")
Back to Journals » Diabetes, Metabolic Syndrome and Obesity » Volume 14
Influence of Pain on the Quality of Life and Disease Acceptance in Patients with Complicated Diabetic Foot Syndrome
Authors Krzemińska S , Kostka A
Received 17 December 2020
Accepted for publication 17 February 2021
Published 19 March 2021 Volume 2021:14 Pages 1295—1303
DOI https://doi.org/10.2147/DMSO.S297887
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Juei-Tang Cheng
Sylwia Krzemińska, Anna Kostka
Department of Clinical Nursing, Faculty of Health Sciences, Wroclaw Medical University, Wroclaw, Poland
Correspondence: Sylwia Krzemińska
Department of Clinical Nursing, Faculty of Health Sciences, Wroclaw Medical University, Bartla 5, Wroclaw, 51-618, Poland
Email [email protected]
Objective: The aim of the study was to evaluate the relationship between pain and quality of life and illness acceptance, anxiety and depression in a group of patients with complicated diabetic foot syndrome, following lower limb amputation.
Patients and Methods: The studies were carried out in three stages: 7 days, 6 months and 12 months after surgery in a group of 100 patients after amputation of the lower limb due to complications resulting from type 2 diabetes. The study was performed using standardised instruments: WHOQOL-BREF, the Acceptance of Illness Scale (AIS), the Hospital Anxiety and Depression Scale (HADS), and the Visual Analog Scale (VAS) for pain intensity assessment.
Results: Pain occurred in the examined patients throughout the study. The greatest intensity of pain was observed in the postoperative period and significantly weakened over time. Pain intensity was significantly associated with worse overall QoL perceived (− 0.255, p=0.011/-0.283, p=0.005) and QoL scores in the physical and psychological domains at the first and second stage of the study (physical domains − 0.257, p=0.011/-0.219, p=0.03 and psychological − 0.22, p=0.029/-0.24/0.018). The intensity of pain negatively correlates with the acceptance of the disease in all three stages of the study, the greater the severity of pain, the lower the acceptance of illness (− 0.298, p=0.003/-0.326, p=0.001/-0.26, p=0.009). The occurrence of anxiety and depression is highly dependent on the severity of pain, especially at the first and second stage of the study (anxiety 0.203, p=0.045/0.257, p=0.01, depression 0.299, p=0.003/0.253, p=0.012). The stronger the pain, the greater the severity of mood disorders.
Conclusion: Pain and its severity are associated with QoL in the patients with complicated diabetic foot syndrome following lower limb amputation. Disease acceptance was lower in patients experiencing more severe pain at all stages of the study. There is an association of pain with the occurrence of anxiety and depression in amputees, especially 6 months after surgery.
Keywords: diabetes, diabetic foot syndrome, quality of life, amputation, disease acceptance, emotional state
Introduction
Diabetic foot syndrome (DFS) is defined by the International Working Group on the Diabetic Foot (IWGDF) as infection, ulceration, or destruction of tissues of the foot in a person with currently or previously diagnosed diabetes mellitus, usually accompanied by neuropathy and/or PAD in the lower extremity.1 Clinically, diabetic foot syndrome is categorised by its predominant pathogenetic factors: neuropathic, ischemic and neuroischemic (mixed).2 Although most patients with diabetic peripheral neuropathy experience no pain, approximately 11% of patients have chronic, painful symptoms which decrease their quality of life, disrupt sleep, and can lead to depression.3,4
Painful diabetic neuropathy can significantly impair patients’ quality of life3 and affect many areas of everyday life.5–7
The number of amputations is growing due to the increasing incidence of diabetes and vascular disease, as well as due to population aging.
In the years 2014–2018, the number of amputations performed in diabetic patients increased by approx. 22.5%. In 2018, 8900 major amputations in Poland were performed on diabetic patients. According to the same report, the percentage of amputations in diabetic patients out of all amputations performed (excluding those due to cancer, trauma, and external factors) increased to 60.1%. This constitutes more than half of all amputations performed in 2018 for reasons other than those listed above.8,9
Diabetes is a major contributor to critical lower limb ischemia, increasing its risk fourfold. The symptoms are additionally exacerbated by smoking, hyperlipidemia, and age exceeding 65 years. Diabetic foot syndrome (DFS), which develops due to peripheral nerve damage, is undoubtedly one of the main diabetes complications leading to amputations. Peripheral neuropathy results in sensation impairment or loss, which in turn leads to the development of non-healing ulcers. Over two-thirds of all non-traumatic lower extremity amputations are performed in diabetic patients.10–13 The objective of amputation is to remove all necrotic tissue, but also to shape an amputation stump that can subsequently be fitted with a prosthesis.14 Proper preparation, holistic care for the patient, and rehabilitation contribute to faster and more complete recovery after the procedure.15
Quality of life (QoL) is assessed individually by each patient. Multiple determinants affect the QoL of patients with a specific condition. Diabetic patients experience complex issues, and those after lower extremity amputation due to diabetes complications are an even narrower, distinct group of patients requiring specialised care. Lower extremity amputation is undoubtedly associated with QoL deterioration, which results from a number of new limitations, changes in the patient’s personal and professional life, and changes in appearance. Among the factors affecting QoL, pain is one of the most significant.16,17
Objective
The aim of the study was to evaluate the relationship between pain and quality of life, acceptance of illness, anxiety and depression in a group of patients with complicated diabetic foot syndrome, following lower limb amputation.
