")
Back to Journals » International Journal of General Medicine » Volume 14
Influence of the Interaction Between Depressive Symptoms and Sleep Disorders on Cardiovascular Diseases Occurrence
Received 18 August 2021
Accepted for publication 15 October 2021
Published 24 December 2021 Volume 2021:14 Pages 10327—10335
DOI https://doi.org/10.2147/IJGM.S334894
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Chunyan Wang, Juan Hu
Department of Vascular Surgery, Affiliated Hospital of North Sichuan Medical College, Nanchong, 637000, Sichuan, People’s Republic of China
Correspondence: Chunyan Wang
Department of Vascular Surgery, Affiliated Hospital of North Sichuan Medical College, No. 1 Maoyuan South Road, Nanchong, 637000, Sichuan, People’s Republic of China
Tel +86 15984869299
Email [email protected]
Purpose: Depressive symptoms and sleep disorders were independent risk factors for cardiovascular diseases (CVD). However, few studies have examined the combined effects of depressive symptoms and sleep disorders on CVD. We aimed to evaluate the association between depressive symptoms, sleep disorders and CVD occurrence.
Methods: Data on 30,398 participants were extracted from the National Health and Nutritional Examination Survey (NHANES) database (2005– 2018). Univariate and multivariate analyses were used for assessing the association of depressive symptoms, sleep disorders, and CVD occurrence. Three indexes, including the relative excess risk of interaction (RERI), attributable proportion of interaction (API), and synergy index (SI), were used to analyze the interaction.
Results: Of 30,398 participants, 11,544 (37.98%) participants had CVD and 18,854 (62.02%) did not. Except for gender, the differences were significant between CVD and non-CVD participants in all variables (all P< 0.001). Depressive symptoms [odds ratio (OR)=1.73; 95% confidence intervals (CI):1.57– 1.91] and sleep disorders (OR=1.76; 95% CI:1.65– 1.88) were associated with an increased risk of CVD after adjusting all confounders. Patients with both depressive symptoms and sleep disorders (OR=2.64; 95% CI:2.32– 3.00) had a higher risk of CVD than those without. There may be a synergistic interaction between depression and sleep disorders on the CVD occurrence (SI=1.763; 95% CI:1.299– 2.394), and the proportion of CVD caused by this interaction was 26.9% (API=0.269; 95% CI:0.148– 0.389). In addition, only moderate depressive symptoms may interact with sleep disorders in the occurrence of CVD.
Conclusion: There may be a synergistic interaction between depressive symptoms and sleep disorders, and the synergistic interaction may increase the occurrence of CVD.
Keywords: depressive symptoms, sleep disorders, cardiovascular diseases, interaction
Introduction
Cardiovascular diseases (CVD) are the leading cause of death in the world, and approximately 18 million people die from CVD every year.1,2 The most important behavioral risk factors of CVD were unhealthy diet, lack of physical activity, tobacco use, and alcohol abuse.3 A more comprehensive understanding of the risk factors that can be modified in CVD and their interactions may help prevent CVD. Some potentially modifiable risk factors for CVD, such as sleep, should be noted.
Sleep disorders including sleep-disordered breathing, insomnia and hypersomnia have been reported to be related to the occurrence of CVD.4,5 A systematic review and meta-analysis found that patients with insomnia symptoms had a 45% increased risk of developing or dying from CVD than those without.4 In addition, several studies revealed that depressive symptoms were also associated with the increased risk of CVD.6–8 Bucciarelli et al systematically summarized gender differences in the relationship between depressive symptoms and CVD.9 Both sleep disorders and depressive symptoms have been recognized as risk factors for CVD, and a systematic review indicated that sleep disorders were bidirectionally related to depression.10 Therefore, there may be pathways between depression and sleep disorders that have a common effect on CVD, which may greatly increase the risk of CVD in people who suffer from the both diseases. However, previous studies have focused on depression and sleep disorders as independent predictors for CVD.6–8 Few studies have assessed the risk of CVD in individuals with both depressive symptoms and sleep disorders.
