")
Back to Journals » Infection and Drug Resistance » Volume 16
Influence of Appropriate Empirical Antibiotic Treatment on the Prognosis of ICU Patients with HAP Caused by Carbapenem-Resistant Gram-Negative Bacteria
Authors Zhang X, Jin X, Ren J, Liu J, Ma H, Fang X, Zhang H, Zhao Y, Hou Y, Luo Y, Guo L, Ma Q, Gao Y, Zhang J, Li J, Wang X, Wang G
Received 21 February 2023
Accepted for publication 18 May 2023
Published 30 May 2023 Volume 2023:16 Pages 3389—3398
DOI https://doi.org/10.2147/IDR.S407383
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 6
Editor who approved publication: Professor Suresh Antony
Xiaoling Zhang, Xuting Jin, Jiajia Ren, Jueheng Liu, Haichang Ma, Xiaoming Fang, Huifan Zhang, Yujie Zhao, Yanli Hou, Yanni Luo, Lei Guo, Qi Ma, Ya Gao, Jingjing Zhang, Jiamei Li, Xiaochuang Wang, Gang Wang
Department of Critical Care Medicine, the Second Affiliated Hospital of Xi’an Jiaotong University, Xi’an, Shaanxi Province, People’s Republic of China
Correspondence: Xiaochuang Wang; Gang Wang, Department of Critical Care Medicine, the Second Affiliated Hospital of Xi’an Jiaotong University, 157 Xi 5 Lu, Xi’an, Shaanxi, 710004, People’s Republic of China, Tel +86-029-8767-9630 ; +86-029-8767-9633, Email [email protected]; [email protected]
Purpose: In patients with carbapenem-resistant Gram-negative bacteria (CRGNB) infection, the impact of appropriate empirical antibiotic treatment (AEAT) initialized before culture results were available remains controversial. We aimed to investigate the effect of AEAT on the prognosis of critically ill patients with hospital-acquired pneumonia (HAP) caused by CRGNB.
Patients and Methods: Patients with CRGNB-infected HAP and received empirical antibiotic treatment (EAT) for at least 3 days in the intensive care unit (ICU) of a tertiary teaching hospital in China from February 2017 to September 2021 were included in the retrospective cohort study. Patients were categorized into AEAT and inappropriate empirical antibiotic treatment (IEAT) groups based on whether they received EAT covering CRGNB. The associations of AEAT with ICU and 28-day mortality were assessed using multivariable logistic regression model.
Results: A total of 94 patients were enrolled, including 29 patients in AEAT group and 65 patients in IEAT group. Patients in AEAT group had a higher Sequential Organ Failure Assessment (SOFA) score (P = 0.003), levels of procalcitonin (PCT) (P = 0.001), and lactic acid (LAC) (P = 0.026); while patients in the IEAT group had a higher platelet count (PLT) (P = 0.001). There was no significant difference in the length of ICU stay between the two groups (P = 0.051). Compared with IEAT, AEAT was associated with an increased risk of 28-day mortality in the univariable logistic regression model (OR: 2.618, 95% CI: 1.063– 6.448). However, after adjusted for SOFA score, PLT, PCT, and LAC level, the association between AEAT and 28-day mortality diminished (OR: 1.028, 95% CI: 0.353– 2.996). AEAT showed no significant association with ICU mortality in neither univariable (OR: 1.167, 95% CI: 0.433– 3.142) nor multivariable (OR: 0.357, 95% CI: 0.097– 1.320) models.
Conclusion: AEAT showed no significant influence on ICU or 28-day mortality in critically ill patients with HAP caused by CRGNB infection.
Keywords: appropriate empirical antibiotics, hospital-acquired pneumonia, carbapenem-resistant, gram-negative bacteria, ICU mortality
Introduction
Patients in intensive care units (ICUs) were more likely to develop health care-associated infections and multidrug-resistant organisms (MDROs) infection due to underlying diseases with disordered pathophysiological conditions.1,2 The procedures undertaken in ICU pose a risk of secondary infections, and the widespread use of broad-spectrum antibiotics in ICU contributes to antimicrobial resistance.2,3 Since 2000, there has been a steady increase in the incidence rates of extended-spectrum β-lactamase-producing (ESBL) Enterobacteriaceae, carbapenem-resistant Enterobacteriaceae (CRE), and multidrug-resistant strains of Pseudomonas aeruginosa (MDRPA) and Acinetobacter baumannii in the United States.4 A report from 341 ICUs in Germany showed an MDRO infection rate of 3.81%.5 Another study from 6 ICUs in New York City showed an average monthly MDRO infection rate of 5.24 per 1000 person days.6 It has been reported that antimicrobial resistance Gram-negative bacteria were the most commonly isolated. Among Gram-negative isolates, Acinetobacter baumannii showed high resistance to antibiotics (95–99%) except for colistin. Klebsiella pneumoniae isolates were mostly resistant to Cefotaxime (72.7%), and Pseudomonas aeruginosa was resistant to Ciprofloxacin (40.3%).7 MDRO infection in ICU patients not only prolongs the length of hospital stays and increases the economic burden but also increases the risk of adverse outcomes.8
For patients with MDRO infection, delayed initiation of antibiotic therapy has often been regarded as a significant risk factor for mortality,9 which supports the idea of early empirical antibiotic treatment. However, whether appropriate empirical antibiotic treatment (AEAT) improves prognosis in patients with MDRO infection is unclear. On the one hand, studies have shown that AEAT was not associated with mortality in patients with bacteremia and pneumonia caused by CRGNB.10,11 On the other hand, it was found that in bloodstream infections with multidrug-resistant Acinetobacter bacteremia, AEAT was associated with decreased ICU mortality risk.12 In a study of patients with hematologic malignancies, empirical treatments that covered CRE were associated with lower 30-day mortality.13 Moreover, although hospital-acquired pneumonia (HAP) was common in ICU patients, evidence on the effectiveness of AEAT in CRGNB-infected HAP patients remained rare. Therefore, our study aims to further assess whether AEAT can reduce ICU mortality in HAP patients caused by CRGNB in ICU.
