")
Back to Journals » HIV/AIDS - Research and Palliative Care » Volume 13
Influence of Lost to Follow Up from Antiretroviral Therapy Among Retroviral Infected Patients at Tuberculosis Centers in Public Hospitals of Benishangul-Gumuz, Ethiopia
Authors Degavi G
Received 12 February 2021
Accepted for publication 10 March 2021
Published 22 March 2021 Volume 2021:13 Pages 315—327
DOI https://doi.org/10.2147/HIV.S306257
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Bassel Sawaya
Girish Degavi
BuleHoraUniversity’s Department of Nursing, College of Health and Medical Science, Bulehora, Hageremaryam, Ethiopia
Correspondence: Girish Degavi
BuleHora University’s Department of Nursing, College of Health and Medical Science, Bulehora, Hageremaryam, Ethiopia
Tel +251-966686212
Email [email protected]
Background: Broadening access to healthcare (ART) antiretroviral therapy has led to a 19% reduction in the death rate of people infected with the human immunodeficiency virus. This study would also describe the status and deciding factors of ART in (TB) tuberculosis centers in public hospitals of Benishangul-Gumuz, Ethiopia, for (LTFU) lost follow-up among (RVI) retroviral infected patients.
Methods: Hospital-based, unrivalled analysis of the case management (3:1) design was conducted. A total of 752 study participants (563 controls and 189 cases) Picked by systematic random sampling methodology, and where reviewed their charts from TB Centers. Data were entered and cleaned using Epi data version 3.1.1 and then exported to SPSS version 22 for analysis. To analyze the statistical relationship between the outcome variable and independent variables, binary logistic regression was used. Relevance was declared at a p-value < 0.05.
Results: A total of 1122 (25.3%) were LTFU. Among index cases with male cases, there were higher odds of lost to follow up (AOR= 1.68, 95% CI; 1.085, 2.609), 15– 24 old age group have no formal education, civil servant were also having high comparatively. In index cases with identified parents, the risk of LTFU up had lower HIV status (AOR=0.5; 95% CI; 0.24, 0.997). Rest all variables showed low odds to LTFU.
Conclusion: A large number of patients enrolled in ARTwere missing from follow-up at TB centers, but unfortunately did not make the next appointment reported. The absence of prophylaxis was accepted as an independent determinant of LTFUfor ART.
Keywords: HIV/AIDS, RVI patients, LTFU, antiretroviral therapy, Benishangul-Gumuz
Introduction
The global HIV epidemic continues to pose the most severe public health risk to infectious diseases and remains a significant threat to socio-economic growth. AIDS is a leading cause of death and resulted in the deaths of 25 million people. 5700 people die from AIDS worldwide every day.1 In 2010, 34 million people were living with HIV (PLWHIV) worldwide, but WHO evidence actually shows that more than 70 million people worldwide were infected with HIV/AIDS by the end of 2017, of which about 35 million died of HIV/AIDS and associated complications, showing how the epidemic has risen in this period of time.2 Sub-Saharan African countries are reportedly home to more than 3.5 million people infected with the virus, making it the most afflicted part of the world, one of the countries in this region of Africa is Ethiopia.3–5
When we see statistics from FHAPCO (Federal HIV AIDS Prevention and Control Office) in Ethiopia, it reveals that there are over 718,550 persons living with HIV, 1.3% of the incidence of national adult HIV. The antiretroviral therapy program was initiated to monitor HIV-related complications and deaths among PLWHIV countries. Over the past 10 years, the widening of access to antiretroviral therapy has resulted in a groundbreaking public health milestone in antiretroviral therapy coverage for more than 17 million people living with HIV (PLWH) in 2015. In-between 2004 to 2009 expanded access to care rendered through antiretroviral therapy led to a 19% reduction in deaths for people living with human immunodeficiency virus (HIV).6–9 Antiretroviral therapy is considered to decrease mortality from causes associated with acquired immunodeficiency syndrome. The lack of patient follow-up lost to follow up of this therapy produces a significant public and health care issue, raises the risk of medication tolerance and treatment relapse, and reduces the immunological value of antiretroviral therapy and increases the morbidity, mortality and hospitalization associated with AIDS.10,11
To initiate lifesaving antiretroviral therapy and encourage the distribution of vital preventive messages to minimize HIV transmission, keeping HIV infected patients in medical care following diagnosis is necessary. In the future, new HIV infections are mostly expected to arrive from individuals living with the virus, recognizing their serostatus and not enrolled in medical programs or absent from the program. Maintaining these clients in care has a potential effect not just on reducing mortality associated with AIDS, but also on avoiding new infections.9
Methods
Study Setting
The research was performed at two Benishangul Gumuz Area hospitals. It is situated in the western part of Ethiopia in latitude. Based on the latest census, the total population is around 6.5 million. More than 80% of the population are residing in rural area. The population density of the region is considered to be 10 people/km2 and the average development rate is just below 5%. (Figure 1)12
 |
Figure 1 Map of Benishangul Gumuz Area in the western part of Ethiopia. The present study is conducted at two Benishangul Gumuz Area hospitals. It is located in the western part of Ethiopia between 34 ° 10 ‘N and 37 ° 40ʹ E; and 09 ° 17 ‘N & 12 ° 06ʹ N. In latitude. Based on the 2007 census, the total population of the district is 670,847. About 85.4% of the national population is rural, while the remaining 14.6% is metropolitan. Adapted from Benishangul-Gumuz Region [Internet]. Benishangul-Gumuz Region; 2021. Available from: https://en.wikipedia.org/wiki/Benishangul- Gumuz_Region. Accessed Jan 13, 2021.12 |
Source Population
Cases
In Tuberculosis center in public Hospital of Benishangul-Gumuz, Ethiopia, all RVI patients who enrolled but lost from antiretroviral therapy January 1, 2016 to December 31, 2018.