The purpose of this study was to evaluate the association between depressive symptoms, sleep disorders, and the risk of CVD based on the National Health and Nutritional Examination Survey (NHANES) database. We hypothesized that individuals with both depressive symptoms and sleep disorders had a higher risk of CVD than those with independent factors, and that depressive symptoms and sleep disorders had an interaction effect on the occurrence of CVD.
Materials and Methods
Study Design and Data Source
This study was a cross-sectional study. All the data were extracted from the NHANES (2005–2018), a series of nationally representative cross-sectional surveys of the non-institutionalized US population, including interviews and health examinations.11 The information collected was designed to assess the incidence of major diseases and disease risk factors to promote health and prevent diseases.12 Participants who did not have depression questionnaire data or sleep disorder data, or lack other information were excluded. This study did not need to be approved by the Institutional Review Board of the Affiliated Hospital of North Sichuan Medical College because the data was accessed from the NHANES (a publicly available database).
Definition
CVD were defined as suffering from any of the following diseases, including hypertension, heart failure, angina pectoris, coronary heart disease, and heart disease. Sleep disorders were determined according to the item “Have you ever told sleep disorders by doctors or professional health workers” from the NHANES. The measurement of depressive symptoms was conducted through the Patient Health Questionnaire 9 (PHQ-9).13 The severity of depressive symptoms was classified into five categories according to the PHQ-9 scores, including no depressive symptoms (0–4), mild depressive symptoms (5–9), moderate depressive symptoms (10–14), moderately-severe depressive symptoms (15–19), and severe depressive symptoms (20–27).14 In this study, depressive symptoms were defined as PHQ-9 scores ≥10.15
Data Collection
The demographic data of participants were collected, including age, gender, body mass index (BMI), ethnicity (Mexicans, Hispanic, non-Hispanic whites, non-Hispanic blacks, and others), marital status (married, widowed, divorced/separated, and unmarried), education levels (< high school, high school, and > high school), family income (<20,000 $ and ≥20,000 $), as well as the history of alcohol consumption and smoking. In addition, the situation of diabetes mellitus, stroke, sleep disorders, depression and its severity (no, moderate, moderate-to-severe, and severe), and CVD were also recorded. All included participants were divided into CVD group and non-CVD group according to the presence or absence of CVD.
Statistical Analysis
The normally distributed measurement data were expressed as mean ± standard deviation (SD), and the t-test was used for comparison between groups; abnormally distributed measurement data were described as median and quartile [M (Q1, Q3)], and the comparison between groups was conducted by Mann–Whitney U rank-sum test. The enumeration data were presented as numbers and percentages [n (%)], and the Chi-square test or Fisher’s exact test were used for comparison. The variables with statistical significance in the univariate analysis were included in the multivariate logistic regression analysis to assess the association of depression, sleep disorders and their interactions with CVD occurrence. In addition, the interaction based on the additive model was evaluated by three indexes including the relative excess risk of interaction (RERI), attributable proportion of interaction (API), and synergy index (SI).16 When 0 was contained in the 95% confidence interval (CI) of RERI and API, or 1 was involved in the 95% CI of SI, there was no interaction.
SAS software (version 9.4, SAS Institute Inc., Cary, NC, USA) was used to analyze the data, and R software (version 4.2) was used to draw the forest plots with odds ratio (OR) and interaction schematic diagrams. All statistical analyses were used the two-sided test, and P < 0.05 was considered statistically significant.
Results
Characteristics of Participants
There were 39,822 participants extracted from the NHANES database between 2005 and 2018. After excluding 5693 participants with missing depression questionnaire data, 26 with missing sleep disorder data, and 3705 with incomplete information, 30,398 participants were included in this study. Of these included participants, 14,995 (49.33%) were males and 15,403 (50.67%) were females; the median age of all participants was 49 (34, 64) years, and the mean BMI was 29.25 ± 7.00 kg/m2; 11,544 (37.98%) participants had CVD, while 18,854 (62.02%) did not. In addition, 7836 (25.78%) participants had sleep disorders, and 2637 (8.67%) participants had depressive symptoms (PHQ-9≥10). Among these participants with depressive symptoms, 1642 (5.40%) had moderate depressive symptoms, 710 (2.34%) had moderate-to-severe depressive symptoms, and 258 (0.94%) had severe depressive symptoms. The detailed characteristics of all participants were shown in Table 1.
