")
Back to Journals » Clinical Epidemiology » Volume 10
Influence of socioeconomic factors and region of residence on cancer stage of malignant melanoma: a Danish nationwide population-based study
Authors Ibfelt EH , Steding-Jessen M, Dalton SO , Lundstrøm SL , Osler M , Hölmich LR
Received 20 December 2017
Accepted for publication 14 February 2018
Published 10 July 2018 Volume 2018:10 Pages 799—807
DOI https://doi.org/10.2147/CLEP.S160357
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Irene Petersen
Else Helene Ibfelt,1,2 Marianne Steding-Jessen,1 Susanne Oksbjerg Dalton,3 Sanne Lykke Lundstrøm,2 Merete Osler,2 Lisbet Rosenkrantz Hölmich4
1The Danish Clinical Registries, Department for Cancer and Cancer Screening, Frederiksberg, Denmark; 2Center for Clinical Research and Prevention, Bispebjerg and Frederiksberg Hospital, Frederiksberg Denmark; 3Danish Cancer Society Research Center, Department of Cancer Survivorship, Copenhagen, Denmark; 4Department for Plastic Surgery, Herlev University Hospital, Copenhagen, Denmark
Background: Socioeconomic differences in survival after melanoma may be due to late diagnosis of the disadvantaged patients. The aim of the study was to examine the association between educational level, disposable income, cohabitating status and region of residence with stage at diagnosis of melanoma, including adjustment for comorbidity and tumor type.
Methods: From The Danish Melanoma Database, we identified 10,158 patients diagnosed with their first invasive melanoma during 2008–2014 and obtained information on stage, localization, histology, thickness and ulceration. Sociodemographic information was retrieved from registers of Statistics Denmark and data on comorbidity from the Danish National Patient Registry. We used logistic regression to analyze the associations between sociodemographic factors and cancer stage.
Results: Shorter education, lower income, living without partner, older age and being male were associated with increased odds ratios for advanced stage of melanoma at time of diagnosis even after adjustment for comorbidity and tumor type. Residence in the Zealand, Central and Northern region was also associated with advanced cancer stage.
Conclusion: Socioeconomically disadvantaged patients and patients with residence in three of five health care regions were more often diagnosed with advanced melanoma. Initiatives to increase early detection should be directed at disadvantaged groups, and efforts to improve early diagnosis of nodular melanomas during increased awareness of the Elevated, Firm and Growing nodule rule and “when in doubt, cut it out” should be implemented. Further studies should investigate regional differences in delay, effects of number of specialized doctors per inhabitant as well as differences in referral patterns from primary to secondary health care across health care regions.
Keywords: melanoma, cancer stage, sociodemographic factors, comorbidity, Denmark, early cancer detection
Introduction
The incidence of melanoma in Denmark has increased with over 4% per year during the past 25 years and by 2012, the yearly incidence was ~30 per 100,000 person-years.1 Melanoma is the fourth and sixth most common cancer type, respectively, in women and men in Denmark.2 Despite a higher incidence rate among persons with higher socioeconomic position, lower socioeconomic position has been associated with poorer survival in this patient group,3–5 and we need to know more about where in the cancer pathway these survival disparities occur. A possible explanation is delayed diagnosis in patients with lower socioeconomic position, and more knowledge is needed in order to detect cancer early in all patient groups and to identify groups at high risk of delayed diagnosis.
A late diagnosis may result in advanced cancer stage at time of diagnosis, and hypothesized explanations are delay in recognizing symptoms of the cancer, delayed health care seeking or later referral to specialized care among patients with lower socioeconomic position. The presence of other chronic disease, which is more frequent among patients with lower socioeconomic position, may influence timing of cancer diagnosis either through an increased observation because of more frequent health care contacts due to the health condition in question or conversely by decreasing individual resources in order to manage further health problems. Histological type of the tumor may also be differentially distributed according to socioeconomic group because some tumor types occur mainly among people with a certain lifestyle or risk behavior in relation to sun exposure.
Furthermore, patients with lower socioeconomic position also tend to live in more rural rather than urban areas, where access to health care services may be lower.