Materials and Methods
Study Design and Participants
This is a retrospective cohort study of CRGNB-infected HAP patients. Participants were enrolled from February 2017 to September 2021 in the ICU of a tertiary teaching hospital in China. Adult patients (≥18 years) received anti-CRGNB therapy were extracted from ICU records. Exclusion criteria were: (1) patients with anti-CRGNB treatment lasted for less than 3 days; (2) patients with bacterial culture denied CRGNB infection or confirmed mixed infections; (3) patients with non-HAP or multisite infections. Patients were divided into AEAT and IEAT groups according to whether received empirical antibiotic therapy against CRGNB. For patient with suspected HAP infections, sputum or bronchoalveolar lavage fluid cultures were obtained for culture test before empirical antibiotic treatment. The timing of empirical antibiotic treatment is within 3 hours after HAP happened. When the culture result is positive, drug sensitivity analysis will be carried out at the same time. It usually takes 36 h to 48 h to confirm the microbial diagnosis in our hospital. The study was approved by the ethics committee of the hospital (NO. 2023042). Since this was a retrospective study and individual patient information was withheld, informed consent was exempt.
Definitions
HAP was defined as pneumonia that occurred 48 hours or more after hospital admission.14 Ventilator-associated pneumonia (VAP) was determined by pneumonia in patients exposed to invasive mechanical ventilation for at least 48 hours. Pneumonia was diagnosed when new or progressive lung infiltrates were proved by Chest X-ray or CT test, plus the presence of two or more following symptoms: (1) fever, T >38 °C; (2) purulent sputum; and (3) peripheral leucocyte count >10,000/mm3 or <4000/mm3. Empirical antibiotic treatment was defined as administration of antimicrobial agents before culture results and susceptibility test results were available. AEAT was defined as administration of at least one antimicrobial agent that was sensitive against CRGNB isolated in vitro. IEAT was defined as administration of antimicrobial agents that was not sensitive against CRGNB isolated in vitro. The anti-CRGNB regimen was comprised of tigecycline or polymyxins in combination with Fosfomycin, meropenem, imipenem, quinolone, aminoglycoside, ceftazidime-avibactam, or sulfamethoxazole.15 Microbiological response includes clearance and presumptive clearance. Clearance refers to the absence of the pathogen of the original infection in the specimen from the respiratory tract after treatment. Presumptive clearance refers to the disappearance of symptoms and signs as treatment progresses, making sputum samples inaccessible or the method of obtaining sputum is too invasive for the recovering patient, and the microbiological results are considered presumptive clearance.
Variables and Outcomes
Antibiotic therapy types (AEAT or IEAT) were the primary independent variables. The primary outcome was ICU mortality, defined as the occurrence of death before ICU discharge for any reason. The secondary outcomes were 28-day mortality and length of ICU stay. 28-day mortality was defined as all-cause mortality at 28 days. Demographic information and clinical data were extracted from the hospital information system, including age, gender, comorbidity, usage of immunosuppressive, duration of carbapenem (d), mechanical ventilation (h), and vasopressor (d) before day of onset. At the same time, we extracted laboratory tests on day of onset, including blood indices, procalcitonin (PCT), C-reactive protein (CRP), LAC, total bilirubin (TBI), albumin (ALB), urea nitrogen, and creatinine. SOFA score on day of onset, Acute Physiology and Chronic Health Evaluation (APACHE) II on day of onset, type of bacteria, antibiotics, microbiological response, duration of mechanical ventilation after HAP, and outcomes were also collected.
Microbiology Methods
Identification of Gram-negative bacteria species was done by the VITEK-II-COMPACT instrument (BioMerieux, France). These isolates were tested for antimicrobial susceptibility to different antibiotics by Broth microdilution test. Interpretation of susceptibility was done according to the Clinical and Laboratory Standards Institute (CLSI) 2017 guidelines.
Statistical Analysis
Continuous variables using t-test or Mann–Whitney U-test according to their distribution, the results were expressed as mean ± standard deviation and median (interquartile range), respectively. Categorical variables were presented as frequencies with percentages and were compared using Chi-square or Fisher’s exact test. We used univariable and multivariable logistic regression models to assess the association between the type of antibiotic therapy (AEAT or IEAT) and ICU or 28-day mortalities.16,17 Associations between mortalities and all the covariates were examined by univariable logistic regression model. Covariates showed significant impact on mortalities in univariable analysis were entered into a multivariable logistic regression. Risk factors for ICU mortality were further screened by logistic regression models. Sensitivity analysis was also performed. Propensity scores were used to match patients in the AEAT group and the IEAT group. A multivariable logistic regression model, including SOFA score, PLT, PCT and LAC, was constructed to generate propensity scores. Patients in the AEAT group were matched to patients in IEAT group in a 1:1 ratio using a greedy, nearest neighbor matching algorithm with no replacement. All statistical analyses were performed using SPSS version 18.0 (SPSS, Chicago, IL). A two-sided P-value <0.05 was considered statistically significant.