 |
Table 1 Baseline Characteristics of Participants |
Difference Between CVD and Non-CVD Patients
Univariate analysis was used to assess the difference between CVD and non-CVD patients (Table 2). The results indicated that patients with CVD had older age (Z=81.639, P<0.001), and higher BMI (t=36.15, P<0.001), and occupied a higher proportion of smoking (χ2=261.744, P<0.001), diabetes mellitus (χ2=2686.306, P<0.001), stroke (χ2=1030.445, P<0.001), sleep disorders (χ2=925.814, P<0.001) and depressive symptoms (χ2=925.814, P<0.001) in comparison with those without. Compared with non-CVD patients, CVD patients had lower education levels (χ2=107.479, P<0.001), lower family incomes (χ2=266.503, P<0.001), and no history of alcohol consumption (χ2=138.355, P<0.001). In addition, significant differences were also observed between CVD and non-CVD patients in ethnicity (χ2=537.055, P<0.001) and marital status (χ2=1917.418, P<0.001).
 |
Table 2 Comparison on the Baseline Characteristic of CVD and Non-CVD Patients |
Association Between Depressive Symptoms and CVD
The association of depressive symptoms with CVD was described in Figure 1. The results showed that the risk of CVD in patients with depressive symptoms was 1.79 times (OR=1.79; 95% CI:1.65–2.35) that in those without. After adjusting for age and gender (model 2), the patients with depressive symptoms had an increased risk of CVD than those without times (OR=2.21; 95% CI:2.02–2.42). In addition, the risk of CVD in patients with depressive symptoms (OR=1.73; 95% CI:1.57–1.91) was still present when all the confounders (model 3), including age, gender, BMI, ethnicity, marital status, educational levels, family income, diabetes mellitus, the history of alcohol consumption and smoking, were adjusted.
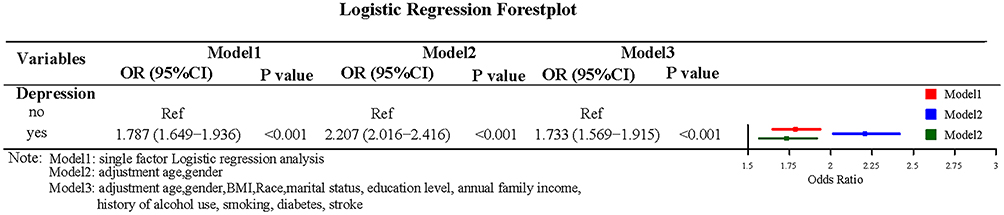 |
Figure 1 Logistic regression forest plot of the association of depressive symptoms with cardiovascular diseases (CVD). |
Association Between Sleep Disorders and CVD
Univariate analysis found that the risk of CVD in patients with sleep disorders was 1.23 times (OR=2.23; 95% CI:2.12–2.35) greater than those without. The multivariate analysis showed that patients with sleep disorders had a higher risk of CVD than those without after adjusting age and gender (OR=2.09; 95% CI:1.97–2.21). When all the confounders were adjusted, the risk of CVD in patients with sleep disorders was 0.76 times (OR=1.76; 95% CI:1.65–1.88) higher than those without. The association of sleep disorders with CVD is shown in Figure 2.
 |
Figure 2 Logistic regression forest plot of the association between sleep disorders and CVD. |
Influence of the Interaction Between Depressive Symptoms and Sleep Disorders on CVD
The additive interaction terms of depressive symptoms and sleep disorders were constructed, including no depressive symptoms and no sleep disorders, no depressive symptoms and sleep disorders, depressive symptoms and no sleep disorders, depressive symptoms and sleep disorders. The sample size of each interaction term is exhibited in Table 3.