Several studies have shown that patients living in neighborhood areas with lower socioeconomic position tended to be diagnosed at a later stage of melanoma.4 Besides results from two Swedish studies,6,7 evidence is sparse from nationwide, population-based studies about the effect of individual level socioeconomic factors, such as education and income, on stage of cancer in melanoma patients. The role of comorbidity has only rarely been investigated, and only a few studies have looked at major geographical differences in combination with the socioeconomic factors.
This study presents results from Denmark where most primary and secondary health care services including all cancer treatments are tax-paid and thereby free of charge, with the aim of minimizing differential access to diagnosis and treatments. A referral from primary to secondary care is required, and the general practitioners play the role of gatekeepers to the rest of the health care system. Data are obtained from a nationwide Clinical Quality register with a coverage of ~95% of all Danish patients with melanoma in recent years8 and unique individual socioeconomic information from national administrative registers. The aim of the study was to investigate whether educational level, disposable income, cohabitating status or region of residence is associated with cancer stage and further to analyze the role of comorbidity and tumor type in these potential relations.
Methods
Study population
From the Danish Melanoma Database (DMD), we identified 13,626 patients diagnosed with their first invasive melanoma between 2008 and 2014. DMD is a clinical register containing prospective and systematically collected data related to clinical observations, diagnostic procedures, tumor characteristics, treatments and outcomes. It was established in 1985 and now has a national coverage of ~93–96%.8
Clinical variables
Information on cancer T-, N- and M-stage; tumor location; histological subtype; tumor thickness; and ulceration was obtained from the DMD. The clinical stage at diagnosis was categorized according to AJCC’s 6th (2008–2013) and 7th edition (2013–2014),9,10 and for the analyses, cancer stage was divided into early (clinical stage I–IIA) and advanced-stage cancer (clinical stage IIB–IV). This cut-point is in accordance with the Danish follow-up program for melanoma, where stage IA is assessed as low-risk cancer and IB–IIA as intermediate-risk cancer, while stage IIB–IV include the thickest tumors (stage IIB and IIC), with regional spread (stage III) or distant metastases (stage IV), all of which have the highest risk of relapse and dismal outcome.11 Tumors were grouped into histological subtypes: superficial spreading malignant melanoma, lentigo maligna melanoma, nodular melanoma, other and unknown/unclassified.
Data on comorbid conditions were obtained from the Danish National Patient Register, which is an administrative register containing data from all hospitalizations at somatic wards in Denmark since 1977.12 Diagnoses other than melanoma were retrieved, and the Charlson comorbidity index (CCI)13 was calculated. The CCI covers 19 selected conditions with a score from 1 to 6 by degree of severity, and these conditions were summed from 10 years before and until 1 year before date of the melanoma diagnosis. The CCI index was grouped into 0 (none), 1–2 and 3+.
Sociodemographic variables
Individual level sociodemographic factors were obtained by linking the unique personal identification number (assigned to all Danish residents) of the study population to the registers of Statistics Denmark, which contains data on each individual and is updated annually.14–16 We retrieved information on educational level, income and cohabiting status 1 year before diagnosis for each patient.
Education was divided into three categories based on Statistics Denmark’s recommendations of categorizing the individual’s highest attained education level: short education (7/9–12 years of basic or youth education), medium education (10–12 years of vocational education) and longer education (short, medium and longer higher education [>13 years of education]).
Yearly disposable income per adult person in the household was calculated and categorized in to three groups based on quartiles of the disposable income per person in the population: 1st quartile (<150.708 Danish crowns [DKK]), 2nd–3rd quartile (150.708–279.715 DKK) and 4th quartile (>279.715 DKK). Persons with high negative income (>50.000 DKK) were excluded from the analyses. One thousand DKK equals ~135 Euros.
Cohabiting status was defined as living with a partner (married or cohabiting) or living without a partner (single, widow/widower or divorced). Cohabiting was defined as, in the absence of marriage, two adults of the opposite sex, with a maximum age difference of 15 years, living at the same address and who have no family relation or with a mutual child.
Information about age, sex and region of residence was obtained from the Civil Registration System.16
From the study population, we excluded 105 patients because there was no match on any sociodemographic information, and further 178 persons were excluded because they had high negative income in Statistics Denmark’s registers. Further 328 patients under the age of 25 years were excluded as those persons might not have reached their final educational level. This yielded 13,015 patients (Table 1). For the adjusted analysis, 2,597 patients (20%) with missing TNM information or unclassifiable clinical stage and 260 patients with unknown educational level were excluded, which resulted in a study group of 10,158 patients (Table 2).