Controls
Almost all RVI patients who enrolled and visited antiretroviral therapy at Tuberculosis centers in public Hospitals of Benishangul-Gumuz, Ethiopia, from January 1, 2017 to December 31, 2018.
Study Population and Unites
Population
Randomly picked antiretroviral therapy enrolled patients who had missed >3 months of follow-up.
Randomly chosen antiretroviral therapy enrolled patients who have daily follow-up and did not fail for 3 months.
Unites
Randomly picked HIV-positive patients from each of the selected hospitals who have missed more than or equivalent to three months of follow-up.
HIV-positive randomly chosen patients from each selected hospital who have routine follow-up and have not been missing for three months.
Inclusion Criteria
Cases
Antiretroviral therapy enrolled patients >15 years of age who missed >3 months of follow-up after antiretroviral therapy from January 1, 2016 to December 31, 2018.
Controls
Antiretroviral therapy enrolled patients >15 years of age and had been in recovery for >3 months January 1, 2016 to December 31, 2018.
Exclusion Criteria
Controls
Missed >3 months and returned to antiretroviral therapy.
Incomplete cards would be omitted for all cases and controls.
Determination of Sample Size
With the following assumptions for an unmatched case-control research design, the sample size was determined using Epi info version 7.2 (Fleiss w/cc): 95% confidence interval (CI), 80% capacity, 18.2% exposure share in the control community, 1:3 case-to-control ratio, and 2.3 odds ratio from previous study for <200 cells/mL CD4 count.4 258 controls and 86 cases were obtained from the Epi details version 7.2 (Fleiss w/cc), multiplied by 2 for design effect, it was 684, assuming that 10% nonresponse rate 757 (568 controls and 189 cases) was finally included. Around 4231 PLHIV were enrolled in antiretroviral therapy treatment during the time of the HIV clinic, according to data from the Hospitals HIV clinic from January 1, 2017 to December 31, 2018, 36 months of data to be analyzed. Cases and controls were separately listed after defining the list of all eligible study participants, and systematic random sampling techniques were used to select sample cases and controls.
Sampling Technique and Procedure
The study was conducted in two hospitals of Benishangul Gumuz Region. The two hospitals, namely, Asossa Hospital, which is located in Asossa zone and Pawe Hospital, which is located in Metekel zone, are the only tertiary health care hospitals serving the majority of the population of the region.12 Then, according to the patients present in each hospital, the sample size was assigned to each hospital and the K interval was 6.
Data Processing and Analysis Procedure
To enable analysis, the collected data was cleaned and entered into Epi data version 3.0.2 and exported to SPSS version 22 for further analysis and then registered, classified, and sorted. To define the characteristics of participants, frequency, percentage, mean, and standard deviation/median and IQR were used. To present the outcome, tables and figures were used. To classify potential variables related to the outcome variable, bivariate and multivariate logistic regression were used. For multivariate logistic regression, variables with a p-value less than or equal to 0.25 in binary logistic regression were entered to determine the final determinants of the outcome variable. The significance level was declared at a p-value <0.05. To report statistically important variables, the modified odds ratio with a 95% confidence interval was used. For model fitness checkup, the Hosmer and Lemeshow goodness of model fit test was used.
Operational Definitions
Loss to Follow-Up
Patients who have missed more than 3 months of appointment to the same health center since the last planned appointment.13
On Follow-Up
Patients who check up periodically in conjunction with the planned visit.
Incomplete Card
When one of the independent variables is not recorded like CD4 cells, WHO level, functional status and Tuberculosis status or other variables.
Result
Sociodemographic Characteristics of Antiretroviral Therapy Patients
The median age of participants was 35 years with an interquartile range (IQR) of 28–42 years for each case and 35 years with an IQR of 30–42 years for the controls. Gender, age group, marital status, educational level and job status were substantially different between cases when compared to controls. Compared to this the patients in treatment, a high proportion of lost to follow up patients more than 50% were male in gender. In the age group over 45 years old, a high percentage of lost to follow up was relative to those in treatment. In lost to follow up patients, single and split patients were prevalent than in treatment, respectively (Table 1).