Results
Patients’ Characteristics
A total of 150 patients met the inclusion criteria. Excluding 33 patients with anti-CRGNB treatment lasted for less than 3 days, 14 patients with bacterial culture denied CRGNB infection or confirmed mixed infections, and 9 patients with non-HAP or multisite infections, 94 were ultimately included in the study, of which 29 (30.9%) were in the AEAT group, and 65 (69.1%) were in the IEAT group. (Figure 1) The mean age was 66.87 ± 1.71 years. Klebsiella pneumoniae was detected in 40 (42.6%) patients, Acinetobacter baumannii in 48 (51.1%) patients, and Pseudomonas aeruginosa in 6 (6.4%) patients. VAP was diagnosed in 68 (72.3%) patients. Treatment options included tigecycline or polymyxins-based combination therapy. (Supplemental Table 1) A total of 24 (25.5%) patients deceased during their ICU stay. The 28-day mortality rate for the overall population was 45.7%.
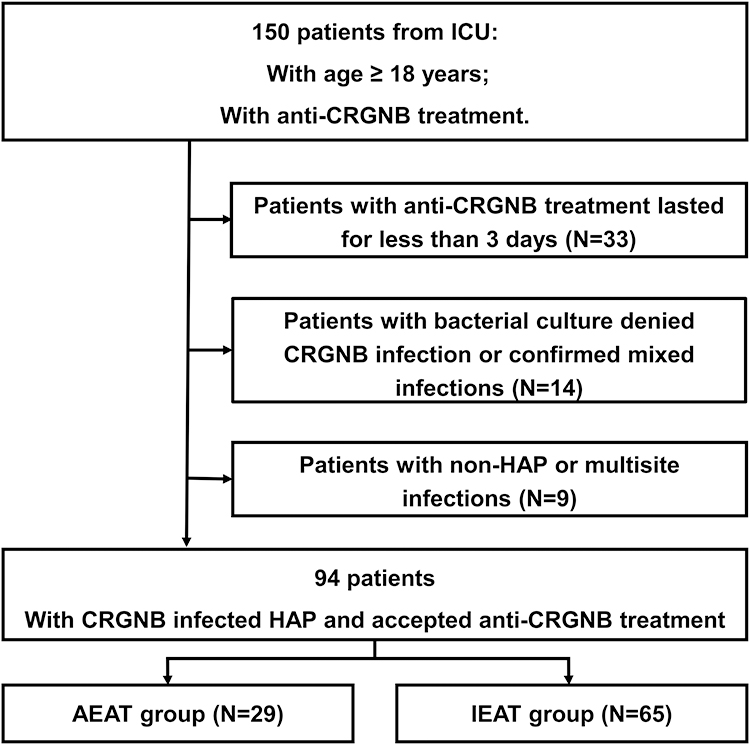 |
Figure 1 Flow chart of participant selection. 94 patients were included in the analysis. Abbreviations: CRGNB, carbapenem-resistant Gram-negative bacteria; AEAT, appropriate empirical antibiotic treatment; IEAT, inappropriate empirical antibiotic treatment. |
Comparison Between AEAT and IEAT Groups
Patients in AEAT group had a higher SOFA score (P = 0.003), levels of PCT (P = 0.004), and LAC (P = 0.029). While patients in the IEAT group had a higher level of PLT (P < 0.001). There was no statistical significance regarding gender, age, comorbidities, duration of carbapenem, vasopressor, and mechanical ventilation before day of onset, the composition of CRGNB, proportion of the microbiological response, the prescription of antibiotics, and the duration of mechanical