anxiety Stress Scales-21 (DASS-21) to measure mental stress is worth mentioning. This study concluded that the UK and France had the highest depression, anxiety, and stress scores compared to other countries. In Italy and Spain, although the situation was worse, participants had lower psychological stress scores compared to France and the UK.37
It is true is that the vast majority of studies consulted affirm a high prevalence of psychological distress among healthcare professionals who have been active during the COVID-19 pandemic.10 In fact, the highest expression of psychological distress during the first pandemic in Spain was manifested by the group of nurses, as compared to the rest of the professional categories. However, the scores on vigour at work were significantly lower in this group according to the UWES-9 scale.38
Apart from stressors, protective factors have been described that may help prevent or mitigate the negative effects of the COVID-19 pandemic on mental health.34 As expected, the level of social support was found to positively correlate with self-efficacy and sleep quality, and negatively with anxiety and stress.39 In this sense, factors such as organisational support, support groups, and improved available information have been described as protective.40
One possible strength of this study is that the proportion of women and men in the sample of this study is similar to the actual percentages by sex in the nursing profession in Spain.41 Even so, the data do not allow for a strict study of the differences between sexes with respect to the AMICO scale, as the reality is that 84% of Spanish nurses, and of the sample, are women. On the other hand, the main limitations of the study are the non-probabilistic sampling used in the data collection and the social desirability effect that appears when using self-administered questionnaires. Likewise, the epidemiological situation at the time of data collection, up to four months after the declaration of the state of alarm in Spain, might have influenced the results obtained, as knowledge about COVID-19 had already advanced.
However, this study highlights the need for action on the part of health managers to offer care and help to those health professionals affected by the COVID-19 situation. In this sense, the results could facilitate the identification of priority areas of intervention to offer care or help to healthcare professionals who need it. In addition, the creation of the figure of the sentinel nurse in nursing care units is proposed as a link with the occupational healthcare services and following specific training and information.
Conclusions
Female nurses with just degree level of education, working in the maternal and childcare areas presented higher levels of anxiety and fear of COVID-19. In this sense, it is necessary to strengthen the mental health networks of all autonomous communities to address all the mental problems that the pandemic has caused to nursing professionals.
On the other hand, the initial psychometric development of this scale provides a new management tool that should allow managers to assess anxiety and fear among their nurses, both in the current COVID-19 pandemic and in other possible future epidemiological situations. Thus, the tool may allow screening for mental health problems in nurses and may even allow monitoring of these problems, seeking to facilitate the necessary support and improve the work climate.
Ethical Considerations
The ethical approval for this study was obtained from the Research Ethics Committee of the Regional Government of Andalusia in Spain (Ref. PI 036/20).
Acknowledgments
Funding for Open Access charge: Universidad de Huelva- CBUA.
Author Contributions
All authors made a significant contribution to the work reported, whether in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
There is no funding to report.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Johnson M. Wuhan 2019 Novel Coronavirus - 2019-nCoV. Mater Methods. 2020;10:1–5. doi:10.13070/mm.en.10.2867
2. Ruiz-Frutos C, Ortega-Moreno M, Allande-Cussó R, Domínguez-Salas S, Dias A, Gómez-Salgado J. Health-related factors of psychological distress during the COVID-19 pandemic among non-health workers in Spain. Saf Sci. 2021;133. doi:10.1016/j.ssci.2020.104996
3. Allande-Cussó R, García-Iglesias JJ, Ruiz-Frutos C, Domínguez-Salas S, Rodríguez-Domínguez C, Gómez-Salgado J. Work engagement in nurses during the COVID-19 pandemic: a cross-sectional study. Healthcare. 2021;9(3):1–11. doi:10.3390/healthcare9030253
4. Páez D, Fernández I, Martín Beristain C. Catástrofes, traumas y conductas colectivas: procesos y efectos culturales [Catastrophes, traumas and collective behaviours: processes and cultural effects]. Catástrofes y Ayuda En Emergencia. 2015;2015:85–148.
5. Allande-Cussó R, Linares Manrique M, Gómez-Salgado J, et al. Anxiety and fear related to coronavirus disease 2019 assessment in the Spanish population: a cross-sectional study. Sci Prog. 2021;104(3):1–14. doi:10.1177/00368504211038191
6. Asmundson GJG, Taylor S. How health anxiety influences responses to viral outbreaks like COVID-19: what all decision-makers, health authorities, and health care professionals need to know. J Anxiety Disord. 2020;71(January):102211. doi:10.1016/j.janxdis.2020.102211
7. Gómez-Salgado J, Allande-Cussó R, Domínguez-Salas S, García-Iglesias JJ, Coronado-Vázquez V, Ruiz-Frutos C. Design of fear and anxiety of COVID-19 assessment tool in Spanish adult population. Brain Sci. 2021;11(3):1–9. doi:10.3390/brainsci11030328
8. Equipo profesional de Red Nacional de Vigilancia Epidemiológica (RENAVE). Análisis de los casos de COVID-19 en personal sanitario notificados a la RENAVE hasta el 10 de mayo en España [Analysis of COVID-19 cases in healthcare workers reported to RENAVE as of 10 May in Spain]. Instituto de Salud Carlos III (ISCIII). 2020:11. Available from: https://www.who.int/dg/speeches/detail/who-director-general-s-remarks-at-The-media-briefing-on-2019-ncov-on-11-february-.