Hypothesis
The assumption was that the presence of pain in the study group may have a negative impact on the quality of life of diabetic patients as well as on the acceptance of the disease and their emotional state.
Patients and Methods
Design and Settings
The observational and correlational study was performed in a group of 117 patients from the Vascular Surgery and Angiology Department of the Regional Specialist Hospital in Wrocław, Poland, and the Surgical Department of the Strzelin Medical Center. The STROBE guidelines (Strengthening the Reporting of Observational Studies in Epidemiology) were followed. The study comprised 3 stages performed over the period of one year. The first stage took place between October 2016 and May 2017, the second stage - six months after surgery, and the third one - 12 months after surgery.
Study Participants
Initially, 117 patients were recruited but those who could not continue their participation at later stages (dropped out/died) were excluded. The group that completed the study consisted of 100 patients.
Eligibility Criteria
Participants included in the study met the following criteria for inclusion: (1) complicated diabetic foot syndrome requiring an amputation, (2) over 60 years of age, (3) duration of diabetes of over 10 year, (4) lack of cognitive disorders, (5) ability to complete questionnaires on one’s own, and (6) patient’s consent to take part in the study.
The first stage of the study took place in the hospital, on the 7th postoperative day. Two subsequent stages took place during follow-up appointments, 6 and 12 months after amputation. Respondents completed the questionnaires themselves.
Research Tools
The study was performed using standardised instruments: the short-form World Health Organization QoL questionnaire (WHOQOL-BREF), the Acceptance of Illness Scale (AIS), the Hospital Anxiety and Depression Scale (HADS), and the Visual Analog Scale (VAS- 10 cm) for the assessment of pain intensity. Patients’ socio-demographic and clinical data were obtained from their medical records. Only those confirmed by a specialist were considered comorbidities.
The subjective assessment of the presence of phantom pain sensations was based on the answers to the following questions: “Do you feel the amputated part of your limb”? And “Do you feel pain in the amputated part of your limb?”. If the patient answered yes to 2 questions, they were included in the group with phantom pains. Also a question related to the assessment of the incidence of pain in the postoperative wound and/or the residual limb was asked. Pain intensity measurements were taken at baseline for all patients 7 days, 6 months and 12 months after surgery using a 10 cm VAS,17,18,19 where 0 indicates no pain and 10 corresponds to the worst pain imaginable - the measurement was always performed by the researcher or a person trained by him.
The WHOQOL-BREF questionnaire enables the evaluation of QoL in six dimensions. The first two subscales (overall QoL and health perceived) are scored between 1 and 5 points, and the remaining ones (physical, psychological, social, and environmental QoL domains) are scored between 4 and 20 points. Higher scores indicate better QoL.20,21
The Acceptance of Illness Scale (AIS) comprises eight statements. For each, the patients rate their agreement or disagreement. Scores range from 8 to 40 points, and higher scores indicate higher acceptance of illness. Based on the total score, the acceptance level is interpreted as follows: 8–18 points — no acceptance, 19–29 points — moderate acceptance, and 30–40 points — a good level of acceptance. The AIS was developed by B. J. Felton, T. A. Revenson, and G. A. Hinrichsen. Its Polish adaptation was created by Z. Juczyński.22
The HADS questionnaire was used to assess anxiety and depression symptoms. It consists of 14 items, seven of which refer to symptoms of anxiety and emotional tension, and the other seven - strictly to depressive symptoms. The Hospital Anxiety and Depression Scale (HADS) was developed for non-psychiatric patients aged 16 to 65.23 It measures anxiety and depression as a state, not a trait.24 The elimination of items referring to somatic complaints has made HADS one of the most commonly used screening tests in medical settings. Due to its high sensitivity and specificity towards the major generalised anxiety and depressive disorders,25 the HADS has also been introduced in diagnostics for healthy adults.
Ethical Considerations
The study was approved by the Bioethics Committee of the Wroclaw Medical University (approval no. KB–554/2016). All patients provided informed consent and were informed that they could withdraw from the study at any time. The study was carried out in accordance with the tenets of the Declaration of Helsinki and Good Clinical Practice guidelines.
Data Analysis
Quantitative variables (expressed with a number) were analysed using means, standard deviations, and median, quartile, minimum and maximum values. Quantitative variables not expressed with a number were analysed using the counts and percentages of each value. Comparisons of quantitative variable values between two groups were performed using Student’s t-test (for normal distributions of a variable in the groups analysed) or the Mann–Whitney test (otherwise). Comparisons of quantitative variable values in three or more groups were performed using ANOVA (for normal distributions of a variable in the groups analysed) or the Kruskal–Wallis test (otherwise). If statistically significant differences were found, post hoc analysis was carried out using the Fisher’s LSD test (for normal distributions) or the Dunn test (for distributions other than normal) to identify groups that were significantly different.