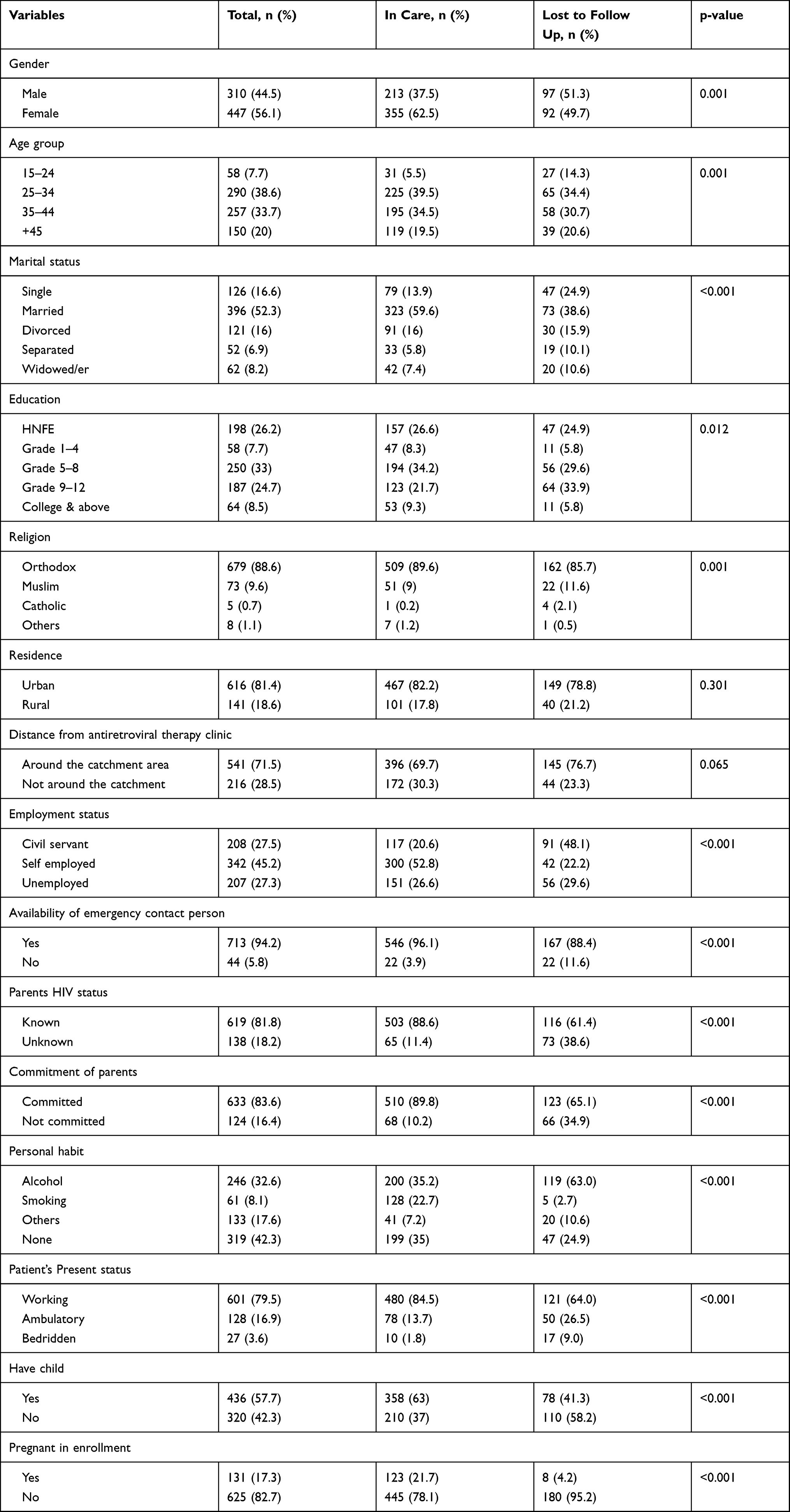 |
Table 1 Sociodemographic Characteristics of Antiretroviral Therapy Patients in Tuberculosis Centers in Public Hospitals of Benishangul-Gumuz, Ethiopia (January 1, 2016 to December 31, 2018) (n=757) |
Clinical Characteristics of Antiretroviral Therapy Patients
More than 80% disclosed their HIV status only by spouse/family members among the research participants, more than 50% were in stage I HIV, above 90% were registered for their next appointment. In cases versus controls, referral results, declaration of HIV status, CD4 count, WHO level, next appointment record, INH prophylaxis, antiretroviral therapy eligibility, and justification for initial antiretroviral therapy adjustment were substantially different. In terms of referral results, more than 75% were referred inside the hospital, compared to lost to follow up patients in treatment. Large number of lost to follow up patients were just above 75% of patients in treatment reported their HIV status to spousal/family members, just below 50% of lost to follow up patients accounted for 200 cells/μL of their CD4 compared to other patients in care, and WHO stage IIIlost to follow-up patients compared with patients in care. Nearly 15% of lost to follow up patients did not have their next visit, compared with patients in care (Table 2).