 |
Table 3 Characteristics of Interaction Terms Between Depressive Symptoms and Sleep Disorders |
The results illustrated that the risk of CVD in patients with both depressive symptoms and sleep disorders was 3.02 times (OR=3.02; 95% CI:2.71–3.35) that of those without. In multivariate analysis, the patients with both depressive symptoms and sleep disorders were found to have a significantly elevated risk of CVD than those without after adjusting for age and gender (OR=3.54; 95% CI:3.15–3.98), and this risk still existed when all the confounders were adjusted (OR=2.64; 95% CI:2.32–3.00; Table 4). The logistic regression analysis indicated that the interactive indexes in three models [single factor (model 1), adjusted age and gender (model 2), and adjusted all confounders (model 3)] were as follows: RERImodel1 (0.587; 95% CI, 0.225–0.948), RERImodel2 (1.020; 95% CI, 0.554–1.486), RERImodel3 (0.710; 95% CI, 0.326–1.094); APImodel1 (0.194; 95% CI, 0.090–0.298), APImodel2 (0.288; 95% CI, 0.182–0.394), APImodel3 (0.269; 95% CI, 0.148–0.389); SImodel1 (1.410; 95% CI, 1.142–1.740), SImodel2 (1.672; 95% CI, 1.327–2.107), SImodel3 (1.763; 95% CI, 1.299–2.394). The 95% CIs of RERI and API suggested that there may be a synergistic interaction between depression and sleep disorders on the CVD occurrence. In addition, the API was 0.269 after adjusting all confounders, indicating that the proportion of CVD that may be caused by the interaction of depression and sleep disorders was 26.9% in all CVD patients. Detailed results are shown in Table 4 and Figure 3.
 |
Table 4 Logistic Regression Analysis of the Interactive Items Between Depressive Symptoms and Sleep Disorders |
 |
Figure 3 Interaction schematic diagram between depressive symptoms and sleep disorders after adjusting for multiple confounders. |
Interaction of Depressive Symptoms and Sleep Disorders on CVD Based on the Severity of Depression
Further analysis was conducted to assess the effect of interaction between different severity of depressive symptoms and sleep disorders on CVD (Table 5). After adjusting for all confounders, the results revealed that only moderate depressive symptom [RERImodel3 (0.701; 95% CI, 0.237–1.165), APImodel3 (0.278; 95% CI, 0.129–0.427), SImodel3 (1.858; 95% CI, 1.244–2.77)] may interact with sleep disorders in occurrence of CVD (Figure 4).
 |
Table 5 Logistic Regression Analysis of the Interactive Items Between Depression Severity and Sleep Disorders |
 |
Figure 4 Interaction schematic diagram between moderate depressive symptoms and sleep disorders after correction of multiple confounders. |
Discussion
In this study, we evaluated the associations between depressive symptoms, sleep disorders and the risk of CVD occurrence based on the NHANES database. This study verified that depressive symptoms and sleep disorders were independent risk factors for CVD, and found that depressive symptoms and sleep disorders may play a synergistic interaction in the occurrence of CVD. The proportion of CVD that may be caused by the interaction of depression and sleep disorders was 26.9% in all CVD patients. Among the different depressive symptoms, only moderate depressive symptoms may interact with sleep disorders in the occurrence of CVD.
The association of depression or sleep disorders with CVD has been reported by many studies.7,17–19 In this study, the risk of CVD in individuals with independent depressive symptoms and sleep disorders was 1.73 times and 1.76 times that of those without, respectively. Our results were generally consistent with previous studies that assessed the association of depressive symptoms20 or sleep disorders21 with the risk of CVD. In addition, the study of Matsuda et al found that there was an association between sleep quality and depression in CVD patients.22 Both sleep disorders and depression have been identified as risk factors for CVD, but their joint effects on CVD were rarely studied. The present results revealed that participants with both depressive symptoms and sleep disorders had 1.64 times higher risk of CVD than those without after adjusting for all confounders. The possible synergistic interaction between depressive symptoms and sleep disorders for the development of CVD was analyzed in this study. This finding may provide evidence for the risk of CVD. In addition, only moderate depressive symptoms may interact with sleep disorders in the development of CVD. However, more prospective clinical studies are needed to make possible explanations.