Correlations between quantitative variables were analysed using Pearson’s correlation coefficient (if the distributions for both variables were normal) or Spearman correlation coefficient (otherwise). Correlation strength was interpreted as follows: |r| ≥ 0.9 – very strong correlation, 0.7 ≤ |r| < 0.9 – strong correlation, 0.5 ≤ |r| < 0.7 – moderate correlation, 0.3 ≤ |r| < 0.5 – weak correlation, |r| < 0.3 – very weak (negligible) correlation.26
Comparisons of quantitative variable values between two repeated measurements were performed using Student’s t-test for paired data (for normal distributions of a variable in the measurements analysed) or the Wilcoxon test for paired data (otherwise).
Comparisons of quantitative variable values in three or more repeated measurements were performed using repeated measures ANOVA (for normal distributions of a variable in the groups analysed) or the Friedman test (otherwise). In case of statistically significant differences, post hoc analysis was performed using Student’s t-tests for paired data (for normal distributions) or the Wilcoxon test for paired data (otherwise) to identify groups that were significantly different. In both cases, the Bonferroni correction was used.
Variable distribution normality was verified using the Shapiro–Wilk test.
A significance level of 0.05 was used in the analysis. Thus all p values of less than 0.05 were interpreted as indicating a strong correlation. In order to assess how well the model fits the data, we used the R-squared determination coefficient. This measure is the proportion of the variance in the dependent variable that is explained by the model. The analysis was carried out using the R software, version 3.6.0.27
Sociodemographic and Clinical Analysis
The characteristics of the patients included in the study are shown in Table 1. The data were collected during stage one of the study.
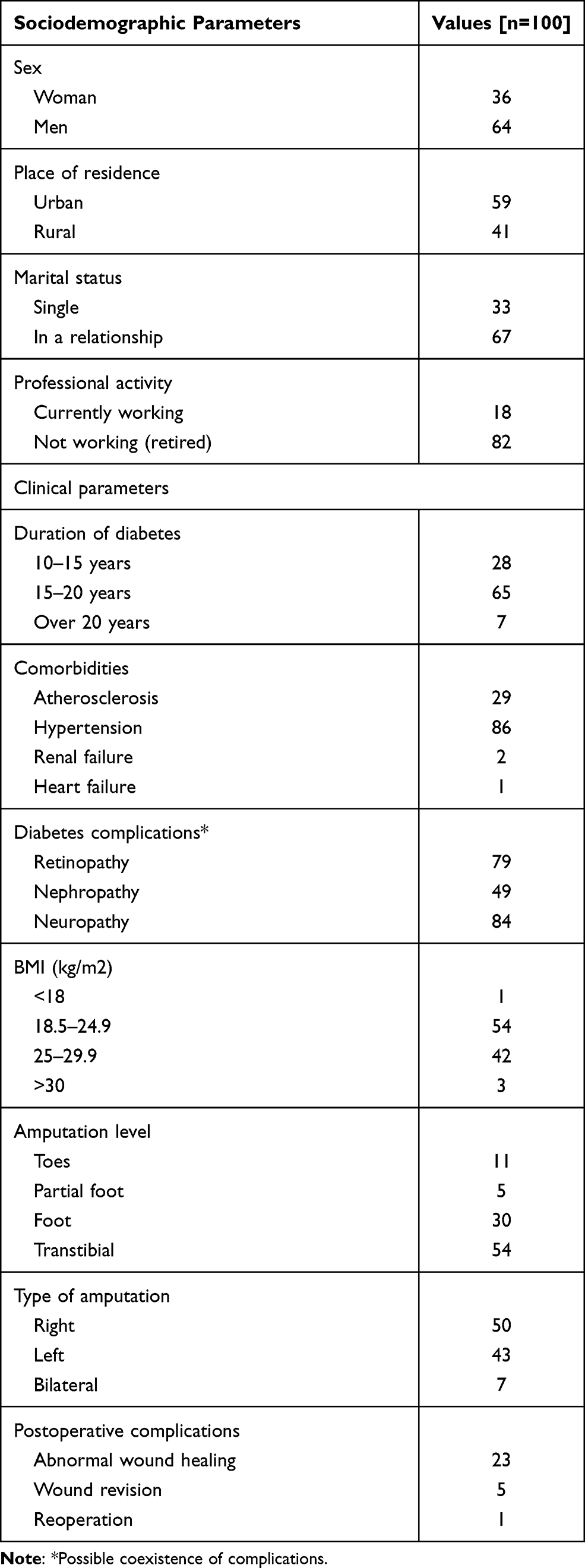 |
Table 1 Sociodemographic and Clinical Characteristics of the Studies Patients |
Occurrence of Postoperative Pain and Residual Limb Pain
At the first stage of the study, 82% of the respondents experienced pain in the wound and/or the residual limb of the limb every day, and 16% of the respondents experienced unceasing pain around the clock. At the second stage of the study, the frequency of pain symptoms changed significantly after six months compared to the state recorded immediately after surgery. Most of the patients reported pain several times a week or several times a month. At the third stage of the study, the respondents declared pain several times a month or no pain at all.