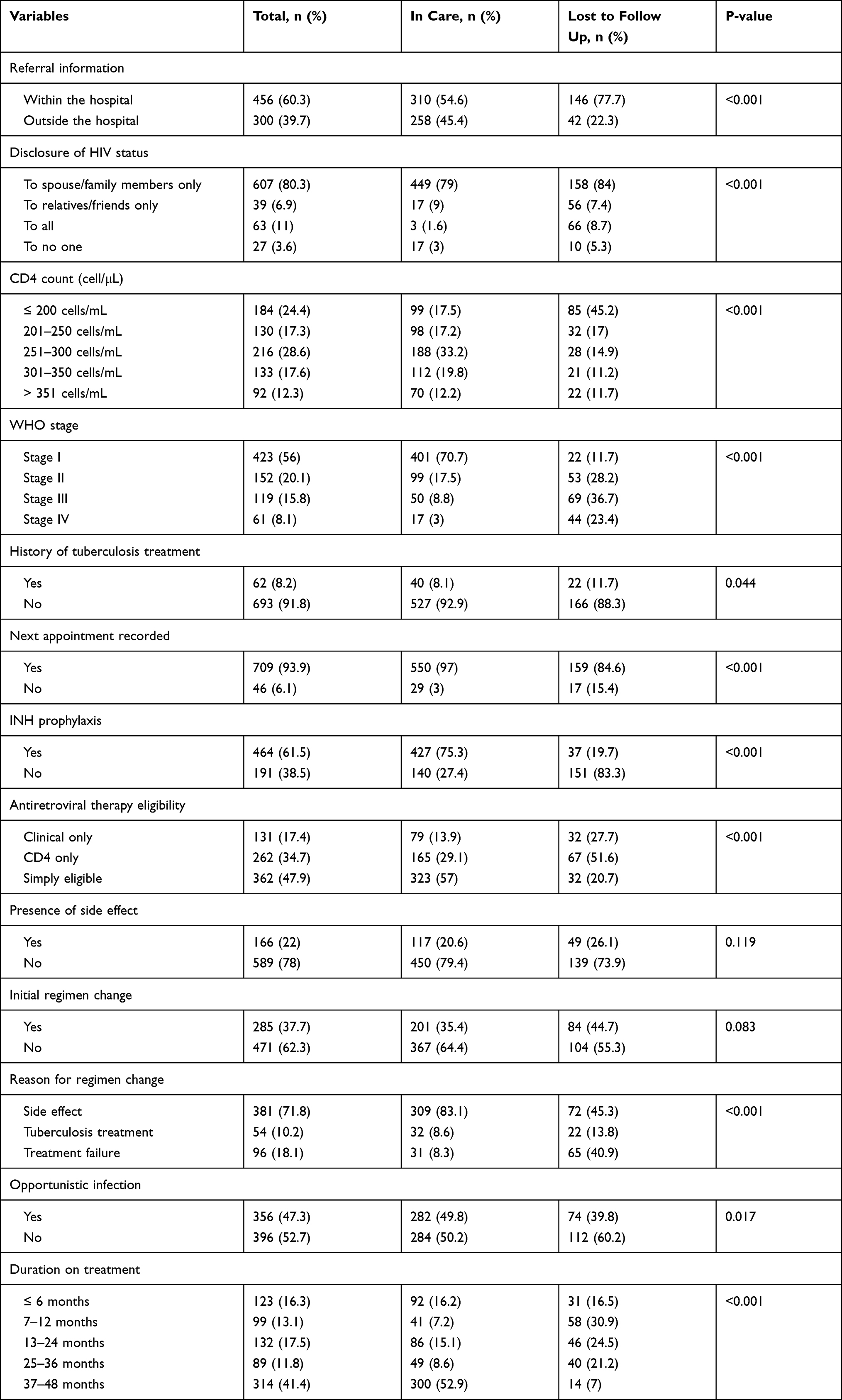 |
Table 2 Clinical Characteristics of Antiretroviral Therapy Patients in Tuberculosis Centers in Public Hospitals of Benishangul-Gumuz, Ethiopia (January 1, 2016 to December 31, 2018) (n=757) |
Sociodemographic and Clinical Factors Associated with Lost to Follow Up
After controlling the possible confounders, the lost to follow up odds were higher among research participants in indexed cases who were male, aged 15–24 years, without formal education and grade 9–12, respectively. Civil servants, alcohol abusers, smokers and other drug consumers showed lost to follow up odds were lower among indexed cases with HIV status of known parents, working and outpatient patients and sociodemographic characteristics, respectively (Table 3).
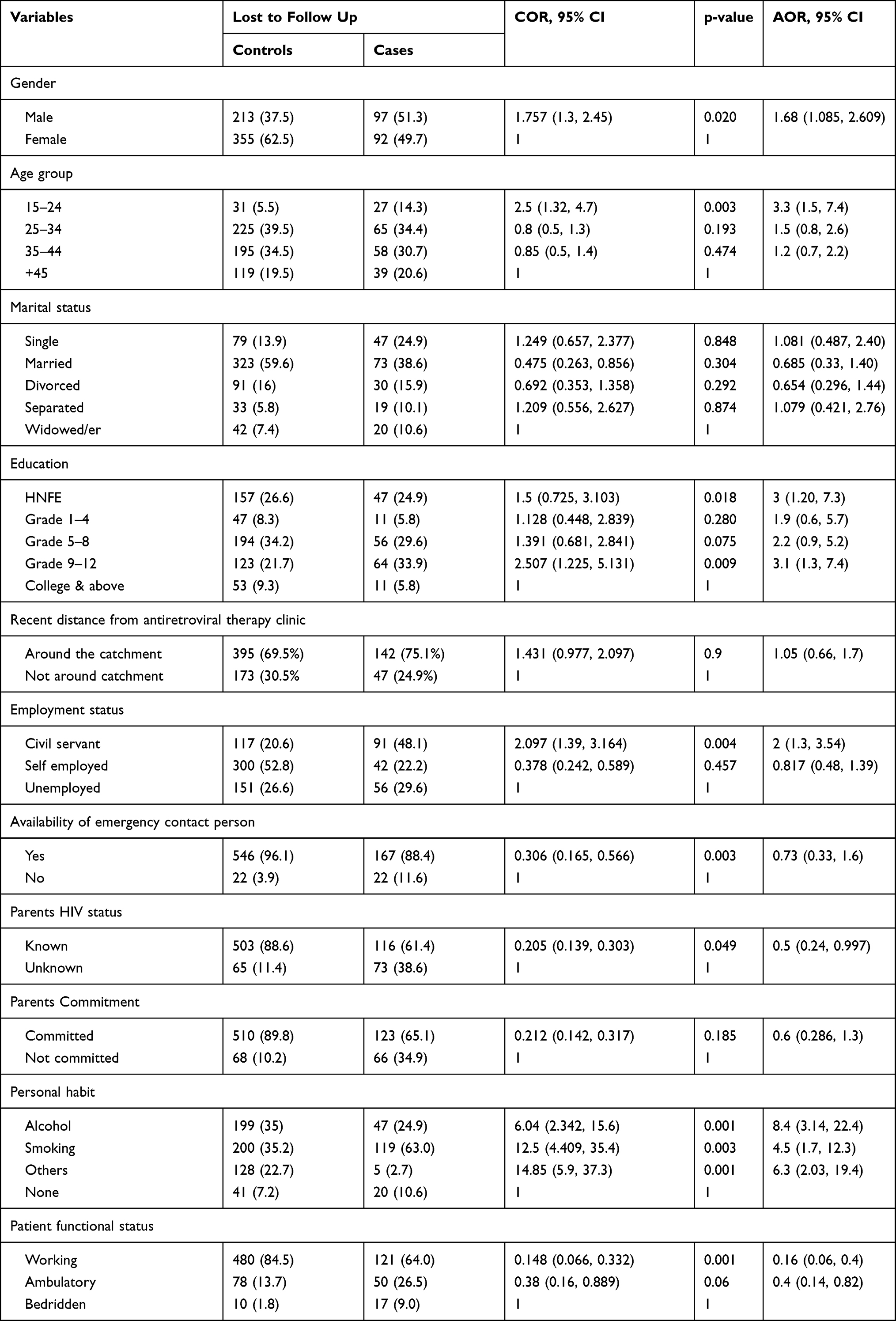 |
Table 3 Association of Socio-Demographic Characteristics of Patients with LT Lost to Follow Up FU from Antiretroviral Therapy in Tuberculosis Centers in Public Hospitals of Benishangul-Gumuz, Ethiopia (January 1, 2016 to December 31, 2018) (n=757) |