The interaction of depressive symptoms and sleep disorders on the occurrence of CVD may be explained by biological and behavioral pathways. There were several common pathways in the association mechanism of depressive symptoms, sleep disorders and CVD, including inflammation, coagulation system, and autonomic nervous system.19,23 Inflammation plays an important role in the relationship between sleep disorders, depressive symptoms and CVD, and it may be a pathway linking sleep disorders and depressive symptoms to CVD.24 For instance, sleep disorders can activate some inflammatory factors to promote the formation of the body’s inflammatory microenvironment,25,26 which was also related to depression and CVD.27,28 In terms of the coagulation system, sleep disorders and depression in patients with CVD were all related to the coagulation system. The study of Bikov et al indicated that the increased risk of CVD from sleep disorders may be associated with accelerated blood clotting and platelet activation.29 Patients with depression may have increased platelet activation, which was thought to contribute to the development of atherosclerosis and peripheral artery disease.30,31 Activation of the coagulation system by depressive symptoms and sleep disorders may be another common pathway to increase the risk of CVD. In addition, sleep disorders and depression were also associated with increased activity of the autonomic nervous system, which may be a mechanism of increasing the risk of CVD.32–34 Three possible mechanisms have been mentioned in the impact of the interaction of depressive symptoms and sleep disorders on CVD development. However, the establishment of these mechanism requires more prospective clinical studies to verify.
Our study analyzed the synergistic interaction between depressive symptoms and sleep disorders on CVD occurrence. In addition, the present results were convincing because this study was based on the nationally representative NHANES database with a large sample size. However, this study had some limitations. First, this study was a cross-sectional study that cannot confirm the causal relationship between the interaction of depressive symptoms and sleep disorders and CVD occurrence, and stronger evidence relies on prospective cohort studies. Second, the history of CVD and sleep disorders in the NHANES were based on the self-reported data of participants. The authenticity of the self-reported data may be questionable. However, several studies have shown that the risk factors of CVD have been determined through self-reported data from the NHANES.35–37 These studies validated the reliability of the self-reported data.
Conclusion
Depressive symptoms and sleep disorders were independent risk factors for CVD occurrence, and there may be a synergistic interaction between depressive symptoms and sleep disorders to increase the occurrence of CVD. In addition, there may be common pathways between depressive symptoms and sleep disorders that lead to the occurrence of CVD. However, more prospective clinical studies should be conducted to further validate our results and explore the mechanisms by which these results occur.
Ethics Approval and Informed Consent
This study did not need to be approved by the Institutional Review Board of the Affiliated Hospital of North Sichuan Medical College because the data was accessed from NHANES (a publicly available database).
Consent for Publication
Informed consent was not needed for this study.
Author Contributions
All authors contributed to data analysis, drafting or revising the article, have agreed on the journal to which the article will be submitted, gave final approval of the version to be published, and agree to be accountable for all aspects of the work.
Funding
There was no funding to report.
Disclosure
The authors reported no conflicts of interest in this work.