Subjectively perceived phantom pain at the first and second stage of the study were declared by 98% of the respondents, and at the third stage of the study by 96% of the respondents.
Pain Intensity Assessment
Pain intensity of the postoperative wound and the limb stump was assessed on the 7th postoperative day. The mean pain intensity score during stage one of the study was 5.14 points (SD=1.24) on a scale of 0–10, and the scores ranged between 0 and 9 points. The median score was 5 points, and the 1st and 3rd quartiles were 4 and 6 points, respectively. Two patients did not provide a pain score despite having reported pain (Table 2).
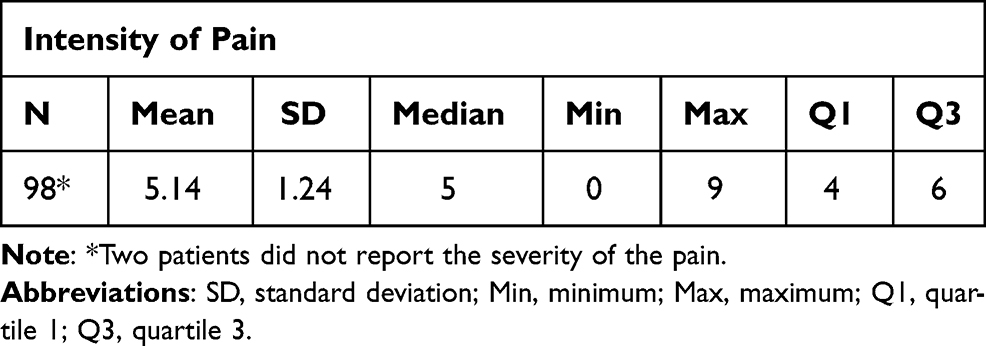 |
Table 2 The Intensity of Pain According to the VAS Scale at the First Stage of the Study |
Pain intensity did not have a normal distribution in the measurements analysed, so the Friedman test was used in the analysis.
P was below 0.05 indicating that pain intensity differed significantly between the measurements. Post-hoc analysis demonstrated that it decreased significantly with each subsequent measurement.
Association Between Pain Intensity and QoL
The WHOQoL BREF scores did not have a normal distribution. At the first stage of the study, pain intensity was significantly associated with worse overall perceived QoL and QoL scores in the physical and psychological domains (p<0.05). The correlations were negative: the stronger the pain, the lower the QoL in these domains (Table 3). At the second stage - after 6 months of observation, the intensity of pain was significantly related to the overall perceived quality of life and health, as well as to the QoL results