9. González-Sanguino C, Ausín B, Castellanos MÁ, et al. Mental health consequences during the initial stage of the 2020 Coronavirus pandemic (COVID-19) in Spain. Brain Behav Immun. 2020;87(May):172–176. doi:10.1016/j.bbi.2020.05.040
10. Domínguez-Salas S, Gómez-Salgado J, Guillén-Gestoso C, Romero-Martín M, Ortega-Moreno M, Ruiz-Frutos C. Health care workers’ protection and psychological safety during the COVID-19 pandemic in Spain. J Nurs Manag. 2021;29(7):1924–1933. doi:10.1111/jonm.13331
11. Gómez-Salgado J, Domínguez-Salas S, Romero-Martín M, Ortega-Moreno M, García-Iglesias JJ, Ruiz-Frutos C. Sense of coherence and psychological distress among healthcare workers during the COVID-19 pandemic in Spain. Sustainability. 2020;12(17):6855. doi:10.3390/SU12176855
12. Erquicia J, Valls L, Barja A, et al. Emotional impact of the COVID-19 pandemic on healthcare workers in one of the most important infection outbreaks in Europe. Med Clin. 2020;155(10):434–440. English, Spanish. doi:10.1016/j.medcli.2020.07.006
13. Shen X, Zou X, Zhong X, Yan J, Li L. Psychological stress of ICU nurses in the time of COVID-19. Crit Care. 2020;24(1):200. doi:10.1186/s13054-020-02926-2
14. Sampaio F, Sequeira C, Teixeira L. Nurses’ mental health during the covid-19 outbreak: a cross-sectional study. J Occup Environ Med. 2020;62(10):783–787. doi:10.1097/JOM.0000000000001987
15. Hamama L, Marey-Sarwan I, Hamama-Raz Y, Nakad B, Asadi A. Psychological distress and perceived job stressors among hospital nurses and physicians during the COVID-19 outbreak. J Adv Nurs. 2022;78(6):1642–1652. doi:10.1111/jan.15041
16. Ahorsu DK, Lin CY, Imani V, Saffari M, Griffiths MD, Pakpour AH. The fear of COVID-19 scale: development and initial validation. Int J Ment Health Addict. 2020;1–9. doi:10.1007/s11469-020-00270-8
17. Martínez-Lorca M, Martínez-Lorca A, Criado-álvarez JJ, Armesilla MDC, Latorre JM. The fear of COVID-19 scale: validation in Spanish university students. Psychiatry Res. 2020;293:113350. doi:10.1016/j.psychres.2020.113350
18. Gómez-Salgado J, Allande-Cussó R, Rodríguez-Domínguez C, et al. Development and criterion validity of the COVID-19 anxiety and fear assessment scale: a cross sectional study. Sci Prog. 2021;104(4):1–15. doi:10.1177/00368504211050291
19. Herzog M, Francis G, Clarke A. Experimental design and the basics of statistics: Signal Detection Theory (SDT). In: Understanding Statistics and Experimental Design. Cham, Switzerland: Springer International Publishing; 2019:13–22.
20. Departamento de Economía del Gobierno de España. Instituto nacional de estadística [National Statistics Institute]. Madrid, España: Gobierno de España; 2020. Available from: https://www.mscbs.gob.es/estadEstudios/sanidadDatos/tablas/tabla14.htm.
21. Buela-Casal G, Guillén-Riquelme A, Sisdedos Cubero N. Manual STAI, Cuestionario de Ansiedad Estado Rasgo. Adaptación española. Tea Ediciones [STAI Manual, Trait State Anxiety Questionnaire. Spanish adaptation]; 2015:7–16. Available from: http://www.web.teaediciones.com/Ejemplos/STAI-Manual-Extracto.pdf.
22. IBM Corporation. IBM SPSS statistics for windows. version 26.0; 2019.
23. Xu J, Capretz L, Ho D. Building an oss quality estimation model with CATREG. Int J Comput Sci Eng. 2010;2(06):1952–1958.
24. Guerra W, Herrera M, Fernández L, Álvarez NR. Categorical regression model for the analysis and interpretation of statistical power. Cuba J Agric Sci. 2019;53(1):13–20.