References
1. GBD 2017 Causes of Death Collaborators. Global, regional, and national age-sex-specific mortality for 282 causes of death in 195 countries and territories, 1980–2017: a systematic analysis for the Global Burden of Disease Study 2017. Lancet. 2018;392:1736–1788. doi:10.1016/S0140-6736(18)32203-7
2. Dagenais GR, Leong DP, Rangarajan S, et al. Variations in common diseases, hospital admissions, and deaths in middle-aged adults in 21 countries from five continents (PURE): a prospective cohort study. Lancet. 2020;395(10226):785–794. doi:10.1016/S0140-6736(19)32007-0
3. Krist AH, Davidson KW, Mangione CM, et al. Behavioral counseling interventions to promote a healthy diet and physical activity for cardiovascular disease prevention in adults with cardiovascular risk factors: US preventive services task force recommendation statement. JAMA. 2020;324(20):2069–2075. doi:10.1001/jama.2020.21749
4. Sofi F, Cesari F, Casini A, et al. Insomnia and risk of cardiovascular disease: a meta-analysis. Eur J Prev Cardiol. 2014;21(1):57–64. doi:10.1177/2047487312460020
5. Javaheri S, Redline S. Insomnia and risk of cardiovascular disease. Chest. 2017;152(2):435–444. doi:10.1016/j.chest.2017.01.026
6. Carney RM, Freedland KE. Depression and coronary heart disease. Nat Rev Cardiol. 2017;14(3):145–155. doi:10.1038/nrcardio.2016.181
7. Harshfield EL, Pennells L, Schwartz JE, et al. Association between depressive symptoms and incident cardiovascular diseases. JAMA. 2020;324(23):2396–2405. doi:10.1001/jama.2020.23068
8. Wium-Andersen MK, Wium-Andersen IK, Prescott EIB, et al. An attempt to explain the bidirectional association between ischaemic heart disease, stroke and depression: a cohort and meta-analytic approach. Br J Psychiatry. 2020;217(2):434–441. doi:10.1192/bjp.2019.130
9. Bucciarelli V, Caterino AL, Bianco F, et al. Depression and cardiovascular disease: the deep blue sea of women’s heart. Trends Cardiovasc Med. 2020;30:170–176. doi:10.1016/j.tcm.2019.05.001
10. Alvaro PK, Roberts RM, Harris JK. A systematic review assessing bidirectionality between sleep disturbances, anxiety, and depression. Sleep. 2013;36:1059–1068. doi:10.5665/sleep.2810
11. Zipf G, Chiappa M, Porter KS, et al. National health and nutrition examination survey: plan and operations, 1999–2010. Vital Health Stat. 2013;1:1–37.
12. Mitchell W, Bhatia R, Zebardast N. Retrospective cross-sectional analysis of the changes in marijuana use in the USA, 2005–2018. BMJ Open. 2020;10:e037905. doi:10.1136/bmjopen-2020-037905
13. Kung S, Alarcon RD, Williams MD, et al. Comparing the Beck Depression Inventory-II (BDI-II) and Patient Health Questionnaire (PHQ-9) depression measures in an integrated mood disorders practice. J Affect Disord. 2013;145(3):341–343. doi:10.1016/j.jad.2012.08.017
14. Kroenke K, Spitzer RL, Williams JB. The PHQ-9: validity of a brief depression severity measure. J Gen Intern Med. 2001;16:606–613. doi:10.1046/j.1525-1497.2001.016009606.x
15. Jorgensen D, White GE, Sekikawa A, et al. Higher dietary inflammation is associated with increased odds of depression independent of Framingham risk score in the national health and nutrition examination survey. Nutr Res. 2018;54:23–32. doi:10.1016/j.nutres.2018.03.004
16. Knol MJ, VanderWeele TJ. Recommendations for presenting analyses of effect modification and interaction. Int J Epidemiol. 2012;41(2):514–520. doi:10.1093/ije/dyr218
17. Meng R, Yu C, Liu N, et al. Association of depression with all-cause and cardiovascular disease mortality among adults in China. JAMA Netw Open. 2020;3(2):e1921043. doi:10.1001/jamanetworkopen.2019.21043
18. Petrovic D, Haba-Rubio J, de Mestral Vargas C, et al. The contribution of sleep to social inequalities in cardiovascular disorders: a multi-cohort study. Cardiovasc Res. 2020;116(8):1514–1524. doi:10.1093/cvr/cvz267
19. Tobaldini E, Fiorelli EM, Solbiati M, et al. Short sleep duration and cardiometabolic risk: from pathophysiology to clinical evidence. Nat Rev Cardiol. 2019;16(4):213–224. doi:10.1038/s41569-018-0109-6