in the physical and psychological spheres (p <0.05). The correlations were negative: the stronger the pain, the lower the QoL in the above-mentioned domains (Table 3). At the third stage, after 12 months of observation, pain intensity was significantly related only to QoL in the environmental domain (p <0.05). The correlation was negative: the stronger the pain, the lower the QoL in this domain (Table 4).
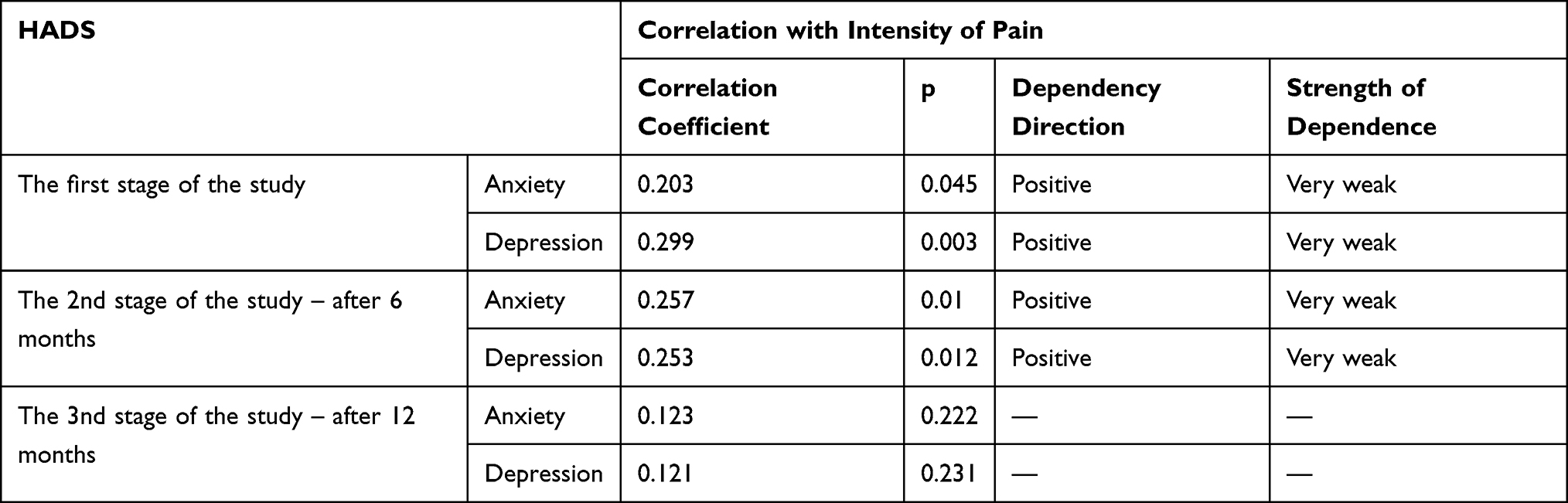 |
Table 3 Correlation Between Pain Intensity and Anxiety/Depression (HADS) |
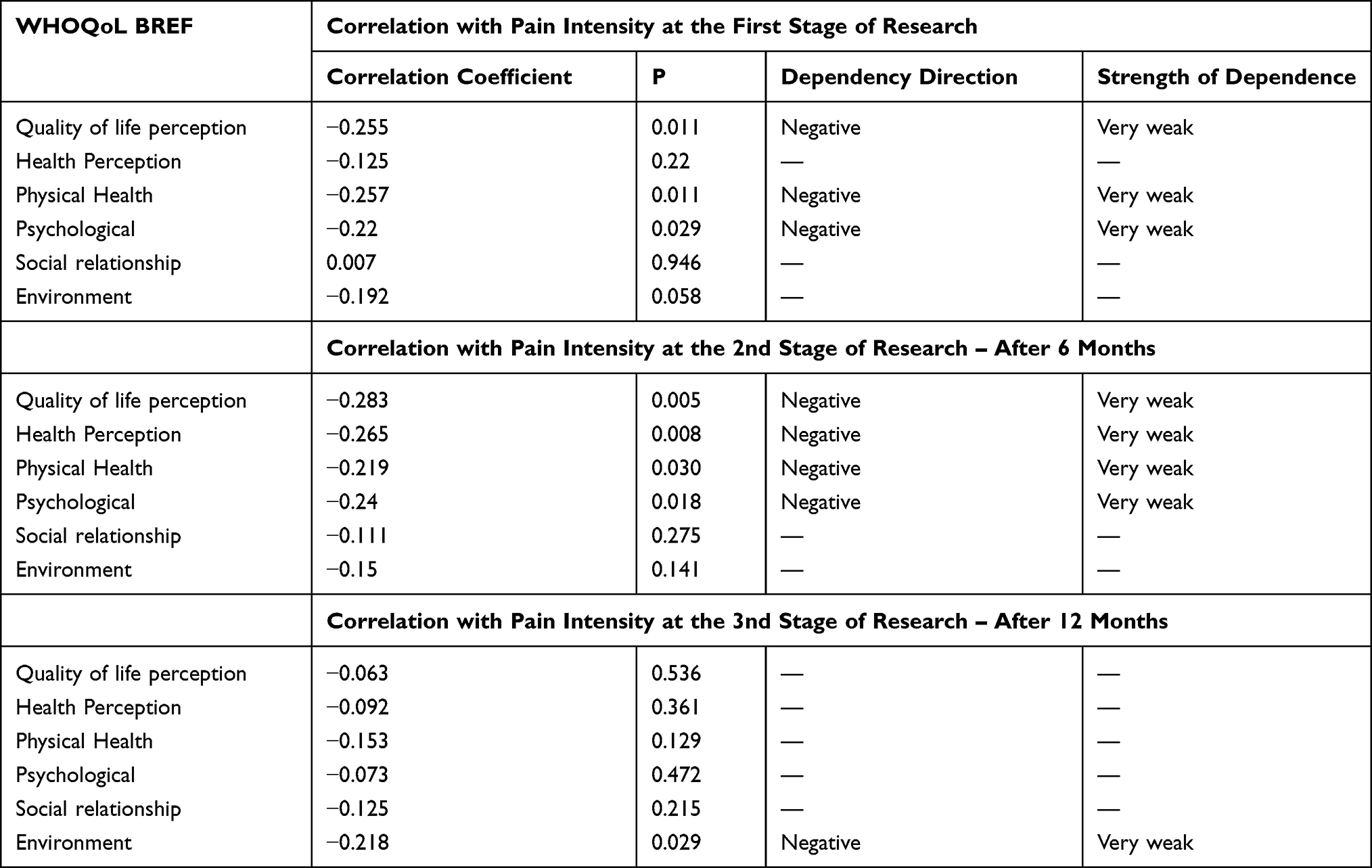 |
Table 4 Correlation Between Quality of Life (WHOQoL BREF) and Intensity of Pain at Individual Stages of the Study |
Association Between Pain Intensity and Illness Acceptance
The correlation coefficients for pain intensity and illness acceptance were statistically significant at all three stages (p<0.05), ie both characteristics were significantly associated (Table 5). The correlation was negative: the stronger the pain, the lower the acceptance level.
 |
Table 5 Correlation Between Illness Acceptance (AIS) and Intensity of Pain at Individual Stages of the Study |
Association Between Pain Intensity and Anxiety/Depression
At the first and second stages, the pain was significantly intensified and related to the severity of anxiety and depression symptoms (p <0.05). The correlations were positive: the stronger the pain, the more severe the affective disorders (Table 3). At the third stage of the study, correlation coefficients were not statistically significant (p>0.05), ie the severity of anxiety and depression symptoms was not significantly associated with pain (Table 3).