Similarly, among the clinical features of the patients, the chances of lost to follow up were higher among the initial regimen shift index cases, side effects, Tuberculosis treatment, and the odds of lost to follow up were lower among the publicly disclosed HIV status, WHO disease stage I and II and the next appointment and INH prophylaxis were registered (Table 4).
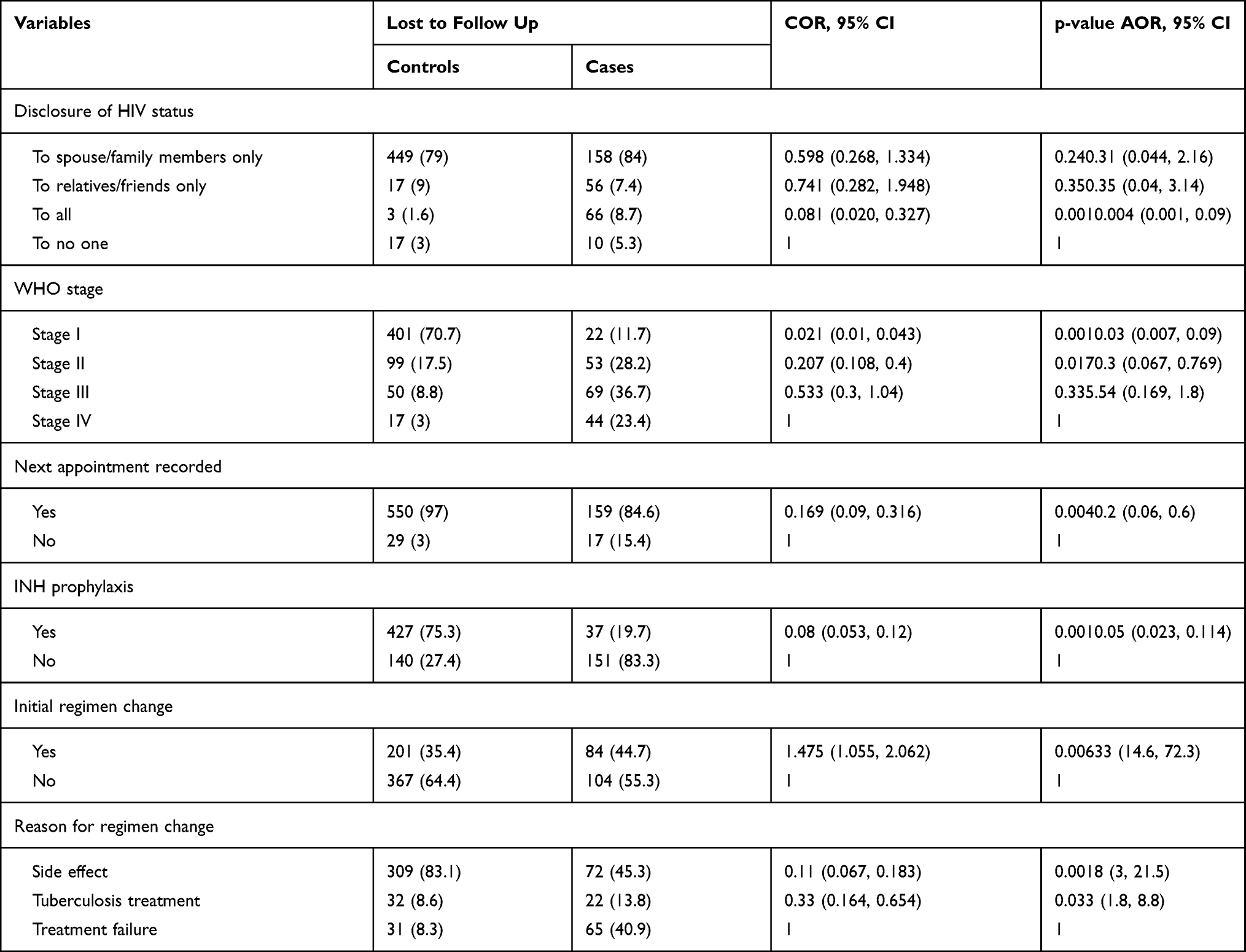 |
Table 4 Association of Clinical Characteristics of Patients with Lost to Follow Up from Antiretroviral Therapy in Tuberculosis Centers in Public Hospitals of Benishangul-Gumuz, Ethiopia (January 1, 2016 to December 31, 2018) (n=757) |
Discussion
We investigated that there was an improvement in weight (50.9+9.9 vs 52.1+10.5 Kg) as well as in immune function (evidenced by increasing CD4 cell counts) (>350 cells/mL CD4 cell counts 92 (12.2%) vs 348 (46.2%) from the time of start of antiretroviral therapy until the last known measurements both in lost to follow up patients.