20. Van der Kooy K, van Hout H, Marwijk H, et al. Depression and the risk for cardiovascular diseases: systematic review and meta analysis. Int J Geriatr Psychiatry. 2007;22(7):613–626. doi:10.1002/gps.1723
21. Dikeos D, Georgantopoulos G. Medical comorbidity of sleep disorders. Curr Opin Psychiatry. 2011;24:346–354. doi:10.1097/YCO.0b013e3283473375
22. Matsuda R, Kohno T, Kohsaka S, et al. The prevalence of poor sleep quality and its association with depression and anxiety scores in patients admitted for cardiovascular disease: a cross-sectional designed study. Int J Cardiol. 2017;228:977–982. doi:10.1016/j.ijcard.2016.11.091
23. Nemeroff CB, Goldschmidt-Clermont PJ. Heartache and heartbreak–the link between depression and cardiovascular disease. Nat Rev Cardiol. 2012;9:526–539. doi:10.1038/nrcardio.2012.91
24. McDade TW, Hawkley LC, Cacioppo JT. Psychosocial and behavioral predictors of inflammation in middle-aged and older adults: the Chicago health, aging, and social relations study. Psychosom Med. 2006;68:376–381. doi:10.1097/01.psy.0000221371.43607.64
25. Irwin MR, Witarama T, Caudill M, et al. Sleep loss activates cellular inflammation and signal transducer and activator of transcription (STAT) family proteins in humans. Brain Behav Immun. 2015;47:86–92. doi:10.1016/j.bbi.2014.09.017
26. Sauvet F, Drogou C, Bougard C, et al. Vascular response to 1 week of sleep restriction in healthy subjects. A metabolic response? Int J Cardiol. 2015;190:246–255. doi:10.1016/j.ijcard.2015.04.119
27. Lamers F, Milaneschi Y, Smit JH, et al. Longitudinal association between depression and inflammatory markers: results FROM the Netherlands Study of Depression and Anxiety. Biol Psychiatry. 2019;85(10):829–837. doi:10.1016/j.biopsych.2018.12.020
28. Liberale L, Montecucco F, Schwarz L, et al. Inflammation and cardiovascular diseases: lessons from seminal clinical trials. Cardiovasc Res. 2021;117(2):411–422. doi:10.1093/cvr/cvaa211
29. Bikov A, Meszaros M, Schwarz EI. Coagulation and fibrinolysis in obstructive sleep apnoea. Int J Mol Sci. 2021;22:2834.
30. Ramirez JL, Drudi LM, Grenon SM. Review of biologic and behavioral risk factors linking depression and peripheral artery disease. Vasc Med. 2018;23(5):478–488. doi:10.1177/1358863X18773161
31. Sanner JE, Frazier L. The role of serotonin in depression and clotting in the coronary artery disease population. J Cardiovasc Nurs. 2011;26(5):423–429. doi:10.1097/JCN.0b013e3182076a81
32. Tobaldini E, Costantino G, Solbiati M, et al. Sleep, sleep deprivation, autonomic nervous system and cardiovascular diseases. Neurosci Biobehav Rev. 2017;74:321–329. doi:10.1016/j.neubiorev.2016.07.004
33. Kop WJ, Stein PK, Tracy RP, et al. Autonomic nervous system dysfunction and inflammation contribute to the increased cardiovascular mortality risk associated with depression. Psychosom Med. 2010;72(7):626–635. doi:10.1097/PSY.0b013e3181eadd2b
34. Tobaldini E, Carandina A, Toschi-Dias E, et al. Depression and cardiovascular autonomic control: a matter of vagus and sex paradox. Neurosci Biobehav Rev. 2020;116:154–161. doi:10.1016/j.neubiorev.2020.06.029
35. Kim DH, Sabour S, Sagar UN, et al. Prevalence of hypovitaminosis D in cardiovascular diseases (from the national health and nutrition examination survey 2001 to 2004). Am J Cardiol. 2008;102(11):1540–1544. doi:10.1016/j.amjcard.2008.06.067
36. Yoon SS, Dillon CF, Illoh K, et al. Trends in the prevalence of coronary heart disease in the U.S.: national health and nutrition examination survey, 2001–2012. Am J Prev Med. 2016;51:437–445. doi:10.1016/j.amepre.2016.02.023
37. Zhang Y, Huang M, Zhuang P, et al. Exposure to acrylamide and the risk of cardiovascular diseases in the national health and nutrition examination survey 2003–2006. Environ Int. 2018;117:154–163. doi:10.1016/j.envint.2018.04.047
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.