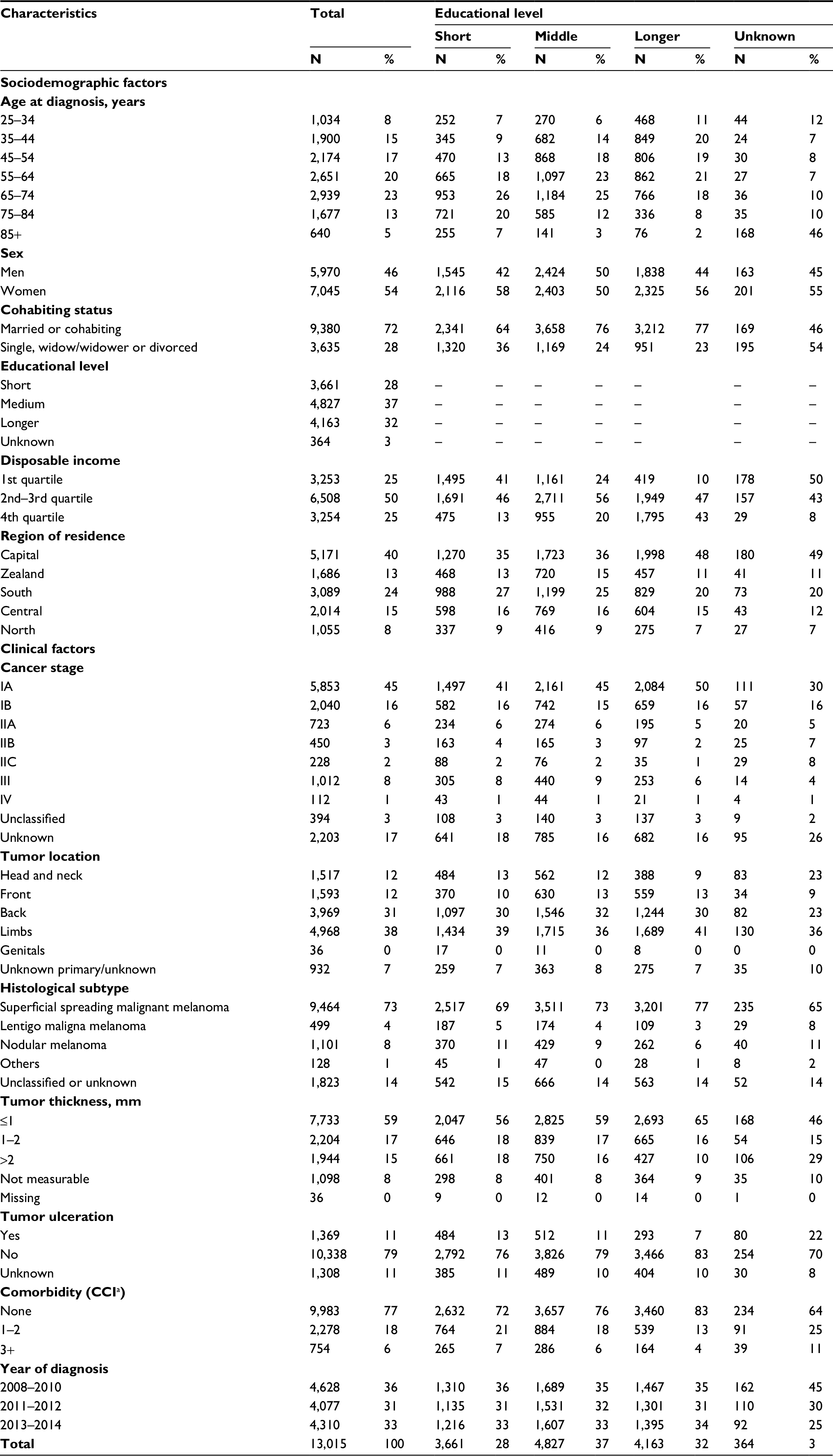 | Table 1 Disease and sociodemographic characteristics of 13,015 Danish melanoma patients diagnosed between 2008 and 2014 Note: aCCI includes 19 selected diseases scored by degree of severity and summed to the CCI score. Abbreviation: CCI, Charlson comorbidity index. |
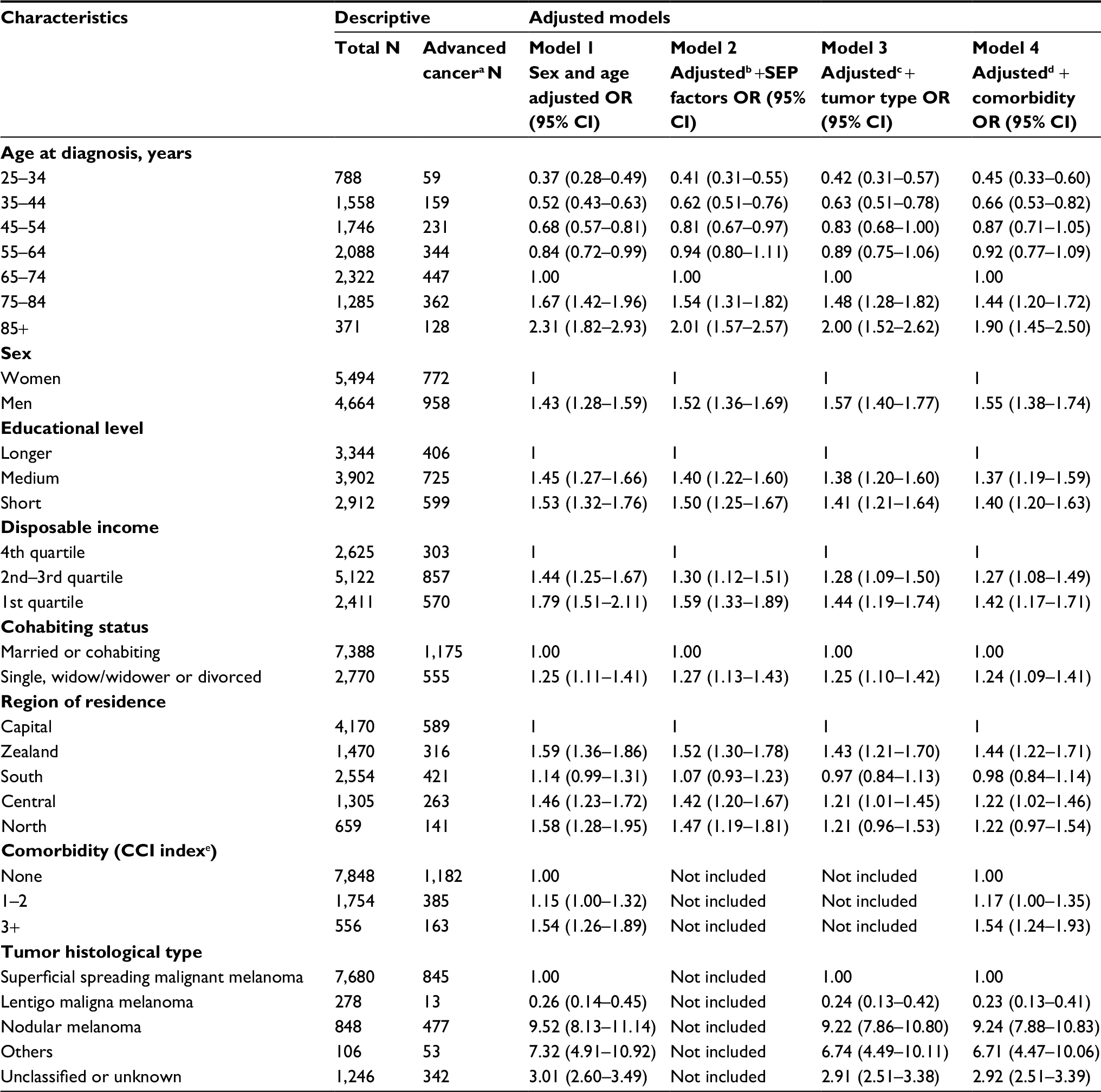 | Table 2 Associations between socioeconomic and -demographic factors with cancer stage at diagnosis in 10,158 melanoma patients (ORs [95% CI]) for advanced vs. early cancera) Notes: aAdvanced cancer defined as TNM stage IIB–IV and early cancer defined as TNM stage I–IIA. bAdjustments as in model 1 and further mutually adjusted for SEP factors (educational level, disposable income, cohabiting status and region of residence). Only education is not adjusted for income, as this is considered a clear mediator of the association between education and cancer stage. cAdjustments as in model 2 and further adjusted for tumor histological type. dAdjustments as in model 3 and further adjusted for comorbidity (CCI). eCCI includes 19 selected diseases scored by degree of severity and summed to the CCI score. Abbreviations: OR, odds ratio; CCI, Charlson comorbidity index; SEP, socioeconomic position. |
Statistical analyses
The associations between socioeconomic and -demographic factors and cancer diagnosis stage were analyzed in a series of logistic regression models. First, the associations between sociodemographic factors and cancer stage were adjusted for age and sex. Second, the results were mutually adjusted for other sociodemographic factors, except for educational level, which was not adjusted for income, because income was hypothesized to be a clear mediator between education and cancer stage. Third, the model included additional adjustment for tumor type and the fourth model also adjusted for comorbidity (CCI index).