The complexities of keeping patients in treatment that contribute a lot in improving the long-term effect of antiretroviral therapy services need to be understood and discussed. It is also important that antiretroviral therapy programs develop a framework that guarantees that patients are routinely tracked for care and treatment facilities,8 For this cause, we decided to research the degree of follow-up and its determinants among patients prompted by antiretroviral therapy in Tuberculosis centers in public hospitals of Benishangul-Gumuz.
In this study, a single institution-based report that reported the level of lost to follow up was reported to be 25.3%, which was greater than the study finding in Wukro primary hospital, Tigray regional state, in 2011, (11%),14 The distinction may be that the prior research was based on a small sample size and a single primary hospital, it was therefore larger than the outcome of the study Adama (23.7%),15 Turkey (7.5%),16 The potential explanations for the disparity may be the research period and duration of the study. The outcome was close to the result of the analysis in Malawi (26%),17 however, for both pre-antiretroviral therapy and after antiretroviral therapy enrolment, this research outcome was placed in an average of lost to follow up, if only lost to follow-up is measured after antiretroviral therapy initiation could be lower than our result. The outcome was also lower than the studies that resulted in Gender which was 29.2%16 and in St. Luke Catholic Hospital, Ethiopia, which was 61.8%,9 India (39%),18 The potential cause for the disparity may be due to the impact of the recently adopted patient recruitment policy and patient retention initiatives that allow early enrollment for antiretroviral therapy and improve patient commitment to antiretroviral therapy, as well as comprehensive patient treatment, community-based support services for adherence, patient active outreach.
Our research analyzed numerous lost to follow up-related socio-demographic and clinical variables and found they were all substantially associated with improved antiretroviral therapy correlating with the study done in Iran.19
Male patients were nearly twice as likely as their female counterparts to be lost to follow-up from antiretroviral therapy, study findings in Gonder,20 Oromia,4 Goba,21 India,18 Aksum20 reported similarly while study results in Ethiopia22 and Malawi contrasts the finding since these research findings suggest that males were more likely to conform to antiretroviral therapy.17 This result shows that in antiretroviral therapy patients, gender is a sensitive problem that requires focus and attention.
Age of antiretroviral therapy patients was a major determinant of lost to follow up, antiretroviral therapy patients were three times more likely to be missed from therapy in the age group of 15–24 years than patients over 45 years of age, this may be because those 15–24 years of age do not have a permanent job as much as most of the time they have a temporary address, this finding is consistent with the outcome of the study in Iran,23 Ethiopia,22 India,18 Malawi.17
Our research showed that lost to follow up was strongly correlated with patients who had no formal schooling. Three times more likely to be lost to follow-up than college and beyond the educational status of antiretroviral therapy patients who have no formal experience. That result was consistent with the outcome of studies in Ethiopia,22 Southern Ethiopia24 and India,18 the possible reason might be if they have no formal education, they might not appreciate the benefit of antiretroviral therapy, and it needs more effort to make them adhere to the therapy so they are at high risk of lost to follow up.
Different research results found that civil servants were more vulnerable to antiretroviral therapy follow-up loss in oromia,4 Nekemte25 parallel with this in our analysis also identified that being civil servants were twice as likely to raise the chances of antiretroviral therapy follow-up loss. This may be linked to fear of stigma, which strongly relates to the study results.
The chances of lost to follow up on antiretroviral therapy were more likely to rise in patients with a personal smoking/alcohol drinking/other drug user habit. It is parallel with the results of the analysis in Goba,21 Jimma,11 the possible reason might be smoking/alcohol drinking/other substance abuse may influence their judgment on the therapy.
In line with this, our study showed that antiretroviral therapy patients with established parental HIV status were 0.5 times less likely to lose their HIV status on antiretroviral therapy than patients with uncertain parental HIV status, understanding their parents HIV status has a vital role to play in increasing patient commitment to treatment and therapy efficacy in Goba,21 Nekemte.25
For patients lost to follow-up, our research showed that working and outpatient patients were less likely to be lost to antiretroviral therapy follow-up than bedridden patients. Patients functional status has its own contribution, respectively. This was consistent with study finding in Jimma.11
Initial change in antiretroviral therapy regimen was described as a positive determinant of loss in antiretroviral therapy follow-up, patients who had reported an initial change in antiretroviral therapy regimen were 33 times more likely be lost from follow-up than patients without an initial change in antiretroviral therapy regimen. This may be because the original explanation for the initial change in antiretroviral therapy could be due to side effect, Tuberculosis treatment or medication failure, and if patients changed the antiretroviral therapy, patients may again experience severe drug side effect and might not understand the value of the therapy, follow-up and then might become hopeless since the presence of side effects of antiretroviral therapy are found to be a positive determinant of loss to follow in India.18
Disclosure of HIV status has been dramatically correlated with patients who have missed antiretroviral therapy follow-up, as the degree of disclosure increases from person to public, the risk of loss from follow-up decreases; this may be due to a shift in understanding of the community’s HIV/AIDS myth as well as patient’s awareness of exposing their HIV status.