ventilation after HAP (P > 0.05) between the two groups (Table 1). The ICU mortality and length of ICU stay were also showed no significant difference between the two groups (P > 0.05). The 28-day mortality in the AEAT group was higher than that in the IEAT group (P = 0.036).
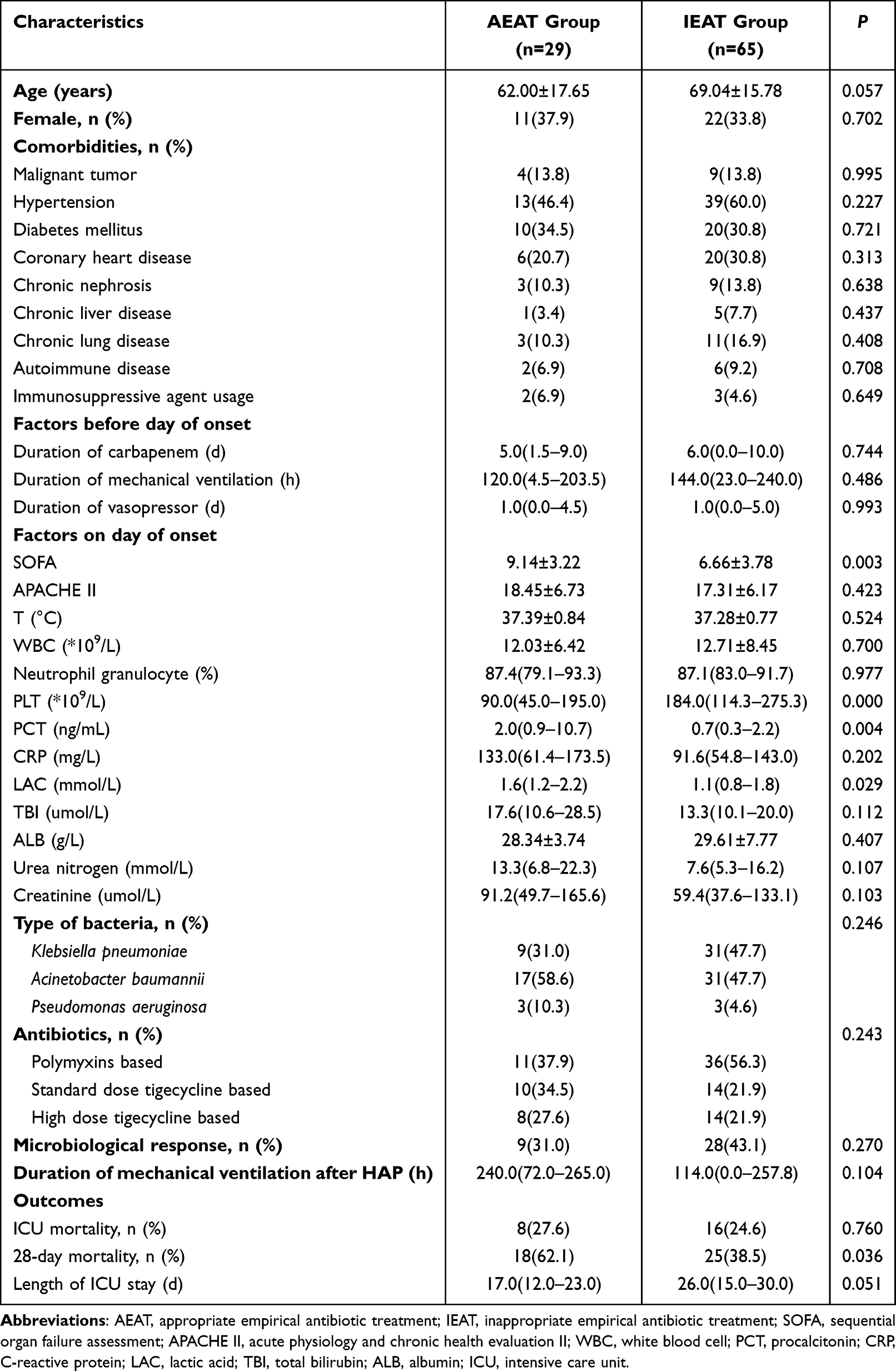 |
Table 1 Characteristics of the Study Subjects |
Association Between AEAT and Mortalities
Compared with IEAT, AEAT was associated with an increased risk of 28-day mortality in the univariable logistic regression model (OR: 2.618, 95% CI: 1.063–6.448). However, after adjusting for SOFA score, PLT, PCT, and LAC level, AEAT was not associated with 28-day mortality (OR: 1.028, 95% CI: 0.353–2.996). AEAT showed no significant association with ICU mortality in both univariable (OR: 1.167, 95% CI: 0.433–3.142) and multivariable (OR: 0.357, 95% CI: 0.097–1.320) models (Table 2).
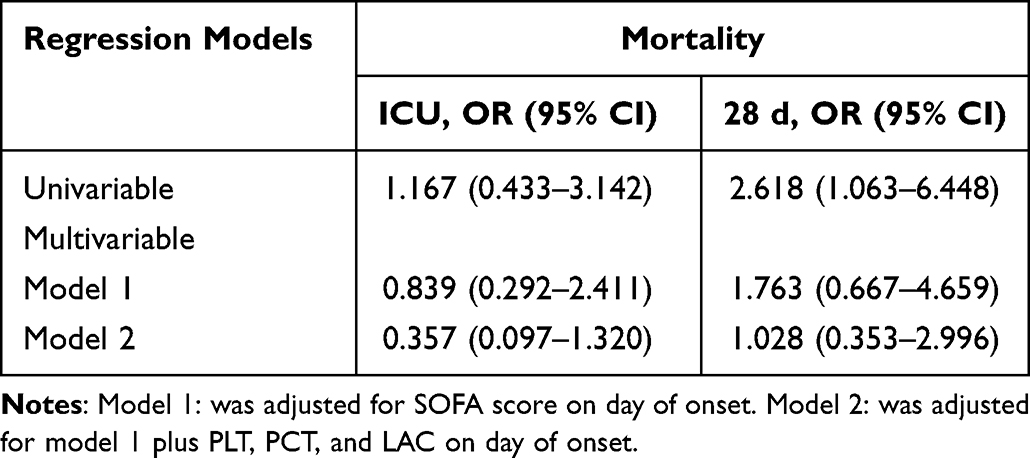 |
Table 2 ORs and 95% CIs for Mortality Associated with AEAT in Overall Patients |
Sensitivity Analysis
Twenty-nine patients in the IEAT group were successfully matched to patients in the AEAT using propensity scores (Table 3). There was no statistical significance regarding SOFA score, PLT, PCT and LAC (P > 0.05) between the two groups after matching. AEAT showed no significant association with ICU or 28-day mortality in univariable models (P > 0.05). SOFA score, PLT, PCT and LAC were included in the multivariable logistic regression model to generate propensity scores. AEAT showed no significant association with ICU mortality (OR: 0.310, 95% CI: 0.080–1.209) or 28-day mortality (OR: 1.082, 95% CI: 0.371–3.160) after adjusting the propensity scores as covariates (Supplemental Table 2).