Interactions between single socioeconomic variables with sex, age, comorbidity and localization of the tumor were tested one pair at a time with Wald test statistics. A significant interaction existed between education and comorbidity with a higher effect of comorbidity on stage for patients with longer compared to short education; however, this was driven by a very small group of patients with long education level and comorbidity 3+ and therefore results were not stratified on this basis. There was an interaction between sex and cohabiting status; however, only borderline significant (P < 0.07) and sex-stratified data are not shown.
Because data completeness was higher in 2013–2014 (start of the DMD as a clinical quality register) than in 2008–2012, we repeated the analyses including only these two most recent years to assure that the interpretation of the results were close to what was found from analyzing the whole cohort.
In supplementary analyses, we repeated all the analyses with the outcome variable clinical stage dichotomized into stage I vs II–IV in order to assure that results were the same even if the cut-point for early vs advanced cancer was changed. This yielded estimates that were close to what is reported in Table 2, and the interpretation of the results from the two categorizations was the same.
The analyses were carried out in SAS 9.4 with the PROC GENMOD procedure, and the level of significance was P < 0.05.
Ethics
Use of data for this project was approved by the Danish Health Authorities under the Capital Region of Denmark (J.no.: 2012-58-0004).
Results
The descriptive statistics in Table 1 show clinical and sociodemographic factors distributed according to the main exposure of interest: educational level. More patients with short compared to long education tended to have higher cancer stages, and thereby also thicker tumors and ulceration, and more short-educated patients had nodular malignant melanoma and comorbidity. Patients with shortest education also tended to have higher age, lower income, lived alone and outside the Capital Region.
Table 2 shows that patients with shorter education, with lower income, living without partner, with male sex, higher age, with comorbidity and who lived in the Northern, Central or Zealand region of Denmark had an elevated odds ratio (OR) of being diagnosed with advanced-stage cancer when adjusted for sex, age and sociodemographic factors. For example, the OR for advanced-stage cancer in patients with short compared to longest education was 1.50 (1.25–1.67) and for lowest vs highest income level OR was 1.59 (1.33–1.89), while OR for advanced cancer stage was 1.52 (1.30–1.78) for patients living in Zealand compared to the Capital region (Table 2, model 2).
When adjusting for tumor type and comorbidity (Table 2, models 3 and 4, respectively), the ORs for advanced-stage cancer by socioeconomic and -demographic factors were only a little lower than the ORs in model 2, ie, for short vs longer education the adjusted OR was 1.40 (1.20–1.63) in the fully adjusted model. The estimates for region of residence were lower when adjusted for tumor type (model 3) than the confounder-adjusted estimates (model 2); however, this reduction in ORs was not found when restricting data to patients with diagnosis year 2013–2014 (data not shown).
Patients with high comorbidity burden had a higher OR of advanced cancer (comorbidity 3+ vs no comorbidity, adjusted OR = 1.54 [1.24–1.93]).
Discussion
The results of the present study showed that patients who were socially disadvantaged in terms of education, income or partner status had an increased risk of a diagnosis with advanced-staged melanoma. Region of residence was also associated with a higher risk of advanced stage when living in the Northern, Central or Zealand health care region. The effects of the socioeconomic factors seemed unexplained by differential distribution of comorbidity or tumor types among different socioeconomic groups.