Discussion
Studies on the prevalence and effect of pain on the quality of life in diabetic foot syndrome (DFS) patients showed results that most often refer to patients with neuropathic pain16 and/or coexisting foot ulceration,17 however, there are no studies on the influence of pain on the quality of life in patients with diabetes and post-amputation diabetic foot syndrome.
As shown in the present study, pain is one of the statistically significant determinants of QoL of patients with diabetic foot syndrome after lower limb amputation. Both shortly after the procedure and at 6-month follow-up, pain intensity significantly affected patients’ overall perceived QoL and health, as well as their QoL in the physical and social domains. One year after the procedure, QoL in the environmental domain was most affected by pain. With each measurement, less pain was reported, however, an association between greater pain intensity and lower QoL of the amputees was still found at all stages of the study. Subjectively perceived phantom pain was reported by the majority of respondents, and persisted throughout the year after the procedure. Van der Shans et al compared QoL between amputees with and without phantom pain. In their study, patients with persistent phantom pain had significantly lower QoL than those without such complaints.18 The authors also reported a negative impact of stump pain on QoL, which may be even more significant than phantom pain.18 In turn, Neil et al report that up to 80% of amputees complain of phantom pain. According to the authors, pain subsides completely within a year in many patients, but in some of them, it persists for the rest of their lives.28 Morgan et al also studied phantom pain and bodily pain experienced by lower-extremity amputees. In their study, three quarters of the patients reported a variety of complaints despite the long time (several years) that had passed since the amputation. Patients in that group reported moderately severe pain and stated that their pain significantly interfered with their daily activities.29 Bosmans et al observed the highest intensity of phantom pain six months after the amputation, which then subsided over time. Overall, phantom pain occurred more often in female patients.30 Holzer et al described a major impact of phantom pain on perceived QoL. In their study, phantom pain significantly affected patients’ perceived health, emotional problems, acceptance, and self-esteem,31 which is consistent with the present findings. A statistically significant impact of phantom pain on QoL deterioration was also reported by Suckow et al32 and Zidarov et al.33 Moreover, QoL can also be affected by complaints related to the contralateral limb which is subject to overload and disease progression.31
Pain combined with increased anxiety considerably reduced amputees’ QoL.34 Pain undoubtedly affects the overall functioning of an individual. Nonetheless, Whyte et al report that amputees are also adversely affected by social dysfunction, insomnia, or anxiety, in addition to somatic complaints.35 In our study, anxiety and depression were closely associated with pain intensity, as was illness acceptance. The correlations were positive, ie more pain was associated with more severe affective disorders. The associations were particularly strong at stage one and two of the study. At 12-month follow-up, pain no longer had a significant impact on anxiety or depression. Muraczyńska et al also found a significant correlation between pain and emotional problems in amputees.36 In the study by Bhutani et al, there was also a positive correlation between pain and both anxiety and depression.37
De Rooij et al studied patients diagnosed with chronic pain to establish its impact on their psychological and emotional condition.38 A strict correlation was found between pain and patients’ emotional condition and self-esteem. Lower pain severity was associated with cessation or alleviation of depressive symptoms at 6- and 18-month follow-up. In addition to less severe pain, factors that alleviated depressive symptoms included coping with pain, treatment control, personal control, and greater belief in one’s self-efficacy.38
Kazemi et al also studied the influence of phantom pain and chronic stump pain on anxiety and depression in lower-extremity amputees. In their group, pathological anxiety was found more often in patients with no phantom pain. Depression symptoms were also more common in patients with chronic stump pain than in those with phantom pain.39 Therefore, it can be concluded that both phantom pain and chronic stump pain may have an adverse effect on the mood of people after lower limb amputation and predispose them to anxiety and depression.
Strengths of the Research
The study had a very good retention rate. Nearly all the subjects included in the group at the first stage were also examined during the third stage.
Weaknesses of the Research
The intensity aspect of phantom pain has not been definitively investigated, focusing on the occurrence of pain in the surgical wound and/or the residual limb. Moreover, the types of amputation considered may produce false results. Patients may perceive pain related to a toe amputation and not experience pain related to a femoral amputation. In addition, pain that occurs in patients with diabetes may have a different origin (eg neuropathic), so it seems necessary to conduct research on a larger group of patients by gender, and to pay attention to additional aspects, both sociodemographic and clinical. Furthermore, the research method applied here did not allow the causal relationship between the factors to be examined, but only made it possible to put forward a statement that such a relationship exists.