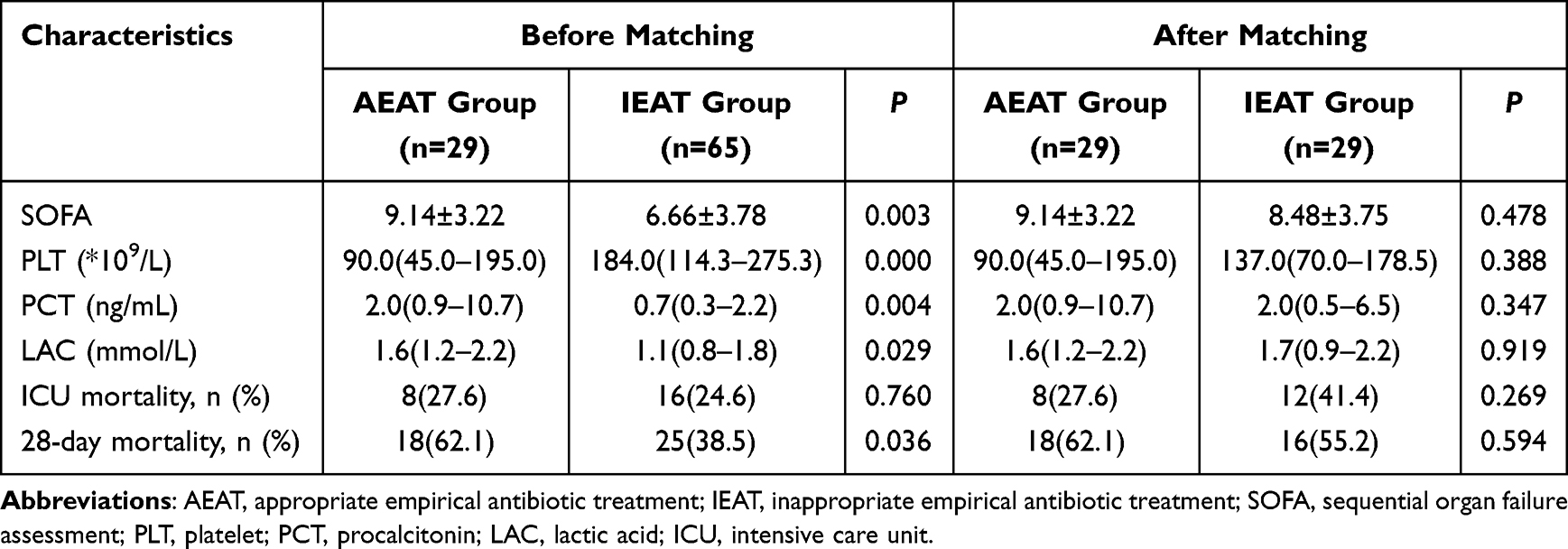 |
Table 3 Characteristics of the Study Subjects Before and After Propensity Score Matching |
Risk Factors for ICU Mortality
The mean SOFA score (8.83 ± 3.45) and mean APACHE II score (21.50 ± 6.16) are both higher in patients deceased (the deceased group) during ICU stay than in those survived (the survived group, P = 0.034 for SOFA score and P < 0.001 for APACHE II score, respectively). The deceased group presented higher levels of WBC (P = 0.041), PCT (P = 0.006), CRP (P = 0.008), and LAC (P = 0.011), lower level of ALB (P = 0.005), lower microbiological response (P < 0.001), and longer duration of mechanical ventilation after HAP (h) (P = 0.003) (Supplemental Table 3).
Discussion
In our retrospective cohort study, multivariable analysis showed no significant difference in ICU and 28-day mortality between AEAT and IEAT in CRGNB-infected HAP patients. There was no significant difference in the length of ICU stay between the two groups. VAP accounted for 72.3% of HAP in our research, consistent with previous studies.18 Carbapenem-resistant Klebsiella pneumoniae (42.6%) and carbapenem-resistant Acinetobacter baumannii (51.1%) were the main pathogens. Treatment options included tigecycline or polymyxins-based combination therapy.
The SSC guidelines state that early administration of appropriate antimicrobials is one of the most effective interventions to reduce mortality in patients with sepsis.19 Studies have shown that the early AEAT can reduce the mortality of ICU patients with septic shock.20 MDRO infections are associated with high morbidity and mortality.21 Delayed initiation of antibiotic therapy has often been considered as a significant risk factor for excess mortality. Therefore, the idea of early empirical antibiotic treatment was recommended by several guidelines.19 Many studies have investigated the efficacy of AEAT in patients with MDRO infection. A multicenter prospective observational cohort study conducted among patients with HAP/VAP caused by MDRO (mainly MDRAB) infection showed that AEAT was significantly associated with reduced mortality.22 Observational studies on patients with MDRPA or CRAB bacteremia showed similar results.23–25 In patients with urinary tract infection, pneumonia, or sepsis caused by CRE infection, AEAT is associated with lower mortality, shorter hospital stays, and lower hospital costs.26 However, some studies showed that AEAT is not related to clinical outcomes in patients infected by ESBL-Enterobacteriaceae or CRGNB. Study performed in the emergency department on patients with bacteremia caused by ESBL-bacteria found no statistical difference in the mortality between patients who received AEAT and those who did not.27 Another study focusing on patients with hematologic malignancy and ESBL-Enterobacteriaceae or CRE bacteremia also found that AEAT did not have influence on duration of hospitalization or 28-day mortality rate.28 A prospective study on patients with invasive infections caused by CRGNB (mainly Acinetobacter baumannii) also found no association between AEAT and 28-day or 14-day mortality.10 The conclusions of the above studies are inconsistent, and previous studies included patients from various sources, while did not focus on those in ICUs. Moreover, the severity of diseases was not evaluated in previous studies. For the first time, our study collected data on patients with HAP caused by CRGNB infection from ICU and a critical care score was collected to comprehensively assess the severity of patients. We collected patients with HAP alone, with more specific types and sites of infection. Our result showed that AEAT had no significant influence on ICU or 28-day mortality.
The reason why treatment with AEAT of CRGNB could not reduce mortality compared with IEAT was not clear. The following two reasons may explain our findings. First, patients with CRGNB infected-HAP suffered from both severe illness and multiple clinical interventions, therefore, the effect of a single therapy may not be easily revealed. Future studies with a larger sample are warranted to further investigate the impact of AEAT. Second, once cultures and susceptibility tests were available, effective antibiotics targeting CRGNB would be initiated even in the IEAT group, which may compensate the impact of inappropriate antibiotic use at first. Our findings can serve as a foundation for future prospective studies on the optimal antibiotic regime for critically ill patients with HAP caused by CRGNB infection.