It is an important finding that several different indicators of socioeconomic position were related to cancer stage at diagnosis, and this adds evidence to the current literature. Studies from USA, Europe and New Zealand consistently showed that patients living in neighborhood areas with lower socioeconomic position tended to be diagnosed with a more advanced stage of melanoma.4,17–20 These studies were, however, based on socioeconomic measures at area level, with the risk of misclassification. Larger differences in health outcomes may be found in populations from USA because of an insurance-based vs the mostly tax-based health care systems that exist in especially the Northern European countries, which should be considered when directly comparing inequality results. A nationwide population-based Swedish study with individually measured educational information reported a dose–response relation between three levels of education and disease stage with effect estimates close to our results.7 Besides this, a few other smaller studies linked data on individual level education to tumor thickness, which is a measure of locally advancement of the disease and reported short education and unemployment to be associated with thick tumors.4
Being married or living with a partner has earlier been associated with an early diagnosis of melanoma.4,21 In a nationwide population-based Swedish study, findings of advanced disease in single living were most pronounced among men.6 We found a similar trend of sex difference (data not shown), and especially men living without a partner seem to be a vulnerable group in terms of diagnostic delay.
A questionnaire study from USA on the link from socioeconomic position to advanced melanoma points to the following underlying reasons for such an association: patients with short education were more likely to believe that melanoma was not very serious, they had less knowledge of skin symptoms of melanoma, they were less likely to have routinely examined their skin and to have ever been told by a physician that they had atypical moles or that they were at risk of skin cancer, or had been instructed by a physician how to look for signs of melanoma.22 However, results from older studies from the Northern Europe are conflicting on the association between socioeconomic position and knowledge and understanding of melanoma. Other studies indicate that higher socioeconomic position is associated with more use of specialist health care services in general,23 and a lower access to specialist dermatologist or specialized hospital treatment among patients with lower socioeconomic position could be an explaining factor for their delayed diagnosis.
Taking several socioeconomic factors into account, we found that patients with residency in three out of five geographical health care regions had a higher risk of advanced-stage cancer. In a recent Swedish study, differences in stage distribution were found across smaller geographical areas,24 and further in the population-based Swedish study, rural/other urban areas had higher melanoma-specific survival compared to metropolitan areas.7 Each of the five Danish Regions has responsibility for primary and secondary health care, and the organization of the referral to specialized care might thus be different between regions. Furthermore, the outer areas of Denmark have less primary and specialized doctors per inhabitant and longer distances to care. For instance, in the Zealand region, there is currently what corresponds to ~16 specialized treatment centers for dermatology/plastic surgery compared to ~27 centers per 100,000 inhabitants in the Capital Region.25 That being said, region of residence may also be a mixture of unmeasured social factors and cultural/behavioral factors as well as a measure of organization of care.
Comorbidity did not seem to explain the socioeconomic difference in stage at diagnosis, although it was a significant independent risk factor for being diagnosed with advanced cancer. The findings point to lower awareness or decreased resources in terms of dealing with another health problem than the comorbid disorder. A similar association was found for melanoma screening in primary practice in France, where chronic disease was associated with non-participation.26 A Danish population-based study showed interaction between comorbidity and cancer stage with an increased mortality among patients with advanced melanoma and high comorbidity,27 underlining the importance of a focus on comorbidity in detection and treatment of melanoma.
We adjusted the socioeconomic and geographical results for histological type of the cancer, because it was hypothesized that some tumor types occur mostly in groups of people with a certain lifestyle or risk behavior. Lentigo maligna melanoma and superficial spreading melanoma are related to sun exposure, and sun habits could be speculated to change in a direction where more people from lower socioeconomic groups are exposed to sun or especially to use of sunbeds.23 However, it was found that more of the patients with longest education were diagnosed with superficial spreading malignant melanoma, whereas more patients with short education had nodular melanoma – even though the risk profile of nodular melanomas is primarily related to biology rather than behavior. As nodular melanomas are often fast growing and sometimes amelanotic, increased awareness hereof is crucial.28 Tumor type seemed to explain part of the geographical differences in cancer stage, but not when looking at the data solely from 2013 to 2014. We suggest that missing data on tumor histology in the early study period drive the finding since a larger part with unknown/unclassified histology appeared in the North and Central regions (19 and 23%, respectively, for the whole study period vs 8% in the Capital Region, data not shown), which may bias the effect of tumor type.