A protective determinant of lost to follow up was the lower stage of the disease (WHO stage I and II), with WHO stage I and II 0.97 times to minimize the risk of lost to follow up. This suggests that the advanced stage of the disease raises the risk of lost to follow up, which was parallel to the result of studies in oromia,4 south Africa,24 Malawi,17 southern Ethiopia,24 Zimbabwe,13 Jimma11 and It contrasted with the conclusions of the report in gonder,20 This intensifies the importance of focusing on patients whose viral loads stay elevated and/or who, after taking antiretroviral therapy, appear to demonstrate advanced clinical stages of HIV disease.
Patients who had the next appointment date reported were 0.2 times less likely to lose antiretroviral therapy than those who had the next appointment date recorded, as it is understood that there would be a high risk of loss to follow-up if the next appointment date is not recorded, this finding was also consistent with study result in Gonder.20
Patients who have undergone INH prophylaxis following screening are less likely to loss antiretroviral therapy. Taking INH prophylaxis reduces the risk of failure of antiretroviral therapy follow-up by 95%. The results were comparable to the study paper from Wukro,20 oromia,4 Jimma.11 This may be because INH prophylaxis tends to improve patient immunity and helps to reduce the occurrence of side effects and opportunistic diseases. Our research showed that there was a strong association between people who received INH prophylaxis and their disease stage (p-value=0.001).
Conclusion
A large number of patients enrolled in antiretroviral therapy were lost to follow-up from Tuberculosis centers in public hospitals of Benishangul-Gumuz Region of Ethiopia. The study found out that the rate of lost to follow-up is high. The LTFU rate could also be minimized by paying particular attention to high-risk groups for incomplete follow-up. Accessible intervention modalities should be improved to mitigate the LTFU by targeting identified risk factors. LTFU was a big concern, and this could extend to other related ART facilities. More than half of the patients were lost to follow-up soon after enrolment, likely resulting in high mortality. The study suggested that retention of the patients should be given high priority.
Purpose of the Study
The purpose of this Hospital-based, unrivalled analysis of the case management (3:1) case control research design is to discover Influence of lost to follow up from antiretroviral therapy among retroviral Infected patients at tuberculosis centers in public Hospitals of Benishangul-Gumuz, Ethiopia. The study aims to understand the status and deciding factors of ART in TB centers in public hospitals of this part of the world, for LTFU among RVI patients. The study was mainly done to explain how retention of the patients will affect in breaking down the failure of antiretroviral treatment which plays an very important role in prognosis of tuberculosis in HIV infected patients.
Duplicated Publication
The writers affirm that the manuscript is original, that it has not been published in a journal, and that no other journal is presently being considered.
Abbreviations
ART, antiretroviral therapy; RVI, Retroviral Infected; LTFU, loss to follow-up; AIDS, acquired immunodeficiency syndrome; TB, tuberculosis; WHO, World health Organization; HIV, human immunodeficiency virus; PLWH, People Living with HIV/AIDS; FHAPCO, Federal HIV AIDS Prevention and Control Office.
Ethical Approval
All studies were conducted in conjunction with the standards for human research as set out in the Helsinki Declaration and the recommendations for the International Conference on Harmonization of Good Clinical Practice. Asossa Hospital and Bule Hora University, institutional review board gave ethical clearance to conduct the study. Respondents were told of the study’s intent and goals. After receiving verbal consent from each individual, the data were obtained.
Consent
A well-informed written consent was obtained from each research participant after the possible risks and benefits as well as the investigational purpose of the study were identified.
Acknowledgments
The researcher would like to thank all the participants and everyone who contributed directly or indirectly in the progress of research work.
Author Contributions
Author made substantial contributions to conception and design, acquisition of data, or analysis and interpretation of data; took part in drafting the article or revising it critically for important intellectual content; agreed to submit to the current journal; final approval of the version to be published; and agree to be accountable for all aspects of the work.
Funding
The author obtained no financial assistance for this article’s analysis, authorship, and/or publishing.
Disclosure
The author reports no conflicts of interest in this work.
References
1. Shewangizaw Z, Girma M, Endazenaw G. Assessment of HIV Sero-Prevalence among St. Marry University Students. Ethiopia Sci J Public Health. 2015;3(4):468–477. doi:10.11648/j.sjph.20150304.14
2. World Health Organization. Consolidated guidelines on the use of ART drugs for treating and preventing HIV infection. Geneva: World Health Organization; 2016.
3. Central Statistical Agency, and ORC Macro. Ethiopia Demographic and Health Survey 2005. Health San Francisco; September 2006: 446.
4. Megerso A, Garoma S, Eticha T, et al. Predictors of loss to follow-up in antiretroviral treatment for adult patients in the Oromia region, Ethiopia. HIV AIDS. 2016;8:83–92. doi:10.2147/HIV.S98137
5. Alvarez-Uria G, Midde M, Pakam R, Naik PK. Predictors of attrition in patients ineligible for antiretroviral therapy after being diagnosed with HIV: data from an HIV Cohort Study in India. Biomed Res Int. 2013;5.