Conclusions
Pain and its intensity are associated with QoL in patients with complicated diabetic foot syndrome. More severe pain was associated with lower QoL in the physical and psychological domains six months after amputation, and with lower QoL in the environmental domain 12 months after amputation. Illness acceptance was lower in patients with more severe pain at all stages of the study. Pain affects the incidence of anxiety and depression in amputees: greater pain intensity was associated with more severe affective disorders at 6-month follow-up.
Indications for Patients Care
Healthcare professionals should recognise and evaluate pain in patients after amputations, and include pain rating as a factor in the assessment of QoL.
Based on the study, we see a need to pay attention to amputee patients in the field of Primary Healthcare and community and family nursing, as well as specialist care. Patients who have undergone amputations should be included in a holistic nursing and educational programme, the task of which is not only to care for the physical sphere (assessment of the somatic state) but also to assess their mental state at specific time intervals, eg 3, 6, 9 and 12, 18, 24 months after surgery. Such an approach could facilitate swift diagnosis of a patient’s physical and mental problems and select the appropriate care and therapy for them.
Acknowledgment
The research was financed from the funds of the Medical University of Wroclaw: SUB.E020.21.002.
Disclosure
The authors report no conflicts of interest for this work.
References
1. Van Netten JJ, Bus SA, Apelqvist J, et al. Definitions and criteria for diabetic foot disease. Diabetes Metab Res Rev. 2020;36(S1):e3268. doi:10.1002/dmrr.3268
2. Volmer-Thole M, LobmannInt R. Neuropathy and diabetic foot syndrome. J Mol Sci. 2016;17:917. doi:10.3390/ijms17060917
3. Navarro-Flores E, Gijón-Noguerón G, Cervera-Marín JA, Labajos-Manzanares MT. Assessment of foot self-care in patients with diabetes: retrospective assessment (2008–2014). Foot Ankle Spec. 2015;8(5):406–412. doi:10.1177/1938640015585963
4. Argoff CE, Cole BE, Fishbain DA, Irving GA. Diabetic peripheral neuropathic pain: clinical and quality-of-life issues. Mayo Clin Proc. 2006;81(4):S3–11. doi:10.1016/s0025-6196(11)61474-2
5. Bouhassira D, Letanoux M, Hartemann A. Chronic pain with neuropathic characteristics in diabetic patients: a French cross-sectional study. PLoS One. 2013;8(9):e74195. doi:10.1371/journal.pone.0074195
6. Navarro-Flores E, Cauli O. Quality of life in individuals with diabetic foot syndrome. Endocr Metabol Immune Disord. 2020;20:1365–1372. doi:10.2174/1871530320666200128154036
7. Huizinga MM, Peltier A. Painful diabetic neuropathy: a management-centered review. Clin Diabetes. 2007;25(1):6–15. doi:10.2337/diaclin.25.1.6
8. Headquarters of the National Health Fund. NFZ o zdrowiu; Cukrzyva [NFZ about health; Diabetes]. Warsaw; 2019 Available from: https://zdrowedane.nfz.gov.pl/pluginfile.php/205/mod_resource/content/4/nfz_o_zdrowiu_cukrzyca.pdf.
9. Headquarters of the National Health Fund. Cukier, otyłość – konsekwencje Przegląd literatury, szacunki dla Polski [Sugar, obesity - consequences. Literature review, estimates for Poland]. Warsaw; 2019. Available from: https://zdrowedane.nfz.gov.pl/pluginfile.php/63/mod_resource/content/4/cukier.pdf.
10. Insull W. The pathology of atherosclerosis: plaque development and plaque responses to medical treatment. Am J Med. 2009;122(1):3–14. doi:10.1016/j.amjmed.2008.10.013
11. Weledji EP, Fokam P. Treatment of the diabetic foot – to amputate or not? BMC Surg. 2014;14:83. doi:10.1186/1471-2482-14-83
12. Mrozikiewicz-Rakowska B, Krasnodębski P, Karliński M, et al. Risk factors for lower limb amputation in diabetic foot syndrome. Leczenie Ran. 2011;8(1):1–54.
13. Karłowicz A, Korzon-Burakowska A, Skuratowicz-Kubica A, Kunicka K, Świerblewska E, Burakowski I. Level of knowledge about diabetic foot syndrome in patients with type 2 diabetes. Diabetologia Praktyczna. 2010;11(4):107–119.
14. Badora A, Będkowska P, Budziński G. Primary and secondary amputations of the lower limbs in the material of one center. Ann Acad Med Silesiensis. 2012;66(2):7–12.
15. Dillingham TR, Pezzin LE. Rehabilitation setting and associated mortality and medical stability among persons with amputations. Arch Phys Med Rehabil. 2008;89(6):1038–1045. doi:10.1016/j.apmr.2007.11.034
16. Dermanovic Dobrota V, Hrabac P, Skegro D, et al. The impact of neuropathic pain and other comorbidities on the quality of life in patients with diabetes. Health Qual Life Outcomes. 2014;12:171. doi:10.1186/s12955-014-0171-7
17. Alosaimi FD, Labani R, Almasoud N, et al. Associations of foot ulceration with quality of life and psychosocial determinants among patients with diabetes; a case-control study. J Foot Ankle Res. 2019;12:57. doi:10.1186/s13047-019-0367-5
18. Van der Schans CP, Geertzen JHB, Schoppen T, Dijkstra PU. Phantom pain and health-related quality of life in lower limb amputees. J Pain Symptom Manage. 2002;24(4):429–436. doi:10.1016/S0885-3924(02)00511-0
19. Misiołek H, Mayzner-Zawadzka E, Dobrogowski J, Wordliczek J. 2011 recommendations for the management of acute and postoperative pain. Ból. 2011;12(2).