Strengths of the current study include the population-based data from both a clinical database and administrative registers, which minimize selection bias, information bias and misclassification of both exposure and outcome measures.
Limitations are some missing clinical data for patients diagnosed during the years 2008–2012 (before onset of the DMD as a Clinical Quality register); however, there was an equal distribution of missing/unclassified TNM stage in the groups of patients with lower and higher socioeconomic position. Furthermore, we checked that the main results were similar for the study period as a whole as for the years 2013–2014.
To measure comorbidity, we used the CCI with summarized data of hospital diagnoses and therefore milder diseases not treated or followed up in hospital setting were not included. This may have resulted in some misclassification with the risk of an underestimation of the true effect of comorbidity on outcome.
Another limitation is that we did not have information on contacts with primary practicing doctors, which could have pointed to some explanation of why there is a socioeconomic difference in cancer stage – patient’s delay in health care seeking or doctor’s delay in referral to specialized care. These relations should be further investigated in future studies.
The incidence of melanoma is increasing1 – an increase that has newly been shown across all socioeconomic groups, but with the highest increase of regional-distant disease among patients from the lowest socioeconomic areas in USA,29 and reducing socioeconomic and sex inequalities in stage at diagnosis would result in substantial reductions in deaths from melanoma.19
Results from our study document important socioeconomic and -demographic differences in stage at diagnosis. Initiatives should be directed to social disadvantaged groups, men and older people in order to increase awareness of symptoms of melanoma. In primary care, an increased attention should be paid to patients from these groups in order to discover skin changes or melanoma at an early stage. Additional efforts to improve early diagnosis of nodular melanomas would improve the early vs advanced ratio and thus have the potential to affect mortality significantly. The newly suggested amendment to the diagnostic ABCD rule with EFG for Elevated, Firm and Growing nodule should be applied, and “when in doubt, cut it out” should be taught to both patients and doctors.28 Further studies should investigate regional differences in delay, effects of number of specialized doctors per inhabitant as well as different referral patterns from primary to secondary health care across health care regions.
Acknowledgments
This study was funded by Program for Clinical Research Infrastructure (PROCRIN) established by the Novo Nordisk and Lundbeck Foundations. The authors thank the Danish Clinical Registries and the Danish Melanoma Group for allowing to use data from the clinical database.
Disclosure
The authors report no conflicts of interest in this work.
References
Helvind NM, Hölmich LR, Smith S, et al. Incidence of in situ and invasive melanoma in Denmark from 1985 through 2012: a National Database Study of 24,059 melanoma cases. JAMA Dermatol. 2015;151(10):1087–1095. | ||
ANCR. Cancer Incidence, Mortality, Prevalence and Survival in the Nordic Countries. Association of the Nordic Cancer Registries. Danish Cancer Society; 2016. Available from: http://www.ancr.nu. Accessed December 15, 2017. | ||
Birch-Johansen F, Hvilsom G, Kjaer T, Storm H. Social inequality and incidence of and survival from malignant melanoma in a population-based study in Denmark, 1994–2003. Eur J Cancer. 2008;44(14):2043–2049. | ||
Jiang AJ, Rambhatla PV, Eide MJ. Socioeconomic and lifestyle factors and melanoma: a systematic review. Br J Dermatol. 2015;172(4):885–915. | ||
McNally RJQ, Basta NO, Errington S, James PW, Norman PD, Craft AW. Socioeconomic patterning in the incidence and survival of children and young people diagnosed with malignant melanoma in northern England. J Invest Dermatol. 2014;134(11):2703–2708. | ||
Eriksson H, Lyth J, Månsson-Brahme E, et al. Later stage at diagnosis and worse survival in cutaneous malignant melanoma among men living alone: a nationwide population-based study from Sweden. J Clin Oncol. 2014;32(13):1356–1364. | ||