The emergence of antibiotic-resistant bacteria has driven exploration of treatment options. For ESBL-producing Enterobacteriaceae, it was reported that colistin treatment was associated with increased mortality rate, and poorer clinical and microbiological response than carbapenems.29 However, for multidrug-resistant (MDR) and extensively drug-resistant (XDR) strains of Pseudomonas aeruginosa, Acinetobacter baumannii, and Enterobacteriaceae, the polymyxins have an important role in salvage therapy.30,31 Meanwhile, among carbapenem-resistant Gram-negative pathogens, tigecycline is active against the majority of CRE, Acinetobacter baumannii, and S. maltophilia strains.32 Therefore, in clinical practice, polymyxins and tigecycline have been used as first-line agents for the treatment of infections caused by CRGNB. And the loading dose of them are highly recommended to rapidly increase the drug concentration in serum, particularly among critically ill patients.31,33 As they all have some limitations as a therapeutic agent of CRGNB infection, combination therapy is often suggested.34–36 In our treatment regimen, polymyxins or tigecycline has been proved sensitive by vitro drug sensitivity tests and other antibiotics were combined.
The population selected for this study was HAP patients in ICU. The treatment regimen included tigecycline or polymyxins-based combinations for both groups. ICU patients showed high SOFA scores and APACHE II score because of multiple organ dysfunction and/or complicated comorbidities. Studies have shown that high SOFA score or APACHE II score are associated with increased mortality.37 Our study also found that higher APACHE II score, higher LAC, and lower ALB were risk factors for ICU mortality. It is suggested that the improvement of prognosis may depend on improving the overall condition, timely resuscitation of septic shock, and correction of hypoproteinemia. Treatment with AEAT of CRGNB might not reduce mortality compared with IEAT.
In our study, the AEAT group had higher SOFA scores, LAC, and PCT levels than the IEAT group. Studies have shown that blood lactic acid and SOFA score can be used to evaluate the severity of the infection and predict prognosis.38 As a biomarker, PCT can reflect systemic inflammatory response syndrome caused by bacterial infection to a certain extent,39 and also support and predict the unfavorable prognosis of sepsis.40 When choosing empiric antimicrobial therapy for ICU patients, we combined the diagnosis of infection, the severity of disease, PCT, blood Lac, SOFA score, and the MDR prevalence in our unit.41 Combined with the differences in SOFA scores, we considered that the patients in the AEAT group might be more critical. However, there was no significant difference in ICU mortality between the AETA and IEAT groups by multivariate regression and propensity scores analysis. In future studies, it is necessary to further explore and optimize the use of empirical coverage of CRGNB therapy to avoid excessive exposure to polymyxins or tigecycline and prevent the increase of bacterial resistance.
The advantages of our study were as follows: first, we included HAP patients in ICU and analyzed multiple variables that might impact ICU mortality, including patient demographic statistics, diseases, test results, infection, SOFA, APACHE II scores, and so on. Second, we collected the antibiotic regimens from all patients. Antibiotic treatments were tigecycline or polymyxins-based combinations (in line with guideline recommendations), which may help us exclude the interference of the treatment regimen on the results. Third, the duration of anti-CRGNB treatment in all patients was 3 days at least to ensure the influence of antibiotics. However, as a retrospective study, there are some limitations. Our study was confined to HAP patients in a single ICU with a limited number of cases. Multi-center studies are warranted in the future to comprehensively evaluate the impact of AEAT in hospitals from different regions. Secondly, this study was limited to nosocomial bacterial pneumonia caused by CRGNB, while community-acquired pneumonia, bloodstream infections, urinary tract infections, and other infections were not considered. Finally, we did not involve molecular mechanisms of drug resistance, which is expected to be involved in future investigations.
Conclusion
In critically ill patients with CRGNB-infected HAP, AEAT, compared with IEAT, showed no significant impact on ICU or 28-day mortality. The effectiveness of AEAT is worthy of further exploration in future prospective studies.
Abbreviations
AEAT, appropriate empirical antibiotic treatment; HAP, hospital-acquired pneumonia; CRGNB, carbapenem-resistant Gram-negative bacteria; ICU, intensive care unit; IEAT, inappropriate empirical antibiotic treatment; MDROs, multidrug-resistant organisms; ESBL, extended-spectrum β-lactamase-producing; CRE, carbapenem-resistant Enterobacteriaceae; MDRPA, multidrug-resistant strains of Pseudomonas aeruginosa; VAP, ventilator-associated pneumonia; PCT, procalcitonin; CRP, C-reactive protein; LAC, lactic acid; TBI, total bilirubin; ALB, albumin; PLT, platelet count.
Ethics Approval and Informed Consent
This study was conducted complying with the Declaration of Helsinki and approved by the medical ethics committee of the Second Affiliated Hospital of Xi’an Jiaotong University (NO. 2023042). Since this was a retrospective study and patient information was protected, informed consent was granted an exemption.
Acknowledgments
The authors appreciate Dr Si Wang, who is from the Department of Laboratory Medicine of the First Affiliated Hospital of Xi’an Jiaotong University, for making a significant contribution during the revision of the paper and provided critical advice on improving the manuscript.
Funding
This study was supported by the National Key Research and Development Program of China (2018YFC1705905) and the Young Talent Support Program of Shaanxi Province University.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Kollef MH, Torres A, Shorr AF, Martin-Loeches I, Micek ST. Nosocomial infection. Crit Care Med. 2021;49(2):169–187. doi:10.1097/ccm.0000000000004783
2. Zhou Y, Yu F, Yu Y, Zhang Y, Jiang Y. Clinical significance of MDRO screening and infection risk factor analysis in the ICU. Am J Transl Res. 2021;13(4):3717–3723.