6. Mohammed F, Assefa N. Determinants of desire for children among HIV-Positive women in the afar region, Ethiopia: case control study. PLoS One. 2016;11:e0150566. doi:10.1371/journal.pone.0150566
7. Assefa Y, Kiflie A, Tesfaye D, et al. Outcomes of antiretroviral treatment program in Ethiopia: retention of patients in care is a major challenge and varies across health facilities. BMC Health Serv Res. 2011;11:81. doi:10.1186/1472-6963-11-81
8. Hontelez JAC, Chang AY, Ogbuoji O, de Vlas SJ, Bärnighausen T, Atun R. Changing HIV treatment eligibility under health system constraints in sub-Saharan Africa. AIDS. 2016;30(15):2341–2350. doi:10.1097/QAD.0000000000001190
9. Somi G, Keogh SC, Todd J, et al. Low mortality risk but high loss to follow-up among patients in the Tanzanian national HIV care and treatment programme. Trop Med Int Health. 2012;17(4):497–506. doi:10.1111/j.1365-3156.2011.02952.x
10. Berheto TM, Haile DB, Mohammed S. Predictors of loss to follow-up in patients living with HIV/AIDS after initiation of antiretroviral therapy. N Am J Med Sci. 2014;6(9):453–459. doi:10.4103/1947-2714.141636
11. Deribe K, Hailekiros F, Biadgilign S, Amberbir A, Beyene BK. Defaulters from antiretroviral treatment in Jimma University Specialized Hospital, Southwest Ethiopia. Trop Med Int Health. 2008;13(3):328–333. doi:10.1111/j.1365-3156.2008.02006.x
12. Benishangul-Gumuz Region [Internet]. Benishangul-Gumuz Region; 2021. Available from: https://en.wikipedia.org/wiki/Benishangul-Gumuz_Region.
13. Mutasa-Apollo T, Shiraishi RW, Takarinda KC, et al. Patient retention, clinical outcomes and attrition-associated factors of HIV-infected patients enrolled in Zimbabwe’s National Antiretroviral Therapy Programme, 20072010. PLoS One. 2014;9:e86305. doi:10.1371/journal.pone.0086305
14. Dessalegn M, Tsadik M, Lemma H. Predictors of lost to follow up to antiretroviral therapy in primary public hospital of Wukro, Tigray, Ethiopia: a case control study.”. J AIDS HIV Res. 2015;7:1–9. doi:10.5897/JAHR2014.0315
15. Endebu T, Deksisa A, Moges T, Kisi T, Ensermu T. Incidence of virological failure and associated factors among adult HIV-Positive patients on first line antiretroviral therapy regimen, Central Ethiopia. Int J HIV/AIDS Prevent Edu Behav Sci. 2018;4(2):44–51.
16. Etienne M, Burrows L, Osotimehin B, et al. Situational analysis of varying models of adherence support and loss to follow up rates; findings from 27 treatment facilities in eight resource limited countries. Trop Med Int Health. 2010;15(Suppl 1):76–81. doi:10.1111/j.1365-3156.2010.02513.x
17. Tweya H, Oboho IK, Gugsa ST, et al. Loss to follow-up before and after initiation of antiretroviral therapy in HIV facilities in Lilongwe, Malawi. PLoS One. 2018;13(1):e0188488. doi:10.1371/journal.pone.0188488
18. Alvarez-Uria G, Naik PK, Pakam R, et al. Factors associated with attrition, mortality, and loss to follow up after antiretroviral therapy initiation: data from an HIV cohort study in India. Glob Health Action. 2013;6:21682. doi:10.3402/gha.v6i0.21682
19. Morowatisharifabad MA, Movahed E, Farokhzadian J, et al. Antiretroviral therapy adherence and its determinant factors among people living with HIV/AIDS: a case study in Iran. BMC Res Notes. 2019;12(1):1–5.
20. Ahmed I, Gugsa ST, Lemma S, Demissie M. Predictors of loss to follow-up before HIV treatment initiation in Northwest Ethiopia: a case control study. BMC Public Health. 2013;13. doi:10.1186/1471-2458-13-867
21. Setegn T, Takele A, Gizaw T, Nigatu D, Haile D. Predictors of mortality among adult antiretroviral therapy users in southeastern Ethiopia: retrospective cohort study. AIDS Res Treat. 2015;2015:1–8. doi:10.1155/2015/148769
22. Melaku Z, Lamb MR, Wang C, et al. Characteristics and outcomes of adult Ethiopian patients enrolled in HIV care and treatment: a multi-clinic observational study. BMC Public Health. 2015;15. doi:10.1186/s12889-015-1776-4
23. Morowatisharifabad MA, Movahed E, Nikooie R, et al. Adherence to medication and physical activity among people living with HIV/AIDS. Iran J Nurs Midwifery Res. 2019;24(5):397–399. doi:10.4103/ijnmr.IJNMR_205_18
24. Belayneh M, Moges M, Mekonnen E, et al. Do loss to follow-up and death rates from ART care vary across primary health care facilities and hospitals in south ethiopia? A retrospective follow-up study. HIV/AIDS - Res Palliat Care. 2015.
25. Kebede A, Wabe NT. Medication adherence and its determinants among patients on concomitant tuberculosis and antiretroviral therapy in south west Ethiopia. N Am J Med Sci. 2012;4:67–71. doi:10.4103/1947-2714.93376
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.