25. World Medical Assembly. Declaration of Helsinki. Geneva, Switzerland. World Health Organization; 1964. Available from: https://www.who.int/bulletin/archives/79(4)373.pdf.
26. Chacón F, Fernández-Hermida JR, García-Vera MP. La psicología ante la pandemia de la COVID-19 en España. La respuesta de la organización colegial [Psychology to face the COVID-19 pandemic in Spain. The response of the professional council]. Clínica y Salud. 2020;31(2):119–123. doi:10.5093/clysa2020a18
27. Brooks SK, Webster RK, Smith LE, et al. The psychological impact of quarantine and how to reduce it: rapid review of the evidence. Lancet. 2020;395(10227):912–920. doi:10.1016/S0140-6736(20)30460-8
28. World Health Organization. Regional Office for Europe. Mental health and psychological resilience during the COVID-19 pandemic; 2020. Available from: https://www.euro.who.int/en/health-topics/health-emergencies/coronavirus-COVID-19/news/news/2020/3/mental-health-and-psychological-resilience-during-The-COVID-19-pandemic.
29. Ornell F, Schuch JB, Sordi AO, Kessler FHP. “Pandemic fear” and COVID-19: mental health burden and strategies. Braz J Psychiatry. 2020;42(3):232–235. doi:10.1590/1516-4446-2020-0008
30. Cheung T, Fong TKH, Bressington D. COVID-19 under the SARS cloud: mental health nursing during the pandemic in Hong Kong. J Psychiatr Ment Health Nurs. 2021;28(2):115–117. doi:10.1111/jpm.12639
31. Torrente M, Sousa PAC, Sánchez-Ramos A, et al. To burn-out or not to burn-out: a cross-sectional study in healthcare professionals in Spain during COVID-19 pandemic. BMJ Open. 2021;11(2):1–12. doi:10.1136/bmjopen-2020-044945
32. Li Z, Ge J, Yang M, et al. Vicarious traumatization in the general public, members, and non-members of medical teams aiding in COVID-19 control. Brain Behav Immun. 2020;88(March):916–919. doi:10.1016/j.bbi.2020.03.007
33. Bjelland I, Krokstad S, Mykletun A, Dahl AA, Tell GS, Tambs K. Does a higher educational level protect against anxiety and depression? The HUNT study. Soc Sci Med. 2008;66(6):1334–1345. doi:10.1016/j.socscimed.2007.12.019
34. Karg RS, Bose J, Batts KR, et al. CBHSQ Data Review: Past Year Mental Disorders Among Adults in the United States: Results from the 2008–2012 Mental Health Surveillance Study. Rockville, MD: Center for Behavioral Health Statistics and Quality, Substance Abuse and Mental Health Services Administration; 2014.
35. Varma P, Junge M, Meaklim H, Jackson ML. Younger people are more vulnerable to stress, anxiety and depression during COVID-19 pandemic: a global cross-sectional survey. Prog Neuropsychopharmacol Biol Psychiatry. 2021;109:110236. doi:10.1016/j.pnpbp.2020.110236
36. Martín J, Padierna Á, Villanueva A, Quintana JM. Evaluation of the mental health of health professionals in the COVID-19 era. What mental health conditions are our health care workers facing in the new wave of coronavirus? Int J Clin Pract. 2021;75(10):1–11. doi:10.1111/ijcp.14607
37. Hummel S, Oetjen N, Du J, et al. Mental health among medical professionals during the COVID-19 pandemic in eight European countries: cross-sectional survey study. J Med Internet Res. 2021;23(1):e24983. doi:10.2196/24983
38. Gómez-Salgado J, Domínguez-Salas S, Romero-Martín M, Romero A, Coronado-Vázquez V, Ruiz-Frutos C. Work engagement and psychological distress of health professionals during the COVID-19 pandemic. J Nurs Manag. 2021;29:1016–1025. doi:10.1111/jonm.13239
39. Xu J, Hui XQ, Wang C, Wang J. Psychological status of surgical staff during the COVID-19 outbreak. Psychiatry Res. 2020;288(April):112955. doi:10.1016/j.psychres.2020.112955
40. Gómez-Salgado J, Ortega-Moreno M, Soriano G, Fagundo-Rivera J, Allande-Cussó R, Ruiz-Frutos C. History of contact with the SARS-COV-2 virus and the sense of coherence in the development of psychological distress in the occupational health professionals in Spain. Sci Prog. 2021;104(2):1–19. doi:10.1177/00368504211026121
41. Instituto Nacional de Estadística del Ministerio de Economía del Gobierno de España. Registered nurses by type of speciality, year and gender; 2020. Available from: https://www.ine.es/jaxi/Tabla.htm?tpx=30726&L=0.
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.