3. Rhodes A, Evans LE, Alhazzani W, et al. Surviving Sepsis Campaign: international Guidelines for Management of Sepsis and Septic Shock: 2016. Intensive Care Med. 2017;43(3):304–377. doi:10.1007/s00134-017-4683-6
4. Kaye KS, Pogue JM. Infections Caused by Resistant Gram-Negative Bacteria: epidemiology and Management. Pharmacotherapy. 2015;35(10):949–962. doi:10.1002/phar.1636
5. Maechler F, Peña Diaz LA, Schröder C, Geffers C, Behnke M, Gastmeier P. Prevalence of carbapenem-resistant organisms and other Gram-negative MDRO in German ICUs: first results from the national nosocomial infection surveillance system (KISS). Infection. 2015;43(2):163–168. doi:10.1007/s15010-014-0701-6
6. Furuya EY, Cohen B, Jia H, Larson EL. Long-Term Impact of Universal Contact Precautions on Rates of Multidrug-Resistant Organisms in ICUs: a Comparative Effectiveness Study. Infect Control Hospital Epidemiol. 2018;39(5):534–540. doi:10.1017/ice.2018.35
7. Santella B, Serretiello E, De Filippis A, et al. Lower Respiratory Tract Pathogens and Their Antimicrobial Susceptibility Pattern: a 5-Year Study. Antibiotics. 2021;10(7):465. doi:10.3390/antibiotics10070851
8. Pop-Vicas AE, D’Agata EM. The rising influx of multidrug-resistant gram-negative bacilli into a tertiary care hospital. Clin Infect Dis. 2005;40(12):1792–1798. doi:10.1086/430314
9. Teixeira PJ, Seligman R, Hertz FT, Cruz DB, Fachel JM. Inadequate treatment of ventilator-associated pneumonia: risk factors and impact on outcomes. J Hosp Infect. 2007;65(4):361–367. doi:10.1016/j.jhin.2006.12.019
10. Zak-Doron Y, Dishon Benattar Y, Pfeffer I, et al. The Association Between Empirical Antibiotic Treatment and Mortality in Severe Infections Caused by Carbapenem-resistant Gram-negative Bacteria: a Prospective Study. Clin Infect Dis. 2018;67(12):1815–1823. doi:10.1093/cid/ciy371
11. Li R, Tang H, Xu H, Cui K, Li S, Shen J. Effect on 30-day mortality and duration of hospitalization of empirical antibiotic therapy in CRGNB-infected pneumonia. Ann Clin Microbiol Antimicrob. 2021;20(1):15. doi:10.1186/s12941-021-00421-2
12. Al-Dorzi HM, Asiri AM, Shimemri A, et al. Impact of empirical antimicrobial therapy on the outcome of critically ill patients with Acinetobacter bacteremia. Ann Thorac Med. 2015;10(4):256–262. doi:10.4103/1817-1737.164302
13. Satlin MJ, Cohen N, Ma KC, et al. Bacteremia due to carbapenem-resistant Enterobacteriaceae in neutropenic patients with hematologic malignancies. J Infect. 2016;73(4):336–345. doi:10.1016/j.jinf.2016.07.002
14. Torres A, Niederman MS, Chastre J, et al. International ERS/ESICM/ESCMID/ALAT guidelines for the management of hospital-acquired pneumonia and ventilator-associated pneumonia: guidelines for the management of hospital-acquired pneumonia (HAP)/ventilator-associated pneumonia (VAP) of the European Respiratory Society (ERS), European Society of Intensive Care Medicine (ESICM), European Society of Clinical Microbiology and Infectious Diseases (ESCMID) and Asociación Latinoamericana del Tórax (ALAT). Eur Respir J. 2017;50(3). doi:10.1183/13993003.00582-2017
15. Tamma PD, Aitken SL, Bonomo RA, Mathers AJ, van Duin D, Clancy CJ. Infectious Diseases Society of America Guidance on the Treatment of Extended-Spectrum β-lactamase Producing Enterobacterales (ESBL-E), Carbapenem-Resistant Enterobacterales (CRE), and Pseudomonas aeruginosa with Difficult-to-Treat Resistance (DTR-P. aeruginosa). Clin Infect Dis. 2021;72(7):e169–e183. doi:10.1093/cid/ciaa1478
16. Hou Y, Ren J, Li J, et al. Relationship Between Mean Vancomycin Trough Concentration and Mortality in Critically Ill Patients: a Multicenter Retrospective Study. Front Pharmacol. 2021;12:690157. doi:10.3389/fphar.2021.690157
17. Ren J, Hou Y, Li J, et al. An evaluation on the association of vancomycin trough concentration with mortality in critically ill patients: a multicenter retrospective study. Clin Transl Sci. 2021;14(5):1780–1790. doi:10.1111/cts.13020
18. Rello J, Vidaur L, Sandiumenge A, et al. De-escalation therapy in ventilator-associated pneumonia. Crit Care Med. 2004;32(11):2183–2190. doi:10.1097/01.ccm.0000145997.10438.28
19. Evans L, Rhodes A, Alhazzani W, et al. Surviving Sepsis Campaign: international Guidelines for Management of Sepsis and Septic Shock 2021. Crit Care Med. 2021;49(11):e1063–e1143. doi:10.1097/ccm.0000000000005337
20. Seymour CW, Gesten F, Prescott HC, et al. Time to Treatment and Mortality during Mandated Emergency Care for Sepsis. N Engl J Med. 2017;376(23):2235–2244. doi:10.1056/NEJMoa1703058
21. Carrara E, Pfeffer I, Zusman O, Leibovici L, Paul M. Determinants of inappropriate empirical antibiotic treatment: systematic review and meta-analysis. Int J Antimicrob Agents. 2018;51(4):548–553. doi:10.1016/j.ijantimicag.2017.12.013