20. Kostka A, Chabowski M, Janczak D. Analysis of selected research tools used in assessing the quality of life of patients after amputation of the lower limbs. Acta Bio Optica Et Informatica Medica Inzynieria Biomedyczna. 2017;23(2):113–118.
21. Gnacińska-Szymańska M, Dardzińska JA, Majkowicz M, Małgorzewicz S. Assessment of the quality of life of people with excessive body weight using the WHOQOL-BREF.. Endokrynologia Otylosc I Zaburzenia Przemiany Materii. 2012;8(4):136–142.
22. Juczyński Z. Measurement Tools in the Promotion of Health. Warszawa, Poland: The Psychological Tests Lab of the Polish Psychological Association; 2001:171–174.
23. Zigmond AS, Snaith RP. The hospital anxiety and depression scale. Acta Psychiatr Scand. 1983;67:361–370. doi:10.1111/j.1600-0447.1983.tb09716.x
24. Herrmann C. International experiences with the Hospital Anxiety and Depression Scale – a review of validation data and clinical results. J Psychosom Res. 1997;42:17–41. doi:10.1016/S0022-3999(96)00216-4
25. Mitchell AJ, Meader N, Symonds P. Diagnostic validity of the Hospital Anxiety and Depression Scale (HADS) in cancer and palliative settings: a meta-analysis. J Affect Disord. 2010;126:335–348. doi:10.1016/j.jad.2010.01.067
26. Hinkle DE, Wiersma W, Jurs SG. Applied Statistics for the Behavioral Sciences.
27. R Core Team. R: a language and environment for statistical computing; 2017. R Foundation for Statistical Computing, Vienna, Austria. Available from: https://www.R-project.org/.
28. Neil MJE. Pain after amputation. BJA Educ. 2016;16(3):107–112. doi:10.1093/bjaed/mkv028
29. Morgan SJ, Friedly JL, Amtmann D, Salem R, Hafner BJ. Cross-sectional assessment of factors related to pain intensity and pain interference in lower limb prosthesis users. Arch Phys Med Rehabil. 2017;98(1):105–113. doi:10.1016/j.apmr.2016.09.118
30. Bosmans JC, Geertzen JH, Post WJ, van der Schans CP, Dijkstra PU. Factors associated with phantom limb pain: a 31/2-year prospective study. Clin Rehabil. 2010;24(5):444–453. doi:10.1177/0269215509360645
31. Holzer LA, Sevelda F, Fraberger G, et al. Body image and self-esteem in lower-limb amputees: journal list. PLoS One. 2014;9(3).
32. Suckow BD, Goodney PP, Nolan BW, et al. Domains that determine quality of life in vascular amputees. Ann Vasc Surg. 2015;29(4):722–730. doi:10.1016/j.avsg.2014.12.005
33. Zidarov D, Swaine B, Gauthier-Gagnon C. Quality of life of persons with lower-limb amputation during rehabilitation and at 3-month follow-up. Arch Phys Med Rehabil. 2009;90(4):634–645. doi:10.1016/j.apmr.2008.11.003
34. Padovani MT, Martins MR, Venâncio A, Forni JE. Anxiety, depression and quality of life in individuals with phantom limb pain. Acta Ortop Bras. 2015;23(2):107–110. doi:10.1590/1413-78522015230200990
35. Whyte AS, Niven CA. Psychological distress in amputees with phantom limb pain. J Pain Symptom Manage. 2001;22(5):938–946. doi:10.1016/S0885-3924(01)00352-9
36. Muraczyńska B, Cieslak T. Functional and social activity of patients after deduction of limb as measures of quality of life. Ann Univ Mariae Curie Sklodowska Med. 2003;58(13):338–343.
37. Bhutani S, Bhutani J, Chhabra A, Uppal R. Living with amputation: anxiety and depression correlates. J Clin Diagn Res. 2016;10(9):RC09–RC12. doi:10.7860/JCDR/2016/20316.8417
38. Rooij A, de Boer MR, van der Leeden M, Roorda LD, Steultjens MPM, Dekker J. Cognitive mechanisms of change in multidisciplinary treatment of patients with chronic wide spread pain: a prospective cohort study.. J Rehabil Med. 2014;46:173–180. doi:10.2340/16501977-1252
39. Kazemi H, Ghassemi S, Fereshtehnejad SM, Amini A, Kolivand PH, Doroudi T. Anxiety and depression in patients with amputated limbs suffering from phantom pain: a comparative study with non-phantom chronic pain.. Int J Prev Med. 2013;4(2):218–225.
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.