Eriksson H, Lyth J, Månsson-Brahme E, et al. Low level of education is associated with later stage at diagnosis and reduced survival in cutaneous malignant melanoma: a nationwide population-based study in Sweden. Eur J Cancer. 2013;49(12):2705–2716. | ||
Hölmich LR, Klausen S, Spaun E, et al. The Danish melanoma database. Clin Epidemiol. 2016;8:543–548. eCollection 2016. | ||
Balch CM, Gershenwald JE, Soong SJ, et al. Final version of 2009 AJCC melanoma staging and classification. J Clin Oncol. 2009;27(36):6199–6206. | ||
Balch CM, Soong SJ, Atkins MB, et al. An evidence-based staging system for cutaneous melanoma. CA Cancer J Clin. 2004;54(3):131–149; quiz 182–184. | ||
The Danish Melanoma Database, Annual report 2016. Copenhagen; 2017. Available from: https://www.sundhed.dk/content/cms/30/57130_%C3%A5rsrapport_melanom_2016_endelig_.pdf. Accessed May 15, 2018. | ||
Schmidt M, Schmidt SA, Sandegaard JL, Ehrenstein V, Pedersen L, Sørensen HT. The Danish National Patient Registry: a review of content, data quality, and research potential. Clin Epidemiol. 2015;7:449–490. | ||
Charlson ME, Pompei P, Ales KL, MacKenzie CR. A new method of classifying prognostic comorbidity in longitudinal studies: development and validation. J Chronic Dis. 1987;40(5):373–383. | ||
Baadsgaard M, Quitzau J. Danish registers on personal income and transfer payments. Scand J Public Health. 2011;39(7 Suppl):103–105. | ||
Jensen VM, Rasmussen AW. Danish education registers. Scand J Public Health. 2011;39(7 Suppl):91–94. | ||
Pedersen CB. The Danish civil registration system. Scand J Public Health. 2011;39(7 Suppl):22–25. | ||
Borghi A, Corazza M, Virgili A, et al. Impact of socioeconomic status and district of residence on cutaneous malignant melanoma prognosis: a survival study on incident cases between 1991 and 2011 in the province of Ferrara, northern Italy. Melanoma Res. 2017;27(6):619–624. | ||
Hu S, Sherman R, Arheart K, Kirsner RS. Predictors of neighborhood risk for late-stage melanoma: addressing disparities through spatial analysis and area-based measures. J Invest Dermatol. 2014;134(4):937–945. | ||
Rutherford MJ, Ironmonger L, Ormiston-Smith N, et al. Estimating the potential survival gains by eliminating socioeconomic and sex inequalities in stage at diagnosis of melanoma. Br J Cancer. 2015;112 Suppl 1:S116–S123. | ||
Salvaggio C, Han SW, Martires K, et al. Impact of socioeconomic status and ethnicity on melanoma presentation and recurrence in Caucasian patients. Oncology. 2016;90(2):79–87. | ||
Buja A, Lago L, Lago S, Vinelli A, Zanardo C, Baldo V. Marital status and stage of cancer at diagnosis: a systematic review. Eur J Cancer Care (Engl). 2018;27(1). | ||
Pollitt RA, Swetter SM, Johnson TM, Patil P, Geller AC. Examining the pathways linking lower socioeconomic status and advanced melanoma. Cancer. 2012;118(16):4004–4013. | ||
Idorn LW, Wulf HC. Socioeconomic status and cutaneous malignant melanoma in Northern Europe. Br J Dermatol. 2014;170(4):787–793. | ||
Strömberg U, Peterson S, Holmberg E, et al. Cutaneous malignant melanoma show geographic and socioeconomic disparities in stage at diagnosis and excess mortality. Acta Oncol. 2016;55(8):993–1000. | ||
Sundhed.dk. Available from: https://www.sundhed.dk/borger/guides/find-behandler/. Accessed December 15, 2017. | ||
Rat C, Quereux G, Grimault C, et al. Inclusion of populations at risk of advanced melanoma in an opportunistic targeted screening project involving general practitioners. Scand J Prim Health Care. 2016;34(3):286–294. | ||
Grann AF, Frøslev T, Olesen AB, Schmidt H, Lash TL. The impact of comorbidity and stage on prognosis of Danish melanoma patients, 1987–2009: a registry-based cohort study. Br J Cancer. 2013;109(1):265–271. | ||
Moscarella E, Lallas A, Longo C, et al. Performance of the “if in doubt, cut it out” rule for the management of nodular melanoma. Dermatol Pract Concept. 2017;7(3):1–5. | ||
Clarke CA, McKinley M, Hurley S, et al. Continued increase in melanoma incidence across all socioeconomic status groups in California, 1998–2012. J Invest Dermatol. 2017;137(11):2282–2290. |
 © 2018 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2018 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.