22. Chang Y, Jeon K, Lee SM, et al. The Distribution of Multidrug-resistant Microorganisms and Treatment Status of Hospital-acquired Pneumonia/Ventilator-associated Pneumonia in Adult Intensive Care Units: a Prospective Cohort Observational Study. J Korean Med Sci. 2021;36(41):e251. doi:10.3346/jkms.2021.36.e251
23. Morata L, Cobos-Trigueros N, Martínez JA, et al. Influence of multidrug resistance and appropriate empirical therapy on the 30-day mortality rate of Pseudomonas aeruginosa bacteremia. Antimicrob Agents Chemother. 2012;56(9):4833–4837. doi:10.1128/aac.00750-12
24. Hernández-Torres A, García-Vázquez E, Gómez J, Canteras M, Ruiz J, Yagüe G. Multidrug and carbapenem-resistant Acinetobacter baumannii infections: factors associated with mortality. Med Clin (Barc). 2012;138(15):650–655. doi:10.1016/j.medcli.2011.06.024
25. Liu CP, Shih SC, Wang NY, et al. Risk factors of mortality in patients with carbapenem-resistant Acinetobacter baumannii bacteremia. J Microbiol Immunol Infect. 2016;49(6):934–940. doi:10.1016/j.jmii.2014.10.006
26. Zilberberg MD, Nathanson BH, Sulham K, Fan W, Shorr AF. Carbapenem resistance, inappropriate empiric treatment and outcomes among patients hospitalized with Enterobacteriaceae urinary tract infection, pneumonia and sepsis. BMC Infect Dis. 2017;17(1):279. doi:10.1186/s12879-017-2383-z
27. Lin JN, Chen YH, Chang LL, Lai CH, Lin HL, Lin HH. Clinical characteristics and outcomes of patients with extended-spectrum β-lactamase-producing bacteremias in the emergency department. Intern Emerg Med. 2011;6(6):547–555. doi:10.1007/s11739-011-0707-3
28. Alrstom A, Alsuliman T, Daher N, Abouharb R. The Impact of Modifying Empirical Antibiotic Therapy Based on Intestinal Colonization Status on Clinical Outcomes of Febrile Neutropenic Patients. Infect Chemotherapy. 2021;53(1):63–74. doi:10.3947/ic.2020.0111
29. Katip W, Yoodee J, Uitrakul S, Oberdorfer P. Efficacy of loading dose colistin versus carbapenems for treatment of extended spectrum beta lactamase producing Enterobacteriaceae. Sci Rep. 2021;11(1):18. doi:10.1038/s41598-020-78098-4
30. Lim LM, Ly N, Anderson D, et al. Resurgence of colistin: a review of resistance, toxicity, pharmacodynamics, and dosing. Pharmacotherapy. 2010;30(12):1279–1291. doi:10.1592/phco.30.12.1279
31. Katip W, Uitrakul S, Oberdorfer P. Clinical Efficacy and Nephrotoxicity of the Loading Dose Colistin for the Treatment of Carbapenem-Resistant Acinetobacter baumannii in Critically Ill Patients. Pharmaceutics. 2021;14(1):31. doi:10.3390/pharmaceutics14010031
32. Stein GE, Babinchak T. Tigecycline: an update. Diagn Microbiol Infect Dis. 2013;75(4):331–336. doi:10.1016/j.diagmicrobio.2012.12.004
33. Grégoire N, Mimoz O, Mégarbane B, et al. New colistin population pharmacokinetic data in critically ill patients suggesting an alternative loading dose rationale. Antimicrob Agents Chemother. 2014;58(12):7324–7330. doi:10.1128/aac.03508-14
34. Katip W, Oberdorfer P. Clinical Efficacy and Nephrotoxicity of Colistin Alone versus Colistin Plus Vancomycin in Critically Ill Patients Infected with Carbapenem-Resistant Acinetobacter baumannii: a Propensity Score-Matched Analysis. Pharmaceutics. 2021;13(2):162. doi:10.3390/pharmaceutics13020162
35. Katip W, Uitrakul S, Oberdorfer P. A Comparison of Colistin versus Colistin Plus Meropenem for the Treatment of Carbapenem-Resistant Acinetobacter baumannii in Critically Ill Patients: a Propensity Score-Matched Analysis. Antibiotics. 2020;9(10):647. doi:10.3390/antibiotics9100647
36. Katip W, Oberdorfer P, Kasatpibal N. Effectiveness and Nephrotoxicity of Loading Dose Colistin-Meropenem versus Loading Dose Colistin-Imipenem in the Treatment of Carbapenem-Resistant Acinetobacter baumannii Infection. Pharmaceutics. 2022;14(6):1266. doi:10.3390/pharmaceutics14061266
37. Qian Y, Bi Y, Liu S, Li X, Dong S, Ju M. Predictors of mortality in patients with carbapenem-resistant Klebsiella pneumoniae infection: a meta-analysis and a systematic review. Ann Palliat Med. 2021;10(7):7340–7350. doi:10.21037/apm-21-338
38. Liu Z, Meng Z, Li Y, et al. Prognostic accuracy of the serum lactate level, the SOFA score and the qSOFA score for mortality among adults with Sepsis. Scand J Trauma Resusc Emerg Med. 2019;27(1):51. doi:10.1186/s13049-019-0609-3
39. Soreng K, Levy HR. Procalcitonin: an Emerging Biomarker of Bacterial Sepsis. Clin Microbiol Newsletter. 2011;33(22):171–178. doi:10.1016/j.clinmicnews.2011.10.004
40. Jekarl DW, Lee S, Kim M, Kim Y, Woo SH, Lee WJ. Procalcitonin as a prognostic marker for sepsis based on SEPSIS-3. J Clin Lab Anal. 2019;33(9):e22996. doi:10.1002/jcla.22996
41. Chaïbi K, Péan de Ponfilly G, Dortet L, Zahar JR, Pilmis B. Empiric Treatment in HAP/VAP: “Don’t You Want to Take a Leap of Faith?”. Antibiotics. 2022;11(3):359. doi:10.3390/antibiotics11030359
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.